
Abstract
Introduction
Clinical trial findings may not be generalizable to routine practice. This study evaluated sarilumab effectiveness in patients with rheumatoid arthritis (RA) and tested the real-world applicability of a response prediction rule, derived from trial data using machine learning (based on C-reactive protein [CRP] > 12.3 mg/l and seropositivity [anticyclic citrullinated peptide antibodies, ACPA +]).
Methods
Sarilumab initiators from the ACR-RISE Registry, with ≥ 1 prescription on/after its FDA approval (2017–2020), were divided into three cohorts based on progressively restrictive criteria: Cohort A (had active disease), Cohort B (met eligibility criteria of a phase 3 trial in RA patients with inadequate response/intolerance to tumor necrosis factor inhibitors [TNFi]), and Cohort C (characteristics matched to the phase 3 trial baseline). Mean changes in Clinical Disease Activity Index (CDAI) and Routine Assessment of Patient Index Data 3 (RAPID3) were evaluated at 6 and 12 months. In a separate cohort, predictive rule was tested based on CRP levels and seropositive status (ACPA and/or rheumatoid factor); patients were categorized into rule-positive (seropositive with CRP > 12.3 mg/l) and rule-negative groups to compare the odds of achieving CDAI low disease activity (LDA)/remission and minimal clinically important difference (MCID) over 24 weeks.
Results
Among sarilumab initiators (N = 2949), treatment effectiveness was noted across cohorts, with greater improvement noted for Cohort C at 6 and 12 months. Among the predictive rule cohort (N = 205), rule-positive (vs. rule-negative) patients were more likely to reach LDA (odds ratio: 1.5 [0.7, 3.2]) and MCID (1.1 [0.5, 2.4]). Sensitivity analyses (CRP > 5 mg/l) showed better response to sarilumab in rule-positive patients.
Conclusions
In real-world setting, sarilumab demonstrated treatment effectiveness, with greater improvements in the most selective population, mirroring phase 3 TNFi-refractory and rule-positive RA patients. Seropositivity appeared a stronger driver for treatment response than CRP, although optimization of the rule in routine practice requires further data.
Plain Language Summary
Rheumatoid arthritis (RA) is a condition that may cause joint damage, if untreated. Sarilumab is an advanced medication, approved for treating moderate-to-severe RA in patients not responding to initial standard medicines. Clinical trials have shown that sarilumab improves RA symptoms; however, some people do not respond. This is a common problem in RA treatment. Physicians measure proteins in people’s blood (called biomarkers; e.g., anticyclic citrullinated peptide antibodies [ACPA], C-reactive protein [CRP], and rheumatoid factor [RF]) to predict a medicine’s response. A previous study showed that people with positive blood tests for ACPA and CRP (> 12.3 mg/l) responded well to sarilumab; this study was based on machine learning (a branch of science using computers) and identified factors that could be linked to treatment benefits. The present study analyzed routine data of 2949 people from the ACR-RISE Registry and showed an improvement in RA symptoms after 6 and 12 months of sarilumab, with a greater improvement noted in patients previously treated with other medicines. Biomarkers were tested in 205 people to check whether they could predict treatment response in day-to-day life. People were called rule-positive if they tested positive for RF and/or ACPA with CRP > 12.3 mg/l, and otherwise rule-negative. After 24 weeks of treatment, rule-positive people had a greater chance of disease improvement than rule-negative people. These results showed the benefits of sarilumab in RA in routine care and suggested the usefulness of machine learning in identifying biomarkers that physicians can use to make treatment decisions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Why carry out this study? |
Randomized controlled trials (RCTs) may lack external validity because of selection of a population based on a strict inclusion and exclusion criteria; thus, their findings may not be generalizable to routine clinical practice. |
Based on the clinical trial data, sarilumab is known to improve the signs and symptoms of rheumatoid arthritis (RA) in patients who have an inadequate response or intolerance to methotrexate or tumor necrosis factor inhibitors (TNFi); a previous analysis identified a rule based on the presence of anticyclic citrullinated peptide antibodies (ACPA) and C-reactive protein (CRP) > 12.3 mg/l that can predict treatment response to sarilumab, derived using machine learning in a clinical trial setting. |
The present study was conducted to evaluate the effectiveness of sarilumab in patients with varying disease severity and test the response predictive rule in a real-world setting. |
What was learned from the study? |
In routine clinical practice, sarilumab demonstrated treatment effectiveness, with a greater improvement noted in patients who closely resembled the clinical trial population (those having inadequate response/intolerance to TNFi). |
Furthermore, treatment responses were in favor of the patients with ACPA and CRP > 12.3 mg/dl; these findings were consistent with the response prediction rule derived from the clinical trial data, although seropositivity appeared to be a stronger driver for treatment response than CRP levels and the rule needs to be further optimized in clinical practice. |
This real-world analysis may support patients, physicians, and payers in understanding treatment response with sarilumab in routine clinical practice, based on the patients’ disease severity and biomarker status, and could help them to make informed treatment decisions. |
Introduction
Sarilumab is a human monoclonal antibody that targets the interleukin-6-receptor (IL-6R). It has demonstrated efficacy in improving the signs and symptoms along with physical function in patients with rheumatoid arthritis (RA) who had an inadequate response or intolerance to methotrexate (MTX) or tumor necrosis factor inhibitors (TNFi) in phase 3 randomized controlled trials (RCTs; MOBILITY [NCT01061736], TARGET [NCT01709578], and MONARCH [NCT02332590]) [1,2,3]. This has led to its approval for the treatment of moderate-to-severe active RA in adults having an inadequate response or intolerance to ≥ 1 disease modifying antirheumatic drugs (DMARDs) [4,5,6]. However, limited data are available regarding the effectiveness of sarilumab in a US-based routine care population.
Although RCTs are considered the gold standard for determining the efficacy of therapeutic interventions [7], they may lack external validity, owing to the strict inclusion and exclusion criteria. RCTs are conducted in a more homogeneous population and are subject to strict quality standards. On the other hand, real-world studies are based on more diverse patient populations in routine care and are dependent on various factors such as varying disease severity, patient-physician relationship, their preferences, and compliance. As a result, findings from the RCTs may not always be generalizable to routine care patients [7,8,9,10].
Literature reviews of RCTs and observational studies in RA have shown substantial differences in patient characteristics, with patients enrolled in RCTs having better prognostic factors such as younger age, shorter disease duration, and fewer comorbidities [11, 12]. In fact, various studies have shown that few RA patients in the clinical setting meet eligibility criteria for RCTs (3–7% for biologic DMARD trials and 8–44% for TNFi trials) [13,14,15,16]. Furthermore, a gap in efficacy and effectiveness has been observed in RCTs and real-world studies, with lower magnitude of improvement observed in real-world clinical practice [13, 15,16,17,18,19].
Accurate identification of patients who respond to a specific therapy can help in the rational selection of medication and optimization of the clinical response in RA [20, 21]. Machine learning (ML; using the generalized, unbiased, interaction detection, and estimation decision tree methods) was adopted to identify a rule (anticyclic citrullinated peptide antibodies positive [ACPA+] and C-reactive protein [CRP] > 12.3 mg/l) that could predict treatment response to sarilumab using datasets from four clinical trials (MOBILITY, MONARCH, TARGET, and ASCERTAIN [NCT01768572]). Overall, rule-positive patients were found to have an improved clinical response to sarilumab (an additional response of − 0.8 to − 5.4 in Clinical Disease Activity Index [CDAI] and − 0.2 to − 1.4 in 28-joint disease activity score using CRP [DAS28-CRP]) compared with rule-negative patients [22], although the rule was less applicable to the TARGET trial, which included patients having an inadequate response or intolerance to TNFi [2]. Since this treatment prediction model was developed using clinical trial data, which selected patients with elevated CRP and high disease activity at baseline [22], the findings may not be applicable to a real-world population, where patients usually have lower disease activity/CRP and have been previously treated with multiple DMARDs [11, 14].
While data from RCTs are useful to develop a prediction model, homogeneity of the enrolled study population may reduce the generalizability and utility of the model in routine practice, highlighting the need to test such models in a real-world setting [23,24,25,26]. Findings from real-world studies can complement RCTs to better understand how a treatment or prediction model performs in routine care and in subgroups of patients who may not have been included in the clinical trials.
Thus, the objectives of this study were to describe the patient population, assess the effectiveness, and test the predictive rule for sarilumab in RA in a real-world setting, using data from the American College of Rheumatology (ACR) Rheumatology Informatics System for Effectiveness (RISE) Registry [27].
Methods
Data Source and Eligibility Criteria
The current analyses were based on data obtained from the RISE Rheumatology Registry, which is the largest real-world electronic health record (EHR)-enabled and Health Insurance Portability and Accountability Act (HIPAA)-compliant Qualified Clinical Data Registry (QCDR) in the USA [27]. The analyses were approved by the local Institutional Review Board (IRB-300000748) at the University of Alabama, Birmingham (US). The study was conducted in accordance with the principles defined in the Declaration of Helsinki.
Using May 2017 to June 2020 data from the RISE Registry, sarilumab initiators were identified who had ≥ 1 prescription of sarilumab on or after May 22, 2017 (Food and Drug Administration [FDA] approval date of sarilumab); the first prescription date was the index date. Eligible patients were required to be ≥ 18 years of age on the index date, with ≥ 1 rheumatologist diagnosis for RA (during the ambulatory visit) prior to the index date, and CDAI > 10 within 30 days prior to or 7 days after the index date and/or Routine Assessment of Patient Index Data 3 (RAPID3) > 6.
Patient Characterization
Cohorts To assess baseline characteristics, all eligible sarilumab initiators were divided into four cohorts based on time since FDA approval; the overall period was divided into calendar years (2017, 2018, 2019, and through June 2020).
Outcomes Demographics and RA-related features (such as CDAI/RAPID3 scores, CRP levels, and prior and concomitant medications) were described for all patients using available data prior to sarilumab initiation. Additionally, a two-page self-reported Multidimensional Health Assessment Questionnaire (MDHAQ; derived from the Stanford Health Assessment Questionnaire) was used to measure physical function, pain, and patient global estimate, a higher score indicating poorer status [28, 29]. To measure the comorbidity burden in patients, the rheumatic disease comorbidity index (RDCI), the Elixhauser total score (both are diagnosis-based indices) [30, 31], and the Rx-Risk score (prescription-based index) [32] were measured, higher scores indicating more comorbidities.
Evaluation of Sarilumab Effectiveness
Cohorts Sarilumab effectiveness was assessed by categorizing all the initiators into three cohorts (with varying disease severity) using progressively restrictive inclusion criteria: (1) Cohort A: sarilumab initiators who had active disease, with CDAI > 10 or RAPID3 > 6, and CRP (if measured) ≥ 8 mg/l; (2) Cohort B: sarilumab initiators from Cohort A, who met the minimal eligibility criteria for the phase 3 trial [2] in RA patients, with an inadequate response or intolerance to TNFi, based on the covariates available in the RISE EHR data (female, age, White race, prior TNFi [1 and > 1], concomitant corticosteroids, rheumatoid factor [RF]-positive status, and CDAI [for CDAI cohort]); (3) Cohort C: sarilumab initiators from Cohort B, who met the minimal eligibility criteria for the phase 3 trial [2] in RA and whose characteristics were further weighted (according to the matching-adjusted indirect comparison method [33]) to balance the key covariates.
Outcomes Baseline characteristics and longitudinal change in disease activity (measured as CDAI and RAPID3) were evaluated with sarilumab treatment over 6 and 12 months (a period of ± 3 months was allowed, with closest values to 6 months in 3–9 months and 12 months in 10–15 months).
Testing Predictive Rule
A separate cohort of sarilumab initiators from the RISE Registry was included in this analysis if they had a CRP value available within 90 days prior to the index date, ≥ 1 CDAI within 6 ± 3 months after the index date, and documented serostatus (ACPA and/or RF). Also, patients should have been on treatment at the time of the second CDAI assessment.
Patient groups Patients were categorized into four groups based on the previously identified predictive rule [22]: seropositive with CRP > 12.3 mg/l (Group 1), seropositive with CRP ≤ 12.3 mg/l (Group 2), seronegative with CRP > 12.3 mg/l (Group 3), and seronegative with CRP ≤ 12.3 mg/l (Group 4). Since patients in routine care may not have ACPA measured [34, 35], the predictive rule from clinical trial data [22] was modified to include RF in the seropositive status, in line with the ACR and European Alliance of Associations for Rheumatology (EULAR) classification criteria for RA [36]; patients were defined as seropositive if they had a history of ACPA+ status or RF+ status (if laboratory results were available) or any International Classification of Diseases (ICD)-10 diagnosis code of M05 (RA patients with RF+ status). Patients who met both criteria of seropositivity and CRP > 12.3 mg/l were considered rule-positive patients (Group 1), while those not meeting these criteria were considered rule-negative patients (Groups 2, 3, and 4).
Outcomes The primary outcome of this analysis was to determine the proportion of patients achieving CDAI low disease activity (LDA) (i.e., CDAI < 10) in sarilumab “rule-positive” compared with “rule-negative” groups at 24 weeks. Secondary outcomes included the proportion of patients achieving CDAI remission (CDAI ≤ 2.8) and CDAI minimal clinically important difference (MCID) in rule-positive patients compared with rule-negative patients at 24 weeks. CDAI MCID was defined as CDAI improvement ≥ 12 if baseline CDAI was > 22 or CDAI improvement ≥ 6 if baseline CDAI was 10 < CDAI ≤ 22. Mean change in CDAI (ΔCDAI) observed in rule-positive patients was also compared with the change in rule-negative patients at 24 weeks.
An exploratory analysis was conducted to explore whether other CRP thresholds improved the performance of the rule in a real-world setting. Based on the distribution of index CRP, the median value of > 5 mg/ml observed in the entire cohort was used as a binary cut point for sensitivity analysis to ensure an even sample size. In sensitivity analysis, patients were categorized into four groups based on seropositivity and a CRP cutoff value of 5 mg/l: seropositive with CRP > 5 mg/l (Group 1), seropositive with CRP ≤ 5 mg/l (Group 2), seronegative with CRP > 5 mg/l (Group 3), and seronegative with CRP ≤ 5 mg/l (Group 4).
Outcomes were also compared between seropositive (Groups 1 and 2) and seronegative (Groups 3 and 4) groups that were pooled based on the seropositivity status, regardless of their CRP values.
Statistical Analyses
Patient characteristics were summarized for four cohorts, based on time since FDA approval, using descriptive statistics. Between-cohort comparisons were made using a chi-square test for categorical variables and a non-parametric test for continuous variables; α = 0.05 was prespecified, P ≤ α was considered significant.
For evaluation of sarilumab effectiveness, patient characteristics along with mean changes in CDAI and RAPID3 at 6 (± 3) and 12 (± 3) months were measured for each of the three cohorts: both as crude values and adjusted for age, sex, race, calendar year, seropositivity, and baseline CDAI/RAPID3.
For the patient cohort to test the predictive rule, baseline demographics and disease characteristics were separately reported as descriptive statistics. Means and standard deviations (SD) were reported for continuous variables, and percentages and numbers were reported for dichotomous or categorical variables. Logistic regression models were used to compare the odds of achieving CDAI LDA or remission, and MCID between rule-positive and rule-negative patients. A linear model was used to compare the change in CDAI from the index period to 3–9 months after the index date between rule-positive and -negative patients. The odds ratio estimates with 95% confidence intervals (CIs) were reported for CDAI LDA and MCID, while least square (LS) means and 95% CI values were reported for the change of CDAI.
All the analyses were conducted using SAS 9.4 (SAS Institute, Cary, NC, US).
Results
Patient Characterization
A total of 2949 patients with RA initiating sarilumab and treated by 585 rheumatologists were identified (Fig. 1). Overall, there was relative similarity in terms of age, sex, race, and most clinical characteristics among sarilumab initiators over the calendar time. However, patients receiving sarilumab shortly after FDA approval had more ambulatory visits (P = 0.05), greater number of previously used non-TNFi (particularly tocilizumab; P < 0.01), and higher comorbidity burden (P = 0.02); they were also more likely to be current users of opioids than sarilumab initiators in subsequent calendar years (P < 0.01) (Supplementary Material, Table S1). However, these differences in baseline characteristics did not impact treatment response to sarilumab.

Patient selection flowchart in the RISE Registry. CDAI, Clinical Disease Activity Index; CRP, C-reactive protein; ESS, effective sample size; FDA, Food and Drug Administration; Ph, phase; RA, rheumatoid arthritis; RAPID3, Routine Assessment of Patient Index Data 3
Evaluation of Sarilumab Effectiveness
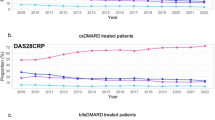
Baseline characteristics for Cohorts A, B, and C based on change in CDAI/RAPID3 at 6 (± 3) and 12 (± 3) months are summarized in Supplementary Material, Tables S2–S5. Mean baseline CDAI score varied substantially by cohort (Cohort A: 24.8 units; Cohort B: 25.0 units; and Cohort C: 42.0 units). Though improvements were noted in CDAI for all three cohorts at 6 months (Cohort A: 17.9 units; Cohort B: 17.9 units; Cohort C: 25.0 units) and 12 months (Cohort A: 16.1 units; Cohort B: 16.8 units; Cohort C: 24.6 units), both the crude and adjusted improvements were greater in Cohort C at 6 months (Cohort A: 7.1 units; Cohort B: 7.8 units; Cohort C: 18.1 units) and 12 months (Cohort A: 9.4 units; Cohort B: 5.6 units; Cohort C: 18.4 units). Mean baseline RAPID3 scores were similar for all cohorts. However, similar trends in improvement were observed in RAPID3, with the exception of Cohorts B and C at 12 months, where improvement was similar (Fig. 2).

Mean change and improvement in CDAI and RAPID3 by cohort. a Crude mean change in CDAI by cohort. b Crude mean change in RAPID3 by cohort. c Adjusteda improvement in CDAI with progressive restriction in inclusion criteria. d Adjustedb improvement in RAPID3 with progressive restriction in inclusion criteria. aAdjusted for age, sex, race, calendar year, seropositivity, and baseline CDAI. bAdjusted for age, sex, race, calendar year, seropositivity, and baseline RAPID3. CDAI, Clinical Disease Activity Index; RAPID3, Routine Assessment of Patient Index Data 3
Testing Predictive Rule
A total of 205 sarilumab initiators met the inclusion criteria for analysis of the predictive rule. Most baseline characteristics of these patients were equally distributed across the four groups in the main analysis (CRP cutoff value: 12.3 mg/l), although differences were observed in race and history of Janus kinase inhibitor (JAKi) use: the rule-positive group included a relatively higher proportion of African American patients (18.9% vs. 3.3%) and fewer patients with a history of JAKi use (34.0% vs. 51.3%) compared with rule-negative groups (Table 1 and Supplementary Material, Table S6). Similar characteristics were observed in the sensitivity analysis (CRP cutoff value: 5 mg/l) (Supplementary Material, Table S7 and Supplementary Material, Table S8).
Outcomes Outcomes assessed in the main analysis and sensitivity analysis are summarized in Table 2 and outcomes observed in the individual groups of the main analysis are shown in Supplementary Material, Table S9. At 24 weeks, a numerically higher proportion of patients (37.7%) in the rule-positive group achieved CDAI LDA compared with the pooled rule-negative group (28.9%) in the main analysis (P = 0.24). In the sensitivity analysis, 33.3% vs. 30.1% of patients achieved CDAI LDA in the rule-positive vs. rule-negative groups (P = 0.63), respectively. Furthermore, CDAI remission was numerically higher (9.4%) in the rule-positive group compared with the pooled rule-negative group (1.3%; P = 0.01) in the main analysis; a similar trend was observed in the sensitivity analysis (CRP cutoff 5 mg/ml).
CDAI MCID was achieved in 37.7% vs. 34.9% of patients in the rule-positive and rule-negative groups, respectively, in the main analysis (P = 0.71). In the sensitivity analysis, 41.7% vs. 32.3% achieved CDAI MCID (P = 0.18). ΔCDAI was also higher in the rule-positive group (mean [SD]: − 8.2 [13.9]) compared with the pooled rule-negative group (− 6.3 [13.6]) in the main analysis (P = 0.32). A similar trend was observed in the sensitivity analysis (− 8.7 [13.3] vs. − 5.8 [13.8]; P = 0.09).
Overall, logistic regression showed that, compared with rule-negative patients, rule-positive patients were more likely to reach LDA/remission and MCID in the main analysis and the sensitivity analysis, although the results were not statistically significant. The difference in ΔCDAI (LS mean [CI]) between rule-positive and rule-negative groups was − 1.2 (− 5.1, 2.7) in the main analysis and − 1.0 (− 4.6, 2.5) in the sensitivity analysis.
Furthermore, the pooled seropositive group showed better outcomes compared with the pooled seronegative group (Table 3): 4.9% vs. 0% achieved CDAI remission in the seropositive and seronegative groups, respectively. The logistic model also showed that the seropositive group was more likely to achieve CDAI LDA compared with the seronegative group (seropositive vs. seronegative group, odds ratio estimate [95% CI]: 1.7 [0.8, 3.6]). The difference in ΔCDAI (LS mean [CI]) between seropositive and seronegative groups was − 2.9 (− 7.2, 1.4).
Scatter plots showed no association between the index CRP and ΔCDAI or first CDAI observed at the 3 to 9 months follow-up (Supplementary Material, Figure S1 and Supplementary Material, Figure S2).
Discussion
Using data from the ACR-RISE Registry [27], this study showed the effectiveness of sarilumab (as noted by CDAI and RAPID3 changes over 6 and 12 months) in active RA patients. Furthermore, the predictive rule for treatment response (based on serostatus and CRP level), developed based on the RCT data [22], was consistent in the real-world setting. Extending the sarilumab effectiveness and utility of the response predictive rule in a real-world practice-based large US registry, beyond the evidence produced in the RCTs, allows a better understanding for guiding treatment choices [26, 37].
The present study included patients with active RA who had received multiple biologics or targeted therapies compared with the previous clinical trials [1,2,3, 38, 39]. Such patients tend to have more severe disease over time, which may lead to poorer treatment outcomes [40, 41]. In this study, modest evidence was observed for channeling of patients to sarilumab shortly after its approval. However, all cohorts (based on progressively restrictive inclusion criteria) demonstrated treatment effectiveness, and there was no impact of calendar year on the treatment response; this highlights the well-established efficacy of sarilumab in patients with RA [1, 3, 38, 39]. Furthermore, the greatest improvements were seen in the cohort that had the highest baseline CDAI score and mirrored the phase 3 trial population in TNFi inadequate responders, consistent with the literature evidence [2, 42, 43]. This could be due to the more selective nature of the clinical trial population, in which better treatment responses are noted than the real-world setting [13, 15,16,17].
Furthermore, owing to the heterogeneity seen in RA treatment response [44, 45], it has become important to characterize the factors that can help to optimize the treatment for maximum benefit while minimizing the associated toxicities. Challenges in identifying the right drug for the right patient have led to significant efforts in the investigation of treatment response predictors in RA, including genomic, protein, and flow cytometry biomarkers [46]. However, each method has few limitations, preventing their clinical utility. Genomic markers may not be applicable to different ethnic groups or may be too weak to contribute to treatment selection for individual patients [47,48,49,50], whereas flow cytometry and protein biomarkers may not be suitable in clinical practice due to requirement of complex laboratory analyses [51]. Other tools to enable precision medicine and rational drug selection in RA (such as ribonucleic acid [RNA] sequencing or molecular signature response classifier) either remain in development or are newly available but have not yet entered mainstream clinical practice [52,53,54,55,56]. ML, a subfield of artificial intelligence (AI), seems promising in predicting treatment response in RA patients, and thus, can be helpful in finding biomarkers of response [50, 57,58,59].
The strength of the current analyses is that the predictive rule tested in this study was derived from ML using clinical trial data [22] and was based on parameters routinely assessed in clinical practice, such as RF and ACPA [60] as well as one of the most used clinical biomarkers, i.e., CRP [61]. To date, available evidence on the association of these individual variables (ACPA, RF, and CRP) with RA treatment response is mixed, showing both positive [21, 62,63,64] or no/negative associations [65,66,67].
A post hoc analysis from the AVERT trial showed that ACPA status at baseline may serve as a predictor for achieving remission (CDAI, simplified disease activity index [SDAI], Boolean, and DAS28-CRP) at 1 year for abatacept plus MTX (in combination) but may not predict response for abatacept or MTX monotherapies [68, 69], while other studies showed that RF/ACPA+ patients had better treatment response to bDMARDs (such as rituximab or infliximab) than ACPA-RA patients [62, 63, 70]. Several other studies showed no or a negative association between seropositivity and treatment response for MTX and TNFi [65, 67, 71]. Studies on the predictive value of serostatus on clinical response to treatment with IL-6R inhibitors were also less conclusive. A meta-analysis showed RF positivity as a predictor of better clinical response (ACR20: odds ratio [OR]: 1.51 [1.21, 1.90]) in six studies with tocilizumab [72]. In contrast, a retrospective study (n = 204) of tocilizumab showed no correlation between seropositivity and EULAR response (RF+ P = 0.18; ACPA+ P = 0.12) or remission (RF+ P = 0.39; ACPA+ P = 0.36) after 6 months of treatment [73].
Evidence for the impact of CRP levels on treatment response is also not well established. In a prospective study, high pretreatment CRP levels resulted in better treatment response to higher doses of infliximab than low pretreatment CRP levels [74], whereas distinct CRP patterns were seen in infliximab non-responders in another study: failure to achieve CRP suppression at Week 2 predicted non-response at Week 12, but CRP suppression at Week 12 predicted a late response to infliximab upon the continuation of treatment [75]. Another retrospective study of tocilizumab showed a positive correlation between high baseline CRP levels and EULAR response (OR: 4.45 [1.45, 13.73]) at 6 months [73].
The present study provides insights on the effectiveness of sarilumab in routine clinical practice and attempts to fill the literature gaps on the prognostic values of ACPA, RF, and CRP for treatment response. However, this study had some limitations. In the current analysis, patients had to be on therapy for 6 and 12 months, which could represent selection bias. Also, the results were inconsistent as the statistical significance was noted for remission but not for LDA, MCID, and change in CDAI. Furthermore, serostatus (ACPA+ and/or RF+) appeared to differentiate patients better than the overall rule for change in CDAI. The study demonstrated that the CDAI changes/measures were not dependent on the index CRP values. Though similar trends were observed in the current analyses with both the evaluated cutoff values of CRP (12.3 mg/l and 5 mg/l), more studies with a larger sample size are needed to validate these findings and verify the potential contribution of a CRP optimal cutoff. The duration of clinical response improvement beyond 6–12 months and differentiation of rule outcomes for various drugs also remain to be elucidated.
Conclusions
Treatment with sarilumab was effective in the real-world setting, with greater improvement seen in the most selective population, mirroring the TNF-refractory phase 3 population. Also, treatment responses were in favor of the patients with seropositive status and elevated CRP, with seropositivity appearing as a stronger driver. Overall, serostatus and CRP levels may help in identifying subpopulations of RA patients who are more likely to respond to sarilumab, which may help physicians tailor treatment for individual patients based on their clinical characteristics. Further work is needed to optimize the rule for clinical practice.
Change history
13 November 2023
A Correction to this paper has been published: https://doi.org/10.1007/s40744-023-00607-4
References
Genovese MC, Fleischmann R, Kivitz AJ, et al. Sarilumab plus methotrexate in patients with active rheumatoid arthritis and inadequate response to methotrexate: results of a phase III study. Arthritis Rheumatol (Hoboken, NJ). 2015;67(6):1424–37.
Fleischmann R, van Adelsberg J, Lin Y, et al. Sarilumab and nonbiologic disease-modifying antirheumatic drugs in patients with active rheumatoid arthritis and inadequate response or intolerance to tumor necrosis factor inhibitors. Arthritis Rheumatol (Hoboken, NJ). 2017;69(2):277–90.
Burmester GR, Lin Y, Patel R, et al. Efficacy and safety of sarilumab monotherapy versus adalimumab monotherapy for the treatment of patients with active rheumatoid arthritis (MONARCH): a randomised, double-blind, parallel-group phase III trial. Ann Rheum Dis. 2017;76(5):840–7.
Lamb YN, Deeks ED. Sarilumab: A review in moderate-to-severe rheumatoid arthritis. Drugs. 2018;78(9):929–40.
Electronic Medicines Compendium. Kevzara 200 mg solution for injection in pre-filled pen. 2023. https://www.medicines.org.uk/emc/product/8145/smpc#gref. Accessed 18 Jan 2023.
Prescribing information. KEVZARA (sarilumab) injection, for subcutaneous use. 2018. https://products.sanofi.us/kevzara/kevzara.pdf. Accessed 18 Jan 2023.
Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–94.
Monti S, Grosso V, Todoerti M, Caporali R. Randomized controlled trials and real-world data: differences and similarities to untangle literature data. Rheumatology (Oxford). 2018;57(57 Suppl 7):vii54–8.
Rothwell PM. External validity of randomised controlled trials: “To whom do the results of this trial apply?” Lancet. 2005;365(9453):82–93.
Blonde L, Khunti K, Harris SB, Meizinger C, Skolnik NS. Interpretation and impact of real-world clinical data for the practicing clinician. Adv Ther. 2018;35(11):1763–74.
Kilcher G, Hummel N, Didden EM, Egger M, Reichenbach S, GetReal Work Package. Rheumatoid arthritis patients treated in trial and real world settings: comparison of randomized trials with registries. Rheumatology (Oxford). 2018;57(2):354–69.
Palmowski A, Buttgereit T, Palmowski Y, et al. Applicability of trials in rheumatoid arthritis and osteoarthritis: a systematic review and meta-analysis of trial populations showing adequate proportion of women, but underrepresentation of elderly people. Semin Arthritis Rheum. 2019;48(6):983–9.
Sugano E, Tanaka E, Inoue E, et al. Differences in patients’ population and efficacy/effectiveness of biologic disease-modifying antirheumatic drugs between randomized controlled trials and real-world settings in patients with rheumatoid arthritis - using the IORRA cohort. Mod Rheumatol. 2021;32(4):675–85.
Vashisht P, Sayles H, Cannella AC, Mikuls TR, Michaud K. Generalizability of patients with rheumatoid arthritis in biologic agent clinical trials. Arthritis Care Res. 2016;68(10):1478–88.
Aaltonen KJ, Ylikyla S, Tuulikki Joensuu J, et al. Efficacy and effectiveness of tumour necrosis factor inhibitors in the treatment of rheumatoid arthritis in randomized controlled trials and routine clinical practice. Rheumatology (Oxford). 2017;56(5):725–35.
Zink A, Strangfeld A, Schneider M, et al. Effectiveness of tumor necrosis factor inhibitors in rheumatoid arthritis in an observational cohort study: comparison of patients according to their eligibility for major randomized clinical trials. Arthritis Rheumatol. 2006;54(11):3399–407.
Kievit W, Fransen J, Oerlemans AJ, et al. The efficacy of anti-TNF in rheumatoid arthritis, a comparison between randomised controlled trials and clinical practice. Ann Rheum Dis. 2007;66(11):1473–8.
Martin K, Bentaberry F, Dumoulin C. Effectiveness and safety profile of leflunomide in rheumatoid arthritis: actual practice compared with clinical trials. Clin Exp Rheumatol. 2005;23(1):80–4.
Wolfe F, Michaud K. Towards an epidemiology of rheumatoid arthritis outcome with respect to treatment: randomized controlled trials overestimate treatment response and effectiveness. Rheumatology (Oxford). 2005;44 Suppl 4:iv18–22.
Ouboussad L, Burska AN, Melville A, Buch MH. Synovial issue heterogeneity in rheumatoid arthritis and changes with biologic and targeted synthetic therapies to inform stratified therapy. Front Med. 2019;6:45.
Wijbrandts CA, Tak PP. Prediction of response to targeted treatment in rheumatoid arthritis. Mayo Clin Proc. 2017;92(7):1129–43.
Rehberg M, Giegerich C, Praestgaard A, et al. Identification of a rule to predict response to sarilumab in patients with rheumatoid arthritis using machine learning and clinical trial data. Rheumatol Ther. 2021;8(4):1661–75.
Coquet J, Bievre N, Billaut V, et al. Assessment of a clinical trial-derived survival model in patients with metastatic castration-resistant prostate cancer. JAMA Netw Open. 2021;4(1): e2031730.
Yan AT, Jong P, Yan RT, et al. Clinical trial-derived risk model may not generalize to real-world patients with acute coronary syndrome. Am Heart J. 2004;148(6):1020–7.
Selby JV, Fireman BH. Building predictive models for clinical care-where to build and what to predict? JAMA Netw Open. 2021;4(1): e2032539.
Johansson FD, Collins JE, Yau V, et al. Predicting response to tocilizumab monotherapy in rheumatoid arthritis: a real-world data analysis using machine learning. J Rheumatol. 2021;48(9):1364–70.
American College of Rheumatology. RISE (Qualified Clinical Data Registry). https://www.rheumatology.org/Practice-Quality/RISE-Registry. Accessed 18 Jan 2023.
Pincus T, Yazici Y, Bergman M. A practical guide to scoring a Multi-Dimensional Health Assessment Questionnaire (MDHAQ) and Routine Assessment of Patient Index Data (RAPID) scores in 10–20 seconds for use in standard clinical care, without rulers, calculators, websites or computers. Best Pract Res Clin Rheumatol. 2007;21(4):755–87.
Pincus T, Swearingen C, Wolfe F. Toward a multidimensional Health Assessment Questionnaire (MDHAQ): assessment of advanced activities of daily living and psychological status in the patient-friendly health assessment questionnaire format. Arthritis Rheumatol. 1999;42(10):2220–30.
England BR, Sayles H, Mikuls TR, Johnson DS, Michaud K. Validation of the rheumatic disease comorbidity index. Arthritis Care Res. 2015;67(6):865–72.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36(1):8–27.
Pratt NL, Kerr M, Barratt JD, et al. The validity of the Rx-risk Comorbidity Index using medicines mapped to the Anatomical Therapeutic Chemical (ATC) Classification System. BMJ Open. 2018;8(4): e021122.
Signorovitch JE, Sikirica V, Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15(6):940–7.
Conrad K, Roggenbuck D, Reinhold D, Dorner T. Profiling of rheumatoid arthritis associated autoantibodies. Autoimmun Rev. 2010;9(6):431–5.
Tenstad HB, Nilsson AC, Dellgren CD, Lindegaard HM, Rubin KH, Lillevang ST. Use and utility of serologic tests for rheumatoid arthritis in primary care. Dan Med J. 2020;67(2):A05190318.
Aletaha D, Neogi T, Silman AJ, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheumatol. 2010;62(9):2569–81.
Tony HP, Feist E, Aries PM, et al. Sarilumab reduces disease activity in rheumatoid arthritis patients with inadequate response to janus kinase inhibitors or tocilizumab in regular care in Germany. Rheumatol Adv Pract. 2022;6(1):rkac002.
Genovese MC, Fleischmann R, Kivitz A, et al. Efficacy and safety of sarilumab in combination with csDMARDs or as monotherapy in subpopulations of patients with moderately to severely active rheumatoid arthritis in three phase III randomized, controlled studies. Arthritis Res Ther. 2020;22(1):139.
Genovese MC, van der Heijde D, Lin Y, et al. Long-term safety and efficacy of sarilumab plus methotrexate on disease activity, physical function and radiographic progression: 5 years of sarilumab plus methotrexate treatment. RMD Open. 2019;5(2): e000887.
Aletaha D, Maa JF, Chen S, et al. Effect of disease duration and prior disease-modifying antirheumatic drug use on treatment outcomes in patients with rheumatoid arthritis. Ann Rheum Dis. 2019;78(12):1609–15.
Choy E, Groves L, Sugrue D, et al. Outcomes in rheumatoid arthritis patients treated with abatacept: a UK multi-centre observational study. BMC Rheumatol. 2021;5(1):3.
Fleischmann R, Genovese MC, Maslova K, Leher H, Praestgaard A, Burmester GR. Long-term safety and efficacy of sarilumab over 5 years in patients with rheumatoid arthritis refractory to TNF inhibitors. Rheumatology (Oxford). 2021;60(11):4991–5001.
Strand V, Reaney M, Chen CI, et al. Sarilumab improves patient-reported outcomes in rheumatoid arthritis patients with inadequate response/intolerance to tumour necrosis factor inhibitors. RMD Open. 2017;3(1): e000416.
Goetz I, Carter GC, Lucero M, et al. Review of treatment response in rheumatoid arthritis: assessment of heterogeneity. Curr Med Res Opin. 2011;27(4):697–711.
Blair JPM, Bay-Jensen AC, Tang MH, et al. Identification of heterogenous treatment response trajectories to anti-IL6 receptor treatment in rheumatoid arthritis. Sci Rep. 2020;10(1):13975.
Romão VC, Vital EM, Fonseca JE, Buch MH. Right drug, right patient, right time: aspiration or future promise for biologics in rheumatoid arthritis? Arthritis Res Ther. 2017;19(1):239.
Sode J, Vogel U, Bank S, et al. Anti-TNF treatment response in rheumatoid arthritis patients is associated with genetic variation in the NLRP3-inflammasome. PLoS ONE. 2014;9(6): e100361.
Weyand CM, Klimiuk PA, Goronzy JJ. Heterogeneity of rheumatoid arthritis: from phenotypes to genotypes. Springer Semin Immunopathol. 1998;20:5–22.
Yamamoto K, Okada Y, Suzuki A, Kochi Y. Genetic studies of rheumatoid arthritis. Proc Jpn Acad Ser B Phys Biol Sci. 2015;91(8):410–22.
Guan Y, Zhang H, Quang D, et al. Machine learning to predict anti–tumor necrosis factor drug responses of rheumatoid arthritis patients by integrating clinical and genetic markers. Arthritis Rheumatol. 2019;71(12):1987–96.
Lequerré T, Rottenberg P, Derambure C, Cosette P, Vittecoq O. Predictors of treatment response in rheumatoid arthritis. Jt Bone Spine. 2019;86(2):151–8.
Humby F, Durez P, Buch MH, et al. Rituximab versus tocilizumab in anti-TNF inadequate responder patients with rheumatoid arthritis (R4RA): 16-week outcomes of a stratified, biopsy-driven, multicentre, open-label, phase 4 randomised controlled trial. Lancet. 2021;397(10271):305–17.
Bergman MJ, Kivitz AJ, Pappas DA, et al. Clinical utility and cost savings in predicting inadequate response to anti-TNF therapies in rheumatoid arthritis. Rheumatol Ther. 2020;7(4):775–92.
Cohen S, Wells AF, Curtis JR, et al. A molecular signature response classifier to predict inadequate response to tumor necrosis factor-α inhibitors: The NETWORK-004 Prospective Observational Study. Rheumatol Ther. 2021;8(3):1159–76.
Mellors T, Withers JB, Ameli A, et al. Clinical validation of a blood-based predictive test for stratification of response to tumor necrosis factor inhibitor therapies in rheumatoid arthritis patients. Netw Syst Med. 2020;3(1):91–104.
Strand V, Zhang L, Arnaud A, Connolly-Strong E, Asgarian S, Withers JB. Improvement in clinical disease activity index when treatment selection is informed by the tumor necrosis factor-a inhibitor molecular signature response classifier: analysis from the Study to Accelerate Information of Molecular Signatures in Rheumatoid Arthritis. Expert Opin Biol Ther. 2022;26(6):801–7.
Hügle M, Omoumi P, van Laar JM, Boedecker J, Hügle T. Applied machine learning and artificial intelligence in rheumatology. Rheumatol Adv Pract. 2020;4(1):rkaa005.
Koo BS, Eun S, Shin K, et al. Machine learning model for identifying important clinical features for predicting remission in patients with rheumatoid arthritis treated with biologics. Arthritis Res Ther. 2021;23(1):178.
Vodencarevic A, Tascilar K, Hartmann F, et al. Advanced machine learning for predicting individual risk of flares in rheumatoid arthritis patients tapering biologic drugs. Arthritis Res Ther. 2021;23(1):67.
de Brito RS, Baldo DC, Andrade LEC. Clinical and pathophysiologic relevance of autoantibodies in rheumatoid arthritis. Adv Rheumatol. 2019;59(1):2.
Pope JE, Choy EH. C-reactive protein and implications in rheumatoid arthritis and associated comorbidities. Semin Arthritis Rheum. 2021;51(1):219–29.
Klaasen R, Cantaert T, Wijbrandts CA, et al. The value of rheumatoid factor and anti-citrullinated protein antibodies as predictors of response to infliximab in rheumatoid arthritis: an exploratory study. Rheumatology. 2011;50(8):1487–93.
Chatzidionysiou K, Lie E, Nasonov E, et al. Highest clinical effectiveness of rituximab in autoantibody-positive patients with rheumatoid arthritis and in those for whom no more than one previous TNF antagonist has failed: pooled data from 10 European registries. Ann Rheum Dis. 2011;70(9):1575–80.
Westhovens R, van Vollenhoven RF, Boumpas DT, et al. The early clinical course of infliximab treatment in rheumatoid arthritis: results from the REMARK observational study. Clin Exp Rheumatol. 2014;32(3):315–23.
Potter C, Hyrich KL, Tracey A, et al. Association of rheumatoid factor and anti-cyclic citrullinated peptide positivity, but not carriage of shared epitope or PTPN22 susceptibility variants, with anti-tumour necrosis factor response in rheumatoid arthritis. Ann Rheum Dis. 2009;68(1):69–74.
Chen Y-M, Chen H-H, Huang W-N, et al. Tocilizumab potentially prevents bone loss in patients with anticitrullinated protein antibody-positive rheumatoid arthritis. PLoS One. 2017;12(11):e0188454-e.
van den Broek M, Dirven L, Klarenbeek N, et al. The association of treatment response and joint damage with ACPA-status in recent-onset RA: a subanalysis of the 8-year follow-up of the BeSt study. Ann Rheum Dis. 2012;71(2):245–8.
Archer R, Hock E, Hamilton J, et al. Assessing prognosis and prediction of treatment response in early rheumatoid arthritis: systematic reviews. Health Technol Assess (Winchester, England). 2018;22(66):1–294.
Huizinga TWJ, Connolly SE, Johnsen A, et al. THU0114 Effect of anti-cyclic citrullinated peptide 2 immunoglobulin M serostatus on efficacy outcomes following treatment with abatacept plus methotrexate in the Avert Trial. BMJ. 2015;74(Suppl 2):234–5.
Couderc M, Mathieu S, Pereira B, Glace B, Soubrier M. Predictive factors of rituximab response in rheumatoid arthritis: results from a French university hospital. Arthritis Care Res (Hoboken). 2013;65(4):648–52.
Lv Q, Yin Y, Li X, et al. The status of rheumatoid factor and anti-cyclic citrullinated peptide antibody are not associated with the effect of anti-TNFα agent treatment in patients with rheumatoid arthritis: a meta-analysis. PLoS ONE. 2014;9(2): e89442.
Maneiro RJ, Salgado E, Carmona L, Gomez-Reino JJ. Rheumatoid factor as predictor of response to abatacept, rituximab and tocilizumab in rheumatoid arthritis: Systematic review and meta-analysis. Semin Arthritis Rheum. 2013;43(1):9–17.
Pers Y-M, Fortunet C, Constant E, et al. Predictors of response and remission in a large cohort of rheumatoid arthritis patients treated with tocilizumab in clinical practice. Rheumatology. 2013;53(1):76–84.
Wolbink GJ, Voskuyl AE, Lems WF, et al. Relationship between serum trough infliximab levels, pretreatment C reactive protein levels, and clinical response to infliximab treatment in patients with rheumatoid arthritis. Ann Rheum Dis. 2005;64(5):704–7.
Buch MH, Seto Y, Bingham SJ, et al. C-reactive protein as a predictor of infliximab treatment outcome in patients with rheumatoid arthritis: defining subtypes of nonresponse and subsequent response to etanercept. Arthritis Rheumatol. 2005;52(1):42–8.
Acknowledgements
The authors thank all patients, investigators, and associated staff for their participation in this study.
Funding
Funding for these analyses, and the journal’s Rapid Service fee, was provided by Sanofi and Regeneron Pharmaceuticals.
Medical Writing Assistance
Medical writing assistance was provided by Vasudha Chachra and Sindhu Doppalapudi of Sanofi and funded by Sanofi.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as whole, and have given their approval for this version to be published.
Author Contributions
Jeffrey R Curtis, Huifeng Yun, Lang Chen, Amy Praestgaard, and Markus Rehberg contributed to the conception and design of the work, data acquisition, and data analysis/interpretation; Stefano Fiore, Kerri Ford, and Ernest Choy contributed to the conception and design of the work and data analysis/interpretation; Stephanie S Ford contributed to the conception and design of the work, and data acquisition; and Hubert van Hoogstraten contributed to the data analysis/interpretation. All authors reviewed and approved this manuscript for submission.
Prior Presentation
Data in part were presented at European Alliance of Associations for Rheumatology (EULAR) 2021 (June 02–05, 2021; Virtual) and American College of Rheumatology (ACR) Convergence 2021 (November 01–10, 2021; Virtual).
Disclosures
Jeffrey R Curtis received grants/contract from AbbVie, Amgen, BMS, Corrona, Eli Lilly, Janssen, Myriad, Novartis, Pfizer, Sanofi, and UCB; and consulting fees from AbbVie, Amgen, BMS, Corrona, Eli Lilly, Janssen, Myriad, Novartis, Pfizer, Roche, Sanofi, Scipher, and UCB. Huifeng Yun received grant from Pfizer, and recently joined GSK, but all work was completed at UAB. Lang Chen and Stephanie S Ford have nothing to disclose. Hubert van Hoogstraten, Stefano Fiore, Kerri Ford, Amy Praestgaard, and Markus Rehberg are employees of Sanofi and may hold stock/stock options in the company. Ernest Choy received grants or contracts from AbbVie, Amgen, AstraZeneca, Biogen, Bio-Cancer, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Chelsea Therapeutics, Chugai Pharma, Daiichi Sankyo, Eli Lilly, Ferring Pharmaceuticals, Gilead, GlaxoSmithKline, Hospira Pharmaceuticals, Ionis Pharmaceuticals, Janssen, Jazz Pharmaceuticals, MedImmune, Merck Sharp & Dohme, Merrimack Pharmaceuticals, Napp, Novartis, Novimmune, ObsEva, Pfizer, R-Pharm, Regeneron Pharmaceuticals, Inc., Roche, Sanofi Genzyme, SynAct Pharma, Tonix, and UCB; received consulting fees from AbbVie, Amgen, AstraZeneca, Biogen, Bio-Cancer, Boehringer Ingelheim, Bristol-Myers Squibb, Celgene, Chelsea Therapeutics, Chugai Pharma, Daiichi Sankyo, Eli Lilly, Ferring Pharmaceuticals, Gilead, GlaxoSmithKline, Hospira Pharmaceuticals, Ionis Pharmaceuticals, Janssen, Jazz Pharmaceuticals, MedImmune, Merck Sharp & Dohme, Merrimack Pharmaceuticals, Napp, Novartis, Novimmune, ObsEva, Pfizer, R-Pharm, Regeneron Pharmaceuticals, Inc., Roche, Sanofi Genzyme, SynAct Pharma, Tonix, and UCB; received honoraria from Amgen, Boehringer Ingelheim, Bristol-Myers Squibb, Chugai Pharma, Eli Lilly, Hospira, Merck Sharp & Dohme, Novartis, Pfizer, Regeneron Pharmaceuticals, Inc., Roche, Sanofi-Aventis, and UCB.
Compliance with Ethics Guidelines
This study is based on the data from the RISE Registry, the first and largest electronic health record-enabled rheumatology registry in the United States and does not contain any new studies with human participants. The analyses were approved by the local Institutional Review Board (IRB-300000748) at the University of Alabama, Birmingham, Alabama, USA. The study was conducted in accordance with the principles defined in the Declarations of Helsinki.
Data Availability
The data collected and used in this analysis were supported by the American College of Rheumatology (ACR) Rheumatology Informatics System for Effectiveness (RISE) Registry. The views expressed represent those of the authors and do not necessarily represent the views of the ACR.
Author information
Authors and Affiliations
Corresponding author
Additional information
Huifeng Yun: Affiliation at the time of the study, currently an employee of GSK and an adjunct professor at the University of Alabama at Birmingham.
Lang Chen: Affiliation at the time of study.
The original online version of this article was revised: To update the supplement files.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Curtis, J.R., Yun, H., Chen, L. et al. Real-World Sarilumab Use and Rule Testing to Predict Treatment Response in Patients with Rheumatoid Arthritis: Findings from the RISE Registry. Rheumatol Ther 10, 1055–1072 (2023). https://doi.org/10.1007/s40744-023-00568-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40744-023-00568-8