
Abstract
Purpose of Review
In this review, we discuss the importance of nutrition evaluation and counseling for living kidney donor candidates (LKDCs) and the roles of the dietitian and transplant physician.
Recent Findings
In the past decades, living kidney donors are becoming older and have higher rates of obesity and glucose intolerance. Like all adult populations, living kidney donors are at risk for developing diabetes, obesity, hypertension, and kidney disease post-donation, and risks may rise as these chronic diseases rise in the general population. Further, implications may be more serious for individuals living with one kidney. However, involvement of the dietitian in the evaluation of LKDCs may vary across transplant centers. Current US policies do not absolutely require a Registered (Transplant) Dietitian to be involved in the care of LKDCs during the various phases of donation.
Summary
Dietitians should be involved in the evaluation of all LKDCs. Individualized lifestyle-focused, sustainable nutrition counseling should be provided to all LKDCs. Transplant clinicians should engage in nutrition counseling of LKDCs as this can increase the impact of the intervention. Nutrition evaluation and counseling can lead to life-long change for the LKDC.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Although registered dietitians (RDs) are required members of the transplant multi-disciplinary team, there is no set requirement for their involvement with the living kidney donor population. The guidelines from the Centers for Medicare and Medicaid Services state that “potential living donors…may require various levels of nutritional assessment” but do not absolutely require that a Registered (Transplant) Dietitian must be involved in the care of living kidney donor candidates (LKDCs) during the various phases of donation [1]. The United Network for Organ Sharing similarly does not have any specific regulations or recommendations regarding the role of the RD with the LKDC population.
Since the top reasons that LKDCs are declined for kidney donation continue to be nutritionally pertinent factors including obesity, diabetes, and hypertension (HTN); this population would directly benefit from RDs’ (specifically transplant dietitians) involvement [2]. As members of the transplant team, RDs are uniquely positioned to provide nutritional health counseling to reduce the lifetime risk of end stage kidney disease (ESKD) in LKDCs. While this notion is increasingly recognized, it is often not completely implemented at many transplant centers. A 2019 Transplant Dietitian Survey representing 196 transplant programs conducted by Pieloch et al. demonstrated an increase in the involvement of dietitians in LKDC assessment from 2014 to 2019. However, only 53% of centers reported completing a nutrition evaluation on all potential donors and 35% reported continuing to utilize screening criterion to only evaluate donors deemed to be “at risk” [3]. According to Pieloch’s survey, dietitians were most involved with LKDC with obesity (73%) and pre-diabetes (52%).
The lack of direction from transplant governing bodies, inadequate staffing resources at many transplant programs, and a long-held assumption that LKDCs are “healthy,” can result in a disservice to this important patient population and miss out opportunities to improve their nutritional health. In this review, we discuss the importance of nutrition evaluation and counseling during the assessment of LKDCs, the roles of the dietitian, and transplant clinicians in LKDC nutritional health and provide resources to improve nutrition counseling for this population.
Nutrition Evaluation of the Potential Living Donor
There are no practice guidelines for nutrition care of LKDCs nor minimum standards defining what the LKDC nutrition evaluation should comprise. Pieloch et al. published the first standardized framework for transplant specific competencies for transplant dietitians in 2017, which identified minimum requirements to be met by transplant RDs when working with this population [4•]. These competencies include identifying nutrition risk factors for donation (obesity, prediabetes, and HTN) and providing medical nutrition therapy (MNT) for donor candidates with significant and modifiable nutritional risks or barriers to donation (obesity, prediabetes, borderline HTN) [4•]. LKDCs meeting with a transplant dietitian as a part of their donor evaluation process should expect to undergo a thorough assessment based on the Nutrition Care Process shown in Table 1 [10]. The assessment of the combination of these factors allows the dietitian to identify lifestyle risk factors associated with current and long-term risk of chronic diseases (obesity, diabetes, and HTN) and counsel the LKDC accordingly. It is important to note that given the short duration of appointments associated with the living donor evaluation process, the bulk of the nutrition evaluation visit is spent on assessment versus counseling.
Importance of Nutrition Counseling for the Potential Living Donor Population
Living Kidney Donors and Chronic Disease Risk
According to the 1990–2016 report on the State of US Health, high body mass index (BMI), high fasting plasma glucose, and high blood pressure were the top risk factors accounting for loss of disability-adjusted life-years [11]. Living kidney donors, while healthier than the general US population, are also at risk for these diseases. In the RELIVE (Renal and Lung Living Donor Evaluation) study, Taler et al. reported on the trends in living kidney donation across three transplant centers over a five-decade period [12]. Review of almost 9000 living kidney donors demonstrated an increase in the percentage of older donors, donors with obesity and donors with glucose intolerance [12]. These findings are consistent with the metabolic changes contributing to the continued rise in the general population of obesity and diabetes.
After donation, living kidney donors are also at risk for the development of diabetes, obesity, and HTN, which contribute to renal dysfunction. A 2017 study by Ibrahim et al. examined the incidence of diabetes after kidney donation and its impact on changes in estimated glomerular filtration rate (eGFR), proteinuria, HTN, and ESKD [13•]. Of the roughly 4000 living donors studied, 7.7% developed diabetes. Those that developed diabetes were more likely to have a higher BMI at the time of donation, higher serum creatinine levels, lower eGFR, and higher glucose levels. Donors who developed diabetes were more likely to develop HTN and proteinuria (average 9.2 years after diabetes diagnosis) and had a larger decline in eGFR compared to those without diabetes, HTN, and proteinuria. Risk factors for development of diabetes post kidney donation are the same as those in the general population (elevated BMI and elevated glucose levels). Further, an analysis of linked national US donor registry data with records from a pharmacy claims warehouse (2007–2016) found that donors with an overweight and obese BMI at donation carried 2 (adjusted HR, 2.23; 95% CI 1.62–3.06) and 4 times (adjusted HR 4.59; 95% CI 3.36–6.27) greater likelihood of using anti-diabetic medication over the following 9 years post-donation, respectively [14].
Other studies have also shown that living kidney donors are at increased risk for the development of ESKD after donation compared to health-matched controls and may have higher levels of proteinuria post-donation [15•, 16]. In a shifting landscape of living kidney donors who are increasingly less healthy, the transplant community should consider that differences in baseline donor health will likely mean clinically significant differences in health outcomes for the donors who are donating today compared with those who donated 20 years ago.
Poor Nutrition Is Foundational to Chronic Disease Development
Poor nutrition is foundational to the development of the most prevalent chronic diseases affecting Americans—cardiovascular disease, diabetes, HTN, and obesity. The 2019 Global Burden of Disease Study of 195 countries found that poor diet was the leading cause of morbidity and mortality for non-communicable diseases [17]. Dietary factors have also been described as associating with the development of chronic kidney disease [18, 19]. Correction of suboptimal nutrition is a powerful way to prevent, control, and often reverse the most common chronic diseases and may also delay the progression of CKD [20, 21, 22•]
The dietary choices of LKDCs are reflective of the dietary choices prevalent in the general US population. According to the 2020–2025 Dietary Guidelines, the core elements that make up a healthy dietary pattern include intake of all types of vegetables, fruit (especially whole fruit), grains (with at least half consisting of whole grains), fat-free or low-fat dairy, protein foods consisting of lean meats, poultry, eggs, seafood, legumes, nuts, seeds, and soy products, and oils [23]. Furthermore, the guidelines place an emphasis on limiting added sugars, saturated fats, sodium, and alcoholic beverages [23]. In our unpublished single-center study of 54 LKDCs presenting for evaluation, we found that none of the LKDCs met adherence criteria for these recommendations. Similar to the general US population, LKDC’s intake of vegetables, fruits, whole grains, dairy, fiber, and potassium did not meet the recommended guidelines while their intake of refined grains, added sugar, sodium, and fats exceeded the recommended guidelines. The inadequate intake of potassium and excessive intake of sodium are concerning given their well-established association with HTN [24]. The reported excess intake of added sugar, excess intake of refined grains, and inadequate intake of fiber are also concerning given the well-established association between these foods and diabetes risk [25].
LKDCs, like the rest of the US population, are heavily influenced by diet fads and misinformation. In our experience, most LKDCs with overweight or obesity have attempted multiple diets before coming for donation evaluation. We often encounter LKDCs who consume excess protein in the form of ultra-processed foods out of a belief that these are health-promoting. Most LKDCs have never received nutrition counseling and the living kidney donor evaluation visit is usually the first time they have ever met with a dietitian. This reflects the current state of the US healthcare system, which focuses on treating chronic diseases rather than preventing them. While some experts believe that nutrition assessment and counseling should be offered to medically complex LKDCs such as those with HTN, obesity, or kidney stones [26•], we believe that all LKDCs should receive nutritional evaluation and counseling given the high rates of poor dietary intake in this population and thus high potential for the development of chronic diseases in the future. Our approach is not to treat only those who have already developed early signs of chronic disease but to do our best to prevent those diseases in all LKDCs. In alignment with the transplant community’s prevention-centered mindset, offering all LKDCs nutritional counseling provides an untapped opportunity to help prevent the development of chronic diseases in this population of selfless individuals.
Effective Nutrition Evaluation and Counseling
Sustainable Behavior Change
Living donor programs recognize the importance of minimizing risk factors for chronic disease development in LKDCs, and implement acceptance thresholds for BMI, blood pressure, and blood glucose. However, simply telling donors the targets to achieve for donation is insufficient. Issa et al. studied post-donation weight change and its association with the risk of developing cardiovascular disease, diabetes, HTN, and ESKD [27]. Over a median of 22.3 years of follow-up, most donors gained weight post-donation. Donors who lost weight between their evaluation and time of donation had the most amount of weight gain and the highest rate of weight gain post-donation. Donors in the highest tertile of post-donation weight gain were also more likely to have a statistically significant increase in systolic and diastolic blood pressures, higher glucose values, and a higher relative risk of HTN and diabetes [27]. This study suggests that providing LKDCs with target metrics alone does not offer long-term protection from obesity, HTN, and hyperglycemia. LKDCs deserve optimal dietary counseling with sustainable lifestyle modifications regardless of donation. This would allow LKDCs to maintain a healthy dietary pattern which is the cornerstone to minimize their risk for chronic diseases.
As a group, LKDCs are highly motivated, selfless individuals. This motivation serves as a positive attribute, usually leading them to make lifestyle changes required to continue with evaluation and eventual organ donation. However, there is also a sense of urgency resulting in some individuals seeking “quick fix” solutions that include experimentation with fad diets that are not sustainable and do not produce long-lasting results. It is important to educate LKDCs that nutritional and lifestyle changes should be sustainable to maximize long-term outcomes. Transplant clinicians should set holistic goals beyond a target metric (i.e., set weight goal) and provide counseling and tools that result in healthy long lasting dietary habits.
We argue that the single most important factor to consider when advising potential donors on lifestyle change is the sustainability of the change. Whether the focus is on lifestyle change for weight loss, glycemic management, or HTN, if the change is not sustainable, the risk factors will re-surface. Good nutrition counseling techniques emphasize meeting individuals where they are, use an individualized, culturally sensitive approach, and are ongoing. Motivational interviewing (MI), a well-studied technique that focuses on the patient aiming to resolve ambivalence in the decision-making process, has been shown to improve patient response to lifestyle change [28], and improve the response to interventions targeting obesity [29] and cardiovascular disease risk factors [30]. Dietitians trained in MI are more effective in fostering patient adherence to changes in dietary habits [31]. However, effective MI requires multiple visits as effective change cannot be achieved through a single session. Several organizations have provided recommendations for the minimum number and frequency of visits for effective change. For example, the Academy of Nutrition and Dietetics recommends a minimum of 3–6 visits over six months for the prevention and treatment of pre-diabetes and type 2 diabetes [32]. Behavior change, especially in relation to nutritional change is difficult. The transplant community should support donor candidates with appropriate resources for effective change. While it may not be possible for transplant centers to provide the repeat counseling visits that are needed, lifestyle-focused goals should be incorporated in standard LKDC counseling.
The Role of the Dietitian
Individualized counseling ensures that recommendations are tailored to the person’s cultural preferences, taste preferences, and socioeconomic needs. Table 1 outlines the components of the nutrition assessment as well as the approach that our team takes when evaluating LKDCs. The nutrition assessment conducted by the transplant dietitian should include a thorough review of food and nutrition history including current and previous dieting attempts, current and previous eating patterns, and any barriers to food intake and/or preparation, including access to food. This information, in conjunction with evaluation of physical activity, anthropometrics, laboratory markers, and the LKDC’s personal and family medical history allows the dietitian to identify risk factors for current or future chronic disease and provide initial counseling on the correlation between these factors and their health. Physical activity information is also collected (Table 1) and used in counseling, though further details about physical activity counseling is beyond the scope of this paper.
Dietary intake assessment tools range from informal methods such as a food frequency questionnaire, to more formal methods like electronic dietary recall tools. At our center, we use the Automated Self-Administered 24-h (ASA24) Dietary Assessment Tool, which is a comprehensive, validated, web-based, multiple-pass questionnaire [5] that has been shown to improve participant recall of foods and reduce recall bias [6, 7]. In our practice, we ask all LKDCs to complete the ASA24 prior to their in-person evaluation visit and information from their ASA24 can be used for individual counseling and follow-up.
It has been previously suggested that nutrition evaluation and counseling in the LKDC population should be focused on medically complex donors presenting with metabolic risk factors given lack of transplant dietitian resources [26•]. We believe that there are several benefits to completing a full nutrition evaluation on all LKDCs, not just those that present with risk. As previously mentioned, most adults in the US do not meet the Dietary Guidelines. Obtaining a thorough diet and physical activity history allows the transplant dietitian to identify areas for improvement in LKDC that do not currently present with obvious risk factors for chronic disease but may be at future risk due to their existing lifestyle. For those presenting to evaluation with existing risk factors, the dietitian can make tailored recommendations to improve risk factors.
The Role of the Physician
While the public perceives physicians as credible and reliable sources of information regarding health and nutrition, physicians generally lack adequate training in evidence-based nutrition, a deficit that is becoming increasingly recognized [33, 34•, 35, 36]. Clinical care guidelines refer to optimizing nutrition as the primary intervention for management of chronic diseases, but physicians are not poised to do this and under-recognize the importance of their involvement in nutrition counseling. Patients who receive weight loss counseling by their physician are more likely to understand the risks of obesity, the benefits of weight loss, and be more motivated for weight loss and behavioral change [37,38,39]. Physician counseling can help patients move further along the spectrum of the stages of change, and the better the counseling given, the more motivated patients can become [38, 39]. Even 3–5 min of structured counseling can be effective in producing patient behavioral change [40]. Guiding patients to making dietary changes requires a team effort, and physicians by default form a part of that team. In our experience working with pre- and post-transplant patients, having physicians participate and reinforce nutritional counseling has a positive impact in patients’ uptake and adherence to recommendations from the dietitians.
Physicians need to take ownership of their own education in nutrition and behavioral change as it is their responsibility to their patients, including the LKDCs whom they evaluate. Fortunately, there is increasing recognition of the crucial role that nutrition plays in medicine. While including a comprehensive list of physician education resources is beyond the scope of this paper, below we offer a compilation of professional societies and educational resources to enhance the knowledge of evidence-based nutrition medicine so physicians can be prepared to provide adequate nutritional counseling to patients.
-
The American College of Lifestyle Medicine (ACLM) provides numerous training opportunities for graduate medical education in nutrition and lifestyle medicine and free resources for physicians to use in patient counseling (see Table 2) [41, 42].
-
The Nutrition in Medicine project created by the University of North Carolina provides free nutrition education for practicing physicians [43].
-
The Physicians’ Committee for Responsible Medicine provides a free Nutrition Guide for Clinicians app and online resource for healthcare professionals [44, 45]. They also provide free patient-facing nutrition information (see Table 2).
-
Nutritionfacts.org is a nonprofit organization providing science-based nutrition education organized in “bite-sized videos, blogs, podcasts and infographics” [46].
Our Center’s Practice
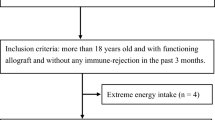
Figure 1 provides a schema of our current approach to LKDC evaluation, focusing on nutritional evaluation and counseling. The evaluation process is a team-based affair that requires input from physicians, dietitians, social workers, and transplant nurse coordinators. We have incorporated the collection of dietary intake information on all LKDCs through the ASA24 in the evaluation process. All LKDCs also provided donor-specific health handouts and the ACLM’s handout about the pillars of healthy lifestyle that the MD or RD reviews with each LKDC. RDs are also involved not only in the initial evaluation of LKDCs but also often circle back to LKDCs to discuss outcomes of committee decisions and to provide counseling for achieving donation success. These contact points may occur many months out from the initial LKDC evaluation.

The living kidney donor evaluation process at UC Davis Health’s Transplant Program
Resources for Evidence-Based Nutrition Counseling
When counseling donors on specific changes, it is important not only to prioritize the underlying disease state or risk of future disease but also to balance recommendations with what is realistic and feasible for the individual. While no one diet has been shown to be superior for management of all chronic diseases, there is substantial evidence that dietary patterns shown to be conducive to overall health include a preponderance of whole plant foods including fruits, vegetables, legumes, nuts/seeds, and whole grains, and minimization of saturated fats, added sugars and added sodium. Examples of this dietary pattern include the “Mediterranean Diet”, the DASH diet, the “Blue Zone” diet, and the “Whole Food Plant Based Diet.” At minimum, transplant clinicians can introduce this dietary pattern to all LKDCs as an important step for long-term health. The focus on whole plant foods allows individualization to the potential donor’s tastes and cultural preferences. The goal is a partnership with the individual to set specific, realistic, and attainable goals. In Table 2, we have listed patient-facing online resources and handouts for evidence-based nutrition information that can assist in nutrition counseling. Additionally, the Dietary Guidelines for Americans 2020–2025 can be used as a starting point to talk about increasing whole plant food intake and reducing ultra-processed foods [23]. Our team has created handouts for our transplant center, including a handout specific to living kidney donors (available on request).
Outside of aiming to reduce risk of chronic disease, some donor candidates will require more specific nutrition education to maintain kidney health. One common example are those LKDCs with excessive protein intake, most commonly seen among athletes or recreational exercise enthusiasts and those following dietary patterns focused on higher protein and lower carbohydrate intake. Given the evidence of accelerated CKD progression in the setting of excessive protein intake, all LKDCs should be counseled on the risks of excessive protein intake and advised against this [22•]. Another special consideration includes donors with a history of kidney stones or at risk of developing them. Recommendations for the management of the various types of kidney stones are outside the scope of this review, but it is recommended that those individuals work with a dietitian and physician specializing in this field as part of their donor evaluation process [47].
Conclusion
Nutrition evaluation and counseling should be provided to all LKDCs to help them become successful donors and maximize post-donation health outcomes. Nutrition counseling is time intensive and requires multiple sessions with well-trained and experienced team members, including dietitians and physicians. We believe all transplant centers should offer access to transplant dietitians to all LKDCs, especially those whose eligibility depends on correction of nutrition-related issues such as obesity, pre-diabetes, and HTN. This may help improve approval of LKDC while allowing donors to achieve better long-term health outcomes, though further research is needed here (Table 3). Utilization of dietitians has been shown to be cost-effective management of chronic diseases like obesity [48], dyslipidemia and cardiovascular risk [48, 49], and diabetes [32, 48].
Recognizing that many transplant centers may not have enough resources to support a model of comprehensive nutritional care for LKDCs, we believe the next best option is to offer LKDCs a one-time meeting with the transplant dietitian at the time of their pre-donation evaluation. Data suggest that only 53% of centers reported doing nutrition assessments on their LKDCs. The transplant dietitian should be involved in all LKDC evaluations to collect nutrition and lifestyle information and provide, at minimum, a brief individualized counseling session. Transplant physicians should participate in peri-transplant lifestyle and nutrition counseling. Transplant centers should consider engaging community resources and list practitioners for referral. Lifestyle medicine is a growing field with certified practitioners increasing across the world, and community dietitians may be a vetted resource for patients outside of their primary care physicians.
Long-term outcomes in living donors require further research, and the Scientific Registry of Transplant Recipients (SRTR) Living Donor Collective is a promising strategy to gather long-term information starting with donor candidates and extending to long term follow-up [2]. However, beyond the usual medical information that is collected on LKDCs, it would be important to consider assessments of lifestyle factors such as dietary intake, which is known to be a major determinant of health outcomes. We have begun collecting dietary intake information from all LKDCs who come for our in-person evaluation using the ASA24. We have found that including dietary information has been helpful to understand the baseline intake of our potential donors, to use as a repeat measure, and to guide how we approach counseling. Beyond being of immediate use to the medical team, diet intake data collected from LKDCs can help to answer important questions about how dietary choices can impact donors in the long term (Table 3).
Nutrition evaluation and counseling for LKDCs remains an untapped opportunity for lifelong change, not just for the LKDC, but for the potential kidney transplant recipient, as each LKDC who goes on to successfully donate a kidney saves the life of another person in need. Through improved nutrition health counseling among LKDC, we may be able to positively influence living kidney donor outcomes in the future.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
CMS Survey and Certification Letter: Organ Transplant Interpretive Guidelines Department of Health and Human Services: Centers for Medicare and Medicaid Services2016 [Available from: https://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/SurveyCertificationGenInfo/Downloads/Survey-and-Cert-Letter-16-10.pdf.
Kasiske BL, Asrani SK, Dew MA, Henderson ML, Henrich C, Humar A, et al. The living donor collective: a scientific registry for living donors. Am J Transplant. 2017;17(12):3040–8.
Pieloch D. Redefining practice in transplant nutrition: results of the 2019 Transplant Dietitian Survey. NATCO Nutrition Conference2020.
• Pieloch D, Friedman GG, DiCecco S, Ulerich L, Beer S, Hasse J. A standardized framework for transplant-specific competencies for dietitians. Prog Transplant. 2017;27(3):281–5. Identified minimum competencies that should be met by transplant RDs when working with LDKCs.
NIH National Cancer Institute Division of Cancer Control and Populations Sciences. Automated Self-Administered 24-Hour (ASA24) Dietary Assessment Tool National Institute of Health National Cancer Institute2022 [Available from: https://epi.grants.cancer.gov/asa24/.
Kirkpatrick SI, Subar AF, Douglass D, Zimmerman TP, Thompson FE, Kahle LL, et al. Performance of the Automated Self-Administered 24-hour Recall relative to a measure of true intakes and to an interviewer-administered 24-h recall. Am J Clin Nutr. 2014;100(1):233–40.
Subar AF, Potischman N, Dodd KW, Thompson FE, Baer DJ, Schoeller DA, et al. Performance and feasibility of recalls completed using the Automated Self-Administered 24-Hour Dietary Assessment Tool in Relation to other self-report tools and biomarkers in the Interactive Diet and Activity Tracking in AARP (IDATA) Study. J Acad Nutr Diet. 2020;120(11):1805–20.
IPAQ - International Physical Activity Questionnaire [Internet]. Updated 2022; cited 2024 Jan 12. Available from: https://sites.google.com/view/ipaq/home.
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–95.
Academy of Nutrition and Dietetics. Nutrition Care Process Overview 2023 [Available from: https://www.eatrightpro.org/practice/nutrition-care-process/ncp-overview.
US Burden of Disease Collaborators, et al. The State of US Health, 1990–2016: Burden of Diseases, Injuries, and Risk Factors Among US States. JAMA. 2018;319(14):1444–72.
Taler SJ, Messersmith EE, Leichtman AB, Gillespie BW, Kew CE, Stegall MD, et al. Demographic, metabolic, and blood pressure characteristics of living kidney donors spanning five decades. Am J Transplant. 2013;13(2):390–8.
• Ibrahim HN, Berglund DM, Jackson S, Vock DM, Foley RN, Matas AJ. Renal consequences of diabetes after kidney donation. Am J Transplant. 2017;17(12):3141–8. Defined incidence of diabetes after kidney donation and its impact on changes in eGFR, proteinuria, HTN, and ESKD.
Lentine KL, Koraishy FM, Sarabu N, Naik AS, Lam NN, Garg AX, et al. Associations of obesity with antidiabetic medication use after living kidney donation: an analysis of linked national registry and pharmacy fill records. Clin Transplant. 2019;33(10):e13696.
• Muzaale AD, Massie AB, Wang MC, Montgomery RA, McBride MA, Wainright JL, et al. Risk of end-stage renal disease following live kidney donation. Jama. 2014;311(6):579–86. Showed that living kidney donors had higher rates of ESRD compared to health-matched controls.
Garg AX, Muirhead N, Knoll G, Yang RC, Prasad GV, Thiessen-Philbrook H, et al. Proteinuria and reduced kidney function in living kidney donors: a systematic review, meta-analysis, and meta-regression. Kidney Int. 2006;70(10):1801–10.
GBD 2017 Diet Collaborators. Health effects of dietary risks in 195 countries, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;393(10184):1958–72.
Kim H, Caulfield LE, Garcia-Larsen V, Steffen LM, Grams ME, Coresh J, et al. Plant-based diets and incident CKD and kidney function. Clin J Am Soc Nephrol : CJASN. 2019;14(5):682–91.
Du S, Kim H, Crews DC, White K, Rebholz CM. Association between ultraprocessed food consumption and risk of incident CKD: a prospective cohort study. Am J Kidney Dis. 2022;80(5):589-98.e1.
Mozaffarian D. Dietary and policy priorities for cardiovascular disease, diabetes, and obesity. Circulation. 2016;133(2):187–225.
Levey AS, Greene T, Beck GJ, Caggiula AW, Kusek JW, Hunsicker LG, et al. Dietary protein restriction and the progression of chronic renal disease: what have all of the results of the MDRD study shown? Modification of Diet in Renal Disease Study group. J Am Soc Nephrol. 1999;10(11):2426–39.
• Kalantar-Zadeh K, Joshi S, Schlueter R, Cooke J, Brown-Tortorici A, Donnelly M, et al. Plant-dominant low-protein diet for conservative management of chronic kidney disease. Nutrients. 2020;12:7. Reviews the current evidence for plant-based low-protein diets in preventing CKD progression.
U.S. Department of Agriculture and U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2020–2025 DietaryGuidelines.gov2020 [9th Edition:[Available from: DietaryGuidelines.gov.
Stone MS, Martyn L, Weaver CM. Potassium intake, bioavailability, hypertension, and glucose control. Nutrients. 2016;8:7.
Ley SH, Hamdy O, Mohan V, Hu FB. Prevention and management of type 2 diabetes: dietary components and nutritional strategies. Lancet. 2014;383(9933):1999–2007.
• Bergen CR, Reese PP, Collins D. Nutrition assessment and counseling of the medically complex live kidney donor. Nutr Clin Pract. 2014;29(2):207–14. Described nutrition evaluation and care of live organ donors.
Issa N, Sánchez OA, Kukla A, Riad SM, Berglund DM, Ibrahim HN, et al. Weight gain after kidney donation: association with increased risks of type 2 diabetes and hypertension. Clin Transplant. 2018;32(9):e13360.
Clifford D, and Curtis, Laura. Motivational Interviewing in Nutrition and Fitness: The Guilford Press; 2016 2016.
Resnicow K, McMaster F, Bocian A, Harris D, Zhou Y, Snetselaar L, et al. Motivational interviewing and dietary counseling for obesity in primary care: an RCT. Pediatrics. 2015;135(4):649–57.
Hardcastle SJ, Taylor AH, Bailey MP, Harley RA, Hagger MS. Effectiveness of a motivational interviewing intervention on weight loss, physical activity and cardiovascular disease risk factors: a randomised controlled trial with a 12-month post-intervention follow-up. Int J Behav Nutr Phys Act. 2013;10:40.
Brug J, Spikmans F, Aartsen C, Breedveld B, Bes R, Fereira I. Training dietitians in basic motivational interviewing skills results in changes in their counseling style and in lower saturated fat intakes in their patients. J Nutr Educ Behav. 2007;39(1):8–12.
Briggs Early K, Stanley K. Position of the Academy of Nutrition and Dietetics: the role of medical nutrition therapy and registered dietitian nutritionists in the prevention and treatment of prediabetes and type 2 diabetes. J Acad Nutr Diet. 2018;118(2):343–53.
Blunt SB, Kafatos A. Clinical Nutrition Education of Doctors and Medical Students: Solving the Catch 22. Adv Nutr. 2019;10(2):345–50.
• Aspry KE, Horn LV, Carson JAS, Wylie-Rosett J, Kushner RF, Lichtenstein AH, et al. Medical nutrition education, training, and competencies to advance guideline-based diet counseling by physicians: a science advisory from the American Heart Association. Circulation. 2018;137(23):e821–41. Reviewed gaps in undergraduate and graduate medical education in nutrition in the US, summarized reforms and outlined opportunities for improvement.
Crowley J, Ball L, Hiddink GJ. Nutrition in medical education: a systematic review. Lancet Planet Health. 2019;3(9):e379–89.
Devries S, Willett W, Bonow RO. Nutrition Education in Medical School, Residency Training, and Practice. JAMA. 2019;321(14):1351–2.
Huang J, Yu H, Marin E, Brock S, Carden D, Davis T. Physicians’ weight loss counseling in two public hospital primary care clinics. Acad Med. 2004;79(2):156–61.
Jay M, Gillespie C, Schlair S, Sherman S, Kalet A. Physicians’ use of the 5As in counseling obese patients: is the quality of counseling associated with patients’ motivation and intention to lose weight? BMC Health Serv Res. 2010;10:159.
Davis TC, Wolf MS, Bass PF, Arnold CL, Huang J, Kennen EM, et al. Provider and patient intervention to improve weight loss: a pilot study in a public hospital clinic. Patient Educ Couns. 2008;72(1):56–62.
Calfas KJ, Long BJ, Sallis JF, Wooten WJ, Pratt M, Patrick K. A controlled trial of physician counseling to promote the adoption of physical activity. Prev Med. 1996;25(3):225–33.
Lifestyle Medicine Education [Internet]. Greenville, South Carolina: University of South Carolina School of Medicine Greenville [updated 2022; cited 2024 Jan 12]. Available from: https://lifestylemedicineeducation.org/.
American College of Lifestyle Medicine [Internet]. Updated 2024; cited 2024 Jan 12. Available from: https://lifestylemedicine.org/.
Nutrition in Medicine [Internet]. Updated 2014; cited 2024 Jan 12. Available from: http://nutritioninmedicine.org/.
Physicians Committee for Responsible Medicine [Internet]. Physicians Committee for Responsible Medicine [Updated 2024; cited 2024 Jan 12]. Available from: https://www.pcrm.org/.
Nutrition Guide for Clinicians [Internet]. Physicians Committee for Responsible Medicine and Unbound Medicine, Inc. [Updated 2024; Accessed 2024 Jan 12]. Available from: https://nutritionguide.pcrm.org/nutritionguide.
NutritionFacts.org [Internet] Updated 2024; cited 2024 Jan 12. Available from: https://nutritionfacts.org/.
Poggio ED, Khan N, Bolanos C, Pham T, Tan JC. Evaluation of renal anatomy, structure and nephrolithiasis in living donor candidates. In: Lentine KL, Concepcion BP, Lerma EV, editors. Living kidney donation: best practices in evaluation, care and follow-up. Springer International Publishing; 2021; p. 93–117.
Casas-Agustench P, Megías-Rangil I, Babio N. Economic benefit of dietetic-nutritional treatment in the multidisciplinary primary care team. Nutr Hosp. 2020;37(4):863–74.
Sikand G, Cole RE, Handu D, deWaal D, Christaldi J, Johnson EQ, et al. Clinical and cost benefits of medical nutrition therapy by registered dietitian nutritionists for management of dyslipidemia: a systematic review and meta-analysis. J Clin Lipidol. 2018;12(5):1113–22.
Author information
Authors and Affiliations
Contributions
GF and LXC: conceptualization, data curation, formal analysis, writing, and reviewing and editing; RP: conceptualization and reviewing and editing.
Corresponding author
Ethics declarations
Competing Interests
GGF and RP have no conflicts of interest to report. LXC reports research support from MEMO Therapeutics, Transplant Genomics, Dexcom, and Veloxis Pharmaceuticals, all of which are not pertinent to the submitted work. LXC is certified in Lifestyle Medicine by the American Board of Lifestyle Medicine.
Human and Animal Rights and Informed Consent Statement
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Friedman, G.G., Perez, R. & Chen, LX. Nutrition Evaluation and Counseling for Potential Living Kidney Donors: An Opportunity for Lifelong Change. Curr Transpl Rep 11, 21–29 (2024). https://doi.org/10.1007/s40472-024-00430-y
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40472-024-00430-y