
Abstract
Introduction
Understanding the effects of corticosteroid utilization prior to initiation of biologic disease-modifying antirheumatic drugs (DMARDs) can inform decision-makers on the appropriate use of these medications. This study examined treatment patterns and associated burden of corticosteroid utilization before initiation of biologic DMARDs among rheumatoid arthritis (RA) patients.
Methods
A retrospective analysis was conducted of adult RA patients in the US MarketScan Database (2011–2015). The following patterns of corticosteroid utilization were analyzed: whether corticosteroids were used; duration of use (short/long duration defined as < or ≥ 3 months); and dosage (low as < 2.5, medium as 2.5 to < 7.5 and high as ≥ 7.5 mg/day). Effects of corticosteroid use on time to biologic DMARD initiation were examined using Cox proportional hazards models. Likelihood and number of adverse events were examined using logistic and negative binomial regression models. Generalized linear models were used to examine healthcare costs. Independent variables in all models included patient demographics and health characteristics.
Results
A total of 25,542 patients were included (40.84% used corticosteroids). Lower hazard of biologic DMARD initiation was associated with corticosteroid use (hazard ratio = 0.89, 95% confidence interval = 0.83–0.96), long duration and lower dose. Corticosteroid users compared to non-users had higher incidence rates of various adverse events including cardiovascular events (P < 0.05). Higher likelihood of adverse events was associated with corticosteroid use and long duration of use, as was increased number of adverse events. Corticosteroid users had a greater annualized mean number of physician visits, hospitalizations, and emergency department (ED) visits than non-users in adjusted analysis. Corticosteroid users compared to non-users had higher mean costs for total healthcare, physician visits, hospitalizations, and ED visits.
Conclusions
Among patients with RA, corticosteroid utilization is associated with delayed initiation of biologic DMARDS and higher burden of adverse events and healthcare utilization/costs before the initiation of biologic DMARDs.
Funding
AbbVie Inc.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rheumatoid arthritis (RA) is an autoimmune inflammatory disease associated with pain, stiffness, swelling, and loss of function in the joints, which can lead to poorer quality of life, and even increased mortality [1, 2]. The primary goal of RA treatment is to maximize long-term quality of life through control of symptoms, prevention of structural progression, and normalization of physical function and social participation [3]. A treat-to-target approach should be used to obtain these goals, which involves setting goals for treatment (e.g., low disease activity or remission), frequently monitoring disease status, and adjusting medication therapy as needed based on monitoring [1, 3].
DMARDs are recommended for all patients as the primary therapy in the treatment of RA as they have been shown to slow the course of the disease [1]. More specifically, the first step in treatment should be initiation of non-biologic DMARD monotherapy. If disease activity remains moderate to severe, biologic DMARDs are recommended as monotherapy or combination therapy with non-biologic DMARDs as they have substantially changed the course of disease and dramatically improved long-term outcomes in RA among patients refractory or intolerant to traditional DMARDs [1, 4].
Corticosteroids are widely used due to their quick anti-inflammatory effect and are recommended by the American College of Rheumatology in low doses as an effective short-term (< 3 months) therapy to ‘bridge’ patients until the benefits of DMARDs are observed or to manage DMARD failure or a disease flare [1]. The most recent guidelines by the European League Against Rheumatism (EULAR) have similar recommendations regarding the use of only short-term corticosteroids [2]. Harmful side effects of corticosteroid use have been reported (e.g., weight gain, worsening of diabetes, increased risk of infection), thus the decision to initiate therapy should be balanced by the lack of long-term corticosteroid safety studies in the RA population [1, 5, 6].
Many patients are not managed according to treatment guidelines, with significant delay in initiating DMARDs [7,8,9,10,11]. Researchers have thus explored the relationship between corticosteroid and biologic DMARD use in clinical practice [6,7,8,9,10]. For example, it was found that corticosteroids are often used as RA treatment prior to initiating DMARDs despite recommendations that all patients should be managed with a DMARD [6]. Another study found that median time from initiation of the traditional DMARD to the first biologic was more than 4 years [8]. Yazdany et al. found that one in ten RA patients receive corticosteroids alone without DMARDs [9]. Additionally, Kim et al. noted that corticosteroid users were more likely to initiate biologic DMARDS, and Caplan et al. found that initiation of biologic DMARDs is associated with the discontinuation of corticosteroids [10, 11].
Further exploration of the relationship between corticosteroid and biologic DMARD use in the treatment of RA is warranted. In particular, understanding corticosteroid treatment patterns and associated burden prior to biologic DMARD initiation can inform clinical and policy decision-makers on the appropriate use of these two drug classes in RA management. Santiago and da Silva noted limitations in the knowledge base regarding adverse events associated with corticosteroid use in RA treatment [6]. These investigators encourage that the “risk and benefit” of corticosteroid use in RA should be “regularly revisited [6]”. Therefore, the objectives of this study were to test whether: (1) corticosteroid utilization was associated with a delay in the initiation of biologic DMARDs among patients with RA; (2) corticosteroid utilization was associated with more adverse events before the initiation of biologic DMARDs among patients with RA; and (3) corticosteroid use was associated with higher healthcare utilization and costs before the initiation of biologic DMARDs among patients with RA.
Methods
A retrospective analysis was conducted of the MarketScan Commercial and Medicare Supplemental Claims and Encounters Database (1/1/2011–12/31/2015) [12]. MarketScan is a de-identified, nationwide medical claims database that includes insurance claims of inpatient, outpatient, emergency department (ED), pharmacy, behavioral healthcare, and enrollment data from a wide variety of health plans. All claims in the MarketScan Database are linkable using a unique patient ID. All claims except outpatient pharmaceutical claims have diagnosis codes associated with service records. Outpatient pharmaceutical claims include National Drug Code, date service incurred, days’ supply, and patient out-of-pocket expenses.
The study population was adults 18 years of age and older diagnosed with RA. To be included, a patient had to have at least two diagnoses of RA at least a week apart within a year in an ambulatory or non-acute setting [9, 13, 14]. The earliest date a patient was diagnosed with RA was identified as the index date as long as there was a six-month washout period before the date of diagnosis. A washout period was applied so there was a reasonable possibility that included patients were newly diagnosed with RA. Additionally, included patients were required to have continuous enrollment in a health insurance plan for 6 months prior to the index date, and 1 year following the index date. Patients were observed from the index date to the first initiation of a biologic DMARD, the end of the patient’s continuous enrollment in health plans or the end of 2015, whichever came first.
Corticosteroids evaluated included all oral corticosteroid prescriptions filled in a pharmacy and injectable corticosteroids administered in an outpatient or inpatient setting with a corresponding HCPCS code. All corticosteroids were converted to a prednisone equivalent dose [15,16,17]. For the purposes of counting treatment duration, injectable corticosteroids were counted the same as a 15-day supply of oral corticosteroids. Biologic drugs evaluated included: abatacept, adalimumab, anakinra, certolizumab, etanercept, golimumab, infliximab, rituximab, and tocilizumab.
Corticosteroid utilization measures were as follows: having used corticosteroids or not, treatment duration, and dosage [18, 19]. Having used corticosteroids or not is defined as a dummy variable, with having not used corticosteroids as the reference group. Treatment duration was defined as short term (< 3 months) and long term (≥ 3 months) based on the 2015 American College of Rheumatology Guidelines for the Treatment of RA [1]. The dosage categories were defined based on average daily dosages of prednisone as low (> 0 to < 2.5 mg/day), medium (2.5 to < 7.5 mg/day), and high (≥ 7.5 mg per day) [18, 19].
The study outcomes were time to initiation of biologic DMARD, diagnosis of adverse events, and health services utilization (physician visits, ED visits, hospitalizations, and medications) and costs (pharmacy and medical). The adverse events include cardiovascular, gastrointestinal, and skin conditions, infection, lipodystrophy, metabolic/endocrinologic, neuropsychiatric, and ophthalmologic conditions, and osteoporotic fractures (refer to Supplementary material: Table S1 for full list of adverse events) [11, 20,21,22,23,24].
The Andersen’s Behavioral Model of Health Services Utilization (Andersen’s Model) was used as the theoretical framework for including independent variables in the models due to the inclusion of outcomes related to utilization of medications and health services [25]. Based on this model, several factors were controlled for in the analysis [26,27,28,29]. Predisposing factors included age, gender, type of health plan, duration of follow-up when studying adverse events and health services utilizations and costs. Enabling factors included metropolitan statistical area, geographic region, and having a rheumatologist visit. Need factors included health services utilization, other medication utilization such as non-biologic DMARDs and/or analgesics, Charlson Comorbidity Index, and risk adjustment summary score based on Diagnostic Cost Group/Hierarchical Coexisting Condition Model.
Statistical Analysis
Descriptive statistics (i.e., mean, standard deviation) and frequency counts were used to summarize the baseline characteristics of the sample. Kaplan–Meier survival analysis was used to compare the duration of time from RA diagnosis to the initiation of the first biologic DMARD across treatment duration categories, and between individuals who have and have not used corticosteroids. Additionally, the time to biologic initiation across the different corticosteroid dose categories was evaluated. In multivariate analysis, the effects of corticosteroid use patterns on the initiation of biologic DMARDs were examined using Cox proportional hazards models.
To examine corticosteroid-related adverse events before the initiation of biologic DMARDs among patients with RA, the incidence rates per 100 patient years for adverse events were ascertained using diagnosis codes (see Supplementary material; Table S1). The following aspects of adverse events were analyzed: whether a patient experienced any corticosteroid-related adverse events and the number of corticosteroid-related adverse events. Multivariate logistic regression and negative binomial regression models were used to estimate the effects of each measure of corticosteroid utilization on adverse events. Logistic regression was conducted to examine the likelihood of an adverse event occurrence. Negative binomial models were used when examining the number of adverse events.
To investigate the effects of corticosteroid use on healthcare utilization before the initiation of biologic DMARDs among patients with RA, patients were observed from the first time corticosteroids were used to the initiation of the first biologic DMARD. Dependent variables included number of physician visits, hospitalizations, and ED visits, as well as costs of physician visits, hospitalizations, and ED visits, other outpatient costs, medication costs, and total healthcare costs. Multivariate logistic regression and negative binomial regression models were used to determine the effects of corticosteroid use on the utilization measures. Logistic regression was conducted to examine the likelihood of using certain health services. Negative binomial model was used when examining the number of health services. Multivariate generalized linear models with log link and gamma distribution were used to examine the effects of corticosteroid utilization on healthcare costs.
Independent variables in all multivariate regression analyses included patient socio-demographic and health characteristics. Data analysis was conducted using SAS®9.4 (SAS Institute Inc, Cary, NC) and STATA®13.1 (STATA Corporation, College Station, TX, USA). This study was approved by the Institutional Review Board at the University of Tennessee Health Science Center.
Results
A total of 25,542 RA patients were included (see Supplementary materials: Figure S1). Table 1 presents overall baseline patient characteristics and the comparison between corticosteroid users and nonusers. Mean patient age was 53.55 years with a standard deviation (SD) of 14.61 years, and the majority was female (70.17%). Among those who used corticosteroids, 90.22% used the medication for a short duration and 9.77% for a long duration (results now shown). The majority of corticosteroid users, 54.52%, used low-dose corticosteroids, while 40.32% used a medium dose and 4.40% used a high dose (results not shown). Those who used corticosteroids were slightly older, and were more likely to be female, have comprehensive health insurance or preferred provider organization, live outside an MSA, live in the south, and be treated by a rheumatologist. Corticosteroid users had higher healthcare utilization and were slightly more likely to also use non-biologic DMARDS, bone-active medications, analgesics, and NSAIDs. Finally, in general, corticosteroid users had more comorbidities. Further, higher proportions of lung diseases, history of infection, and mental illness were found in corticosteroid users (37.99, 11.43, and 20.69%, respectively) than nonusers (30.87, 9.03, 17.62%, respectively; P < 0.01; results not shown).
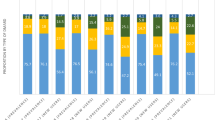
Based on Kaplan–Meier survival analysis, corticosteroid users (Fig. 1), had delayed time to initiation of a biologic DMARD compared to their counterparts (nonusers) (P < 0.001, based on log rank tests). Additional Kaplan–Meier survival analysis (not shown) found that those with longer duration of corticosteroid use and those in lower corticosteroid dosage categories had delayed time to initiation of a biologic DMARD compared to their counterparts (those with shorter duration and higher dosages, respectively) (P < 0.001, based on log rank tests). According to the Cox proportional hazards analysis (Table 2), lower hazard of biologic DMARD initiation was associated with corticosteroid use [Hazard Ratio (HR) = 0.89, 95% Confidence Interval (CI) = 0.83–0.96, compared to nonusers], long corticosteroid duration (HR = 0.73, 95% CI = 0.60–0.89, compared to short duration) and lower dosages (HR = 1.10, 95% CI = 0.98–1.23 for medium dose and HR = 1.87, 95% CI = 1.53–2.28 for high dose compared to low dose).

Time to biologic disease-modifying antirheumatic drug (DMARD) initiation by corticosteroid use
Corticosteroid users compared to non-users had significantly higher incidence rates of cardiovascular events, gastrointestinal events, infections, skin events, lipodystrophy, metabolic/endocrinologic events, neuropsychiatric events, and ophthalmologic events (P < 0.05; Table 3). In the multivariate regression (Table 4), corticosteroid use was associated with higher likelihood of experiencing an adverse event (OR = 1.13, 95% CI = 1.06–1.20). Long-duration of corticosteroid use compared to short duration was associated with increased likelihood of an adverse event (OR = 1.75, 95% CI = 1.47–2.09). Corticosteroid dosage categories were not associated with likelihood of an adverse event. Corticosteroid use was also associated with increased number of adverse events compared to non-use [incidence rate ratio (IRR) = 1.09, 95% CI = 1.05–1.14]. Long duration of corticosteroid use compared to short duration was associated with increased number of adverse events (IRR = 1.31, 95% CI = 1.19–1.44). Among the dosage categories, medium dose compared to low dose was associated with reduced number of adverse events (IRR = 0.94, 95% CI = 0.88–0.99). There was no significant difference in the number of adverse events between high dose and either medium or low dose.
Differences in average annualized healthcare utilizations and costs per patient between corticosteroid users and non-users are summarized in Table 5. In the unadjusted analysis (Table 5, Panel 1), corticosteroid use compared to non-use was associated with increased number of physician visits (SD) [10.06 (6.71) vs. 7.27 (5.97), respectively; P < 0.001], hospitalizations [0.15 (0.42) vs. 0.10 (0.10), respectively; P < 0.001], and ED visits [0.84 (1.90) vs. 0.57 (2.15), respectively; P < 0.001]. After adjustment with multivariate negative binomial regression (Table 5, Panel 2), corticosteroid use compared to non-use was associated with an increase of 2.82 physician visits (from 7.29 to 10.11, P < 0.001), an increase of 0.04 hospitalizations (from 0.11 to 0.15, P < 0.001), and an increase of 0.32 ED visits (from 0.57 to 0.89, P < 0.001).
In the unadjusted analysis (Table 5, Panel 1), corticosteroid users had higher mean costs (SD) compared to non-users for total healthcare costs [$9130.75 (21,083.24) vs. $6659.03 (24,631.57), respectively; P < 0.001], physician visits [$729.94 (715.53) vs. $570.89 (856.02), respectively; P < 0.001], ED visits [$253.56 (940.1) vs. $179.08 (893.55), respectively; P < 0.001], and medications [$1807.48 (3484.32) vs. 1311.39 (3154.19), respectively; P < 0.001]. Costs were similar between corticosteroid users and non-users for hospitalizations [$2351.68 (10,760.88) vs. $1957.77 (20,289.88), respectively; P = 0.07]. After adjusting for baseline characteristics (Table 5, Panel 2), corticosteroid users compared to non-users had higher mean costs (standard error) for total healthcare costs [$10,344.63 (268.84) vs. $7578.95 (272.88), respectively P < 0.001], physician visits [$735.91 (5.97) vs. $573.89 (9.07), respectively; P < 0.001], hospitalizations [$1661.88 (95.42) vs. $1072.92 (51.02), respectively; P < 0.001], ED visits [$273.63 (13.73) vs. $188.18 (9.67), respectively; P < 0.001], and medications [$1970.63 (52.31) vs. $1462.53 (43.11), respectively; P < 0.001].
Discussion
The current study examined the associations between corticosteroid treatment patterns and initiation of biologic DMARDs, as well as associations between corticosteroid use and adverse events, healthcare utilization and costs before initiation of biologic DMARDs. The findings indicated that compared to non-corticosteroid users, RA patients who use corticosteroids, as well as those patients who use corticosteroids for a longer duration and at lower dosages, are less likely to initiate biologic DMARDS at any particular point in time. Corticosteroid users also experienced higher incidence rates of various adverse events than non-users. Likewise, corticosteroid users compared to non-users had greater healthcare utilization and costs prior to initiating biologic DMARDS.
In contrast to Kim et al., who found that corticosteroid users were more likely than non-users to initiate biologic DMARDs, this study found that corticosteroid utilization was associated with lower likelihood of initiating a biologic DMARD, as were longer duration of corticosteroid use and lower dosage [10]. We speculate that healthcare providers and RA patients who use corticosteroids, particularly for a longer length of time and/or at recommended lower dosages, may be hesitant to disrupt a stable treatment regimen by initiating biologic DMARDs. However, this may have negative consequences for patients, as Emery et al. noted that early initiation of biologic DMARDs was associated with improved outcomes and decreased hospitalizations [30].
As previously stated, corticosteroid use has historically been associated with serious adverse events such as development or worsening of diabetes. Likewise, the current study found that corticosteroid users had greater incidence rates than non-users of an array of adverse events including cardiovascular and metabolic/endocrinologic events, and were more likely to experience an adverse event occurrence as well as an increased number of adverse events. Use of corticosteroids for a longer duration compared to shorter duration was also associated with occurrence and increased number of adverse events. These findings support the ongoing concerns regarding the safety of corticosteroids in this patient population, as well as the conservative approach to corticosteroid use adopted by the 2015 American College of Rheumatology Guideline for the Treatment of RA [1].
The issue of corticosteroid safety in RA treatment is further complicated by this study’s dosage findings, in which medium dose (defined in this study as 2.5 to < 7.5 mg/day) was associated with reduced number of adverse events compared to low dose. This seemingly contradicts recent studies of corticosteroids in RA treatment suggesting that low dosage (even in the long-term) may result in non-significant, limited or mild adverse events [5, 6, 31]. However, without full access to the medical record of individual patients, it is difficult to fully explain this finding. Another critical barrier in interpreting and comparing this finding to prior studies is the lack of a consistent definition of “low dosage.” The present study set low dose as < 2.5 mg/day, but other studies have used a higher threshold such as < 7.5 mg/day or < 10 mg/day. For example, Panoulas et al. defined low dose as < 7.5 mg compared to medium dose of ≥ 7.5 mg, and found that long-term use of medium-dose corticosteroid therapy was associated with an increased prevalence of hypertension in RA patients compared to low dose and no use groups [32]. Moreover, the literature is by no means consistent concerning low-dose corticosteroids and their association with adverse events. For example, Haraoui et al. found that, compared to non-corticosteroid users, risk of infection was significantly increased among RA patients who used corticosteroids at either lower doses (≤ 5 mg) or higher doses (> 5 mg) [33]. As such, there are challenges in understanding the nuances of how corticosteroid dosage may impact adverse events. This point is reinforced by Santiago and da Silva who cautioned that the quantity and “especially the quality of evidence are too limited to establish conclusions” concerning the safety of low-dose corticosteroid use in RA [31].
Regarding healthcare utilization, this study found that corticosteroid use compared to non-use was associated with increased number of physician visits, hospitalizations, and ED visits. This is consistent with the findings of Yazdany et al. who also found that RA patients on glucocorticoid monotherapy had increased physician visits and hospitalizations compared to those who had at least one DMARD claim [9]. Likewise, the current study found that corticosteroid users had higher total healthcare costs, as well as higher costs associated with physician visits, hospitalizations, ED visits, and medications. While the literature is more limited concerning the impact of corticosteroid use on healthcare costs in the RA population, similar findings have been noted in studies of corticosteroid use in other chronic autoimmune disease populations. For example, a study by Chen et al. among patients with systemic lupus erythematosus found that glucocorticoid users compared to non-users had significantly greater healthcare utilization and costs [34]. Although our findings suggest that RA patients who use corticosteroids incur greater healthcare utilization and costs than those who do not, the reasons for this pattern are not known. A variety of factors may play a role in this finding. Users of corticosteroids may have higher healthcare utilization and costs than nonusers because of side effects associated with the use of corticosteroids, or they may experience more severe RA than nonusers. Another possibility may be that patients were put on corticosteroids for their RA because they had pre-existing medical conditions, which their physician judged would be worsened less by corticosteroids than by DMARDs. Future prospective studies should further explore and clarify the relationship between corticosteroid use and healthcare utilization/costs among RA patients.
Limitations
This study has limitations. Due to the observational nature of the study, it was impossible to explore the clinical rationale, disease activity, and duration, and/or patient background factors that may guide the observed treatment patterns. For example, patients may be using corticosteroids because they cannot tolerate some DMARDs, or have medical conditions that could be worsened by DMARDs. Second, there is a possibility that the method of calculating corticosteroid use may underestimate or overestimate the daily dosage or duration of therapy. This is because patients may take medications at doses lower or higher than the prescribed doses in the database. Third, this study is based on administrative databases that do not include clinical parameters related to study outcomes such as body mass index, smoking status, lab tests, etc. Further, all adverse events were determined based on the claims database. Other measures such as radiograph of the spine, body weight, hemogram, and lab variables for liver and kidney functions were not available. Finally, it is challenging to establish a causal relationship based on observational analysis such as this study; prospective studies are needed to establish a causal relationship between corticosteroid use and outcomes such as adverse events and healthcare utilization and costs. Despite these limitations, the methods proposed in this study represent the state of the art for this type of research, and this study produced important findings in relation to the appropriate use of corticosteroids in RA treatment.
Conclusions
In summary, the findings indicate that RA patients who use corticosteroids, those with longer duration of use and lower dosages are less likely to initiate biologic DMARDS compared to their counterparts. RA patients who use corticosteroids and those with longer duration have increased likelihood and number of adverse events prior to initiating biologic DMARDS. Additionally, RA patients who use corticosteroids have increased healthcare utilization and costs prior to initiating biologic DMARDS. This study thus provides evidence that corticosteroid utilization may have deleterious effects on RA patient health and may increase the cost burden associated with treatment. Future studies should continue to examine the appropriate and optimal use of corticosteroids and biologic DMARDs in RA treatment.
References
Singh JA, Saag KG, Bridges SL Jr, et al. 2015 American College of Rheumatology Guidelines for the Treatment of Rheumatoid Arthritis. Arthritis Care Res. 2016;68:1–25.
Smolen JS, Landewé R, Bijlsma J, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann Rheum Dis. 2017;76:960–77.
Smolen JS, Breedveld FC, Burmester GR, et al. Treating rheumatoid arthritis to target: 2014 update of the recommendations of an international task force. Ann Rheum Dis. 2016;75:3–15.
Tanaka Y. Next stage of RA treatment: is TNF inhibitor-free remission a possible treatment goal? Ann Rheum Dis. 2013;72(Suppl 2):ii124–7.
Pincus T, Sokka T, Castrejón I, Cutolo M. Decline of mean initial prednisone dosage from 10.3 to 3.6 mg/day to treat rheumatoid arthritis between 1980 and 2004 in one clinical setting, with long-term effectiveness of dosages less than 5 mg/day. Arthritis Care Res. 2013;65:729–36.
Santiago T, da Silva JAP. Safety of low- to medium-dose glucocorticoid treatment in rheumatoid arthritis: myths and reality over the years. Ann NY Acad Sci. 2014;1318:41–9.
Harrold LR, Harrington JT, Curtis JR, et al. Prescribing practices in a US cohort of rheumatoid arthritis patients before and after publication of the American College of Rheumatology treatment recommendations. Arthritis Rheum. 2012;64:630–8.
Harrold LR, Greenberg JD, Bao Y, et al. Time to biologic therapy driven by rheumatoid arthritis disease activity and severity. Ann Rheum Dis. 2014;2014:243–4.
Yazdany J, Tonner C, Schmajuk G, Lin GA, Trivedi AN. Receipt of glucocorticoid monotherapy among Medicare beneficiaries with rheumatoid arthritis. Arthritis Care Res. 2014;66:1447–55.
Kim G, Barner JC, Rascati K, Richards K. Factors associated with the initiation of biologic disease-modifying antirheumatic drugs in Texas Medicaid patients with rheumatoid arthritis. J Manag Care Spec Pharm. 2015;21:401–7.
Caplan L, Wolfe F, Russell AS, Michaud K. Corticosteroid use in rheumatoid arthritis: prevalence, predictors, correlates, and outcomes. J Rheumatol. 2007;34:696–705.
Truven Health MarketScan Research Databases. Truven Health Analytics. 2017. http://truvenhealth.com/assets/HP_11517_0912_MarketScanResearchDatabasesForHP_SS_WEB.pdf. Accessed March 2017.
Schmajuk G, Trivedi AN, Solomon DH, et al. Receipt of disease-modifying antirheumatic drugs among patients with rheumatoid arthritis in Medicare managed care plans. JAMA. 2011;305:480–6.
Schmajuk G, Schneeweiss S, Katz JN, et al. Treatment of older adult patients diagnosed with rheumatoid arthritis: improved but not optimal. Arthritis Rheum. 2007;57:928–34.
Dixon JS, Furst DE, editors. Second-line agents in the treatment of rheumatic diseases. Inflammatory disease and therapy series. Vol. 9. New York: Marcel Dekker; 1992; p. 648.
Meikle AW, Tyler FH. Potency and duration of action of glucocorticoids. Am J Med. 1977;63:200.
Webb R, Singer M. Oxford handbook of critical care. New York: Oxford University Press; 2005.
van Staa TP, Leufkens HG, Abenhaim L, Begaud B, Zhang B, Cooper C. Use of oral corticosteroids in the United Kingdom. QJM. 2000;93:105–11.
van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Oral corticosteroids and fracture risk: relationship to daily and cumulative doses. Rheumatology. 2000;39:1383–9.
van Everdingen AA, Jacobs JW, Siewertsz Van Reesema DR, Bijlsma JW. Low-dose prednisone therapy for patients with early active rheumatoid arthritis: clinical efficacy, disease-modifying properties, and side effects: a randomized, double-blind, placebo-controlled clinical trial. Ann Intern Med. 2002;136:1–12.
Curtis JR, Westfall AO, Allison J, et al. Population-based assessment of adverse events associated with long-term glucocorticoid use. Arthritis Rheum. 2006;55:420–6.
Fardet L, Flahault A, Kettaneh A, et al. Corticosteroid-induced clinical adverse events: frequency, risk factors and patient’s opinion. Br J Dermatol. 2007;157:142–8.
Saag KG. Low-dose corticosteroid therapy in rheumatoid arthritis: balancing the evidence. Am J Med. 1997;103:31S–9S.
Saag KG, Koehnke R, Caldwell JR, et al. Low-dose long-term corticosteroid therapy in rheumatic arthritis: an analysis of serious adverse events. Am J Med. 1994;96:115–23.
Gelberg L, Andersen RM, Leake BD. The Behavioral Model for Vulnerable Populations: application to medical care use and outcomes for homeless people. Health Serv Res. 2000;34:1273–302.
Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–83.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–9.
Stuart B, Doshi JA, Briesacher B, Wrobel MV. Baysac F. Impact of prescription drug coverage on hospital and physician cost: a case study of Medicare beneficiaries with chronic obstructive pulmonary disease. Clin Ther. 2004;26:1688–99.
Centers for Medicare & Medicaid Services. 2006. Part D payment and risk adjustment. https://www.cms.gov/Medicare/Prescription-Drug-Coverage/DrugCoverageClaimsData/RxClaims_PaymentRiskAdjustment.html. Accessed March 2017.
Emery P, Solem C, Majer I, Cappelleri JC, Tarallo M. A European chart review study on early rheumatoid arthritis treatment patterns, clinical outcomes, and healthcare utilization. Rheumatol Int. 2015;35:1837–49.
Santiago T, da Silva JA. Safety of glucocorticoids in rheumatoid arthritis: evidence from recent clinical trials. NeuroImmunoModulation. 2015;22:57–65.
Panoulas VF, Douglas KM, Stavropoulos-Kalinoglou A, et al. Long-term exposure to medium-dose glucocorticoid therapy associates with hypertension in patients with rheumatoid arthritis. Rheumatology. 2008;47:72–5.
Haraoui B, Jovaisas A, Bensen WG, et al. Use of corticosteroids in patients with rheumatoid arthritis treated with infliximab: treatment implications based on a real-world Canadian population. RMD Open. 2015;1:e00078. https://doi.org/10.1136/rmdopen-2015-000078.
Chen S-Y, Choi C-B, Li Q, et al. Glucocorticoid use in patients with systemic lupus erythematosus: association between dose and health care utilization and costs. Arthritis Care Res. 2015;67:1086–94.
Acknowledgements
Funding
The design, study conduct, and financial support for the study were provided by AbbVie Inc. Article processing charges were funded by AbbVie Inc. AbbVie participated in the interpretation of data, review, and approval of the publication.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval to the version to be published. All authors had full access to all of the data in this study and take complete responsibility for the integrity of the data and accuracy of the data analysis.
Medical writing, Editorial, and Other Assistance
The authors would like to acknowledge Ms. Yanru Qiao at the University of Tennessee Health Science Center College of Pharmacy for her research assistance. This support was funded by AbbVie.
Disclosures
Junling Wang received research funding from AbbVie. Christina A. Spivey received research funding from AbbVie. Arnold Postlethwait received research funding from AbbVie. Cameron Kaplan received research funding from AbbVie. Jenny Griffith is a shareholder and employee of AbbVie. Arijit Ganguli is a shareholder and employee of AbbVie.
Compliance with Ethics Guidelines
This study was approved by the Institutional Review Board at the University of Tennessee Health Science Center.
Data Availability
We cannot share data because our data sources are proprietary. However, we have included additional details of our methods and findings in a supplementary file.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Author information
Authors and Affiliations
Corresponding author
Additional information
Enhanced content
To view enhanced content for this article go to www.medengine.com/Redeem/95FCF06043088BD4.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (https://creativecommons.org/licenses/by/4.0), which permits use, duplication, adaptation, distribution, and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Spivey, C.A., Griffith, J., Kaplan, C. et al. A Retrospective Analysis of Corticosteroid Utilization Before Initiation of Biologic DMARDs Among Patients with Rheumatoid Arthritis in the United States. Rheumatol Ther 5, 255–270 (2018). https://doi.org/10.1007/s40744-017-0089-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-017-0089-8