
Abstract
Background
Female athletes are four to six times more likely to sustain an anterior cruciate ligament (ACL) injury than male athletes. Jump-landing biomechanics are influenced by maturation, with post-pubertal female athletes at a heightened risk of ACL injuries.
Objective
The aim of our systematic review was to identify and summarise the current evidence regarding the changes in kinematic and kinetic risk factors associated with ACL injuries during jump-landing tasks in female athletes at various stages of maturity.
Methods
A systematic search was conducted in PubMed, CINAHL, Web of Science, SPORTDiscus, EMBASE and Scopus. Articles were included if they: (1) conducted the research on uninjured female athletes with no restriction on playing level/experience; (2) provided information regarding the stage of the maturity and the scale used for estimating the maturity status of the participants; and (3) reported a biomechanical risk factor associated with ACL injuries during jump-landing tasks across at least two different maturity groups (e.g. pre-pubertal vs post-pubertal).
Results
Sixteen articles involving 2323 female athletes were included in our review. A total of 12 kinematic and 8 kinetic variables were identified across these studies. Of the 12 kinematic variables reported in our review, we found strong evidence for higher peak knee abduction angle in post-pubertal female individuals compared with pre-pubertal girls (p < 0.05). With regard to the 8 kinetic variables, we found strong evidence for lower relative peak vertical ground reaction force, higher external knee abduction moment and internal rotation moment in post-pubertal compared with pre-pubertal athletes. The strength of evidence for the remaining kinematic and kinetic variables ranged from conflicting to moderate and, in some instances, could not be determined.
Conclusions
Our study provides an overview of the changes in biomechanical risk factors in female athletes during jump-landing tasks at various stages of maturity. We found moderate-to-limited evidence for most kinematic and kinetic variables, highlighting the need for further research.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
There was strong evidence for post-pubertal female athletes to have higher peak knee abduction angle compared with pre-pubertal athletes. |
There was strong evidence for post-pubertal athletes to have higher peak external knee abduction moment and internal rotation moment compared with pre-pubertal athletes. |
There was strong evidence for pre-pubertal athletes to have higher relative vertical ground reaction force compared with post-pubertal athletes. |
It is recommended that future research should explore the changes in jump-landing biomechanics across hip and ankle joints in addition to the knee joint across various maturity levels in female athletes. |
1 Introduction
Anterior cruciate ligament (ACL) injuries have been traditionally considered to be of limited concern in skeletally immature athletes based on the relative low incidence [1]. However, more recent research findings have shown trends of an increased incidence in ACL injury rates in this population. For example, in Australia, the rate of ACL injuries in children aged between 5 and 14 years increased by 148% between 2005 and 2015 [2]. In Italy, the overall percentage of ACL reconstruction surgeries in children aged younger than 15 years has increased from 0.13 to 0.95% between 2001 and 2015, with 97.3% of these surgeries being performed on children aged 10–14 years [3]. Apart from the financial burden associated with ACL injuries, there is an increased risk of longer term health issues. Athletes with prior knee injuries have been reported to have negative health-related outcomes including knee-related pain, poor quality of life and a higher body mass index [4]. Further, some youth who have an ACL injury experience an early onset of osteoarthritis within 15 years of the injury [5,6,7]. In young athletes, the risk of secondary ACL injury has been reported to be as high as 25–35% [8,9,10] within 2–5 years of the first injury, underlining the importance of early risk mitigation.
Anterior cruciate ligament injuries commonly occur during the deceleration phase of dynamic movements such as single-leg (SL) or double-leg jump-landing [11,12,13]. The majority of ACL injuries during these movements occur in non-contact scenarios [14], and are usually a consequence of poor multiplanar biomechanics [14]. Reduced knee flexion angle, greater knee abduction angle and moments and peak vertical ground reaction force (vGRF) during jump-landing tasks are biomechanical factors associated with an increased risk of sustaining a non-contact ACL injury [15]. A prospective biomechanical and epidemiological investigation showed that adolescent female athletes that sustained ACL injuries demonstrated a knee abduction angle that was 8° greater at initial contact (IC) during a jump-landing task as compared with their uninjured peers [15]. The female athletes who went on to sustain a ACL injury also landed with a 2.5 times higher peak knee abduction moment and 20% greater ground reaction forces prior to injury compared with uninjured teammates [15]. Despite research being conducted in this domain for over two decades, the findings are still inconclusive as the aforementioned variables have only shown associations with ACL injury and as such cannot be considered as an ACL injury risk factor, [16, 17]. Recent literature highlighted that more high-quality research studies (i.e. prospective studies, level 1 evidence) related to biomechanical risk factors for non-contact ACL injuries need to be conducted as the majority of existing evidence comes from lower quality studies (i.e. retrospective, level 2 evidence) or associative study designs (i.e. level 3) [16]. Further, the biomechanics and the forces acting on the knee joint can be altered by the motion occurring across the hip and ankle joint [18]; however, few studies have reported kinematic and kinetic variables across all three joints [16, 17, 19]. Therefore, further exploring the biomechanical risk factors during jump-landing tasks across various planes of motion at the hip, knee and ankle joints will help to better understand the contributing risk factors to ACL injuries.
The literature suggests that changes in anatomy [20], joint biomechanics [21], hormones [22, 23] and neuromuscular control [24, 25] during the adolescent growth spurt could potentially influence the rates of ACL injuries. This is a period when the long bones (tibia and femur) grow at a rapid rate resulting in increased stature [26]. The pubertal growth spurt leads to longer levers, which translate into greater potential for increased torques on the knee joint [21]. Further, the increased limb length leads to a higher centre of mass, which makes muscular control of body position more challenging [27]. In addition, the ability to balance and dampen forces during high-velocity movements (such as jump-landing tasks) becomes more difficult and therefore injury risk is heightened [21]. As female individuals transition though the various stages of adolescence and reach the latter stages of maturity, they typically land with less knee flexion and higher ground reaction forces and external knee moments, thus putting them at a higher risk of sustaining an ACL injury [28]. The absence of sufficient neuromuscular control to stabilise the knee while performing activities involving large forces and torques might partly explain the increased incidence of ACL injuries in post-pubertal female individuals compared with prepubertal and pubertal female athletes [15, 25]. Hence, identifying the magnitude of variation in biomechanical risk factors during jump-landing tasks relative to maturational development might help to understand if these risk factors are present during the childhood years or are exacerbated as a result of growth and maturation in female athletes.
To date, the literature is limited to isolated investigations without any syntheses that provide comprehensive conclusions related to the influences of maturation on multi-joint landing mechanisms in female athletes. Therefore, the primary objective of our systematic review was to identify and summarise the current scientific evidence regarding the changes in kinetic and kinematic risk factors associated with ACL injuries during jump-landing tasks in female athletes at various stages of maturity.
2 Methods
This review was conducted in accordance with Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) [29]. A review protocol was not pre-registered for this review. This systematic review focused on providing a comprehensive summary regarding the changes in biomechanical variables across various maturity groups during jump-landing tasks in female athletes.
2.1 Eligibility Criteria
The inclusion criteria were based on the population, intervention, comparator, outcome and study design (PICOS) concept as follows, whereby studies needed to: (1) conduct the research on uninjured female athletes with no restriction on playing level/experience; (2) provide information regarding the stage of maturity and the scale used for estimating the maturity status of the participants; and (3) report a kinematic (e.g. joint angles at various instances such as IC, peak values, range of motion/displacement) and/or kinetic variables (e.g. absolute or relative forces, absolute or relative moments) during jump-landing tasks across at least two different maturity groups (e.g. prepubertal vs post-pubertal; pubertal vs post-pubertal).
The exclusion criteria for the review were as follows: (1) studies that did not report the maturity status of the participants; (2) studies that did not include female athletes; (3) studies that reported biomechanical variables during non-jump-landing tasks, such as side-stepping and cutting; (4) studies in which no biomechanical variables were reported during jump-landing tasks; (5) studies that reported results based on simulation models; (6) book chapters, reviews, systematic reviews and meta-analyses, conference proceedings, poster presentations, conference abstracts, reviews, clinical commentaries, theses and dissertations; and (7) articles not published in English.
2.2 Information Sources and Search Strategy
A systematic literature search was conducted across the following scientific databases to identify original research articles published from inception to July 2022 and then updated in May 2023: PubMed, CINAHL, Web of Science, SPORTDiscus, EMBASE and Scopus. The Boolean operator ‘AND’ and ‘OR’ were used to combine the various search terms. The complete search strategy across the different databases has been provided in Appendix S1 of the Electronic Supplementary Material (ESM). The reference lists of the included studies were also screened by one author (AKR) to identify any additional studies that were relevant for this review.
2.3 Selection Process
One author (AKR) carried out the search across all the relevant databases. Potential titles and abstracts were imported into Endnote (Version 20; Clarivate, Philadelphia, PA, USA) and the duplicate articles were removed. The articles were then screened according to the inclusion/exclusion criteria. A three-stage process was followed to identify the relevant articles. First, articles were included in the first stage if they had investigated biomechanics related to ACL injuries, and jump-landing tasks. Second, the abstract of each study was then screened and the studies that did not report findings on female participants were excluded. The third and final stage involved reviewing the full text of all relevant studies that satisfied the eligibility criteria to scrutinise their suitability for final inclusion. Two authors (AKR and RSL) independently performed all these tasks. All potential discrepancies regarding the inclusion/exclusion of studies were discussed between the two authors and resolved. Another member of the authorship team (JLO) was identified to consult in the event that any discrepancies could not be resolved.
2.4 Data Extraction and Reduction
The following data were extracted from the included articles: (1) author name, year of publication; (2) age, stature, mass and maturity status of the participants; (3) sporting activity and level; (4) various jump-landing tests that were used; (5) mode of data collection; (6) measurement units; (7) kinematic and kinetic data that were analysed; and (8) mean and standard deviation for each of the biomechanical risk factors across the various maturity groups.
When the data were reported in a graphical format, WebPlotDigitiser (https://automeris.io/WebPlotDigitizer/) was used to derive the numerical data. This procedure has proven to be valid (r = 0.99, p < 0.001) in previous studies [30]. In cases where studies had reported 95% confidence intervals, the recommended formula presented in the Cochrane handbook [31] was used for obtaining the standard deviation values:
In cases where the standard error was reported, the following formula was used to convert it to a standard deviation, where N is the sample of the respective group (pre-pubertal, pubertal or post-pubertal):
With regard to the kinetic variables, absolute joint moments were normalised using various techniques such as dividing moments by body weight [BW] (Nm/kg), BW times height (dimensionless) or BW times leg length (Nm/m), with the methods being inconsistent among researchers [32]. When a study reported values using different normalising techniques, moments normalised to BW (Nm/kg) were included in our review as this is the most commonly used technique used to report kinetic findings in biomechanical research [32].
2.5 Quality Assessment of Included Studies
Two authors (AKR and RSL) independently carried out the quality assessment of the included studies. The Downs and Black checklist [33] was used for the methodological quality assessment of the included studies (ESM). The original checklist consists of 27 items that address methodological components, including external validity, internal validity (bias and confounding variables) and power. The quality index of the checklist has been reported to have a high criterion validity (r = 0.90), high internal consistency (KR-20 = 0.89), test–retest (r = 0.88) and inter-rater (r = 0.75) reliability. However, we used the modified version of this checklist consisting of 17 items [34], which has been used previously in research because of the subjectivity in interpretation of the original questions. The question for power was modified from a scale of 0–5 to a binary scale, in which all questions were given a score of 0 (no) or 1 (yes). However, question 20 was given a score of 0 (no), 1 (partial) or 2 (yes); a score of 2 was given when the study had reported the accuracy and described the methods clearly, while 1 point was given when only the methods were described. These modifications resulted in a total critical appraisal score of 18 points for the assessment of the included studies. The points obtained using the Downs and Black rating scale were converted to a percentage score, with studies classified as high (≥ 71%), moderate (51–70%) or poor (≤ 50%) quality [35]. In cases of disagreement, a consensus was reached in consultation with a third author (JLO).
2.6 Strength of Evidence Synthesis
To determine the strength of evidence of a biomechanical risk factor associated with ACL injuries across various maturity stages in female athletes, the classification system proposed by van Tulder et al. [36] was used:
Strong evidence Consistent findings across a minimum of two high-quality studies.
Moderate evidence Consistent findings across multiple studies of including at least one high-quality study.
Limited evidence One high-quality or multiple moderate-quality or low-quality studies.
Very limited One moderate-quality or low-quality study.
Conflicting evidence Inconsistent findings across multiple studies.
The findings were rated as consistent and inconsistent when ≥ 75 or < 75% of the studies reported consistent directionality in the findings, respectively [37]. All studies that reported a particular kinematic or kinetic factor were considered in determining the consistency of the findings, irrespective of the study quality. The directionality of the findings was based on the mean values for each biomechanical variable reported across various stages of maturity irrespective of the level of significance (p < 0.05).
3 Results
3.1 Search Results and Selection
The electronic database and manual search yielded 6290 articles, from which a total of 2743 articles remained after the removal of duplicate studies and 2624 articles were then excluded based on title and abstract screening. Subsequently, a total of 119 full-text articles were screened from which 16 studies [21, 24, 25, 27, 38,39,40,41,42,43,44,45,46,47,48,49] met full inclusion criteria in our review. The complete search strategy has been detailed in Fig. 1.

Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) flowchart describing the study selection process. ACL anterior cruciate ligament
3.2 Study Characteristics
In total, 2323 (623 pre-pubertal, 745 pubertal and 955 post-pubertal) female athletes were included in our review. Two studies had classified participants according to their maturity level but did not provide the information regarding the sample size in each maturity group [21, 42], although a combined total of 761 female athletes within the age range of 10–18 years were included in these studies. Based on the data reported from 14 studies, the mean age, stature and mass of the pre-pubertal girls were 10.4 ± 1.2 years, 143.9 ± 7.6 cm and 37.9 ± 5.6 kg; pubertal female girls were 12.5 ± 0.7, 157 ± 4.1 cm and 47.3 ± 4.3 kg; post-pubertal female individuals were 16.7 ± 3 years, 165 ± 2.7 and 59.4 ± 3.4 kg. The maturity level of the athletes was determined using the Pubertal Maturational Observation Scale (PMOS) [38, 39, 43], modified PMOS [24, 25, 27, 40, 42, 45], percentage predicted adult height (PAH) [21, 49], self-assessed Tanner Scale [44], Tanner 5 stages of maturity [46], Tanner grouping [48] and onset of menarche [41]. In two studies that used percentage adult stature for determining maturity status, post-pubertal female individuals were reported to be > 91% of adult stature in one study [21] and > 94% of adult stature in the other study [49]. Across the various scales used in the included studies for estimating the maturity status, the lowest values were used for classifying pre-pubertal girls (i.e. < 85% PAH, Tanner Stage 1, PMOS stage 1), highest for post-pubertal female individuals (i.e. > 95% PAH, Tanner Stages 4–5, PMOS stage 5) and the values in-between for pubertal girls (i.e. 85–95% PAH, Tanner Stages 2–4, PMOS stages 2–4).
The studies included in our review assessed the biomechanical risk factors for ACL injuries during various jump-landing tests. Twelve studies had the participants perform the drop vertical jump [21, 24, 25, 38,39,40,41,42,43, 46, 47, 49] (DVJ), one study used the SL vertical stop jump test [44], one study used the maximum vertical jump test [48], while two studies had the participants perform the SL drop lateral jump [41, 45] and one study performed the drop jump with a static landing sequence [49]. With respect to the DVJ test, the height from which the participants were asked to jump was predominantly 31 cm [21, 24, 25, 27, 38,39,40, 42, 43, 49]; however, 30 cm [46] and 36 cm [47] were also used, while the drop height was not reported in one study [41]. Kinematic data were collected using three-dimensional motion capture systems in nine studies [21, 24, 25, 38,39,40, 44, 48, 49], while two studies used two-dimensional video cameras [41, 46]. Overall, eight studies compared changes in biomechanical variables across all three maturity groups (pre-pubertal, pubertal and post-pubertal) [25, 39, 42, 43, 45,46,47, 49], four studies compared only pubertal and post-pubertal female individuals [21, 24, 27, 40], and four studies compared pre-pubertal and post-pubertal female athletes [38, 41, 44, 48]. Ten studies were cross-sectional in nature [25, 39, 41, 42, 44,45,46,47,48,49], four were longitudinal [21, 27, 38, 43] and two had nested cohort [24, 40] study designs. Further details regarding the participant characteristics for all the individual studies have been provided in Table 1.
3.3 Methodological Quality
The overall methodological quality (mean ± standard deviation) for the included studies was 70 ± 8%, with a range from 53 to 89%. Nine studies [21, 27, 38, 42, 43, 45,46,47,48] were classified to be of high quality and seven studies [24, 25, 39,40,41, 44, 49] were of moderate quality. The detailed scoring for each study can be found in Table 2. Additionally, the criteria used for scoring each question of the Downs and Black checklist can be found in Table S1 of the ESM.
3.4 Strength of Evidence Synthesis
For the kinematic variables, we found strong evidence for post-pubertal female individuals having a higher peak knee abduction angle compared with pre-pubertal and pubertal girls. With regard to the kinetic variables, we found strong evidence for post-pubertal female individuals having higher knee abduction and internal rotation moments compared with pre-pubertal girls. There was strong evidence for pre-pubertal girls having higher peak relative vGRF (normalised to BW) compared with post-pubertal female individuals. The strength of evidence for all the other kinematic and kinetic variables ranged from moderate to conflicting and could not be determined in some instances. Table 3 and Fig. 2 provide the detailed results of the findings.

Summary of the strength of evidence for the kinematic and kinetic variables across various stages of maturity. IC initial contact, vGRF ground reaction force, ↑ indicates higher kinematic or kinetic values as female athletes progress to the next stage of maturity, ↓ indicates lower kinematic or kinetic values as female athletes progress to the next stage of maturity, ↔ indicates similar kinematic and kinetic values as female athletes progress to the next stage of maturity, ↑↓ indicates conflicting evidence
3.5 Kinematic Risk Factors
A total of 12 kinematic variables were identified across the included studies. The findings of the kinematic variables from the individual studies are summarised in Table 4.
3.5.1 Knee Kinematics
Seven studies reported variables associated with the knee flexion angle during various jump-landing tests, including the knee angle at IC, peak knee flexion and knee flexion at peak vGRF. Post-pubertal female individuals had the lowest knee flexion at IC in three studies [24, 39, 41, 44] of moderate quality and the highest knee flexion at IC in one high-quality study [48] when compared with pre-pubertal girls. Two moderate-quality studies [24, 39] reported post-pubertal female individuals to have the lower knee flexion angle at IC compared with pubertal girls. One moderate-quality study [39] reported pre-pubertal girls to have lower knee flexion at IC compared with pubertal girls.
Knee flexion angle at peak knee flexion was reported in four studies, with variable findings [24, 38, 44, 49]. The high-quality study by DiCesare et al. [38] reported post-pubertal female individuals to have a lower peak knee flexion angle compared with pre-pubertal girls. Other studies of moderate quality showed equivocal findings, with higher peak knee flexion in pre-pubertal [49] or post-pubertal [44] groups. Two studies of moderate quality found post-pubertal female individuals to have lower peak knee flexion compared with pubertal girls [24, 49]. For knee flexion angle at peak vGRF, pre-pubertal girls were found to have lower values than post-pubertal female individuals [48].
Knee abduction angle during jump-landing tasks was reported in seven studies. A high-quality study by Swartz et al. [48] reported pre-pubertal girls to have higher knee abduction compared with post-pubertal peers. However, contradictory findings were reported in two studies of moderate quality [25, 44], in which pubertal girls were found to have the highest knee abduction angle at IC compared with pre-pubertal and post-pubertal girls in one moderate-quality study.
Five studies reported data for the peak knee abduction angle [21, 25, 38, 40, 49], with varying quality of evidence showing post-pubertal female individuals had higher peak knee abduction compared with pre-pubertal and pubertal girls. A high-quality study by Swartz et al. [48] reported pre-pubertal girls to have a higher peak knee abduction angle compared with post-pubertal peers at the instant of peak vGRF. Knee abduction displacement was reported in two studies of high [46] and moderate quality [25], with post-pubertal athletes displaying consistently higher values compared with pubertal and pre-pubertal girls.
Several other knee-related kinematic variables were reported by two studies of moderate [39] and poor [41] quality. Post-pubertal female individuals had higher knee flexion [39, 52] and knee abduction displacement [41] compared with pubertal and pre-pubertal girls, with the exception of the knee adduction angle at IC, which was higher in pubertal girls [39].
3.5.2 Hip Kinematics
Hip flexion angle at IC and peak vGRF [24, 48], hip extension angle at IC [39], and hip flexion, adduction and rotation displacement [39] were reported in several individual studies. These studies were of high [48] and moderate [24] quality. Pre-pubertal girls had lower hip flexion at IC and peak vGRF compared with pubertal and post-pubertal female individuals [47, 56], with the highest values reported in pubertal female individuals [47]. Pubertal and post-pubertal female individuals had lower hip flexion and angular displacement than pre-pubertal girls [39]. Pubertal girls had higher hip adduction displacement and extension at IC than pre-pubertal and post-pubertal girls [39].
3.5.3 Ankle Kinematics
One study reported the ankle plantarflexion and dorsiflexion angle, which showed that post-pubertal female individuals had a higher ankle plantarflexion at IC, but a lower peak ankle dorsiflexion, compared with pubertal girls [24].
3.6 Kinetic Risk Factors
A total of eight kinetic variables were identified across the included studies. The moments reported for the hip, knee and ankle joints were external moments. The findings of the kinetic variables from the individual studies are summarised in Table 5.
3.6.1 Knee Kinetics
Sagittal plane external knee extensor moment was reported in both a high-quality study [38] and a moderate-quality [41] study. While DiCesare et al. [38] reported post-pubertal female individuals had a higher peak knee extensor moment compared with pre-pubertal girls, contradictory findings were reported in the other study [41]. Post-pubertal female individuals had the highest peak external knee flexion moment (i.e. more quadriceps dominant) values followed by pubertal and then pre-pubertal girls [45, 49].
Peak external knee abduction moment during jump-landing tasks was reported in three high-quality studies [21, 38, 45] and three moderate-quality studies [40, 41, 49]. Post-pubertal female individuals had the highest values followed by pubertal and pre-pubertal girls in five studies [21, 24, 38, 45, 49], while pre-pubertal girls had the highest value in one study [41].
Post-pubertal female individuals had the highest peak internal rotation moment values followed by pubertal and pre-pubertal girls. Post-pubertal female individuals also had the highest average knee adductor moment followed by pubertal and pre-pubertal girls.
3.6.2 Hip and Ankle Kinetics
Peak external hip flexion and ankle dorsiflexion moments were reported in one moderate-quality study [24], which identified that post-pubertal girls had higher values compared with pubertal girls.
3.6.3 Vertical Ground Reaction Force
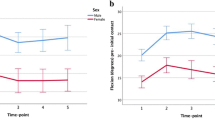
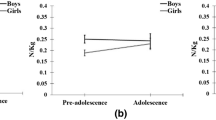
Vertical ground reaction force normalised to BW during various jump-landing tasks were reported in four high-quality studies [27, 42, 43, 48] and three moderate-quality studies [39, 41, 44]. In addition, a moderate-quality study [42] reported the percentatage change in landing vGRF across various stages of maturity. Overall, pre-pubertal girls were found to have consistently higher values in vGRF compared to post-pubertal female individuals in five studies [39, 41, 43, 44, 48], The findings were equivocal when pre-pubertal girls were compared with pubertal girls. While one high-quality study [43] reported pre-pubertal girls to have marginally higher values, the other study [39] reported the values to be the same in both groups. Similarly, the findings were contradictory when pubertal girls were compared with post-pubertal female individuals. While a high-quality study [43] and a moderate-quality study [39] reported pubertal girls to have higher values, another high-quality study [27] reported the values to be the same in both groups. One study reported changes in vGRF during the landing phase of a jump-landing task [50]. The vGRF in female individuals decreased by 5.3% and then increased by 8.4% from Tanner stages 2 to 3 and then decreased by 16.8% from Tanner stages 3 to 4 and 4 to 5.
4 Discussion
Our review aimed to synthesise the changes in potential biomechanical risk factors associated with ACL injuries across various stages of maturity in female athletes. Common scales used for determining the maturity level of female athletes included PMOS, modified PMOS, % predicted adult height, self-assessed Tanner Scale, Tanner 5 stages of maturity, Tanner grouping and onset of menarche. The jump-landing tasks used for reporting the variation in biomechanics across different stages of maturity were DVJ, SL vertical stop jump test, maximum vertical jump, SL drop lateral jump and drop jump with a static landing sequence. Of the 12 kinematic variables reported in our review, we found strong evidence for a higher peak knee abduction angle in post-pubertal female individuals compared with pre-pubertal girls during deceleration tasks. With regard to the eight kinetic variables, we found strong evidence for higher knee abduction and internal rotation moments in post-pubertal female individuals compared with pre-pubertal girls (Fig. 3). There was also strong evidence for higher peak vGRF in pre-pubertal girls compared with post-pubertal female individuals (Fig. 3). The strength of evidence for the remaining kinematic and kinetic variables ranged from conflicting to moderate and, in some instances, could not be determined highlighting the need for further research in this area.

Summary of kinematic and kinetic variables in the A sagittal and B frontal plane for meaningful changes from pre-pubertal (red skeletons) to post-pubertal (white skeleton) female individuals. This figure has been adapted from the study published by Galloway et al. [82] with permission from the publisher (License Number: 5746521199753). vGRF vertical ground reaction force
4.1 Knee Abduction
We found strong evidence for a higher peak knee abduction angle in post-pubertal female individuals compared with pre-pubertal athletes. Further, post-pubertal female individuals also had higher knee abduction displacement compared with pre-pubertal athletes. Our findings are similar to previous meta-analytical data in which female individuals were found to have an increased knee abduction angle with increasing maturity [50]. Anterior cruciate ligament load is a result of the combination of higher knee abduction and internal rotation moments [51], and we found strong evidence that these kinetic variables were increased with maturation and peaked in post-pubertal female individuals. It has been speculated that female individuals tend to become more ligament dominant as they mature whereby they employ more limited knee flexion and rely more on frontal place loading to decelerate their centre of mass during maturation [21, 25, 52]. In addition, the rapid increases in lower extremity limb length accompanied by a marked increase in body mass that occur during adolescence, in the absence of sufficient neuromuscular adaptation, are related to decreased dynamic knee stability and increased joint torque loads in female athletes [21]. Interestingly, we found conflicting evidence for the knee abduction angle at IC between pre-pubertal and post-pubertal female individuals and peak knee abduction angle between pre-pubertal and pubertal female individuals. A variety of jump-landing tasks such as the DVJ, SL vertical stop jump and maximum vertical jump tests were used across various studies. Therefore, variation and complexity in the jumping protocol implemented along with differences in sample size (see Table 1), mode of data collection (two dimensional or three dimensional), inadequate training experience and poor technique in performing advanced jumping tests such as SL vertical jumping, and the use of various scales for estimating the maturity status of female athletes (PMOS vs % adult stature) could have led to equivocal findings across the respective studies.
Notably, DiCesare et al. [38] found sport-specialised athletes had a higher knee abduction angle compared with multi-sport athletes; however, higher values were observed in post-pubertal female individuals compared with pre-pubertal girls irrespective of their specialisation status. The literature suggests that diversification of movement should be prioritised during early childhood and adolescence for comprehensive motor and coordination development [53]. Conversely, early sport specialisation may reduce movement variability [54] and promote the development of a narrow range of specialised skills, thereby negatively impacting the development of a child’s motor skills portfolio [55]. Therefore, future research should consider the potential role of sports specialisation on jump-landing biomechanics across various maturity levels and whether it predisposes athletes to a higher risk of ACL injury. Incorporating other training programmes could be beneficial for athletes in order to develop movement competence during various tasks irrespective of their participation in single or multiple sports. For instance, previous research has indicated that neuromuscular training programmes were effective in reducing the risk of ACL injuries in early or mid-teens by 72% (odds ratio: 0.278) [56]. This review included studies that had performed various interventions such as plyometrics, balance training, weight training, and speed and agility training. Another review highlighted that a multi-faceted training intervention with at least three different exercise types and techniques was beneficial in reducing ACL injuries in female athletes under 19 years of age, with plyometric and strength training being the most commonly recommended forms of exercises [57]. In light of these findings, it might be beneficial for female athletes to be exposed to neuromuscular training interventions from a young age (i.e. in the pre-pubertal years) to improve their jump-landing biomechanics and reduce their risk of ACL injury.
4.2 Knee Flexion
We found limited evidence differentiating pre-pubertal and pubertal female athletes for knee flexion angle at IC and conflicting evidence for maturational differences in peak knee flexion during jump-landing tasks. Of the three studies that compared pre-pubertal and post-pubertal female individuals, two studies of high [38] and moderate [49] quality found post-pubertal female individuals had lower peak knee flexion compared with pre-pubertal girls, whereas another study [44] reported the former to have a higher peak knee flexion angle, albeit the findings were non-significant. Interestingly, we also found very limited evidence that pre-pubertal girls had reduced knee flexion range of motion compared with post-pubertal female individuals during SL static, vertical and lateral drop jump-landing tasks [41]. These differences could primarily be attributed to the differences in jump-landing protocols incorporated in the included studies. While DiCesare et al. [38] and Westbrook et al. [49] had their participants perform a DVJ, Pletcher et al. [44] had their participants perform a SL vertical stop jump. Previous findings have reported lower hip and knee flexion angles at IC during SL landing tasks compared with double-leg landing tasks [58,59,60]. Additionally, SL landing tasks are biomechanically more challenging for the knee joint in comparison to double-leg landing tasks because of greater lower extremity loading, greater motor control and a smaller base of support [48], which in turn could have resulted in pre-pubertal girls adopting a different landing strategy during these tasks.
Despite the findings being equivocal across various studies, landing with less knee flexion increases the load on the ACL because of the increased quadriceps and reduced hamstring muscle activity [61]. An increased knee flexion helps in decreasing the vGRF and rate of force development during jump-landing tasks [62,63,64,65], ultimately reducing anterior tibial translation load at the knee. Previous studies have indicated that female athletes tend to land with less knee flexion after 12 years of age during SL stride jump and double-leg stop jump tasks [66, 67]. A prospective study by Hewett et al. [25] reported that female athletes sustaining ACL injuries demonstrated 10.4° less peak knee flexion prior to injury compared with uninjured teammates during a DVJ test. Interestingly, we found moderate evidence for post-pubertal female individuals having higher knee flexion moments compared with pre-pubertal girls, with the latter group displaying less knee flexion at landing in two studies. This highlights that female athletes tend to use a more quadriceps dominant strategy while performing jump-landing tasks as they progress through the maturity stages. Leppanen et al. [17] reported that female athletes with higher peak knee external moment were at an increased risk of injury because of higher quadricep forces. The same authors had previously reported that female athletes also presented with less peak knee flexion [68]. Landing with less knee flexion can result in an increased anterior tibial shear load, especially in early deceleration phases of movement, in turn increasing the possibility of athletes sustaining an ACL injury. Female individuals gain approximately 8–10 kg per year 6–9 months after the onset of the growth spurt [69]. However, this gain in mass is primarily absolute and relative fat instead of lean mass [70]. Therefore, the absence of sufficient strength in addition to the rapid increase in size and weight at about, or near, puberty in female athletes might increase their risk of sustaining ACL injuries [71]. Overall, our review highlights that the knee flexion angle varies at different stages of maturity in female athletes, but the direction of these changes with advancing maturation were not consistent. This highlights the need for further research to better understand the influence of this particular kinematic variable.
4.3 Vertical Ground Reaction Force
We found strong evidence for higher relative peak vGRF in pre-pubertal girls than post-pubertal female individuals. Normalisation of vGRF is performed to account for the differences in various body characteristics such as stature and body mass. Such an approach allows for a valid analysis and comparison of results between different groups/participants [72]. The higher relative vGRF in pre-pubertal athletes could be a result of the normalisation process as post-pubertal female individuals tend to have a higher body mass than pre-pubertal girls. However, this speculation could not be confirmed as the included studies did not provide absolute vGRF values across different maturity groups. The study by Pedley et al. [43] stated that absolute vGRF was higher in more mature groups during a drop jump test, although the absolute values were not reported. Larger force peaks during the early phase of jump-landing tasks are a concern as the majority of ACL injuries have been reported to occur during the first 40 ms of ground contact [73]. An increase in absolute peak vGRF of 100 N has been found to increase the probability of ACL injury by 26% in young female athletes [68]. Therefore, future studies should consider reporting absolute and relative vGRF values across various maturity groups. Further, landing is a motor skill that children do not develop until the age of 12 years and continue to refine as they progress through various developmental stages into adulthood [74]. Previous findings have suggested that the ability to modulate vGRF upon impact and throughout the landing phase improves with the process of ageing owing to contributions from factors such as physical maturity, skill development and experience in performing jumping tasks [75]. Given that the average age of pre-pubertal athletes assessed in the included studies was 10.4 years, the higher relative vGRF in this group could be attributed to their lack of experience in performing the jump-landing tasks as they are still in the process of motor skill acquisition. Koga et al. [73] previously found that elite female athletes who sustained an ACL injury during competitive matches had a peak vGRF of 3.2–4.5 times BW occurring at 40 ms after IC while performing jump-landing tasks. Interestingly, the relative vGRF values were found to range between 3.21 and 8.42 times BW even in pre-pubertal athletes in our review. Therefore, jump-landing techniques with high vGRF, combined with the anatomical, hormonal, biomechanical and neuromuscular changes occurring during the process of growth and maturation, might partly explain the increased incidence of ACL injuries in female adolescent athletes. This further highlights the need for early training interventions in female athletes. As an example, neuromuscular training interventions combining strength and plyometric exercises have been found to reduce the ground reaction forces in female netball players aged 11–13 years (g > − 1.30) [76]. Further, a study by Hewett et al. [77] reported that female adolescents performing plyometric exercises significantly decreased their peak landing forces during a vertical jump by 1.2 times their BW. Participation in such training programmes could help female athletes develop the requisite strength levels and enhanced landing technique as they transition through various stages of maturity, which in turn could reduce the ACL injury rates in this population.
4.4 Other Kinematic/Kinetic Findings
Several biomechanical variables related to the hip and ankle were reported in three studies [24, 39, 48]. Pre-pubertal athletes were found to have a higher hip extension angle at IC compared with post-pubertal female athletes, albeit the differences were non-significant. Although Swartz et al. [48] did not perform an exclusive statistical comparison between pre-pubertal and post-pubertal female athletes, the former were found to have a lower hip flexion angle. However, attenuation of impact forces during landing depends more on active hip flexion than the angle at IC [13]. Given that pre-pubertal girls had higher hip flexion displacement compared with post-pubertal female individuals, the higher relative vGRF could be attributed to the jump-landing technique adopted by pre-pubertal girls. Interestingly, peak hip flexion moment was found to be higher in post-pubertal female individuals, a result that is in line with previous findings in which female athletes between 12 and 21 years of age were found to have a higher peak hip flexion moment compared with their uninjured cohort [17]. However, there was no statistically significant association between this kinetic variable and ACL injury.
With regard to ankle biomechanics, pubertal female athletes did not differ in peak ankle dorsiflexion angle or moment compared to post-pubertal female athletes. A greater ankle plantar flexion angle at IC has been found to reduce the risk of ACL injuries [78, 79]. For instance, trends of ACL injured athletes having a marginally lower ankle flexion compared with uninjured athletes during a DVJ test has been observed in floorball (a form of indoor hockey with five players and a goalkeeper) and basketball athletes between the age of 12 and 21 years [17]. Limited ankle plantar flexion at IC during landing could lead to higher vGRF being subsequently transferred and in turn, loading the knee to a greater extent [78]. However, these interpretations are speculative and the association and variation in magnitude of effect of the above-mentioned variables on knee biomechanics and ACL injury risk across different stages of maturity are still unknown.
4.5 Limitations
While the current review has provided novel analyses of the existing data, certain limitations need to be acknowledged. First, the maturity level of the athletes was classified using several different scales. Even when studies used the same method [25, 49], there were variations in the manner of interpreting the maturity outcome. However, we reduced the heterogeneity of the findings by limiting our review to studies that had clearly reported the scale used for measuring the maturity status of the participants. As an example, a study by Hass et al. [66] in which pubertal and post-pubertal female individuals had been compared was excluded from the review because they did not provide information regarding the scale used for estimating maturity. Second, we could not perform a meta-analysis of the reported kinematic and kinetic variables because of the variation in the study design; the mode of data collection varied across the included studies and certain variables were not reported in all studies. Such a quantitative analysis would help to identify the standardised magnitude of changes of the reported biomechanical variables across various stages of maturity. However, we have aimed to summarise all the kinematic and kinetic variables reported in the literature across various stages of maturity during jump-landing tasks, and in doing so have highlighted the most commonly researched kinematic and kinetic variables reported across various maturity groups in young female athletes.
4.6 Future Research Directions
Jump-landing tasks are usually conducted as part of screening tests to identify athletes at a higher risk of sustaining injuries [80]. Several tests such as a vertical jump, DVJ and tuck jump are routinely performed as part of the screening process. For young and inexperienced athletes, it should be noted that more demanding jumping tasks (e.g. SL jumps) might be difficult to perform without the requisite levels of motor competence. Therefore, future studies should also consider the role of training and sporting experience of the athlete prior to performing various SL and double-leg jump-landing tasks as part of the screening process. Such an approach should provide further clarity on the suitability of a particular jumping test for athletes at certain stages of maturity/technical competence.
Numerous SL and double-leg landing tasks were performed across various studies included in our review. Task constraints play a crucial role in influencing the biomechanical demands during these tasks [81]. The variation in the testing protocols implemented in the studies could be one of the reasons for the strength of evidence being conflicting for a few kinematic and kinetic variables in our review. However, when the same jump-landing task was performed across various studies, there was an improvement in the level of strength of evidence. As an example, we found strong evidence for higher peak knee abduction angle in post-pubertal female individuals as participants in five of the six studies [21, 25, 38, 40, 49] that reported this variable had performed the same DVJ test. Therefore, further research that uses common jump-landing protocols is required to better understand the associations between the biomechanical variables reported in our study and ACL injury.
We found only three studies that had compared the changes in hip and ankle biomechanics across various stages of maturity. The hip and ankle joint play a key role in influencing knee motion during the deceleration phase of jump-landing tasks. However, the strength of evidence for the majority of hip and ankle biomechanical variables ranged from limited to very limited. Therefore, future research is needed to better understand how changes in kinetics and kinematics at the hip and ankle may contribute to ACL injury risk at different stages of maturity.
5 Conclusions
We found strong evidence for a higher peak knee abduction angle, knee abduction and internal rotation moment in post-pubertal female athletes. There was also strong evidence for pre-pubertal girls having higher peak vGRF compared with the athletes in the more mature groups. These findings highlight that growth and maturation influence landing biomechanics, which may increase injury mechanisms at different stages of development. It might be beneficial to incorporate strength and conditioning training programmes from a young age in order to help reduce the magnitude of alterations in multiplanar landing biomechanics as female athletes progress through various stages of maturity. However, further research is required to achieve a better understanding of the association between hip, knee and ankle biomechanics and ACL injury across different stages of maturity.
References
Shea KGAP, Pfeiffer RP. Anterior cruciate ligament injury in paediatric and adolescent patients: a review of basic science and clinical research. Sports Med. 2003;33(6):455–71.
Shaw L, Finch CF. Trends in pediatric and adolescent anterior cruciate ligament injuries in Victoria, Australia 2005–2015. Int J Environ Res Public Health. 2017;14(6):599.
Longo UG, Salvatore G, Ruzzini L, Risi Ambrogioni L, de Girolamo L, Vigano M, et al. Trends of anterior cruciate ligament reconstruction in children and young adolescents in Italy show a constant increase in the last 15 years. Knee Surg Sports Traumatol Arthrosc. 2021;29(6):1728–33.
Whittaker JL, Toomey CM, Nettel-Aguirre A, Jaremko JL, Doyle-Baker PK, Woodhouse LJ, et al. Health-related outcomes after a youth sport-related knee injury. Med Sci Sports Exerc. 2019;51(2):25–63.
Caine DJ, Golightly YM. Osteoarthritis as an outcome of paediatric sport: an epidemiological perspective. Br J Sports Med. 2011;45(4):298–303.
Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007;35(10):1756–69.
Myklebust GHI, Maehlum S, Engebretsen L, Bahr R. Clinical, functional, and radiologic outcome in team handball players 6 to 11 years after anterior cruciate ligament injury: a follow-up study. Am J Sports Med. 2003;31(6):981–9.
Dekker TJ, Godin JA, Dale KM, Garrett WE, Taylor DC, Riboh JC. Return to sport after pediatric anterior cruciate ligament reconstruction and its effect on subsequent anterior cruciate ligament injury. J Bone Joint Surg Am. 2017;99(11):897–904.
Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of second ACL injuries 2 years after primary ACL reconstruction and return to sport. Am J Sports Med. 2014;42(7):1567–73.
Webster KE, Feller JA, Klemm HJ. Second ACL injury rates in younger athletes who were advised to delay return to sport until 12 months after ACL reconstruction. Orthop J Sports Med. 2021;9(2):2325967120985636.
Boden BP, Dean GS, Feagin JA Jr, Garrett WE Jr. Mechanisms of anterior cruciate ligament injury. Orthopedics. 2000;23(6):573–8.
Pappas E, Shiyko MP, Ford KR, Myer GD, Hewett TE. Biomechanical deficit profiles associated with ACL injury risk in female athletes. Med Sci Sports Exerc. 2016;48(1):107–13.
Yu B, Lin CF, Garrett WE. Lower extremity biomechanics during the landing of a stop-jump task. Clin Biomech (Bristol, Avon). 2006;21(3):297–305.
Walden M, Krosshaug T, Bjorneboe J, Andersen TE, Faul O, Hagglund M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: a systematic video analysis of 39 cases. Br J Sports Med. 2015;49(22):1452–60.
Hewett TE, Myer G, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501.
Sharir R, Rafeeuddin R, Staes F, Dingenen B, George K, Vanrenterghem J, et al. Mapping current research trends on anterior cruciate ligament injury risk against the existing evidence: in vivo biomechanical risk factors. Clin Biomech (Bristol, Avon). 2016;37:34–43.
Leppanen M, Pasanen K, Krosshaug T, Kannus P, Vasankari T, Kujala UM, et al. Sagittal plane hip, knee, and ankle biomechanics and the risk of anterior cruciate ligament injury: a prospective study. Orthop J Sports Med. 2017;5(12):2325967117745487.
Boden BP, Torg JS, Knowles SB, Hewett TE. Video analysis of anterior cruciate ligament injury: abnormalities in hip and ankle kinematics. Am J Sports Med. 2009;37(2):252–9.
Mason-Mackay AR, Whatman C, Reid D. The effect of reduced ankle dorsiflexion on lower extremity mechanics during landing: a systematic review. J Sci Med Sport. 2017;20(5):451–8.
Wild CYSJ, Munro BJ. Why do girls sustain more anterior cruciate ligament injuries than boys? A review of the changes in estrogen and musculoskeletal structure and function during puberty. Sports Med. 2012;42(9):733–49.
Hewett TE, Myer GD, Kiefer AW, Ford KR. Longitudinal increases in knee abduction moments in females during adolescent growth. Med Sci Sports Exerc. 2015;47(12):2579–85.
Hewett TE, Myer GD, Ford KR. Anterior cruciate ligament injuries in female athletes: part 1, mechanisms and risk factors. Am J Sports Med. 2006;34(2):299–311.
Sarwar R, N B, Rutherford OM. Changes in muscle strength, relaxation rate and fatiguability during the human menstrual cycle. J Physiol. 1996; 493(1):267–272.
Ford KR, Myer GD, Hewett TE. Longitudinal effects of maturation on lower extremity joint stiffness in adolescent athletes. Am J Sports Med. 2010;38(9):1829–37.
TE Hewett MG, Ford KR. Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Jt Surg Am. 2004;86(8):1601–8.
Tanner JMDP. Clinical longitudinal standards for height and height velocity for North American children. J Pediatr. 1985;107(3):317–29.
Quatman CE, Ford KR, Myer GD, Hewett TE. Maturation leads to gender differences in landing force and vertical jump performance: a longitudinal study. Am J Sports Med. 2006;34(5):806–13.
Renstrom P, Ljungqvist A, Arendt E, Beynnon B, Fukubayashi T, Garrett W, et al. Non-contact ACL injuries in female athletes: an International Olympic Committee current concepts statement. Br J Sports Med. 2008;42(6):394–412.
Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. 2021;10(1):89.
Drevon D, Fursa SR, Malcolm AL. Intercoder reliability and validity of WebPlotDigitizer in extracting graphed data. Behav Modif. 2017;41(2):323–39.
Higgins JPTTJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Cochrane handbook for systematic reviews of interventions. 2nd ed. Chichester: Wiley; 2019.
Wannop JWWJ, Stefanyshyn DJ. Normalization of ground reaction forces, joint moments, and free moments in human locomotion. J Appl Biomech. 2012;28(6):665–76.
Downs SHBN. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–84.
Cronstrom A, Creaby MW, Nae J, Ageberg E. Gender differences in knee abduction during weight-bearing activities: a systematic review and meta-analysis. Gait Posture. 2016;49:315–28.
Kennelly J. Methodological approach to assessing the evidence. In: Reducing racial/ethnic disparities in reproductive and perinatal outcomes. Boston: Springer; 2011. p. 7–19.
van Tulder M, Furlan A, Bombardier C, Bouter L, Editorial Board of the Cochrane Collaboration Back Review Group. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine. 2003;28(12):1290–9.
Furlan AD, Malmivaara A, Chou R, Maher CG, Deyo RA, Schoene M, Editorial Board of the Cochrane Back, Neck Group, et al. 2015 updated method guideline for systematic reviews in the Cochrane Back and Neck Group. Spine. 2015;40(21):1660–73.
DiCesare CA, Montalvo A, Barber Foss KD, Thomas SM, Ford KR, Hewett TE, et al. Lower extremity biomechanics are altered across maturation in sport-specialized female adolescent athletes. Front Pediatr. 2019;7:268.
DiStefano LJ, Martinez JC, Crowley E, Matteau E, Kerner MS, Boling MC, et al. Maturation and sex differences in neuromuscular characteristics of youth athletes. J Strength Cond Res. 2015;29(9):2465–73.
Ford KR, Shapiro S, Myer GD, Van Den Bogert AJ, Hewett TE. Longitudinal sex differences during landing in knee abduction in young athletes. Med Sci Sports Exerc. 2010;42(10):1923–31.
Hass CJ, Schick EA, Tillman MD, Chow JW, Brunt D, Cauraugh JH. Knee biomechanics during landings: comparison of pre- and postpubescent females. Med Sci Sports Exerc. 2005;37(1):100–7.
TE Hewett MG, Ford KR, Slauterbeck JR. Preparticipation physical examination using a box drop vertical jump test in young athletes: the effects of puberty and sex. Clin J Sport Med. 2006;16(4):298–304.
Pedley JS, DiCesare CA, Lloyd RS, Oliver JL, Ford KR, Hewett TE, et al. Maturity alters drop vertical jump landing force-time profiles but not performance outcomes in adolescent females. Scand J Med Sci Sports. 2021;31(11):2055–63.
Pletcher ER, Dekker TJ, Lephart SM, Sell TC. Sex and age comparisons in neuromuscular and biomechanical characteristics of the knee in young athletes. Int J Sports Phys Ther. 2021;16(2):438–49.
Sayer TA, Hinman RS, Paterson KL, Bennell KL, Fortin K, Timmi A, et al. Differences in hip and knee landing moments across female pubertal development. Med Sci Sports Exerc. 2019;51(1):123–31.
Schmitz RJSS, Nguyen AD. Dynamic valgus alignment and functional strength in males and females during maturation. J Athl Train. 2009;44(1):26–32.
Sigward SM, Pollard CD, Powers CM. The influence of sex and maturation on landing biomechanics: implications for anterior cruciate ligament injury. Scand J Med Sci Sports. 2012;22(4):502–9.
Swartz EE, Decoster LC, Russell PJ, Croce RV. Effects of developmental stage and sex on lower extremity kinematics and vertical ground reaction forces during landing. J Athl Train. 2005;40(1):9–14.
Westbrook AE, Taylor JB, Nguyen AD, Paterno MV, Ford KR. Effects of maturation on knee biomechanics during cutting and landing in young female soccer players. PLoS ONE. 2020;15(5): e0233701.
Holden S, Boreham C, Delahunt E. Sex differences in landing biomechanics and postural stability during adolescence: a systematic review with meta-analyses. Sports Med. 2016;46(2):241–53.
Shin CS, Chaudhari AM, Andriacchi TP. Valgus plus internal rotation moments increase anterior cruciate ligament strain more than either alone. Med Sci Sports Exerc. 2011;43(8):1484–91.
Pollard CD, Sigward SM, Powers CM. Limited hip and knee flexion during landing is associated with increased frontal plane knee motion and moments. Clin Biomech (Bristol, Avon). 2010;25(2):142–6.
Wiersma L. Risks and benefits of youth sport specialization: perspectives and recommendations. Pediatr Exerc Sci. 2000;12:13–22.
Riehm CD, Bonnette S, Riley MA, Diekfuss JA, DiCesare CA, Schille A, et al. Movement regularity differentiates specialized and nonspecialized athletes in a virtual reality soccer header task. J Sport Rehabil. 2022;32(3):248–55.
Sylvia M,Jon O, Paul R, John C, Gregory M, Rhodri L. Practical strategies for integrating strength and conditioning into early specialization sports. J Strength Cond Res. 2021; 44(1):4–45.
Myer GD, Sugimoto D, Thomas S, Hewett TE. The influence of age on the effectiveness of neuromuscular training to reduce anterior cruciate ligament injury in female athletes: a meta-analysis. Am J Sports Med. 2013;41(1):203–15.
Mattu AT, Ghali B, Linton V, Zheng A, Pike I. Prevention of non-contact anterior cruciate ligament injuries among youth female athletes: an umbrella review. Int J Environ Res Public Health. 2022;19(8):4648.
Earl JE, Monteiro SK, Snyder KR. Differences in lower extremity kinematics between a bilateral drop-vertical jump and a single-leg step-down. J Orthop Sports Phys Ther. 2007;37(5):245–52.
Harty CM, DuPont CE, Chmielewski TL, Mizner RL. Intertask comparison of frontal plane knee position and moment in female athletes during three distinct movement tasks. Scand J Med Sci Sports. 2011;21(1):98–105.
Pappas EHM, Sheikhzadeh A, Nordin M, Rose D. Biomechanical differences between unilateral and bilateral landings from a jump: gender differences. Clin J Sport Med. 2007;17(4):263–8.
Ebben WPFM, Petushek EJ, Garceau LR, Hsu BE, Lutsch BN, Feldmann CR. Gender-based analysis of hamstring and quadriceps muscle activation during jump landings and cutting. J Strength Cond Res. 2010;24(2):408–15.
Cowling EJSJ, McNair PJ. Effect of verbal instructions on muscle activity and risk of injury to the anterior cruciate ligament during landing. Br J Sports Med. 2003;37(2):126–30.
Irmischer BS, Harris C, Pfeiffer RP, DeBeliso MA, Adams KJ, Shea KG. Effects of a knee ligament injury prevention exercise program on impact forces in women. J Strength Cond Res. 2004;18(4):703–7.
McNair PJ, Prapavessis H, Callender K. Decreasing landing forces: effect of instruction. Br J Sports Med. 2000;34(4):293–6.
Onate JA, Guskiewicz KM, Marshall SW, Giuliani C, Yu B, Garrett WE. Instruction of jump-landing technique using videotape feedback: altering lower extremity motion patterns. Am J Sports Med. 2005;33(6):831–42.
Hass CS, Elizabeth, Chow, John, Tillman, Brunt, Denis, Cauraugh, James. Lower extremity biomechanics differ in prepubescent and postpubescent female athletes during stride jump landings. J Appl Biomech. 2003;19:139–52.
Yu B, McClure SB, Onate JA, Guskiewicz KM, Kirkendall DT, Garrett WE. Age and gender effects on lower extremity kinematics of youth soccer players in a stop-jump task. Am J Sports Med. 2005;33(9):1356–64.
Leppanen M, Pasanen K, Kujala UM, Vasankari T, Kannus P, Ayramo S, et al. Stiff landings are associated with increased ACL injury risk in young female basketball and floorball players. Am J Sports Med. 2017;45(2):386–93.
Tanner JMWR. Clinical longitudinal standards for height, weight, height velocity, weight velocity, and stages of puberty. Arch Dis Child. 1976;51(3):170–9.
Malina RM, Rogol AD, Cumming SP, Coelho e Silva MJ, Figueiredo AJ. Biological maturation of youth athletes: assessment and implications. Br J Sports Med. 2015;49(13):852–9.
Griffin LY, Albohm MJ, Arendt EA, Bahr R, Beynnon BD, Demaio M, et al. Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005. Am J Sports Med. 2006;34(9):1512–32.
Mullineaux DRMC, Davis IS, Hamill J. Normalization of ground reaction forces. J Appl Biomech. 2006;22(2):230–3.
Koga H, Nakamae A, Shima Y, Iwasa J, Myklebust G, Engebretsen L, et al. Mechanisms for noncontact anterior cruciate ligament injuries: knee joint kinematics in 10 injury situations from female team handball and basketball. Am J Sports Med. 2010;38(11):2218–25.
Barber-Westin SD, Noyes FR, Galloway M. Jump-land characteristics and muscle strength development in young athletes: a gender comparison of 1140 athletes 9 to 17 years of age. Am J Sports Med. 2006;34(3):375–84.
Angulo-Barroso R, Ferrer-Uris B, Jubany J, Busquets A. Children’s strategies in drop-landing. Front Psychol. 2022;13: 982467.
Hopper AJ, Haff EE, Joyce C, Lloyd RS, Haff GG. Neuromuscular training improves lower extremity biomechanics associated with knee injury during landing in 11–13 year old female netball athletes: a randomized control study. Front Physiol. 2017;8:883.
Hewett TE, Stroupe A, Nance TA, Noyes FR. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24(6):765–73.
Lee J, Shin CS. Association between ankle angle at initial contact and biomechanical ACL injury risk factors in male during self-selected single-leg landing. Gait Posture. 2021;83:127–31.
Wahlstedt C, Rasmussen-Barr E. Anterior cruciate ligament injury and ankle dorsiflexion. Knee Surg Sports Traumatol Arthrosc. 2015;23(11):3202–7.
Bahr R. Why screening tests to predict injury do not work-and probably never will …: a critical review. Br J Sports Med. 2016;50(13):776–80.
Emamian A, Hashemi Oskouei A, Azreh R, Carroll K. Effects of task constraints on countermovement jump kinematics following a short-term training. J Motor Learn Dev. 2022;10(2):257–72.
Galloway RT, Xu Y, Hewett TE, Barber Foss K, Kiefer AW, DiCesare CA, et al. Age-dependent patellofemoral pain: hip and knee risk landing profiles in prepubescent and postpubescent female athletes. Am J Sports Med. 2018;46(11):2761–71.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
No funding was received for the conducting of this study or the preparation of this article.
Conflict of interest
Gregory D. Myer consults with commercial entities to support commercialisation strategies and applications to the US Food and Drug Administration but has no direct financial interest in the commercialisation of the products. Gregory D. Myer’s institution receives current and ongoing grant funding from National Institutes of Health/NIAMS Grants U01AR067997, R01 AR070474, R01AR055563, R01AR076153, R01 AR077248, R61AT012421, the Department of Defense W81XWH22C0062 and Arthritis Foundation OACTN. Gregory D. Myer has received industry sponsored research funding to his institutions related to injury prevention and sport performance and has current ongoing funding from Arthrex, Inc. to evaluate ACL surgical treatment optimisation strategies. Gregory D. Myer receives author royalties from Human Kinetics and Wolters Kluwer. Gregory D. Myer is an inventor of biofeedback technologies (Patent No.: US11350854B2, Augmented and Virtual reality for Sport Performance and Injury Prevention Application, Approval Date: 06/07/2022, Software Copyrighted) designed to enhance rehabilitation and prevent injuries that receives licensing royalties. Akhilesh Kumar Ramachandran, Jason S. Pedley, Sylvia Moeskops, Jon L. Oliver and Rhodri S. Lloyd have no conflicts of interest that are directly relevant to the content of this article.
Ethics approval
Not applicable.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Availability of data and material
All data and material reported in this systematic review are only from peer-reviewed publications. All the extracted data have been provided in Tables 1 and 5 of the ESM.
Code availability
Not applicable.
Author contributions
AKR, JLO and RSL conceived the idea for the review. AKR and RSL undertook the systematic search, screening and quality assessment. JLO provided consensus where needed on quality rating and inclusion criteria. AKR and RSL drafted the manuscript. JP, SM, JLO, GM and RSL reviewed and edited the manuscript. All authors read and approved the final version.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ramachandran, A.K., Pedley, J.S., Moeskops, S. et al. Changes in Lower Limb Biomechanics Across Various Stages of Maturation and Implications for ACL Injury Risk in Female Athletes: a Systematic Review. Sports Med 54, 1851–1876 (2024). https://doi.org/10.1007/s40279-024-02022-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40279-024-02022-3