
Abstract
The calcineurin inhibitor tacrolimus is an effective immunosuppressant and is extensively used in solid organ transplantation. In the first week after heart and lung transplantation, tacrolimus dosing is difficult due to considerable physiological changes because of clinical instability, and toxicity often occurs, even when tacrolimus concentrations are within the therapeutic range. The physiological and pharmacokinetic changes are outlined. Excessive variability in bioavailability may lead to higher interoccasion (dose-to-dose) variability than interindividual variability of pharmacokinetic parameters. Intravenous tacrolimus dosing may circumvent this high variability in bioavailability. Moreover, the interpretation of whole-blood concentrations is discussed. The unbound concentration is related to hematocrit, and changes in hematocrit may increase toxicity, even within the therapeutic range of whole-blood concentrations. Therefore, in clinically unstable patients with varying hematocrit, aiming at the lower therapeutic level is recommended and tacrolimus personalized dosing based on hematocrit-corrected whole-blood concentrations may be used to control the unbound tacrolimus plasma concentrations and subsequently reduce toxicity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
In the first week after thoracic organ transplantation, extreme interoccasion (dose-to-dose) variability in pharmacokinetic parameters is shown to be higher than interindividual variability and is mainly due to excessive variability in bioavailability. |
The whole-blood to unbound plasma concentration ratios differ with changes in hematocrit, and show saturation in the higher range of whole-blood tacrolimus concentrations, which may increase toxicity in these higher concentration ranges. |
Due to the complicated bioanalytical challenges, hematocrit-corrected whole-blood concentrations may be the most feasible and suitable surrogate for the prediction of clinical outcomes. |
1 Introduction
Tacrolimus has been considered the cornerstone of immunosuppressant regimens of solid organ transplantation since the late twentieth century. Early after thoracic organ transplantation, tacrolimus is difficult to dose because of considerable physiological changes due to clinical instability. We discuss the variability in tacrolimus pharmacokinetics due to these physiological changes, and the consequences for therapeutic monitoring and dosing.
2 Efficacy and Toxicity of Tacrolimus
Extensive research has demonstrated the efficacy of tacrolimus in solid organ transplantation [1,2,3]. For instance, acute rejection rates after 6 months (biopsy-proven acute rejection [BPAR] grade 3A or higher) were shown to be significantly lower for tacrolimus (28%) than cyclosporine A (42%) [4].
Although tacrolimus is known to be effective, heart and lung transplantation patients often show signs of toxicity and rejection [5,6,7,8]. Toxicity and rejection both have major consequences for the outcome of heart and lung transplantation, with a higher risk for morbidity and mortality [5, 9,10,11].
Acute kidney injury often evolves into chronic kidney disease and appears in approximately half of the patients during the first weeks after thoracic organ transplantation [5, 6]. The occurrence of acute kidney injury has been associated with supratherapeutic (> 15 ng/mL) whole-blood tacrolimus trough concentrations in the first week after thoracic organ transplantation [7, 8], and an increasing tacrolimus concentration has been associated with higher AKI risk and severity [12]. Furthermore, a higher rejection rate has been associated with a high variability in whole-blood concentrations after heart and lung transplantation [13, 14]. Therefore, it is of the utmost importance to prevent supratherapeutic whole-blood concentrations and to reduce the variability in tacrolimus concentrations.
3 Variability in Tacrolimus Pharmacokinetics Early After Heart and Lung Transplantation
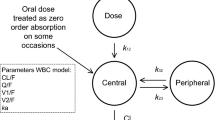
In the first days after transplantation, heart and lung recipients frequently show a high variability in tacrolimus blood concentrations due to clinical instability caused by shock and systemic inflammation (see Fig. 1 for a schematic overview of tacrolimus pharmacokinetics for the effect of physiological changes) [15]. The systemic inflammation resulting in organ dysfunction is due to the surgical procedure with the application of (extended) extracorporeal circulation, as well as ischemia–reperfusion injury of the transplanted organ(s) and bleeding with blood transfusions [15]. Clinical instability causes a cascade of processes influencing all these aspects of tacrolimus pharmacokinetics. For instance, gut dysmotility may highly influence absorption of tacrolimus that is already limited in stable patients, with an estimated bioavailability of around 25% [16,17,18].

Schematic overview of tacrolimus pharmacokinetics: gut transport, absorption, blood distribution, hepatic metabolism, and excretion of tacrolimus. CYP cytochrome P450, OATP1 organic anion–transporting peptide, ABCB1 efflux pump of the ABCB1 cassette, RBC red blood cells
Tacrolimus is generally administered orally. Inflammation may result in reduced blood flow and ileus, reducing bioavailability by delaying transport, minimizing luminal degradation and dissolution, and decreasing contact with the gut wall [19]. On the opposite, increased blood flow increases gut motility, shortening transit time and increasing degradation and dissolution of tacrolimus. A sudden peak in the blood concentrations may occur.
In the enterocyte, cytochrome P450 (CYP) 3A4/5 are the main enzymes metabolizing tacrolimus [12, 20, 21]. Tacrolimus is repeatedly taken up and pumped out of the enterocytes into the gut lumen by the transporter ATP-binding cassette B1 (ABCB1), increasing the probability of tacrolimus being metabolized [20]. Shock and inflammation decrease the activity of the CYP3A4/5 enzymes and the ABCB1 transporter [22]. Saturation of the CYP3A4/5 enzymes may occur, facilitating tacrolimus transport into the blood and resulting in higher uptake into the blood compartment [22]. Miano et al. showed that CYP3A5 and CYP3A4*22 are of relevance for the concentration:dose (C/D) ratio in the early phase after lung transplantation. Nevertheless, only a small part of the C/D ratio is determined by CYP enzyme activity in the first week [12]. Initially after lung transplantation, CYP enzyme activity may also be influenced by hypoxemia and drug–drug interactions, which are not dependent on the intrinsic enzyme activity [15]. For instance, corticosteroids induce CYP3A enzymes and the ABCB1 transporter [23, 24]. Corticosteroids are administered in high doses in the first days after transplantation and tapered thereafter, increasing tacrolimus absorption. In the blood, tacrolimus distributes mainly into erythrocytes and, to a lesser extent, to (lipo)proteins (albumin, high-density lipoprotein, and α1-acid glycoprotein) [25]. Inflammation, blood loss, and blood transfusions may increase unbound concentrations by anemia and hypoalbuminemia. Furthermore, extracorporeal life support may increase blood volume, decrease protein concentrations, and cause hemolysis and sequestration of tacrolimus into the equipment. Until now, only one study on tacrolimus pharmacokinetics in combination with extracorporeal life support has been executed [26]. This was an ex vivo study with a pediatric extracorporeal circulation, and the researchers found that tacrolimus concentrations lowered by approximately 16%, which was not as much as expected on lipophilicity alone and may be due to the extensive erythrocyte binding. These unfavorable clinical conditions alter the pharmacokinetics and induce large variations in tacrolimus concentrations.
3.1 Interoccasion Variability in Tacrolimus Pharmacokinetics
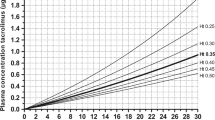
Whole-blood tacrolimus concentrations at 12 h post-administration (C12h) highly vary after heart and lung transplantation, and this extremely high dose-to-dose variability persists in the first week post-transplantation [27]. The study by Sikma et al. showed further that the majority of C12h, almost 70%, were out of the target range (9–15 ng/mL). Half of the patients displayed subtherapeutic concentrations and approximately 20% of patients displayed supratherapeutic concentrations [28]. Moreover, the interoccasion (dose-to-dose) variability in pharmacokinetics was extreme and exceeded the interpatient variability [29]. Personalizing the dose based on C12h seems to be virtually impossible in clinically unstable thoracic organ recipients. Moreover, Bayesian forecasting that may improve tacrolimus dosing in clinically stable patients may be difficult in clinically unstable thoracic organ recipients [30]. However, this does not mean that tacrolimus monitoring is redundant; it should still be used to prevent toxicity.
The interoccasion variability was mainly caused due to a substantial variability in relative bioavailability in patients exhibiting clinical instability. Extremely slow (time to reach maximum concentration [Tmax > 8 h]) and extremely rapid (Tmax < 30 min) absorption was observed. The variability in this bioavailability (55%) far exceeded the variability of other pharmacokinetic parameters, such as clearance (35%), indicating highly variable absorption of tacrolimus [29]. The situation totally differs from that of kidney transplant recipients early after transplantation, in whom bioavailability has been shown to be dose-dependent, and with a much smaller interoccasion variability of approximately 25% [17, 18]. To circumvent this high variability in bioavailability, intravenous administration may be preferred over oral administration early post-transplantation. Applying tacrolimus intravenously may improve tacrolimus dosing despite the higher costs and risk of additional nephrotoxicity of the solvent HCO-60 [15, 31, 32].
3.2 Interpretation of Whole-Blood Tacrolimus Concentrations Early After Heart and Lung Transplantation
One may even wonder whether the whole-blood tacrolimus concentration is an adequate predictor of clinical outcomes in the early post-transplant phase. Although acute kidney injury seems to be associated with supratherapeutic whole-blood concentrations, the relation between tacrolimus whole-blood exposure and the development of nephrotoxicity is poor. Even within the therapeutic whole-blood concentration range, tacrolimus-associated nephrotoxicity arises [2, 3]. Whether monitoring of intracellular tacrolimus concentrations and calcineurin activity is better related to outcome than whole-blood concentrations is still unclear due to the lack of a standardized and validated analysis [33,34,35,36,37]; however, in current clinical transplantation practices, whole-blood tacrolimus concentrations are used for therapeutic drug monitoring. Moreover, where toxicity is concerned, the unbound tacrolimus plasma concentrations or hematocrit-corrected tacrolimus is of importance, but more research is warranted [25].
Tacrolimus is particularly distributed into erythrocytes, next to being associated with (lipo)proteins (see Fig. 2) [38, 39]. Within the erythrocytes, tacrolimus is known to be highly associated with the FK-binding protein [40,41,42,43]. In the clinically unstable transplant patient, erythrocyte counts may highly fluctuate due to bleeding, red blood cell transfusions, dilution, bone marrow depression, and hemolysis due to extracorporeal equipment. This has large consequences with regard to the interpretation of the whole-blood concentrations, e.g. a decrease in red blood cells decreases whole-blood concentrations, although not necessarily the unbound concentrations. To correct for these low whole-blood tacrolimus concentrations, transplant physicians may be enticed to raise the dose; however, raising the dose may lead to higher unbound concentrations, posing the patient at a higher risk of toxicity, while decreasing, or at least not increasing the dose might be more appropriate based on the unbound concentration. Moreover, a 12-h whole-blood concentration above 15 ng/mL necessitates lowering or discontinuing the dose until concentrations fall below this level. Aiming for the lower therapeutic range value in the early phase after transplantation may decrease the unbound concentration, hence the risk for toxicity. For instance, a 9 ng/mL concentration could be targeted when the therapeutic whole-blood range is 9–15 ng/mL.

A theoretical representation of a decrease in erythrocyte and albumin concentrations resulting in changes in whole-blood, total plasma, and unbound tacrolimus concentrations. a Hematocrit and albumin in normal ranges. b Decreased erythrocyte count with a decrease in whole-blood concentration and an increase in unbound concentration. A decrease in albumin concentration may increase the unbound plasma concentration to a lesser extent
3.3 Hematocrit-Corrected Tacrolimus Dosing
Although the unbound concentration is known to be related to hematocrit, studies investigating the unbound tacrolimus plasma concentrations are scarce because quantification of unbound tacrolimus concentrations is bioanalytically challenging, costly, and time-consuming [44]; however, the accuracy and precision of plasma concentration quantification is vulnerable to hemolysis of the whole-blood sample. As such, the relationship between whole-blood and unbound concentrations has not systematically been studied and no pharmacokinetic models are currently available to predict the unbound concentrations based on whole-blood concentrations. Moreover, a therapeutic range of unbound tacrolimus plasma concentrations is lacking for routine therapeutic drug monitoring [38, 44,45,46].
Because of the large influence of hematocrit on whole-blood concentrations, hematocrit-corrected whole-blood concentrations may be suitable as a substitute for the prediction of clinical outcomes. Two studies showed that for clinically stable renal transplants, hematocrit standardized whole-blood concentrations improved the prediction of whole-blood concentrations [18, 47]. Størset assumed that when hematocrit increases, the unbound concentration remains similar, which may be an incorrect assumption in patients with lower hematocrit fractions [18]. The relationship between whole-blood and plasma tacrolimus concentrations has shown to be non-linear [48]; therefore, hematocrit-corrected tacrolimus dosing could be more appropriate. No validation studies on hematocrit-corrected whole-blood concentrations versus measured unbound or total plasma concentrations are currently available. In clinically unstable patients with varying hematocrit, tacrolimus personalized dosing based on hematocrit-corrected whole-blood concentrations may be used to control the unbound tacrolimus plasma concentration and subsequently reduce toxicity. Therapeutic drug monitoring based on hematocrit-corrected whole-blood concentrations may be directly implemented in daily practice and may improve tacrolimus dosing in clinically unstable thoracic organ recipients in order to reduce toxicity and rejection.
4 Conclusions
Tacrolimus pharmacokinetics differ between clinically stable and clinically unstable patients, such as thoracic organ recipients. This results in higher rates of tacrolimus nephrotoxicity in these latter patients. In unstable thoracic organ recipients, a large interoccasion variability in relative bioavailability makes pharmacokinetic-guided dosing of orally administered tacrolimus of limited added value. Within the blood compartment, erythrocyte concentrations appear to be an important factor to consider as tacrolimus is mainly associated with these cells. In clinically unstable thoracic organ transplant patients, erythrocyte concentrations are highly variable, subsequently changing the unbound tacrolimus concentrations. To improve tacrolimus personalized dosing in the future, we recommend administering tacrolimus intravenously and aiming at the lower therapeutic range value in the first days after transplantation. Monitoring hematocrit-corrected whole-blood concentrations may further improve tacrolimus dosing.
References
Atalan HK, Gucyetmez B, Aslan S, Yazar S, Polat KY. Postoperative acute kidney injury in living donor liver transplantation recipients. Int J Artif Organs. 2017;41:37–42.
Rayar M, Tron C, Jézéquel C, Beaurepaire J-M, Petitcollin A, Houssel-Debry P, et al. High intrapatient variability of tacrolimus exposure in the early period after liver transplantation is associated with poorer outcomes. Transplantation. 2018;102:e108–14.
Nankivell BJ, Png CH, Oconnell PJ, Chapman JR. Calcineurin inhibitor nephrotoxicity through the lens of longitudinal histology: comparison of cyclosporine and tacrolimus eras. Transplantation. 2016;100:1723–31.
Grimm M, Rinaldi M, Yonan NA, Arpesella G, Arizón Del Prado JM, Pulpón LA, et al. Superior prevention of acute rejection by tacrolimus vs. cyclosporine in heart transplant recipients—a large European trial. Am J Transplant. 2006;6:1387–97.
Wehbe E, Duncan AE, Dar G, Budev M, Stephany B. Recovery from AKI and short- and long-term outcomes after lung transplatation. Clin J Am Soc Nephrol. 2013;8:19–25.
Tjahjono R, Connellan M, Granger E. Predictors of acute kidney injury in cardiac transplantation. Transpl Proc. 2016;48:167–72.
Sikma MA, Hunault CC, van de Graaf EA, Verhaar MC, Kesecioglu J, de Lange DW, et al. High tacrolimus blood concentrations early after lung transplantation and the risk of kidney injury. Eur J Clin Pharmacol. 2017;73:573–80.
Sikma MA, Hunault CC, Kirkels JH, Verhaar MC, Kesecioglu J, de Lange DW. Association of whole blood tacrolimus concentrations with kidney injury in heart transplantation patients. Eur J Drug Metabol Pharmacokinet. 2018;43:311–20.
Paradela de la Morena M, La Torre Bravos De M, Prado RF, Delgado Roel M, García Salcedo JA, Fieira Costa E, et al. Chronic Kidney Disease After Lung Transplantation: Incidence, Risk Factors, and Treatment. Transplant Proc. 2010;42:3217–9.
Ojo AO, Held PJ, Port FK, Wolfe RA, Leichtman AB, Young EW, et al. Chronic renal failure after transplantation of a nonrenal organ. N Engl J Med. 2003;349:931–40.
Mastrobuoni S, Ubilla M, Cordero A, Herreros J, Rabago G. Two-dose daclizumab, tacrolimus, mycophenolate mofetil, and steroid-free regimen in de novo cardiac transplant recipients: early experience. Transpl Proc. 2007;39:2163–6.
Miano TA, Flesch JD, Feng R, Forker CM, Brown M, Oyster M, et al. Early tacrolimus concentrations after lung transplant are predicted by combined clinical and genetic factors and associated with acute kidney injury. Clin Pharmacol Ther. 2019. https://doi.org/10.1002/cpt.1629.
Gueta I, Markovits N, Yarden-Bilavsky H, Raichlin E, Freimark D, Lavee J, et al. High tacrolimus trough level variability is associated with rejections after heart transplant. Am J Transplant. 2018;18:2571–8.
Gallagher HM, Sarwar G, Tse T, Sladden TM, Hii E, Yerkovich ST, et al. Erratic tacrolimus exposure, assessed using the standard deviation of trough blood levels, predicts chronic lung allograft dysfunction and survival. J Heart Lung Transplant. 2015;34:1442–8.
Sikma MA, van Maarseveen EM, van de Graaf EA, Kirkels JH, Verhaar MC, Donker DW, et al. Pharmacokinetics and toxicity of tacrolimus early after heart and lung transplantation. Am J Transplant. 2015;15:2301–13.
Sikma MA, van Maarseveen EM, Donker DW, Meulenbelt J. Letter to the editor: “Immunosuppressive drug therapy—biopharmaceutical challenges and remedies”. Expert Opin Drug Deliv. 2015;12:1955–7.
Ekberg H, Mamelok RD, Pearson TC, Vincenti F, Tedesco-Silva H, Daloze P. The challenge of achieving target drug concentrations in clinical trials: experience from the symphony study. Transplantation. 2009;87:1360–6.
Størset E, Holford N, Hennig S, Bergmann TK, Bergan S, Bremer S, et al. Improved prediction of tacrolimus concentrations early after kidney transplantation using theory-based pharmacokinetic modelling. Br J Clin Pharmacol. 2014;78:509–23.
Mittal N, Thompson JF, Kato T, Tzakis AG. Tacrolimus and diarrhea: pathogenesis of altered metabolism. Pediatr Transplant. 2001;5:75–9.
Christians U, Schmitz V, Haschke M. Functional interactions between P-glycoprotein and CYP3A in drug metabolism. Expert Opin Drug Metab Toxicol. 2005;1:641–54.
Díaz-Molina B, Tavira B, Lambert JL, Bernardo MJ, Alvarez V, Coto E. Effect of CYP3A5, CYP3A4, and ABCB1 genotypes as determinants of tacrolimus dose and clinical outcomes after heart transplantation. Transpl Proc. 2012;44:2635–8.
Renton KW. Regulation of drug metabolism and disposition during inflammation and infection. Expert Opin Drug Metab Toxicol. 2005;1:629–40.
Lam S, Partovi N, Ting LSL, Ensom MHH. Corticosteroid interactions with cyclosporine, tacrolimus, mycophenolate, and sirolimus: fact or fiction? Ann Pharmacother. 2008;42:1037–47.
Christians U, Jacobsen W, Benet LZ, Lampen A. Mechanisms of clinically relevant drug interactions associated with tacrolimus. Clin Pharmacokinet. 2002;41:813–51.
Zahir H, McCaughan G, Gleeson M, Nand RA, McLachlan AJ. Changes in tacrolimus distribution in blood and plasma protein binding following liver transplantation. Ther Drug Monit. 2004;26:506–15.
Heith CS, Hansen LA, Bakken RM, Ritter SL, Long BR, Hume JR, et al. Effects of an ex vivo pediatric extracorporeal membrane oxygenation circuit on the sequestration of mycophenolate mofetil, tacrolimus, hydromorphone, and fentanyl. J Pediatr Pharmacol Ther. 2019;24:290–5.
Sikma MA, Hunault CC, van Maarseveen EM, Huitema ADR, van de Graaf EA, Kirkels JH, et al. Extreme variability of oral tacrolimus pharmacokinetics early after thoracic organ transplantation due to excessive fluctuations in bioavailability (NTR 3912). 15th International Congress of Therapeutic Drug Monitoring and Clinical Toxicology; 24–27 September 2017: Kyoto.
Sikma MA, Hunault CC, Van Maarseveen EM, Huitema ADR, Van de Graaf EA, Kirkels JH, et al. High variability of whole-blood tacrolimus pharmacokinetics early after thoracic organ transplantation. Eur J Drug Metab Pharmacokinet (2019). https://doi.org/10.1007/s13318-019-00591-7.
Sikma MA, Hunault CC, Huitema ADR, Verhaar MC, van de Graaf EA, Kirkels JH, et al. Tacrolimus whole blood and unbound plasma concentrations early after heart and lung transplantation (NTR3912). 16th International Congress of Therapeutic Drug Monitoring and Clinical Toxicology. 16–19 September 2018: Brisbane.
Størset E, Holford N, Midtvedt K, Bremer S, Bergan S, Åsberg A. Importance of hematocrit for a tacrolimus target concentration strategy. Eur J Clin Pharmacol. 2014;70:65–77.
Snell GI, Ivulich S, Mitchell L, Westall GP, Levvey BJ. Evolution to twice daily bolus intravenous tacrolimus: optimizing efficacy and safety of calcineurin inhibitor delivery early post lung transplant. Ann Transplant. 2013;18:399–407.
Worbs S, Köhler K, Pauly D, Avondet M-A, Schaer M, Dorner MB, et al. Ricinus communis intoxications in human and veterinary medicine-a summary of real cases. Toxins (Basel). 2011;3:1332–72.
Capron A, Lerut J, Latinne D, Rahier J, Haufroid V, Wallemacq P. Correlation of tacrolimus levels in peripheral blood mononuclear cells with histological staging of rejection after liver transplantation: preliminary results of a prospective study. Transpl Int. 2011;25:41–7.
Lemaitre F, Blanchet B, Latournerie M, Antignac M, Houssel-Debry P, Verdier M-C, et al. Pharmacokinetics and pharmacodynamics of tacrolimus in liver transplant recipients: inside the white blood cells. Clin Biochem. 2015;48:406–11.
Pensi D, De Nicolò A, Pinon M, Calvo PL, Nonnato A, Brunati A, et al. An UPLC-MS/MS method coupled with automated on-line SPE for quantification of tacrolimus in peripheral blood mononuclear cells. J Pharm Biomed Anal. 2015;107:512–7.
Tron C, Allard M, Petitcollin A, Ferrand-Sorre M-J, Verdier M-C, Querzerho-Raguideau J, et al. Tacrolimus diffusion across the peripheral mononuclear blood cell membrane: impact of drug transporters. Fundam Clin Pharmacol. 2019;33:113–21.
Brunet M, Van Gelder T, Åsberg A, Haufroid V, Hesselink DA, Langman L, et al. Therapeutic drug monitoring of tacrolimus-personalized therapy: second consensus report. Ther Drug Monit. 2019;41:261–307.
Zahir H, McCaughan G, Gleeson M, Nand RA, McLachlan AJ. Factors affecting variability in distribution of tacrolimus in liver transplant recipients. Br J Clin Pharmacol. 2004;57:298–309.
Rifai N, Chao F-F, Pham Q, Thiessen J, Soldin SJ. The role of lipoproteins in the transport and uptake of cyclosporine and dihydro-tacrolimus into HepG2 and JURKAT cell lines. Clin Biochem. 1996;29:149–55.
Biagiotti S, Paoletti MF, Fraternale A, Rossi L, Magnani M. Drug delivery by red blood cells. IUBMB Life. 2011;63:621–31.
Biagiotti S, Rossi L, Bianchi M, Giacomini E, Pierigè F, Serafini G, et al. Immunophilin-loaded erythrocytes as a new delivery strategy for immunosuppressive drugs. J Control Release. 2011;154:306–13.
Nagase K, Iwasaki K, Nozaki K, Noda K. Distribution and protein binding of FK506, a potent immunosuppressive macrolide lactone, in human blood and its uptake by erythrocytes. J Pharm Pharmacol. 1994;46:113–7.
Walensky LD, Gascard P, Fields ME, Blackshaw S, Conboy JG, Mohandas N, et al. The 13-kD FK506 binding protein, FKBP13, interacts with a novel homologue of the erythrocyte membrane cytoskeletal protein 4.1. J Cell Biol. 1998;141:143–53.
Zahir H, Nand RA, Brown KF, Tattam BN. Validation of methods to study the distribution and protein binding of tacrolimus in human blood. J Pharmacol Toxicol Methods. 2001;46:27–35.
Zheng S, Davis CL, Hebert MF. Pharmacokinetics of tacrolimus during pregnancy. Ther Drug Monit. 2012;34:660–70.
Bittersohl H, Schniedewind B, Christians U, Luppa PB. A simple and highly sensitive on-line column extraction liquid chromatography-tandem mass spectrometry method for the determination of protein-unbound tacrolimus in human plasma samples. J Chromatogr A. 2018;1547:45–52.
Schijvens AM, van Hesteren FHS, Cornelissen EAM, Bootsma-Robroeks CMHHT, Brüggemann RJM, Burger DM, et al. The potential impact of hematocrit correction on evaluation of tacrolimus target exposure in pediatric kidney transplant patients. Pediatr Nephrol. 2018;34:507–515.
Jusko WJ, D’Ambrosio R. Monitoring FK 506 concentrations in plasma and whole blood. Transplant Proc. 1991;23:2732–5.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Maaike A. Sikma, Claudine C. Hunault, Alwin D.R. Huitema, Dylan W. de Lange, and Erik M. van Maarseveen declare no conflicts of interest or financial support.
Funding
No funding was received for this work.
Additional information
Invited proposal CPKA-D-18-00212.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Sikma, M.A., Hunault, C.C., Huitema, A.D.R. et al. Clinical Pharmacokinetics and Impact of Hematocrit on Monitoring and Dosing of Tacrolimus Early After Heart and Lung Transplantation. Clin Pharmacokinet 59, 403–408 (2020). https://doi.org/10.1007/s40262-019-00846-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40262-019-00846-1