
Abstract
Introduction
The aim of this work is to evaluate whether the addition of home oxygen therapy (HOT) would reduce readmission in chronic obstructive pulmonary disease (COPD) patients.
Methods
PubMed, ScopeMed, Cochrane, Scopus, and Google Scholar databases were searched. The search strategy used the following keywords “chronic obstructive pulmonary disease”, the intervention “long-term oxygen therapy”, and the outcome “readmission” combined with the AND operator. The Newcastle–Ottawa Scale and Jadad Scale were used for assessing the quality of cohort studies and clinical trials, respectively. A random-effects model was employed in this study after calculating the standard errors by 95% confidence intervals. The I2 statistic and Cochran’s Q-test were used to measure heterogeneity. To address heterogeneity, subgroup analyses were carried out according to the length of LTOT, which was classified as “over 8 months” and “under 8 months”.
Results
Seven studies were included in the analysis. In the pooled analysis, the RR [CI95%, p value], heterogeneity criteria for readmission reduced by 1.542 [1.284–1.851, < 0.001], I2 = 60%, and 1.693 [1.645–1.744, < 0.001], I2 = 60% for patients with a length of LTOT treatment under and above 8 months, respectively. A sensitivity analysis was conducted by systematically omitting each study, and it showed no influential studies. Egger’s test indicated no publication bias (p = 0.64).
Conclusions
Based on our results in this systematic review, long-tern oxygen therapy (LTOT) at home was associated with a significantly lower risk ratio of hospital readmission. However, the sample sizes in the studies necessitate larger RCTs to evaluate the effect of LTOT on readmission in COPD patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Chronic obstructive pulmonary disease (COPD) is at a higher level and more advanced staging of spirometricallly confirmed than has been typically reported. |
It is associated with increased morbidity, mortality, hospitalization, healthcare burden, substantial societal burden, and impaired quality of life. |
In an attempt to combat COPD-related hospitalization, researchers have studied the effects of oxygen therapy. Long-term oxygen therapy (LTOT) has been revealed to improve the survival and life quality of COPD patients and stabilize pulmonary hypertension in these patients. |
This systematic review evaluated based on the hypothesis that the addition of HOT would reduce readmission for COPD patients to provide evidence on appropriate indications for HOT. |
Based on our results in this systematic review, LTOT at home was associated with a significantly lower risk ratio of hospital readmission in COPD patients. |
Introduction
Globally, exacerbation is an event of considerable importance in the course of chronic obstructive pulmonary disease (COPD). It is associated with increased morbidity, mortality, hospitalization, impaired quality of life, increased healthcare burden, and substantial societal burden [1, 2]. Hence, it is viewed as a severe public health problem in many countries.
Based on the projection model in 12 Asian countries, it was estimated that 56.6 million people aged 30 years and above were suffering from moderate-to-severe COPD [3]. The World Health Organization (WHO) projects that COPD will be the third main cause of death worldwide by the year 2030, followed by ischemic heart disease and cerebrovascular disease [4].
In an attempt to combat COPD-related hospitalization, researchers have evaluated the results of oxygen therapy in these patients. Long-term oxygen therapy (LTOT) has been shown to improve life quality and survival in COPD patients and stabilize their pulmonary hypertension [5,6,7].
Home oxygen therapy (HOT) is the at-home administration of oxygen at concentrations greater than the ambient air concentration. Nevertheless, findings regarding the effect of HOT on hospitalization are diverse. While several studies have designated that LTOT reduces hospital admissions [8, 9], one study presented no effect [10]. Most studies indicated that LTOT had an impact on hospital admission, especially since the greatest association has been detected among severely hypoxemic COPD patients [11]. However, in moderately hypoxemic COPD patients, HOT may not lessen hospitalizations [10]. On the other hand, hospital admission is more likely in LTOT users and inappropriate oxygen consumption can impose an additional financial burden on the patient [12]. It would be mentioned that prescriptions for oxygen therapy are circumstances that predispose patients to repeated hospital admissions [13, 14].
This systematic review was evaluated based on the hypothesis that the addition of HOT would reduce readmission for COPD patients to provide evidence on appropriate indications for HOT.
Methods
Search Strategy and Selection
The search strategy for the retrieval of English articles was made by three main concepts and their synonyms, including the problem “chronic obstructive pulmonary disease”, the intervention “long-term oxygen therapy”, and the outcome “readmission” combined with the AND operator. The synonyms of this concept were extracted from thesauruses like Medical Subject Headings (MeSH) and EMtree. The search strategy used for databases is shown in the supporting information (Table 1).
We searched multiple international scientific databases (PubMed, Medline, ISI-Web of Science-Core Collection, Scopus, Cochrane Central Register of Controlled Trials, and Embase). We did not consider any time limitation and all published studies from inception to September 2020 were included in this study. However, the records are limited to research articles and articles in the English language.
Study Selection and Eligibility Criteria
Duplicate papers were removed, and the selection of suitable studies was conducted in three phases. In the first and second phases, titles and abstracts of papers were screened, and irrelevant papers were excluded. In the last phase, the full text of identified papers was explored deeply to select only relevant papers. Two independent reviewers did all three screening phases. Discrepancies were resolved by consultation and consensus.
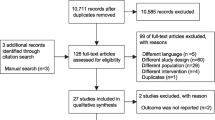
The number of searched articles and articles in each step was defined in the PRISMA diagram (Fig. 1). Prescribing criteria for oxygen therapy was according to PaO2 ≤ 55 mmHg (7.3 kPa) or oxygen saturation as measured by pulse oximetry (SpO2) ≤ 88%; or PaO2 = 56–59 mmHg (7.5–7.9 kPa) or SpO2 = 89% plus one of the following: edema, hematocrit ≥ 55%, or P pulmonale on an ECG [15, 16]. LTOT is prescribed for at least 15 h/day. patients’ hours of oxygen use [15, 16].

Flow diagram of study selection process
Quality Assessment
Cohort studies were assessed by the Newcastle–Ottawa and Jaded Scale, which evaluate the description of randomization, blinding, and dropouts used to assess the clinical trial (Tables 2, 3).
Data Extraction and Abstraction
To extract and summarize the data, we developed an extraction form (Table 4). This form contained several elements including name, country, and period in which the model was operating. Two independent reviewers did all screening phases. Discrepancies were resolved by consultation and consensus.
Statistical Analysis
For the meta-analysis of case–control studies, RR was transformed to natural logarithms and the 95% confidence intervals (CIs) were used to calculate the standard errors. We assumed that the true effect could vary between studies. Thus, we employed a random-effects model. We used the I2 statistic and Cochran’s Q-test to measure heterogeneity. A significant Q test (p value < 0.05) or I2 > 50% indicated the presence of heterogeneity [17].
To address heterogeneity, we carried out subgroup analyses using the following comparison groups: length of LTOT; over and under 8 months.
Sensitivity analyses were conducted by omitting each study to test the stability of the results. Finally, publication bias was evaluated using the funnel plot and Egger’s test [18].
These analyses were conducted using the software Comprehensive Meta-Analysis version 3.
Ethics
The Research Committee of Isfahan University of Medical Sciences approved the study protocol, and the Ethics Committee confirmed it (IR.MUI.MED.REC.1399.040). This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the authors.
Results
Literature Search Results
A total of 687 studies were identified using keywords in the initial database search. After the removal of duplicate articles and reviewing 428 titles and abstracts, 108 full-text articles were retrieved and assessed for eligibility. During the processing process, the two reviewers had no disagreement on involving studies and 14 studies met the inclusion criteria in the qualitative analysis. After failing to receive the data required to perform the analysis for one study, seven studies were included in our final quantitative analysis.
Sub-group analysis has been performed based on the length of LTOT; over and under 8 months (Fig. 2). Information on the seven studies that met the eligibility criteria is shown in Table 4. All of the variables such as sex, age, COPD grade, smoking, FEV1, outcome, and length of LTOT treatment were entered systematically and due to the low number of studies in every variable, we could not enter in meta-analysis.

Forest plot of the total and subgroup analysis (representing odds ratio in patients with length of LTOT treatment under and above 8 months)
In the pooled analysis, the RR [CI 95%, p value], I2 for readmission reduced 1.542 [1.284–1.851, < 0.001], I2 = 60%, and 1.693 [1.645–1.744, < 0.001, I2 = 60%] for patients with length of LTOT treatment under and above 8 months, respectively. A forest plot of the total and subgroup analysis is presented in Fig. 2.
Accordingly, comparing the two subgroups shows that the rate of readmission in COPD patients who have received LTOT for more than 8 months is lower than those who have received LTOT for less than 8 months in comparison with the patients who have not received LTOT. A sensitivity analysis was conducted by systematically omitting each study, and it showed no influential studies. Egger’s test indicated no publication bias (p = 0.64).
As shown in Table 2, characteristics of included studies have been classified based on countries including the USA, west Malaysia, Korea, Spain, Italy, and Birmingham East and North, type of studies including a clinical trial, retrospective cohort study, and prospective cohort study, year of study as well as other variables such as age, gender, mortality, ICU admission, COPD grade, smoking, etc.
Discussion
Based on our results in this systematic review, LTOT at home was associated with a significantly lower risk ratio of hospital readmission.
Recently, the frequency of exacerbations has been considered a noteworthy criterion to be measured in patients suffering from COPD. Frequent exacerbations are attributed to advanced impairment of lung function. Furthermore, as a result of increased disease severity, exacerbations became more frequent and severe [19]. In addition, the frequency of hospital admission is considered a prognostic factor with the higher frequency of hospital admission at any time after discharge but does not rise the risk of mortality [20].
Consistent with our findings in this meta-analysis, an early study from the 1970s and two other studies, all including a small number of patients acting as their control, have indicated that LTOT reduces the number of hospitalizations [16, 21,22,23]. The first months of LTOT were found to be associated with a noteworthy decrease in the number of days spent in the hospital when compared to the pre-oxygen period [8] and also LTOT is concomitant with a reduction in hospitalization in patients with hypoxemic chronic obstructive pulmonary disease [8, 24]. It seems that any effect of oxygen therapy on hospitalization could have resulted from improving attacks of severe desaturations and alleviating pulmonary hemodynamics [25,26,27].
Oxygen therapy could reduce dyspnea by decreasing the demanding effort for breathing and preventing anxiety and distress development, consequently avoiding hospitalization of some COPD patients in stable conditions even without permanent hypoxemia [28].
Cho et al. revealed that HOT was associated with a 27% decreased risk of hospitalization only in patients with COPD grade 1 (FEV1 of ≤ 25% or a resting PaO2 of ≤ 55 mmHg) and a 65% decreased risk after matching. Also, in COPD patients with other grades of COPD, similar results related to HOT treatment were not observed [11]. It was concluded that physicians could prescribe HOT according to the clinical status of patients [11].
Nevertheless, most previous studies have shown a consistent tendency to oxygen therapy in patients with severe hypoxemia in whom HOT was associated with decreased hospital admissions. However, there is a discrepancy between the confirmed documents related to the rule of LTOT treatment in the number of readmissions in COPD patients.
Indeed, a randomized control group that was conducted with Medical Research Council (MRC) study failed to approve this advantage of LTOT [7].
Ringbaek et al. [10] designated that HOT was not effective in lessening the hospitalization rate in patients with moderate hypoxemia. One recent paper recommended that oxygen use outside the National Institute for Health and Care Excellence (NICE) guidance did not seem to prevent admissions [12].
Furthermore, in many previous studies, FEV1% could be considered a predictor of acute exacerbation hospitalization [29, 30]. In addition, several studies [14, 20, 31] showed that the risk of readmission was high in LTOT users, especially after adjustment for severity variables such as predicted FEV1 or PaO2 [14].
Indeed, the excess risk of re-admission in patients with COPD associated with medical care-related factors might be partially due to confounding by indication [11]. This discrepancy in the result part may be explained that patients receiving oxygen therapy have chronic respiratory failure and more severe disease [13]. In addition, patients with COPD who treat with constant oxygen therapy at home have inadequate effort and exercise ability, which might affect morbidity and mortality [14].
However, our meta-analysis showed that LTOT at home was associated with a significantly lower risk ratio of readmission in the hospital.
Long-term home oxygen therapy improved survival in severe hypoxemia of COPD patients [32] and several measures of health-related quality of life functional status and gas exchange were improved with LTOT treatment [33].
Patients with oxygen-dependent COPD with impaired exercise tolerance and health-related quality of life [34] usually experience more anxiety and depression leading to social isolation and restrictions in daily life activities, and also a high risk of hospitalizations associated with suffering and high health care costs [14]. Thus, it is critical to explore factors influencing these measurements. In our meta-analysis, it has been shown that LTOT at home was associated with a noteworthy lower risk ratio of readmission in hospitals. There are fairly complex reasons for emergency room visits and hospital admissions in COPD patients [35].
This study has several limitations. Firstly, we were not capable of assessing some factors that could potentially influence hospital admissions. For example, we had no data on smoking history, body mass index, health behaviors, use of systemic corticosteroids, laboratory results, etc. Secondly, due to a lack of sufficient information on systematic review variables, we could not analyze other variables that will be influenced in the result section. Finally, the sample sizes in the studies necessitate larger RCTs to evaluate the effect of LTOT on readmission in COPD patients.
Conclusions
Based on our results in this systematic review, LTOT at home was associated with a significantly lower risk ratio of hospital readmission. However, the sample sizes in the studies necessitate larger RCTs to evaluate the effect of LTOT on readmission in COPD patients.
References
Anzueto A, Sethi S, Martinez FJ. Exacerbations of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2007;4(7):554–64.
Perera PN, Armstrong EP, Sherrill DL, Skrepnek GH. Acute exacerbations of COPD in the United States: inpatient burden and predictors of costs and mortality. COPD J Chron Obstruct Pulmon Dis. 2012;9(2):131–41.
Group RCW. COPD prevalence in 12 Asia-Pacific countries and regions: Projections based on the COPD prevalence estimation model. Respirology. 2003;8(2):192–8.
Organization WH. World health statistics 2009: World Health Organization; 2009.
Law S, Boyd S, MacDonald J, Raeside D, Anderson D. Predictors of survival in patients with chronic obstructive pulmonary disease receiving long-term oxygen therapy. BMJ Support Palliat Care. 2014;4(2):140–5.
Coleta KD, Silveira LV, Lima DF, Rampinelli EA, Godoy I, Godoy I. Predictors of first-year survival in patients with advanced COPD treated using long-term oxygen therapy. Respir Med. 2008;102(4):512–8.
Party MW. Long-term domiciliary oxygen therapy in chronic hypoxic cor pulmonale complicating chronic bronchitis. Lancet. 1981;1:681–5.
Ringbaek T, Viskum K, Lange P. Does long-term oxygen therapy reduce hospitalisation in hypoxaemic chronic obstructive pulmonary disease? Eur Respir J. 2002;20(1):38–42.
Roselle S, D’Amico F. The effect of home respiratory therapy on hospital readmission rates of patients with chronic obstructive pulmonary disease. Respir Care. 1982;27(10):1194–9.
Ringbaek T, Fabricius P, Lange P. The effect of home oxygen therapy on hospitalization in moderate hypoxaemic COPD. Chron Respir Dis. 2005;2(2):107–8.
Cho KH, Kim YS, Nam CM, Kim TH, Kim SJ, Han K-T, et al. Home oxygen therapy reduces risk of hospitalisation in patients with chronic obstructive pulmonary disease: a population-based retrospective cohort study, 2005–2012. BMJ Open. 2015;5(11): e009065.
Turner AM, Sen S, Steeley C, Khan Y, Sweeney P, Richards Y, et al. Evaluation of oxygen prescription in relation to hospital admission rate in patients with chronic obstructive pulmonary disease. BMC Pulm Med. 2014;14(1):1–6.
Kessler R, Faller M, Fourgaut G, Mennecier B, Weitzenblum E. Predictive factors of hospitalization for acute exacerbation in a series of 64 patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;159(1):158–64.
Garcia-Aymerich J, Farrero E, Felez M, Izquierdo J, Marrades R, Anto J. Risk factors of readmission to hospital for a COPD exacerbation: a prospective study. Thorax. 2003;58(2):100–5.
Jacobs SS, Krishnan JA, Lederer DJ, Ghazipura M, Hossain T, Tan A-YM, et al. Home oxygen therapy for adults with chronic lung disease. An official American Thoracic Society clinical practice guideline. Am J Respir Crit Care Med. 2020;202(10):e121–e41.
Ringbaek TJ. Continuous oxygen therapy for hypoxic pulmonary disease: guidelines, compliance and effects. Treat Respir Med. 2005;4:397–408.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–60.
Egger M, Smith GD, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–34.
Donaldson G, Wedzicha J. COPD exacerbations· 1: Epidemiology. Thorax. 2006;61(2):164–8.
Sana’MH A, Tangiisuran B, Ali IAH, Khim TL, Davies G. Prognostic factors associated with poor outcomes among multiethnic patients with acute exacerbation of chronic obstructive pulmonary disease. Asian Biomed. 2017;9(4):481–90.
Crockett A, Moss J, Cranston J, Alpers J. The effects of home oxygen therapy on hospital admission rates in chronic obstructive airways disease. Monaldi Arch Chest Dis Archivio Monaldi per le malattie del torace. 1993;48(5):445–6.
Stewart BN, Hood CI, Block AJ. Long-term results of continuous oxygen therapy at sea level. Chest. 1975;68(4):486–92.
Buyse B, Demedts M. Long-term oxygen therapy with concentrators and liquid oxygen. Acta Clin Belg. 1995;50(3):149–57.
Clini E, Vitacca M, Foglio K, Simoni P, Ambrosino N. Long-term home care programmes may reduce hospital admissions in COPD with chronic hypercapnia. Eur Respir J. 1996;9(8):1605–10.
GROUP* NOTT. Continuous or nocturnal oxygen therapy in hypoxemic chronic obstructive lung disease: a clinical trial. Annals of internal medicine. 1980;93(3):391–8.
Weitzenblum E, Sautegeau A, Ehrhart M, Mammosser M, Pelletier A. Long-term oxygen therapy can reverse the progression of pulmonary hypertension in patients with chronic obstructive pulmonary disease. Am Rev Respir Dis. 1985;131(4):493–8.
Zieliński J, Tobiasz M, Hawrytkiewicz I, Sliviński P, Palasiewicz G. Effects of long-term oxygen therapy on pulmonary hemodynamics in COPD patients: a 6-year prospective study. Chest. 1998;113(1):65–70.
Woodcock A, Gross E, Geddes D. Oxygen relieves breathlessness in" pink puffers". The Lancet. 1981;317(8226):907–9.
Mohktar MS, Redmond SJ, Antoniades NC, Rochford PD, Pretto JJ, Basilakis J, et al. Predicting the risk of exacerbation in patients with chronic obstructive pulmonary disease using home telehealth measurement data. Artif Intell Med. 2015;63(1):51–9.
Kon SS, Jones SE, Schofield SJ, Banya W, Dickson MJ, Canavan JL, et al. Gait speed and readmission following hospitalisation for acute exacerbations of COPD: a prospective study. Thorax. 2015;70(12):1131–7.
González C, Servera E, Ferris G, Blasco M, Marín J. Risk factors of readmission in acute exacerbation of moderate-to-severe chronic obstructive pulmonary disease. Archivos de Bronconeumología ((English Edition)). 2004;40(11):502–7.
Cranston JM, Crockett A, Moss J, Alpers JH. Domiciliary oxygen for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2005. https://doi.org/10.1002/14651858.CD001744.pub2.
Duiverman ML, Wempe JB, Bladder G, Jansen DF, Kerstjens HA, Zijlstra JG, et al. Nocturnal non-invasive ventilation in addition to rehabilitation in hypercapnic patients with COPD. Thorax. 2008;63(12):1052–7.
Coquart JB, Le Rouzic O, Racil G, Wallaert B, Grosbois J-M. Real-life feasibility and effectiveness of home-based pulmonary rehabilitation in chronic obstructive pulmonary disease requiring medical equipment. Int J Chron Obstruct Pulmon Dis. 2017;12:3549.
Wang Q, Bourbeau J. Outcomes and health-related quality of life following hospitalization for an acute exacerbation of COPD. Respirology. 2005;10(3):334–40.
Acknowledgements
The authors express their gratitude to everyone who helped us with this research, and especially the editor and reviewer, who helped improve the quality of final version of the manuscript.
Funding
This study was funded by Isfahan University of Medical Sciences, Isfahan, Iran.
Author contributions
RS and RM generated the idea, conception, and design of study. MAS and RG searched the literatures in databases and wrote the manuscript. MM performed statistical analyses and edited result part. RS and RM revised the manuscript. RS wrote the Discussion section. RM acted as the corresponding author.
Disclosures
The authors take complete accountability for the content of this paper. Affiliations for the authors have been inserted in the title page. All authors have contributed to the preparation of this article. Ramin Sami, Mahsa Akafzadeh Savari, Marjan Mansourian, Roghayeh Ghazavi, and Rokhsareh Meamar declare that they have no competing interests.
Compliance with Ethics Guidelines
The Research Committee of Isfahan University of Medical Sciences approved the study protocol, and the Ethics Committee confirmed it (IR.MUI.MED.REC.1399.040). This article is based on previously conducted studies and does not contain any new studies with human participants or animals performed by any of the author.
Data Availability
The collection of papers/data used for this review article is available from the corresponding author on reasonable request.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, which permits any non-commercial use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc/4.0/.
About this article

Cite this article
Sami, R., Savari, M.A., Mansourian, M. et al. Effect of Long-Term Oxygen Therapy on Reducing Rehospitalization of Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis. Pulm Ther 9, 255–270 (2023). https://doi.org/10.1007/s41030-023-00221-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s41030-023-00221-3