
Abstract
Background
Metformin is the most widely used oral antihyperglycemic agent for patients with type 2 diabetes mellitus (T2DM). Despite the possible benefits of metformin on diabetes mellitus (DM) and heart failure (HF), acute or unstable HF remains a precaution for its use.
Objective
The aim of the present prospective randomized controlled trial was to assess whether metformin treatment has beneficial effects on patients with T2DM with hypertension without overt HF.
Methods
A total of 164 patients (92 males, 72 females; median age 66 years) were included in this study. Patients with T2DM with a history of hypertension were randomized 1:1 to treatment for 1 year with either metformin (metformin-treated group) or other hypoglycemic agents (control group). The primary endpoints were changes in brain natriuretic peptide (BNP) levels, left ventricular (LV) mass index, and indicators of LV diastolic function. We also evaluated changes in both clinical findings and blood laboratory examination data.
Results
We observed no significant changes between baseline and 1-year post-treatment in LV mass index, BNP levels, or E/e′ (early diastolic transmitral flow velocity/early diastolic mitral annular velocity; an indicator of LV diastolic function) in either the metformin-treated (n = 83) or the control (n = 81) groups. The metformin-treated group had a significant reduction of body mass index (BMI) and low-density lipoprotein cholesterol (LDL-C), but the control group did not. We determined that renal function, including serum creatinine and estimated glomerular filtration rate, deteriorated significantly in the control group but not in the metformin-treated group.
Conclusion
LV mass and diastolic function were not affected after 1 year of metformin treatment in patients with T2DM. However, we observed benefits in terms of reductions in both BMI and LDL-C levels and preservation of renal function.
Trial Registration
UMIN000006504. Registered 7 October 2011.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
In addition to lowering blood glucose levels, metformin has been reported to exert cardio-protective effects. |
One year of treatment with metformin did not affect the LV mass or diastolic function in patients with type 2 diabetes mellitus and hypertension. |
Treatment with metformin was associated with a reduction of body mass index and serum LDL-C levels, and preservation of renal function. |
1 Introduction
The prevalence of type 2 diabetes mellitus (T2DM) among patients with heart failure (HF) continues to increase, approaching 40% in recent clinical trials [1, 2]. Studies have reported that diabetes mellitus (DM) is the second most common pathology related to HF, after coronary artery disease, with a doubled risk of HF [3]. It has also been shown that HF is usually an initial manifestation of cardiovascular disease in patients with T2DM [4]. On the other hand, the severity of HF is associated with a slightly increased risk of developing DM [5].
Metformin is the most widely used oral antihyperglycemic agent in patients with T2DM. It has been shown to improve insulin sensitivity, mainly in the skeletal muscles and liver, and reduces blood glucose by decreasing gluconeogenesis in the liver. It also appears to have cardioprotective potential. Various experimental and clinical studies have demonstrated that metformin has a beneficial effect on lipid, atherosclerotic, and inflammatory profiles as well as on endothelial function [6, 7]. In dogs with pacing-induced HF, metformin also significantly reduced pulmonary capillary wedge pressure and left ventricular (LV) end-diastolic pressure versus control [8]. The mechanisms underlying these beneficial effects have been linked to the activation of 5′ adenosine monophosphate-activated protein kinase (AMPK) [9]. A recent study indicated that metformin also has AMPK-independent effects, including hepatic glucagon-signaling inhibition following decreased production of cyclic AMP [10]. Despite these possible benefits of metformin on DM and HF, Japan’s Ministry of Health, Labour and Welfare classifies HF as a contraindication to metformin therapy because of the risk of developing lactic acidosis [11]. The US FDA has removed HF as a contraindication to metformin use, but acute or unstable HF remains a precaution.
The aim of the present prospective randomized controlled trial was to assess whether metformin treatment has beneficial effects on patients with T2DM and hypertension without overt HF. To this end, we analyzed the effects of metformin on LV mass (LVM) and diastolic function in patients with T2DM with a history of hypertension.
2 Methods
2.1 Study Population
This multicenter, prospective, randomized controlled trial was conducted at 26 centers in Japan between September 2011 and December 2017. This trial (UMIN000006504) conformed to the Declaration of Helsinki and good clinical practice guidelines and was approved by independent ethics committees. All patients provided written informed consent before participating in trial-related activities. Key inclusion criteria were as follows: (1) patients aged 30–75 years with a history of hypertension; (2) blood pressure < 140/90 mmHg and stable for at least 1 month; (3) T2DM with glycated hemoglobin (HbA1c) levels > 6.5% in the absence of metformin, thiazolidinediones, or insulin treatment; and (4) absence of renal dysfunction (serum creatinine < 1.3 mg/dL in males and < 1.2 mg/dL in females). Key exclusion criteria included a diagnosis of type 1 or secondary DM; severe liver dysfunction or cirrhosis; acute coronary syndrome, severe coronary heart disease (left main trunk disease or triple vessel disease); atrial fibrillation or implanted pacemaker; and shock, congestive HF, or pulmonary embolism with hypoxia. Additional exclusion criteria were as follows: a history of lactic acidosis; alcohol abuse or dehydration with gastrointestinal dysfunction; severe ketosis, diabetic coma, or pre-coma; severe infection or perioperative condition or severe trauma; malnutrition, weakness, dysfunction in pituitary or adrenal gland; history of allergic reaction to metformin; pregnancy or plans to become pregnant; and individuals recognized as inappropriate by the physician. Following initial screening, eligible patients were randomized 1:1 into one of the following groups: to be treated with metformin (metformin-treated group) or other hypoglycemic agents without metformin (control group). Both groups received therapy for 1 year. Since earlier studies have shown that thiazolidinediones affect cardiac hypertrophy [12], they were not used in this trial for either group.
Patients were allocated using a secure web response system, in accordance with the sequence from the randomization list. We adjusted the following factors as confounding for randomization: age, sex, blood pressure, and HbA1c levels. All patients received diabetes education at enrollment and reinforcement of this throughout the study. Specifically, the latter consisted of routine clinical practice, including dietary and exercise suggestions according to Japanese guidelines. Metformin was initiated at 500 mg/day and titrated up to 2250 mg/day. If required, antihyperglycemic agents were added to the therapeutic protocol, with the exception of thiazolidinediones.
At baseline, eligible patients underwent the following procedures: physical examination, urine test (including urine albumin and creatinine concentration), and fasting blood sampling for biological measurements (including brain natriuretic peptide [BNP], liver enzyme, plasma lipids, and HbA1c). Plasma BNP was measured with a chemiluminescent enzyme immunoassay. We also performed chest X-ray examination, electrocardiogram, and echocardiography. Similar examinations were also performed at 6 months and 1 year post-randomization.
2.2 Echocardiography
Echocardiography was performed at rest. During the test, patients were in the partial left decubitus position, and we used standard parasternal and apical views. M-mode echocardiograms of the LV chamber were recorded under two-dimensional control. We followed the recommendations of the American Society of Echocardiography in performing the measurements of the interventricular septal thickness at end-diastole (IVSd), LV end-diastolic dimension (LVEDD), and posterior wall thickness at end-diastole (PWd). LVM was measured according to the following formula:
LVM index (LVMI) was calculated by dividing LVM with body surface area (BSA) using weight (W) and height (H), defined as follows:
We measured the peak flow velocity of early diastole (E wave). Color tissue Doppler imaging loops were obtained in the apical four-chamber view. Peak early diastolic mitral annulus velocity (e′) was measured at the base of the septum, and the E/e′ ratio was calculated.
2.3 Definitions
The primary endpoints for the current analysis were as follows: changes in LVMI, plasma BNP levels, and echocardiographic parameters that indicate LV diastolic function, including the E/e′ ratio. Other evaluation items included clinical findings and blood laboratory examination data.
2.4 Statistical Analysis
Data are presented as numbers and percentages, mean value ± standard deviation, or median and interquartile range (IQR). We used Fisher’s exact test to compare categorical variables. Continuous two variables were compared using the Student’s t test or the Mann–Whitney U test, according to their distributions. We compared continuous three variables using repeated-measures analysis of variance (ANOVA), the Friedman test, the paired t test with Bonferroni correction, or the Wilcoxon signed-rank test with Bonferroni correction according to their distributions. We used JMP 10.0 (SAS Institute Inc, Cary, NC, USA) to perform all analyses. We considered all p values < 0.05 to be statistically significant.
3 Results
3.1 Baseline Characteristics
A total of 231 patients with T2DM with a history of hypertension without metformin treatment were included in the study (randomized 1:1 into metformin-treated and control groups). Serial echocardiography and BNP data were missing in 64 and 52 patients, respectively, and a further 67 patients were excluded, leaving 164 patients for analysis (see Fig. 1). As Table 1 shows, despite randomization, we observed significant differences in body mass index (BMI) within the baseline characteristics of the metformin-treated and control groups (p < 0.01).

Flow chart of study process. BNP brain natriuretic peptide, E/e′ early diastolic transmitral flow velocity/early diastolic mitral annular velocity, T2DM type 2 diabetes mellitus
3.2 Primary Efficacy Endpoint
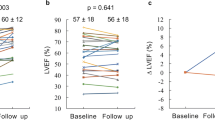
We observed no difference in serial changes in LVMI in both groups during the 1-year treatment period. BNP levels were significantly changed in the control group (p < 0.017) (Table 2) but were unchanged in the metformin-treated group (Table 3). Comparing BNP changes between two timepoints showed no statistical significance following Bonferroni correction in the control group (Table 3). When percentage change between baseline and 1 year in each parameter between control and metformin-treated groups was compared, no difference in changes in BNP levels was found (Table 4). E/e′, which indicates LV diastolic function, was unchanged during the treatment period in both groups.
3.3 Other Evaluation Data
Over the study period, the median HbA1c significantly reduced in both groups (p < 0.001). Of note, the median BMI was significantly reduced only in the metformin-treated group (p = 0.001). A post-hoc analysis of the Friedman test indicated that BMI changes were statistically significant between the baseline versus 6 months and baseline versus 1 year, even after Bonferroni correction. When comparing percentage change between baseline and 1 year in each parameter, only BMI was significantly reduced in the metformin-treated versus the control group (p < 0.01). We observed that serum creatinine and estimated glomerular filtration rate (eGFR) levels were significantly changed in the control group (p < 0.0074 for creatinine; p < 0.0074, for eGFR) (Table 2) but not in the metformin-treated group (Table 3). A comparison of changes in creatinine and eGFR between two time points showed a statistically significant difference between baseline versus 6 months and baseline versus 1 year in the control group. Conversely, low-density lipoprotein cholesterol (LDL-C) and non-high-density lipoprotein cholesterol (HDL-C) levels were significantly changed in the metformin-treated group (p < 0.00016 for LDL-C; p < 0.0012 for non-HDL-C) (Table 3). However, no changes were found in the control group. Comparing changes in LDL-C between the two time points identified a significant reduction between baseline and 6 months and between baseline and 1 year. The reduction in non-HDL-C was significant only between baseline and 6 months. Comparing percentage change between baseline and 1 year in each parameter between control and metformin-treated groups showed no changes in creatinine, eGFR, LDL-C, or non-HDL-C (Table 4). Mean metformin doses at 6 months and 1 year were 857 and 909 mg/day, respectively. Table 5 summarizes the changes of metformin doses. Oral hypoglycemic agents used at baseline included sulfonylureas, dipeptidyl peptidase-4 (DPP-4) inhibitors, and α-glucosidase inhibitors (Table 5). Tables 6, 7 and 8 summarize the serial changes of other medications. No differences were observed in the use of lipid-lowering agents between the two groups in the course of the treatment period.
4 Discussion
The main finding of this study was that 1 year of metformin treatment in patients with T2DM did not affect LVM or LV diastolic function versus treatments with other hypoglycemic agents. However, it significantly reduced BMI and LDL-C levels and preserved renal function.
Metformin is an oral hypoglycemic drug of the biguanide class that lowers blood glucose levels by decreasing hepatic glucose production and improving the insulin sensitivity of the peripheral tissues by increasing glucose uptake. It is currently used as a first-line treatment for T2DM. The drug is recommended during all stages of therapy as monotherapy and in combination with other oral antihyperglycemic drugs as well as insulin. Such guidelines are due to its low cost, safety, and association with a reduction in the risk of cardiovascular events [13,14,15].
T2DM is an independent risk factor for cardiovascular disease and is associated with a higher incidence of HF, as first reported in the Framingham study [16]. The risk of HF in patients with T2DM is almost two times higher for men and five times higher for women than in the general population, and patients with T2DM account for one-third of all HF cases [17]. However, concerns regarding the development of lactic acidosis with the use of phenformin led the US FDA to apply a black box warning to metformin cautioning against using it in the setting of chronic kidney disease because of possible impaired drug excretion. It also recommended caution in patients with conditions that may promote lactate accumulation. Examples of the latter include congestive HF and chronic liver disease. The FDA has removed congestive HF as a contraindication to metformin use. However, acute or unstable congestive HF remains a precaution. In Japan, to date, HF is classified as a contraindication to metformin therapy because of the risk of lactic acidosis [11]. Therefore, we aimed to verify the effects of metformin on cardiac morphology and function in patients with hypertension who were at risk for HF development.
Our study showed no clear changes in the indicators of LV diastolic function and LVM. There are various reasons for not having proved our working hypothesis. First, the previously observed effects of metformin on the reduction of cardiovascular events differ from the prevention of cardiac hypertrophy and/or diastolic dysfunction observed in the early phase of hypertension. Several events are associated with HF development, and additional factors may be associated with metformin treatment. Second, the use of DPP-4 inhibitors increased in the control group over the treatment period. Several reports have shown beneficial effects from DPP-4 inhibitors on cardiac hypertrophy in animal experiments. They act by suppressing sodium-proton pump exchanger type 1 or insulin-like growth factor-I [18, 19]. However, several clinical studies have reported that the use of DDP-4 inhibitors was associated with worsening of HF [20]. A meta-analysis [21] of randomized controlled trials investigating the effects of hypoglycemic agents on LVM recently showed that gliclazide was the only medication to significantly reduce LVM in patients with T2DM. Additionally, metformin exhibited negative effects on the prevention of cardiac hypertrophy. Our results are in line with this report. Sodium–glucose co-transporter 2 (SGLT2) inhibitors have proven effective in reducing HF hospitalization in patients with DM, and glucagon-like peptide-1 (GLP-1) receptor agonists are beneficial for patients with ischemic heart disease [22, 23]. However, GLP-1 receptor agonists were not used in either of our groups in this study. The use of SGLT2 inhibitors had not been approved by the Japan Ministry of Health, Labor, and Welfare when this study was conducted.
We observed several beneficial effects of metformin in our study population. Like previous reports, we observed a significant decrease in BMI following metformin treatment, and its effect was more evident in the first 6 months of treatment [24,25,26]. A possible explanation for this effect is the higher usage of sulfonylureas in the control group than in the metformin-treated group. However, other explanations for the mechanisms of metformin-induced weight loss may be considered. An earlier study suggested that metformin reduces weight by affecting appetite signals in the brain, fat oxidation, and fat storage in the liver [27]. An additional report suggested that metformin-induced weight loss, secretion of GLP-1 and peptide YY, and increases in conjugated bile acid are associated with alterations of the gut microbiota [28, 29].
Renal function in the control group deteriorated during the 1-year study but was unchanged in the metformin-treated group. Uncertainty remains about the underlying mechanisms. Recently published data support the use of metformin in patients with renal diseases [30]. An analysis by the REACH (Reduction of Atherothrombosis for Continued Health) registry suggested that the proposed cardiovascular benefits of metformin may include patients with established atherosclerosis and moderate chronic kidney disease [31]. However, the abovementioned reports do not support the hypothesis of a renoprotective effect. Metformin has previously been shown to attenuate renal fibrosis in both AMPKα2-dependent and -independent manners [32]. In our study group, kidney function may have been preserved by such antifibrotic effects. Hypertension causes renal damage, which in turn further increases blood pressure. Consequently, patients with DM and hypertension may be good candidates for metformin treatment.
In the metformin-treated group, LDL-C significantly decreased in the study period. This was more evident during the first half of the study than the last. It has been recently shown in patients with T2DM that metformin treatment reduces the levels of three acyl-alkyl-phosphatidylcholine metabolites [33]. The reduction of LDL-C levels may be due to such changes in metabolic profiles. The latter is most likely induced by metformin-induced activation of AMPK and consequent suppression of sterol regulatory element-binding protein 1c (SREBP1c) and fatty acid desaturation [33]. These findings suggest that metformin may have a beneficial effect on lipid metabolism for the prevention of atherosclerosis in patients with hypertension.
The present study has several limitations. First, our protocol set the target sample size at 440 patients (UMIN000006504). We assumed the annual LV weight reduction with metformin treatment would be 6 g [34]. To determine the superiority of these values with 80% power and a two-sided overall significance level of 5% required 185 patients per arm. To allow for a loss-to-follow-up rate of 15%, we determined that we would need to enroll 220 patients in each study arm. However, slow recruitment meant we only recruited 231 patients, which reduced the power of this trial. Second, our findings are subject to confounding factors because the two study groups had different BMI values at baseline. Finally, the metformin dose was relatively small compared with that used in other countries, which may have limited the effects of metformin.
5 Conclusion
Treatment of patients with T2DM with metformin did not affect LVM or LV diastolic function versus treatments with other hypoglycemic agents over the course of 1 year. However, metformin reduced BMI, lowered LDL-C, and preserved renal function.
References
McMurray JJ, Packer M, Desai AS, Gong J, Lefkowitz MP, Rizkala AR, et al. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N Engl J Med. 2014;371:993–1004.
Cohen-Solal A, Beauvais F, Logeart D. Heart failure and diabetes mellitus: epidemiology and management of an alarming association. J Card Fail. 2008;14:615–25.
Yang H, Negishi K, Otahal P, Marwick TH. Clinical prediction of incident heart failure risk: a systematic review and meta-analysis. Open Heart. 2015;2:e000222.
Shah AD, Langenberg C, Rapsomaniki E, Denaxas S, Pujades-Rodriguez M, Gale CP, et al. Type 2 diabetes and incidence of cardiovascular diseases: a cohort study in 1.9 million people. Lancet Diabetes Endocrinol. 2015;3:105–13.
Demant MN, Gislason GH, Kober L, Vaag A, Torp-Pedersen C, Andersson C. Association of heart failure severity with risk of diabetes: a Danish nationwide cohort study. Diabetologia. 2014;57:1595–600.
Wong AK, Symon R, AlZadjali MA, Ang DS, Ogston S, Choy A, et al. The effect of metformin on insulin resistance and exercise parameters in patients with heart failure. Eur J Heart Fail. 2012;14:1303–10.
Ladeiras-Lopes R, Fontes-Carvalho R, Bettencourt N, Sampaio F, Gama V, Leite-Moreira A. Novel therapeutic targets of metformin: metabolic syndrome and cardiovascular disease. Expert Opin Ther Targets. 2015;19:869–77.
Sasaki H, Asanuma H, Fujita M, Takahama H, Wakeno M, Ito S, et al. Metformin prevents progression of heart failure in dogs: role of AMP-activated protein kinase. Circulation. 2009;119:2568–77.
Rena G, Hardie DG, Pearson ER. The mechanisms of action of metformin. Diabetologia. 2017;60:1577–85.
Miller RA, Chu Q, Xie J, Foretz M, Viollet B, Birnbaum MJ. Biguanides suppress hepatic glucagon signalling by decreasing production of cyclic AMP. Nature. 2013;494:256–60.
Misbin RI, Green L, Stadel BV, Gueriguian JL, Gubbi A, Fleming GA. Lactic acidosis in patients with diabetes treated with metformin. N Engl J Med. 1998;338:265–6.
Asakawa M, Takano H, Nagai T, Uozumi H, Hasegawa H, Kubota N, et al. Peroxisome proliferator-activated receptor gamma plays a critical role in inhibition of cardiac hypertrophy in vitro and in vivo. Circulation. 2002;105:1240–6.
Rojas LB, Gomes MB. Metformin: an old but still the best treatment for type 2 diabetes. Diabetol Metab Syndr. 2013;5:6.
Zheng J, Woo SL, Hu X, Botchlett R, Chen L, Huo Y, et al. Metformin and metabolic diseases: a focus on hepatic aspects. Front Med. 2015;9:173–86.
Pharmacologic approaches to glycemic treatment. Diabetes Care. 2017;40:S64–S74.
Kennel WB, Hjortland M, Castelli WP. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol. 1974;34:29–34.
Kinsara AJ, Ismail YM. Metformin in heart failure patients. Indian Heart J. 2018;70:175–6.
Miyoshi T, Nakamura K, Yoshida M, Miura D, Oe H, Akagi S, et al. Effect of vildagliptin, a dipeptidyl peptidase 4 inhibitor, on cardiac hypertrophy induced by chronic beta-adrenergic stimulation in rats. Cardiovasc Diabetol. 2014;13:43.
Kawase H, Bando YK, Nishimura K, Aoyama M, Monji A, Murohara T. A dipeptidyl peptidase-4 inhibitor ameliorates hypertensive cardiac remodeling via angiotensin-II/sodium-proton pump exchanger-1 axis. J Mol Cell Cardiol. 2016;98:37–47.
Li L, Li S, Deng K, Liu J, Vandvik PO, Zhao P, Zhang L, Shen J, Bala MM, Sohani ZN, Wong E, Busse JW, Ebrahim S, Malaga G, Rios LP, Wang Y, Chen Q, Guyatt GH, Sun X. Dipeptidyl peptidase-4 inhibitors and risk of heart failure in type 2 diabetes: systematic review and meta-analysis of randomised and observational studies. BMJ. 2016;352:i610.
Ida S, Kaneko R, Murata K. Effects of oral antidiabetic drugs on left ventricular mass in patients with type 2 diabetes mellitus: a network meta-analysis. Cardiovasc Diabetol. 2018;17:129.
Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, Mattheus M, Devins T, Johansen OE, Woerle HJ, Broedl UC, Inzucchi SE, EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373:2117–28.
Mann JFE, Ørsted DD, Brown-Frandsen K, Marso SP, Poulter NR, Rasmussen S, Tornøe K, Zinman B, Buse JB, LEADER Steering Committee and Investigators. Liraglutide and renal outcomes in type 2 diabetes. N Engl J Med. 2017;377:839–48.
Stumvoll M, Nurjhan N, Perriello G, Dailey G, Gerich JE. Metabolic effects of metformin in non-insulin-dependent diabetes mellitus. N Engl J Med. 1995;333:550–4.
Malin SK, Nightingale J, Choi SE, Chipkin SR, Braun B. Metformin modifies the exercise training effects on risk factors for cardiovascular disease in impaired glucose tolerant adults. Obesity (Silver Spring). 2013;21:93–100.
Long-term safety, tolerability, and weight loss associated with metformin in the Diabetes Prevention Program Outcomes Study. Diabetes Care. 2012;35:731–7.
Malin SK, Kashyap SR. Effects of metformin on weight loss: potential mechanisms. Curr Opin Endocrinol Diabetes Obes. 2014;21:323–9.
Ejtahed HS, Tito RY, Siadat SD, Hasani-Ranjbar S, Hoseini-Tavassol Z, Rymenans L, et al. Metformin induces weight loss associated with gut microbiota alteration in non-diabetic obese women: a randomized double-blind clinical trial. Eur J Endocrinol. 2018.
Pascale A, Marchesi N, Govoni S, Coppola A, Gazzaruso C. The role of gut microbiota in obesity, diabetes mellitus, and effect of metformin: new insights into old diseases. Curr Opin Pharmacol. 2019;49:1–5.
Lipska KJ, Bailey CJ, Inzucchi SE. Use of metformin in the setting of mild-to-moderate renal insufficiency. Diabetes Care. 2011;34:1431–7.
Connolly V, Kesson CM. Metformin treatment in NIDDM patients with mild renal impairment. Postgrad Med J. 1996;72:352–4.
Feng Y, Wang S, Zhang Y, Xiao H. Metformin attenuates renal fibrosis in both AMPKalpha2-dependent and independent manners. Clin Exp Pharmacol Physiol. 2017;44:648–55.
Xu T, Brandmaier S, Messias AC, Herder C, Draisma HH, Demirkan A, et al. Effects of metformin on metabolite profiles and LDL cholesterol in patients with type 2 diabetes. Diabetes Care. 2015;38:1858–67.
van der Meer RW, Rijzewijk LJ, de Jong HW, Lamb HJ, Lubberink M, Romijn JA, Bax JJ, de Roos A, Kamp O, Paulus WJ, Heine RJ, Lammertsma AA, Smit JW, Diamant M. Pioglitazone improves cardiac function and alters myocardial substrate metabolism without affecting cardiac triglyceride accumulation and high-energy phosphate metabolism in patients with well-controlled type 2 diabetes mellitus. Circulation. 2009;119:2069–77.
Acknowledgements
The authors thank the other members, cooperators, and participants of the ABLE-MET study for their valuable contributions.
Author information
Authors and Affiliations
Consortia
Contributions
Conception and design: KO and KH; Analysis and interpretation of the data: KO, HW, NA, HI, KU, JF, AO, TH, MF, AS, and KH; Drafting of the article: KO and KH. Statistical expertise: KH; Collection and assembly of data: KO, HW, NA, HI, KU, JF, AO, TH, MF, AS, and KH. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics Approval and Consent to Participate
This study was approved by the institutional review board of each institute.
Consent for Publication
Not applicable.
Availability of Data and Material
The datasets used or analyzed during the current study are available from the corresponding author on reasonable request.
Conflict of interest
Koh Ono, Hiromichi Wada, Noriko Satoh-Asahara, Hitoki Inoue, Keita Uehara, Junichi Funada, Atsushi Ogo, Takahiro Horie, Masatoshi Fujita, Akira Shimatsu, and Koji Hasegawa have no conflicts of interest that are directly relevant to the content of this article.
Funding
This work was supported by Grants to KO and KH for a large-scale clinical study for the promotion of evidence-based medical practices by the National Hospital Organization.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Ono, K., Wada, H., Satoh-Asahara, N. et al. Effects of Metformin on Left Ventricular Size and Function in Hypertensive Patients with Type 2 Diabetes Mellitus: Results of a Randomized, Controlled, Multicenter, Phase IV Trial. Am J Cardiovasc Drugs 20, 283–293 (2020). https://doi.org/10.1007/s40256-019-00381-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40256-019-00381-1