
Abstract
Introduction
The pericapsular nerve group (PENG) block has been shown to be an effective approach to alleviating pain and reducing the need for opioids among older adults following hip surgery, with possible motor-sparing effects. No reports to date, however, have described appropriate ropivacaine volumes for use in the context of PENG block. The present prospective randomized controlled study was thus developed to assess the quadriceps muscle strength and analgesic efficacy associated with PENG block performed using three different volumes of 0.33% ropivacaine following general anesthesia in older adults undergoing hip arthroplasty.
Methods
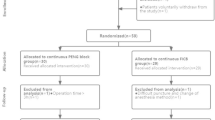
In this prospective randomized double-blind controlled clinical study, 60 patients were assigned at random to undergo ultrasound-guided PENG block for hip arthroplasty using different volumes of ropivacaine. Specifically, these patients were administered 10 ml (Group A, n = 20), 20 ml (Group B, n = 20), or 30 ml (Group C, n = 20) of 0.33% ropivacaine. Quadriceps muscle strength was evaluated at 6 h post-surgery. Visual analog scale (VAS) scores at rest and with movement were assessed at 4, 6, 12, and 24 h post-surgery. Block duration, adverse event incidence, and patient satisfaction were evaluated at 24 h post-surgery.
Results
Quadriceps motor block incidence rates at 6 h post-surgery in the 10 ml, 20 ml, and 30 ml groups were 5%, 20%, and 75%, respectively. Quadriceps muscle weakness at 6 h post-surgery was significantly more common in the 30 ml group relative to the others (p < 0.001). Patients administered 10 ml 0.33% ropivacaine exhibited significantly higher VAS pain scores at rest and with movement relative to those patients in the 20 ml and 30 ml treatment groups at all time points (p < 0.05). No apparent differences in analgesic efficacy were observed when comparing the 20 ml and 30 ml groups at 4, 6, 12, and 24 h post-surgery. No significant differences in block duration, satisfaction, or adverse event incidence were observed among groups.
Conclusions
The preservation of motor function in the 20 ml 0.33% ropivacaine group was superior to that in the 30 ml 0.33% ropivacaine group. Relative to the group that received 10 ml 0.33% ropivacaine during PENG block, those elderly patients administered 20 ml and 30 ml volumes of 0.33% ropivacaine experienced superior postoperative pain relief following hip arthroplasty.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
No reports to date, however, have described appropriate ropivacaine volumes for use in the context of the pericapsular nerve group (PENG) block |
This study aimed to assess the quadriceps muscle strength and analgesic efficacy associated with PENG block performed using three different volumes of 0.33% ropivacaine following general anesthesia in older adults undergoing hip arthroplasty |
What was learned from the study? |
The preservation of motor function in the 20 ml 0.33% ropivacaine was superior to that in the 30 ml 0.33% ropivacaine for PENG block in patients undergoing hip surgery |
Introduction
Excitation of the sympathetic nervous system following hip fracture surgery can result from severe pain, contributing to the release of stress hormones into systemic circulation whereupon they can alter hemodynamic parameters, increase the cardiovascular burden, and potentially contribute to the incidence of adverse cardiovascular events [1]. Surgical reduction and internal fixation is the most common approach to treating hip fractures, but this procedure often entails acute postoperative pain [2]. It is thus vital that patients undergoing hip fracture surgery be provided with appropriate pain management to ensure their optimal postoperative rehabilitation [3, 4].
As opioids can provide satisfactory postoperative analgesia, they have emerged as the primary approach to meeting the analgesic needs of patients recovering from hip fracture procedures. However, adverse events associated with opioid use are particularly common among the elderly, affecting an estimated 80% of patients [5]. Due to functional declines in many physiological systems, elderly patients generally exhibit poor narcotic tolerance while under regional or general anesthesia [6]. For these patients, it is vital to minimize the effects of anesthesia on various whole-body systems while also ensuring that these patients are provided with adequate perioperative pain relief so as to minimize the incidence of associated adverse outcomes. In 2018, Girón-Arango et al. [7] first suggested ultrasound-guided PENG block of the hip as an approach to providing postoperative analgesia for patients undergoing hip surgery.
Girón-Arango et al. [8] suggested that injecting a local anesthetic volume > 20 ml may result in motor block owing to the spread of these anesthetic agents to the femoral nerve between the pubic muscle and the Psoas major muscle. To date, however, no studies have clarified the optimal local anesthetic dosage for use when performing PENG block procedures in the clinic. Accordingly, this study was developed to compare the effects of utilizing different 0.33% ropivacaine volumes for ultrasound-guided PENG block procedures in patients undergoing hip surgery, exploring the most appropriate femoral nerve-sparing volume of ropivacaine while also comparing the analgesic effects of various analgesic volumes after surgery in an effort to provide a reference for future clinical use.
Methods
Ethical Approval
This was a prospective, double-blind, randomized controlled study. It was approved by The Ethics Committee of the First Affiliated Hospital of Wannan Medical College (No. 2 Zhe shan Street, Wuhu, Anhui, China) on February 27, 2023 (no. 2023-012). This study was registered in the Chinese Clinical Trial Registration Center (www.chictr.org.cn; ChiCTR2000029859, date of registration, February 15, 2020; date of patient enrollment, March 1,2023). All participants provided written informed consent, and the Declaration of Helsinki was adhered to for all clinical analyses.
Patient Enrollment
This study enrolled 60 patients 60–80 years of age undergoing hip arthroplasty at our hospital between February 2023 and August 2023. These patients ranged from 50 to 90 kg in body weight, and the American Society of Anesthesiologists (ASA) physical status of each patient ranged from I–III. Eligible patients were individuals without any history of prior hip surgery, allergies to local anesthetics, lower limb dysfunction, coagulatory dysfunction, puncture site infections, long-term opiate use, mental illnesses, or other conditions with the potential to affect cooperation. These patients were separated at random into three groups administered different volumes of 0.33% ropivacaine using a random number table: 10 ml (Group A, n = 20), 20 ml (Group B, n = 20), and 30 ml (Group C, n = 20). Patient groupings were kept confidential from investigators responsible for assessing block quality. Intraoperative data were collected by a resident anesthesiologist who remained blinded to randomization assignments. Postoperative data were collected by another investigator blinded to group assignments. A statistician conducted all statistical analyses, and the entire process remained confidential at all times.
PENG Block
All patients underwent preoperative fasting in accordance with the Enhanced Recovery After Surgery (ERAS) model. On entry into the operating room, NIBP, HR, ECG, SpO2, and PETCO2 were routinely monitored, and a venous infusion pathway was established in the upper limb. PENG block was then performed using an improved version of the approach described by Giron-Arango et al. [7]. The same experienced anesthesiologist performed ultrasound-guided PENG block before general anesthesia induction. Briefly, patients were placed in the supine position, and a curved low-frequency ultrasound probe (Nave S, Wisonic Medical, Inc., Wisonic, Shenzhen; 2–5 MHz) was vertically positioned on the transverse plane of the anterior inferior iliac spine (Fig. 1). This probe was then rotated in a counterclockwise manner to an angle of ~ 45° such that it was aligned with the pubic ramus. This plane enables the observation of the femoral artery, anterior inferior iliac spine, iliopubic eminence, and psoas tendon (Fig. 2). Then, a 22-G 80-mm nerve stimulation needle was inserted via an intra-plane approach, with the needle tip positioned on the fascial plane between the anterior aspect of the iliopsoas tendon and the posterior ramus of the pubic bone. After backdrawing to ensure the absence of blood, patients were then injected with 10, 20, or 30 ml 0.33% ropivacaine as per their groups.

PENG block via a lateromedial approach. a Demonstration of patient and probe positioning with needle insertion site indicated. b Ultrasonographic images of PENG block. AIIS indicates anterior inferior iliac spine, FA femoral artery, IPE iliopubic eminence, PT psoas tendon, IPM iliopsoas muscle

Comparison of the VAS scores at rest. Abbreviations: Group A 10-ml injection, Group B 20-ml injection, Group C 30-ml injection, VAS visual analog scale. T0: preoperative; T1: 4 h after surgery; T2: 6 h after surgery; T3: 12 h after surgery; T4: 24 h after surgery
Perioperative Management
An attending anesthesiologist blinded to patient groups performed all general anesthesia administration. LMA general anesthesia was administered after the PENG block procedure, with etomidate (0.2–0.5 mg/kg), sufentanil (0.5–0.7 µg/kg), and cis-atracurium (0.15–0.2 mg/kg) being used for induction, while maintenance was achieved using propofol (4–6 mg/kg/h) and remifentanil (0.2–0.5 µg/kg/min). BIS values were used to adjust anesthetic dosages during the procedure so that the BIS value remained in the 40–60 range.
Postoperative Analgesia
After the procedure was complete, IV patient-controlled analgesia (PCA) was provided for all patients with an intravenous analgesic pump (2 µg/kg of sufentanil and 16 mg of ondansetron, in normal saline at a final volume of 100 ml). Treatment parameters were as follows: bolus = 2 µg; continuous infusion volume = 2 ml/h; lockout interval = 15 min.
Measurement and Calculation
The primary outcome was quadriceps motor block incidence at 6 h postoperatively. Quadriceps motor block was defined by paralysis or paresis of knee extension. To assess knee extension, patients were evaluated in the supine position with the hip at knee respectively flexed at 45° and 90° angles. Patients were then requested to initially extend their knee against gravity and to do so against resistance. A 3-point scale was used to grade knee extension as follows: 0 = normal strength (able to extend against both gravity and resistance), 1 = paresis (able to extend against gravity but not resistance), and 2 = paralysis (extension not possible). A 75–100% decrease in knee extension was defined as complete quadriceps motor block, while 25–7%% and < 25% reductions respectively were defined as partial quadriceps motor block and the absence of quadriceps motor block. Quadriceps motor block incidence was quantified based on the number of patients exhibiting partial or complete quadriceps motor block.
The secondary outcome in this study was VAS pain scores after surgery. All pain analyses were assessed by an investigator blinded to patient groupings with VAS scores at rest and with movement (VAS; 0–10; 0: no pain, 10: worst imaginable pain) at 4 (T1), 6 (T2), 12 (T3), and 24 (T4) h after the surgery. Baseline pain levels for each patient were also evaluated 1 day before surgery (T0).
Complications and adverse events were evaluated at 15 min after PENG block. Block duration and patient satisfaction score (using a scale of 0–10, 10 being the most satisfied) were analyzed at 24 h post-surgery.
Study Sample Size and Statistics Analysis
The sample size was calculated using the GPower 3.1.1 computer program software. With a power of 0.9 and a set α error of 0.05, the minimum sample size was 18 patients per group. Accounting for a 10% dropout rate, 60 patients were enrolled, with 20 patients allocated to each group.
SPSS 26.0 (IBM, Armonk, NY, USA) was used to conduct statistical analyses. Continuous data were assessed for normality and were analyzed with Student’s t-tests when normally distributed. Skewed and ordinal data were compared with MannßWhitney U tests. Categorical data were compared with the χ2 test. Fisher’s exact test was used for any cell with a count ; 5. A two-sided p value < 0.05 was the threshold of significance.
Results
This study enrolled 60 total patients, with no dropouts. The characteristics of these patients are presented in Table 1.
The incidence of quadriceps motor block at 6 h post-surgery in Groups A, B, and C was 5%, 20%, and 75%, respectively, with significantly more patients in Group C experiencing quadriceps muscle weakness at 6 h (p < 0.001) post-surgery (Table 2).
Similar baseline pain at rest and with movement were observed among groups before surgery: Group A: 4.65 ± 1.04 vs. Group B: 4.30 ± 0.98 vs. Group C: 4.10 ± 0.97 (p = 0.729) and 5.30 ± 0.80 vs. 4.90 ± 0.85 vs. 4.60 ± 0.94 (p = 0.709), respectively. At all time points, significantly higher VAS pain scores at rest and with movement were recorded in Group A relative to Groups B and C (p < 0.05) (Figs. 2, 3). No apparent differences in analgesic efficacy were observed between Groups B and C at 4, 6, 12, or 24 h post-surgery.

Comparison of the VAS scores at movement. Abbreviations: Group A 10-ml injection, Group B 20-ml injection, Group C 30-ml injection, VAS visual analog scale. T0: preoperative; T1: 4 h after surgery; T2: 6 h after surgery; T3: 12 h after surgery; T4: 24 h after surgery
No significant differences among groups were observed regarding block duration (p = 0.214) or patient satisfaction (p = 0.813) at 24 h post-surgery. Rates of postoperative nausea and vomiting (PONV) (p = 0.436) and urinary retention (p = 0.804) were similar across groups (Table 2).
Discussion
The utilization of ultrasound-guided PENG block as an approach to providing perioperative analgesia to patients undergoing hip surgery is becoming increasingly common [9, 10]. While PENG block can yield satisfactory analgesic efficacy, it also has the potential to block the function of the femoral nerve [11]. Femoral nerve block, in turn, reduces quadriceps muscle strength, thereby delaying the ability of patients to initially get out of bed following hip surgery. The present study was the first comparison of the effects of using three different volumes of 0.33% ropivacaine to perform PENG block as a means of providing postoperative analgesia to older patients undergoing hip arthroplasty while preserving quadriceps strength. Relative to a 10 ml volume of 0.33% ropivacaine, 20 ml and 30 ml injection volumes were associated with greater postoperative pain relief. However, while both the 20 ml and 30 ml injection volumes were associated with comparable analgesic effects, the 30 ml volume was associated with increased incidence of quadriceps muscle weakness at 6 h post-surgery relative to the 20 ml volume.
As a novel regional nerve block approach first proposed by Girón-Arango et al., PENG block consists of the injection of local anesthetic agents between the pubic ramus and psoas tendon to block the femoral, obturator, and accessory obturator nerves. Short et al. reported that the joint branch of the femoral nerve enters the ilium at the L4-5 level before going deep into the psoas major muscle and tendon between the ilium and iliac crest, innervating the hip joint capsule [12]. In their cadaver study, Ciftci et al. [13] determined that the injection of 30 ml dye between the pubic branch and psoas tendon led to its eventual distribution throughout the iliopsoas, medial femoral, and gluteus medius muscles while staining the femoral and obturator nerves. In the present study, quadriceps muscle block affected 5%, 20%, and 75% of patients in the 10 ml, 20 ml, and 30 ml injection groups, respectively, at 6 h post-surgery. These data strongly support a link between the utilized anesthetic volume and the risk of quadriceps muscle weakness. Leurcharusmee et al. [14] recently explored the optimal femoral nerve-sparing volume for PENG block procedures using cadavers and determined that 13.2 ml methylene blue was the MEV90 volume necessary to spare the femoral nerve in this system. However, additional clinical research will be necessary to clarify the degree to which this MEV90 value correlates with outcomes associated with local anesthetic volumes injected in live patients.
The postoperative recovery of patients following hip surgery benefits greatly from early active functional exercise, which can be restricted to some degree by persistent quadriceps muscle weakness. There is thus clear clinical significance to performing additional studies focused on identifying the minimum femoral nerve-sparing injection volume for use when performing PENG block procedures. Some research teams have also explored the effects associated with utilizing large local anesthetic injection volumes for PENG block procedures in the context of hip surgery. For example, Ahiskalioglu et al. determined that injecting a 30 ml volume of local anesthetic when performing a PENG block can result in the upward diffusion of the anesthetic, potentially resulting in a lumbar plexus block-like effect [15]. In a recent anatomical study, simultaneous staining of the femoral nerve was observed in 6/12 (50%) 20 ml specimens and 12/12 (100%) 30 ml specimens [16]. Additional randomized controlled clinical studies will be necessary to clarify whether high-volume PENG block can replace lumbar plexus block.
Local anesthetic volume is an important determinant of the range, duration, and safety of nerve block procedures [17, 18]. The analgesic efficacy associated with larger local anesthetic volumes in the present study was superior to that associated with lower volumes. Block duration was comparable in all three patient groups. As such, increases in local anesthetic volume had no impact on the duration of block efficacy. Importantly, no patients in any of these treatment groups experienced any serious postoperative complications.
There are multiple limitations to this study. For one, the quadriceps muscle strength of participating patients was not validated via electromyography or other electrophysiological examination techniques, which may have yielded more objective findings. Second, imaging approaches were not employed to assess the diffusion ranges for different volumes of 0.33% ropivacaine. Most studies of local anesthetic diffusion in the context of PENG block procedures conducted to date have been performed using human cadavers, with few analyses of live patients and/or volunteers. In the future, MRI or 3D-CT strategies will be employed to better visualize the diffusion of local anesthetics administered with radioactive contrast agents when performing PENG block procedures. Moreover, the effects of different local anesthetic injection volumes on patient rehabilitation following hip arthroplasty were not assessed. Furthermore, all block procedures were also performed by a single anesthesiologist, reducing bias but also potentially restricting the degree to which these results can be generalized. Lastly, the time of analgesic onset was not compared among groups.
Conclusions
The preservation of motor function in the 20 ml 0.33% ropivacaine was superior to that in the 30 ml 0.33% ropivacaine for pericapsular nerve group block in patients undergoing hip surgery. Relative to the group that received 10 ml 0.33% ropivacaine during PENG block, those elderly patients administered 20 ml and 30 ml volumes of 0.33% ropivacaine experienced superior postoperative pain relief following hip arthroplasty.
Data Availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Anger M, Valovska T, Beloeil H, et al. PROSPECT guideline for total hip arthroplasty: a systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76:1082–97.
Panzenbeck P, von Keudell A, Joshi GP, et al. Procedure-specific acute pain trajectory after elective total hip arthroplasty: systematic review and data synthesis. Br J Anaesth. 2021;127:110–32.
Skinner HB, Shintani EY. Results of a multimodal analgesic trial involving patients with total hip or total knee arthroplasty. Am J Orthop (Belle MeadNJ). 2004;33:85–92.
Tan M, Law LS, Gan TJ. Optimizing pain management to facilitate enhanced recovery after surgery pathways. Can J Anaesth. 2015;62:203–18.
Okike K, Chang RN, Chan PH, et al. Prolonged opioid usage following hip fracture surgery in opioid-naïve older patients. J Arthroplasty. 2023;38:1528–34.
Stone JM, Pujari A, Garlich J, et al. A retrospective cohort study on chronic opioid use after geriatric hip fracture surgery-risk factors, trends, and outcomes. J Am Acad Orthop Surg. 2023;31:312–8.
Giron-Arango L, Peng PWH, Chin KJ, et al. Pericapsular nerve group (PENG) block for hip fracture. Reg Anesth Pain Med. 2018;43:859–63.
Giron-Arango L, Tran J, Peng PW, et al. A novel indication of pericapsular nerve group block: surgical anesthesia for vein ligation and stripping. J Cardiothorac Vasc Anesth. 2020;34:845–6.
Lin XF, Liu CWY, Goh QY, et al. Pericapsular nerve group (PENG) block for early pain management of elderly patients with hip fracture: a single-center double-blind randomized controlled trial. Reg Anesth Pain Med. 2023;48:535–9.
Wang Y, Wen HC, Wang ML, et al. The efficiency of ultrasound-guided pericapsular nerve group block for pain management after hip surgery: a meta-analysis. Pain Ther. 2023;12:81–92.
Tomlinson J, Ondruschka B, Prietzel T, et al. A systematic review and meta-analysis of the hip capsule innervation and its clinical implications. Sci Rep. 2021;11(1):5299.
Short AJ, Barnett J, Gofeld M, et al. Anatomic study of innervation of the anterior hip capsule: implication for image-guided intervention. Reg Anesth Pain Med. 2018;43:186–92.
Ciftci B, Ahiskalioglu A, Altintas HM, et al. A possible mechanism of motor blockade of high volume pericapsular nerve group (PENG) block: a cadaveric study. J Clin Anesth. 2021;74: 110407.
Leurcharusmee P, Kantakam P, Intasuwan P, et al. Cadaveric study investigating the femoral nerve-sparing volume for pericapsular nerve group (PENG) block. Reg Anesth Pain Med. 2023;48:549–52.
Ahiskalioglu A, Aydin ME, Celik M, et al. Can high volume pericapsular nerve group (PENG) block act as a lumbar plexus block? J Clin Anesth. 2020;61: 109650.
Kim JY, Kim JY, Kim D-H, et al. Anatomical and radiological assessments of injectate spread stratified by the volume of the pericapsular nerve group block. Anesth Analg. 2023;136:597–604.
Christiansen CB, Madsen MH, Rothe C, et al. Volume of ropivacaine 0.2% and sciatic nerve block duration: a randomized, blinded trial in healthy volunteers. Acta Anaesthesiol Scand. 2020;64:238–44.
Kim H, Han J, Lee WJ, et al. Effects of local anesthetic volume (standard versus low) on incidence of hemidiaphragmatic paralysis and analgesic quality for ultrasound-guided superior trunk block after arthroscopic shoulder surgery. Anesth Analg. 2021;133:1303–10.
Acknowledgements
We thank all the patients who participated in this study.
Medical Writing/Editorial Assistance.
Initial study design, ethical approval, and recruitment of the study participants were conducted by Meijing Lu and Huaichang Wen.We thank LetPub (www.letpub.com) for linguistic assistance and pre-submission expert review, which was funded by the Anhui Province Clinical Key Specialized Suggested Project Funding.
Funding
The present work was supported by grants from the Anhui Province Clinical Key Specialized Suggested Project Funding. The Rapid Service Fee was funded by the authors.
Author information
Authors and Affiliations
Contributions
Meijing Lu and Huaichang Wen contributed to the study design. Huaichang Wen and Weihua Zhang wrote the manuscript. Yi Wang, Weihua Zhang collected the data. Weihua Zhang and Yi Wang performed the data analysis. Meijing Lu and Huaichang Wen reviewed the final draft. All authors read and approved the final manuscript. Meijing Lu is responsible for this article.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare no conflicts of interest.
Ethical Approval
This prospective, double-blind, randomized controlled study adhered to the World Medical Association Declaration of Helsinki. Data are presented in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statement. This study was approved by the Ethics Committee of the First Affiliated Hospital of Wannan Medical College, No. 2 Zhe shan Street, Wuhu, Anhui, China, on 27/02/2023. The study was registered in the Chinese Clinical Trial Registration Center on www.chictr.org.cn (registration number: ChiCTR2000029859). Written informed consent was obtained from all volunteers before the study procedures.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Wen, H., Zhang, W., Wang, Y. et al. Effects of Different Volumes of Ropivacaine for Pericapsular Nerve Group Block on Incidence of Quadriceps Weakness and Analgesic Efficacy Following Hip Arthroplasty: A Randomized Controlled Trial. Pain Ther 13, 533–541 (2024). https://doi.org/10.1007/s40122-024-00590-w
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40122-024-00590-w