
Abstract
This paper aims to assess the care preferences of the elderly in China and how the multi-level factors including individuals, communities and provinces affect the elderly’s care preferences. Using data from the 2014 China Longitudinal Aging Social Survey (CLASS) and China Statistical Yearbook 2015, we apply concentration index to examine the utilization of regional resources in the elderly and a multi-level model to examine those relationships. Results show that the elderly who live in communities with well-developed health care facilities prefer to choose family care. There are also significant differences at the provincial level. The developed provinces context increases the likelihood of formal care, but decreases informal care probability. In high social security expenditure provinces, the elderly are more likely to choose formal care. Our findings emphasize the influence of the communities and provinces context on the elderly’s care preferences. We suggest the government pay attention to the care status of the elderly who are outside the social care system.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
With the rapid population aging, the increasing of disability, and the changes in family structure, taking care of the elderly has gradually become a social issue in China. As the recipients of care services, the care preferences of the elderly are crucial. Care preference is a typical subjective concept, which includes an individual's subjective understanding of their preferences for care related factors such as care location and care responsibility. The explanation mechanism based on individual behaviorist methods and premise assumptions is insufficient. The economic development level, social security policies, and care resources at the macro level shape the unique texture of the social scene older people live in, which may have a potential impact on their care preferences.
Scholars have recently shown increased interest in the impact of macro structures on individual behavior and preferences (Zhao et al., 2021; Liu & Zai, 2023). In particular, a growing slew of literature has demonstrated that good social structure factors have a positive association with older adults’ health (Jiao, 2018; Lu et al., 2017). Related studies have found that a variety of family and community characteristics, such as public service availability, physical environment, the family intergenerational support all influence care preferences (Du et al., 2017; Luo et al., 2020). Little research has studied provinces’ resources disparities in how macro care context affects care preferences of the elderly. Overlooking the province level factors might obscure the true association between multi-level factors and care preferences of the elderly. This study contributes to the existing literature in three ways. First, it is the first to examine the three level factors affecting care preferences. Specifically, we utilize province level factors, distinguishing our study from previous studies that employed individual and community factors (Lu et al., 2017). Second, we investigate the concentration index to measure the equal utilization of care resources among older adults. This provides the basis for the subsequent stratified analysis. Third, our study accounts for the interaction between the individual and family, community and regional levels.
2 Literature review
2.1 The definitions and related theory
Family care, also known as informal care, has been the main care form of the elderly in China (Wu, 2020). With the development of the national elderly care service and health care systems, the multi-level elderly care system is comprised of community-based care, institutional care, integrated care and other care forms. The elderly have many care forms to choose from based on their own needs and preferences.
There are three explanatory dimensions in existing literature regarding the relationship between different care modes: mutual exclusion, mutual promotion, and mixed responsibilities (Motel-Klingebiel et al., 2005). Some scholars (Mair et al., 2016; Parsons, 1942) generally believe that families and government are mutually exclusive and substitute each other in terms of care provision preferences, and the development of a welfare state will inevitably lead to a dramatic fall in the role of families with respect to the welfare of the elderly (Bonsang, 2009). A welfare state provides a variety of formal services, and the functions these services undertake are often the same types of services that the family previously provided. Among them, the economic support and family care needed by the elderly are similar to the main functions undertaken by formal services (Ku et al., 2013; Logan et al., 1998). Also, other studies provide contrasting conclusions that informal care substitutes formal care (Bolin et al., 2008). From this view, older adults who receive informal care are less likely to call upon formal types of care (or delay nursing home entry) and reduce medical expenditures (Van Houtven & Norton, 2004). Still, this traditional perception is now being challenged by the perspective of mutual promotion, as proposed by scholars who study the sociology of families. This perspective holds that families and government complement and reinforce each other. Research has shown that the provision of welfare by governments does not weaken family support, and in fact, encourages and enhances the role of the latter (Künemund & Rein, 1999; Lambotte et al., 2018). Following the elderly’s security, the formal assistance provided by governments for families not only strengthens family ties but also enables children to provide more informal support for their parents, known as the perspective of mixed responsibilities.
Embeddedness theory also provides theoretical support for explaining care preferences of the elderly. The theory holds that humans do not make decisions or take actions outside of their social context, and the intentions behind individual purposeful actions are embedded in the constantly evolving system of social relationships. These networks of relationships form a crucial part that connects individual actions, social systems, and the macro environment (Granovetter, 2005). Structural Embedding Theory, as an important dimension of Embedding Theory, emphasizes that individuals and their networks are embedded in the social structure composed of them, and are influenced and determined by the cultural and value factors of their own social structure (Granovetter, 2005). Structural embeddedness reflects the overall structure of the network in which an individual embeds and exerts influence on the individual (Granovetter, 2017). The elderly, as socialized individuals, live within the social network they construct, and the care preferences may be closely related to their social relationship system and influenced by social structure. Previous studies have found that elderly care preferences are not only influenced by individual and family factors, but also by social structural factors in the regions where they live (Kemp et al., 2013). In Western society, studies have shown a significant relationship between care preferences and the direction of government welfare systems (Mair et al., 2016).
2.2 Empirical studies
The factors that affect the older adults’ care preferences can be roughly divided into three levels: individual factors including personal basic status, health status, income, cultural beliefs, family resources etc., community factors including care resources, access to healthcare and social factors including social norms and values, social development level, elderly care policies (Cheung et al., 2006; Daatland, 1990; Kane & Kane, 1980; Lambotte et al., 2018; Pinquart & Sorensen, 2002; Wolff et al., 2008). Structural embeddedness theory certainly starts with human characteristics at the center and family as the immediate ecology for an individual, then progresses to the community and the province.
Previous empirical studies have shown that regional factors have a significant impact on elderly people’s care preferences. Regional or national inclusive welfare policies would encourage the aged to choose formal care. Seniors with formal care preferences are more likely to live in an environment where government provides care support and can access convenient and accessible community care resources (Zarit, 1999; Lu et al., 2021). A comparative study on the care preferences of the aged in Germany and the United States found that Germany's inclusive health care policy has made formal care popular, while the United States' medical health insurance policy provides limited support for non-medical or institutional care, making informal care more widespread (Brody, 1985; Stoller, 1985). Although individuals may prefer policies that already exist, those with care needs or vulnerabilities tend to have more comprehensive welfare policies (Blekesaune, 2007; Kikuzawa et al., 2008). Additionally, the care preferences of the elderly are also influenced by the accessibility of care resources, and therefore fairness is used to measure the allocation and utilization of care resources (Luo et al., 2020). Research has found that the elderly in East Germany are willing to use formal care, but do not have the accessible care facilities and services (Lehnert et al., 2018), and the distribution of utilization is greatly influenced by policies (Wagstaff & Van Doorslaer, 2000). In European welfare countries with high government public expenditure, the distribution of social elderly care services is relatively balanced, even benefiting low-income groups (Carrieri et al., 2017; Rodrigues et al., 2018). Lower income levels have become obstacles for older people to receive formal support. Therefore, if there is a lack of formal social support, older people prefer informal support (Pinquart & Sorensen, 2002).
For example, studies have found that economic inequality at the community level can have an impact on the risk of death for individuals aged 45 and above (Zhao et al., 2021). In the United States, the government's provision of medical subsidies for formal family care significantly increases the likelihood of adults providing family care for their parents (Liu & Zai, 2023).
Overall, there has been an abundance of research on older adults care and preferences both domestically and internationally, and inspiring conclusions have been drawn. However, there are still three major challenges when examining the following areas that need further research. First, there is insufficient attention on the subjectivity of the elderly’s care preferences. The elderly’s care preference refers to the subjective attitude of the elders towards their choices of care responsibilities and care locations, which involves social psychology's theoretical explanations of individual attitudes and behavioral relationships, as well as meso and macro relationships with their respective families and countries. Second, further research is needed to examine the impact of social structure on the elderly’s care preferences. There are significant differences in economy, social development and support between regions. The mechanism by which social structure affects the care preferences should also be included in the research perspective. Third, the measurement indicators of the macro dimensions are relatively scattered. There is no unified indicator for the selection of macro level elderly care policies and investment resources.
2.3 The current study
Drawing from the aforementioned evidence, this study aims to answer three questions. 1) What are the care preferences of the elderly? 2) Is there regional fairness in the utilization of social care and health care resources? 3) Do social structural factors have an impact on the care preferences of the elderly? Based on the previous research, we have proposed the following hypotheses:
Hypothesis 1a:
From the perspective of social equity regarding relationship on resources distribution and care preferences, we expect that older persons who live in communities with better health care resources are more likely to choose family care, while those in communities with inadequate health care facilities prefer formal care.
Hypothesis 1b:
The elderly living in communities with well-equipped care facilities are more inclined to choose integrated care. Conversely, the elderly living in communities with inadequate facilities tend to prefer family care.
Hypothesis 2:
According to Chinese cultural traditions, we suppose that family relationships affect the older adults’ care preferences. The elderly living in close-knit intergenerational relationships are more likely to choose informal care. Conversely, the older adults living in estranged-oriented intergenerational relationships prefer to choose formal care.
Hypothesis 3a:
Based on Embedding Theory, we hypothesize that social structures have an impact on care preferences. The elderly who live in developed provinces may prefer formal care, whereas those living in undeveloped provinces would be more inclined to choose family care.
Hypothesis 3b:
We hypothesize the interaction between individual factors, community care factors and provinces conditions in shaping the care preferences of the elderly. The elderly living in poor community and province contexts who lack family supports are more preferred integrated care and formal care.
3 Research methods
3.1 Analysis strategy
The analysis strategy includes three steps as follows.
First, the concentration index is used to determine whether there is unequal resources utilization of the elderly in China. Based on the utilization of elderly care services, we construct the community social care and health care resources utilization concentration index to judge the fairness of older adults community social and health care resources utilization.
The Concentration Index (CI) is a commonly used indicator to measure fairness in the field of health services. The concentration curve is an intuitive method to display the distribution of target variables among populations with different economic conditions (Luo & Ding, 2020). The calculation formula is as follows:
Among them, N is the sample size, μ is the utilization mean, yi is the utilization status of sample i, and ri is the ranking of sample i on the income horizontal axis (Wagstaff & Van Doorslaer, 2000). Here, r is sorted by per capita annual expenditure of households, and h is whether community care services (or healthcare services) have been utilized, μ is the mean. Due to the fact that 'service utilization' is a binary variable with boundaries, direct application of equ 1 may result in estimation bias. Therefore, the method proposed by Wagstaff & Van Doorslaer (2000) was used to correct it, namely:
In equ 2, \(\beta_{k}^{m} ,\;\overline{x}_{k}\) and CInk are the bias effects, mean, and corrected concentration index of the k-th explanatory variable when taking the mean based on probit regression.
\(\frac{{\beta_{k}^{m} \overline{x}_{k} }}{\mu }\) is the elasticity coefficient of the explanatory variable xk, the product of this coefficient and CInk is the contribution of explanatory variable xk to the difference in service utilization. \(\frac{{GCI_{n\varepsilon } }}{\mu }\) is an unexplained residual contribution. The value range is (-1, 1). If the concentration index is 0, it indicates that the relevant variables are absolutely fair. When the concentration index is positive, it indicates that the relevant variables are mostly concentrated in high-income groups, when the concentration index is negative, it indicates that the relevant variables are mostly concentrated in low-income groups. From the perspective of the concentration curve, the horizontal axis of the concentration curve represents the cumulative percentage of the population with a personal income level ranking from low to high, while the vertical axis represents the cumulative percentage of "service utilization". If service resources are more equally utilized among low-income groups, the concentration curve is above the absolute fairness line, and vice versa; The more obvious the curvature of the curve, the greater the distribution difference.
Second, a three-layer Bernoulli layered model were constructed at the community and provincial levels, respectively, to gradually explore the mechanisms that affect older adults care preferences at the individual, community, and regional levels. It should be noted that in the modeling process, family intergenerational relationships are theoretically at the meso level, while methodological indicators are at the individual level of the older adults, and individual levels are included in the model. At the same time, in order to analyze the macro level impact in a more three-dimensional manner, macro factors are divided into community level and provincial level in modeling.
Individual Level (Level 1):
Community Level (Level 2):
The impact of community care and health resources on the elderly’s care preferences:
Individual factor effects in the older adults:
Control variable effects:
Provincial Level (Level 3):
Provincial preferences for elderly care:
Community resource effect:
Control variable effects:
Among them, P is the probability of institutional care corresponding to the original virtual coding dependent variable Y with a value of 1. Due to the lack of deterministic scale information in logistic regression coefficients, that is to say, Bernoulli regression coefficients provide the relative amplitude of the independent variable's influence, not the absolute amplitude. At this point, the odds ratio is usually used to represent the ratio between two categories. B is the intercept of the layer one model, and other coefficients represent the effect of individual characteristic variables, reflecting the elderly care preferences due to their individual characteristics (gender, age), subjective norms, behavior control, individual attitudes and family intergenerational relationships. The random error in the layer one model represents a unique senior age adult, that is, the part of the difference that cannot be explained by the systematic influence of community, province and personal characteristics. Xi represents the independent variable of layer one. The second level is community characteristics, mainly consisting of three variables: community health care facilities, community social care facilities, and community type.
We believe that the community characteristics of layer two have an impact on the intercept and coefficients of layer one, resulting in undetermined \(\upgamma\) coefficients and random perturbation term \({\upmu }_{0}\). The third layer is the characteristics of provinces, including two variables: the regional GDP and the proportion of general public service expenditure in each province in 2014. The characteristics of provinces in layer three have an impact on the intercept and coefficients in layer two, so it is necessary to estimate the coefficients such as \(\upeta\) and random disturbance term \({\uptheta }_{00}\). The equation of the Layer 2 and Layer 3 model determines the direction of the independent variable coefficient effect in Layer 1 model, namely strength. Due to the limited sample size, especially in some communities, which is very unfavorable for stratified research, we must set all slope models of Layer 2 and Layer 3 units as fixed effects models, that is, they do not have random effects, in order to maintain the necessary level of statistical significance as much as possible.
Finally, due to the dual structure of urban and rural areas in China, urban–rural differences are an important dimension of structural differences. Through a hierarchical model of urban and rural samples, this study examines the differences in care preferences among the elderly in urban and rural areas and their explanatory mechanisms.
3.2 Data source and study sample
This study used survey data from the 2014 China Longitudinal Aging Social Survey (CLASS) and summary data from the China Statistical Yearbook 2015. The China Longitudinal Aging Social Survey (http://class.ruc.edu.cn/) is a national and continuous large-scale social survey project. By regularly and systematically collecting data on the social and economic background of the elderly population in China. The class project conducted two pilot surveys in 2011 and 2012, and the first nationwide baseline survey was conducted in 2014. Follow ups will be conducted every two years thereafter, with preliminary preparations for three separate surveys in 2016, 2018 and 2020. In this study, we use the 2014 baseline survey. The survey adopts a stratified and multi-stage probability sampling method. Select county-level areas (including counties, county-level cities, and districts) as primary sampling units (PSUs), and village/neighborhood committees as secondary sampling units (SSUs). The survey subjects are Chinese citizens aged 60 and above. In 2014, the survey was officially conducted in 28 provinces, and a total of 462 community survey questionnaires were obtained, and 11,511 individual valid questionnaires were collected for older people aged 60 and above. In all, after removing 953 samples with missing key variables, the valid sample for this study is 10,558. The survey strictly ensures data quality, and the overall age distribution of the samples is relatively close to the results of the sixth population census in 2010, indicating good data quality (Du & Wang, 2017).
3.3 Outcome variable and measurements
The dependent variable of this study was the elderly’s care preferences, which were divided into two dimensions, namely the preferences for care locations and the preferences for care responsibilities. Regarding the care locations, we selected the question "Where do you plan to live in the future?". Referring to the previous research foundation (Zhang et al., 2014; Meng et al., 2017), we coded the outcome variable as 0- if the seniors want to receive care at their own home and children's home; 1- if the seniors want to receive care at day care centers and nursing homes in the community or in care institutions. Regarding the care provider, we used the question "Who do you think is mainly responsible for the care of the elderly?" This question had multiple response choices, with the options being divided into the government, community, children, the elderly themselves or their spouses, and the government, children, and the elderly jointly. Considering the increasing international emphasis on community care (Lambotte et al., 2018; Ridic et al., 2012) and referencing literatures, we recoded the outcome variable as unordered three categorical variables: defined as informal care if the care was provided by children, the elderly, or the spouse, and integrated care if the care was provided by government, children, and the elderly jointly and formal care by government and community care.
The independent variables were divided into individual-level variables, community-level variables and province-level variables. At the individual level, we selected variables including behavioral attitudes, subjective norms, and behavioral control based on the analysis framework of planned behavior theory in social psychology. Behavioral attitudes refer to the elderly’s attitudes toward family care and institutional care. Subjective norms mean personal subjective feelings about what important others think should be done, which are operationalized as “Do your family want you to stay in a nursing home?” Behavior control refers to individual's subjective perception of whether they are confident in successfully completing a specific behavior (Eagly & Chaiken, 1993). In this study, behavioral control refers to the sense of control that older adults can achieve their care preference. We selected three variables measuring behavioral control, including economic ability, number of surviving children, and marital status. Family intergenerational relationships was crucial for the older adults’ care preferences. We use latent variable analysis to form three main types of intergenerational relationships: tight, loose, and detached based on the dimensions of intergenerational solidarity and conflict (Bengtson et al., 2002). At the community level, we measured two types of community care resources; care facilities and health facilities. At the province level, we measured provincial resources by two indicators: the per capita GDP of each province in 2014 and the proportion of social security expenditure to local general public budget expenditure in 2014. Generally speaking, provinces with higher per capita GDP would have higher levels of economic development. Social security expenditures as the mean of social redistribution are provided by the government to ensure the basic living rights of citizens. Social security expenditure is the main force for the government to narrow the income gap among residents and achieve social equity (Yue et al., 2017). Meanwhile, considering the differences in development levels between urban and rural areas in China, we also included the types of communities in the model. The control variables include age, gender, education and self-rated health.
4 Results
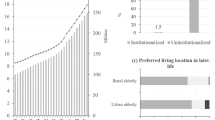
Starting with variables statistics (Table 1), 95.79% of older people want to live at home in the future and only 4.21% prefer to live in institution. As to the care responsibility, nearly 70% older adults prefer informal care and 19.06% of integrated care and 11.41% of formal care. In the individual level, the proportions of three types of intergenerational relationships in families is 43.43% for close-knit relationships, 34.59% for loose-oriented relationships and 21.99% for estranged-oriented relationships., The overall impression of elderly people towards nursing homes is average, accounting for 61.53%. The family’s negative attitude on staying in a nursing home accounts for 94.60%. The perceived control factors include income (8.82), marriage with spouse (64.79%) and number of living children (2.97). As to the community level, the community having health care facilities and social care facilities separately accounted for 86.49% and 69.37%. The urban community account for 64.29%. In terms of province level, the average provincial Per Capita Gross Regional Product in 2014 is 52.3 thousand yuan, and the mean proportion of provincial social security expenditure in 2014 is 12.9%. In terms of control variables, the main proportion in samples is about 70 years of old age, female, low education.
4.1 Analysis of equity in the utilization of elderly care resources
In this study, we analyzed the utilization of social care services and health care services. Social care services provided by the community include daily living care, meal delivery services, household chores, rehabilitation care, transportation services, home visits, emergency assistance, etc. The health care services provided by the community for the older people include community clinics and healthcare service centers. The analysis results show that the utilization rate of community social care services by the elderly is low, with only 7% of the aged using nine types of community care services. The coverage of community health care service facilities, such as community hospitals, health clinics, and consultation rooms, is relatively wide, reaching 86.49%. However, only 6% of the older adults have utilized family care, home treatment, and rehabilitation treatment. Overall, the proportion of the elderly utilizing social care services and health care services is relatively low.
Figures 1 and 2 show the concentration curves of community social care service utilization and community healthcare services utilization with individual income, respectively. The results show that the concentration curve of community social care service utilization was below the absolute fairness line, indicating that care service utilization is more distributed among high-income groups, while the concentration curve of service utilization in health care services is located above the absolute fairness line, indicating that service utilization in health care services is more distributed among middle and low-income populations. In addition, the concentration curve of community social care service utilization is significantly more curved than that of community health care services, indicating a greater distribution difference in care services.

Concentration curve of care services utilization in communities for the elderly

Concentration curve of health service utilization in communities for the elderly
The elderly have different characteristics in utilizing community social care services and community health care services. Community social care services are more commonly used by high-income older people, while community health care services are more commonly used by middle and low income seniors. There may be some explanations. Firstly, community care services are more concentrated in urban areas from the distribution perspective, with the aged being densely populated and their children not around, and they have the economic ability to use these services. Since care services are sparsely distributed in rural areas, their utilization by rural seniors is less. Secondly, China's medical and health services have made significant progress, with the level of medical security constantly improving. Community health service centers and village clinics have basically achieved full coverage in urban and rural areas, especially in remote areas. In the latest health poverty alleviation campaign, the gaps in village clinics have been eliminated, and low-income groups can also use fair and accessible medical and health services. The unfair utilization of the elderly’s resources reflects the unequal distribution of the elderly’s care resources. Related studies have found that the utilization of social care services for the elderly tends to be "pro high-income groups"; rural seniors are mainly driven by physiological factors, while urban older adults are driven by socioeconomic factors (Lu et al., 2017). Therefore, the following will examine the impact of macro factors on the elderly’s care preferences from the perspective of fairness of resource allocation in communities and provinces.
Table 2 shows the correlation between province-level variables and older adults care preferences. The results show that there are provincial differences in the care preferences of the elderly. In 2014, the per capita Gross Domestic Product (GDP) of provinces that prefer institutional care was 71,400 yuan, based on the attractiveness of the care location; for provinces with preferences for family care it was 52,500 yuan, which is significantly lower than the provinces with a preference for institutional care; while in 2014, the proportion of social security expenditures in provinces where the elderly preferred to choose family care was 12.32%. Provinces where the elderly preferred institutional care were significantly higher than those who chose family care, with a proportion of 16.08%.
From the perspective of care responsibility, provinces with higher per capita GDP tend to choose formal care; Provinces with a higher proportion of social security expenditure tend to choose formal care, and the two show a significant correlation. In terms of the proportion of social security expenses in 2014, the proportions of family care, integrated care, and formal care were 12.12%, 13.41%, and 13.86%, respectively, showing a gradually increasing trend. Existing researches on the relationship between national investment and elderly care preferences have shown that older people living in countries with higher national health care investment are more inclined to choose formal care, while older people living in countries with lower national investment may struggle with conflicts of interest (Mair et al., 2016; Marcum et al., 2013). From the relevant analysis results, the conclusion of this study is consistent with previous studies.
4.2 The impact of regional factors on elderly care preferences
Table 3 presents the results of hierarchical regression analyzing the elderly’s care location preference. It consists of four models, which were formed by gradually incorporating variables from each level. The null model only includes the dependent variable and community and province level variables, indicating that the intercept coefficient is statistically significant. A z-test was conducted to compare the differences between the community level and province level variables in the second and third layers, and the intraclass correlation coefficient at the community level is 10.6%, at the province level is 14.4%, which means the community level explained 10.6% of the total variation, while the province level explained 14.4%. The results indicate that there are differences in the elderly’s care preferences between communities and provinces. The hierarchical model in this study is reasonable.
The individual model adds control variables and individual and family factors of the elderly. The results indicate that among the types of family relationships, older people who are in close-knit intergenerational relationships with their families have significant preferences for family care (OR = -0.25), while older people who are in loose-oriented intergenerational relationship do not show statistically significant with care preferences. The relevant studies have also found that older people with close-knit intergenerational relationships tend to choose family care (Liu et al., 2018). From subjective norms perspective, there is a strong positive correlation between family members' willingness to nursing homes and the senior’s own preferences for institutional care.
The community model adds community variables, and the results show that the social care facilities in the community have no significant impact on care preferences, but community health care facilities have a significant negative correlation with institutional care preferences. That means, older people living in communities with better health care facilities tend to choose family care. Older people living in urban communities are more likely to choose institutional care.
The full model adds province variables, including per capita regional GDP in 2014 and the proportion of social security expenditure in each province. The results show that provinces with higher per capita regional GDPs are more likely to choose institutional care. The proportion of social security expenditure has a significant positive effect on the elderly’s institutional care preferences, indicating that provinces with higher government social security expenditure are more likely to have seniors choosing institutional care. After adding province variables, most of the independent variables in the original model continue to maintain their impact on the dependent variable, indicating that the model is generally stable. However, the impact of independent variables on the individual and community level models has been weakened. For example, the impact coefficient of the number of surviving children on institutional care preferences has become smaller. After controlling province level variables, its standardized correlation coefficient has become smaller, indicating that the number of living children has weaker impact on institutional care preferences.
Table 4 presents the results of generalized multinomial regression analyzing the elderly’s care preferences on who should take the responsibility of caregiving. In the zero model, the intercept term has statistical significance. The z-test also shows significant differences, indicating the necessity for stratified research. In the first layer model, older people who are in estranged intergenerational relationships tend to choose formal care, while there is no significant difference between informal care and integrated care.
In the second layer model, the results show that older people living in communities with health care facilities tend to choose informal care over integrated care or formal care. However, community care facilities have no significant impact on care preferences. Additionally, older people living in urban communities are more inclined to choose formal care, which is positively correlated with the proportion of social security expenditure. In the third layer model, the per capita GDP has a weak positive correlation with integrated care and formal care, indicating that as the province economic level improves, older people are more likely to choose integrated care and formal care. The proportion of social security expenditure also has a positive correlation with formal care preferences, indicating that in provinces with higher social security expenditure, the elderly are more inclined to choose formal care. Previous studies have also found that formal care preferences are more likely to occur in areas where the government provides support for elderly care needs and has convenient community care resources (Zarit, 1999). In areas where the government invests more in public welfare, older people may be more inclined to choose formal care. Conversely, in areas where public investment is less, older people may be more inclined to choose informal care (Mair et al., 2016). This suggests that government public investment in elderly care field has a potential significant impact on care preferences.
4.3 Stratified regression results on elderly care preferences: urban vs. rural
Taking into account the significant economic and social differences between urban and rural areas in China, this study further conducts separate sample regression on the care preferences of the elderly in urban and rural areas. Tables 5 and 6 present the stratified regression results of urban and rural seniors using generalized binary and generalized multinomial regression models, respectively. After separating the samples by urban and rural areas, the significance of the community-level variables disappears, indicating that the differences in the distribution of elderly care facilities and health care facilities between urban and rural areas have canceled each other out.
The results in Table 6 show that after including province-level factors, the impact of community-level factors on urban and rural seniors become non-significant. In the three-layer model, only subjective norms and the number of living children show statistical significance among the individual factors of rural older people. A positive attitude of family members towards rural seniors living in nursing homes and having fewer surviving children had a significant impact on their institutional care preferences. Family intergenerational relationships don’t have a significant impact on the care preferences of urban and rural older people. After distinguishing urban and rural samples, some variables showed differences between the two groups. On the one hand, lack of informal care resources will significantly increase the likelihood of rural older people choosing formal care and reduce the possibility of older people obtaining informal care. Previous studies have also shown that the elderly living in cities are more likely to receive formal care, mainly due to the individual resource advantages of urban older people, especially their higher income, which encourages their choice of formal care, and the availability of care resources in urban areas further strengthens the formal care advantage (Luo et al., 2020).
From the provincial level, the elderly living in economically developed urban areas tend to choose institutional care, while the rural economic situation in each province has no significant impact on elderly care preferences. Social security expenditure has a significant positive impact on the institutional care preferences of urban and rural seniors, and has a greater impact on rural seniors. Further analysis shows that the elderly care service system in urban areas with higher levels of economic development is more complete, and the government's expenditure on social security related to senior care is higher, which promotes the possibility of urban older people choosing integrated care and formal care. Research has demonstrated at the regional level that the socio-economic advantages of the eastern region have been transformed into accessibility advantages for care services, benefiting the elderly in the region (Luo et al., 2020).
Table 5 presents the hierarchical regression results on elderly care preferences between urban and rural areas. The table shows the interactive influence of various levels on older care preferences. After incorporating the provincial factors into the three-layer model, individual factors such as individual values were found to have strong statistical significance in both urban and rural models. Subjective norms had the greatest impact on the formal care preferences of rural older people, while the number of surviving children had the greatest impact on their family care preferences. The higher the personal income of the urban elderly, the more likely they are to choose formal care. Previous studies have also found that lower income levels can hinder seniors from choosing formal support (Pinquart & Sorensen, 2002).
Overall, ageing people in urban areas with strong individual control abilities tend to choose formal care, while rural older people with greater social vulnerability, including those with few children, low income, and poor self-rated health, tend to choose formal care and avoid choosing informal care. The differences in economic and social conditions between urban and rural areas and individual endowments, as well as differences in family intergenerational relationships, put elderly care preferences at various stages of policy formulation and implementation.
5 Conclusions and discussion
In this study, we analyze the impact of individual, community and province factors on care preferences of the elderly from the multi-level perspective. Moreover, we investigate how this relationship is explained from theoretical perspectives on social psychology, cultural traditions, and social structure. The research has the following conclusions:
First, our findings highlight the inequitable utilization of elderly care resources in China at the community level. Older people demonstrate significant differences in accessing resources related to care, including social care services and health care services. Utilization of social care services varies greatly among the elderly, with a greater distribution among high-income groups. Besides, utilization of health care resources is more evenly distributed among middle and low-income groups. High-income groups have greater access to social care services, while low-income groups benefit more from health care services. The inequitable utilization of resources by older people reflects the inequality in the distribution of elderly care resources. Previous studies have found that insufficient service utilization are related to undeveloped community care services, including inaccessible and unaffordable care services older people need and the quality of services. Since the unbalanced development of care services between rural and urban, rural seniors lack the economic ability to purchase care services and have the lower preference for formal care and integrated care.
Second, older people living in communities with relatively complete health care facilities show obvious family care preferences. Community health centers play a role in encouraging the elderly to choose family care. Community health facilities can meet the daily health care needs of the elderly and make up for the shortcomings of family health care, rehabilitation, and chronic disease management. Studies have shown that most older people prefer to rely on family rather than community services to help them meet their daily needs (Weaver et al., 2018). However, when the seniors' care needs exceed the ability of what the family can provide, the older adults usually accept formal services to continue living in their familiar family and community (Mair et al., 2016). Therefore, improving community healthcare services plays a promoting role in family care. These outcomes largely lend support to Hypothesis 1a.
Third, our findings regarding the social care facilities in community have no significant impact on elderly care preferences might appear counterintuitive at first glance. Although community care facilities do not show significant influence in the model, their impact on formal care is positive, which can reflect their positive promotional effect on integrated care and formal care. Older people's preferences for care models are based on the care services accessibility and affordability. Community care services are not widely available in rural areas, and many rural older people are unaware of these services, let alone use and choose them. So hypothesis 1b has not been validated. Western studies through comparative studies have found that family care is more widespread in the United States, formal care is more popular in Europe mainly due to the European welfare state model's substitution of family care (Daatland, 1990). The descriptive statistics of this study show that current community care facilities in China are relatively insufficient and have limited distribution, which explains why they have no significant impact.
Besides, from the Confucianism and filial piety culture tradition perspectives, older people are embedded in family relationships and their care preferences are influenced by the intergenerational family relationships. The elderly in close-oriented intergenerational relationship tend to prefer family care. Conversely, older people in estranged-oriented relationships tend to prefer integrated care and formal care. These outcomes lend support to hypothesis 2. The practices of developed countries have proven that taking care of the elderly has always been an important family function and responsibility. After experiencing the welfare of social policies, many developed countries are facing government financial crises and macro intergenerational conflicts, and have to "bring their families back" (Peng & Hu, 2015).
Last, our findings highlight the importance of social structure in shaping the care preferences of seniors and hypothesis 3a and 3b are supported. The more economically developed the provinces are, the more likely the elders prefer to choose formal care and integrated care. The elderly living in provinces with higher social security expenditure tend to choose integrated care and formal care. Generally, the aging care service systems in economically developed urban areas are much improved, and governments provide higher social security expenditure related to elderly care, so urban seniors are more likely to choose integrated care and formal care. The socio-economic advantages of regions can be transformed into advantages in accessing care services, benefiting the elderly in those areas (Luo et al., 2020). We investigate that the interaction between individual factors, community care factors and province conditions are all in shaping the care preferences of the elderly. The possibility of the elderly living in undeveloped communities and provinces who lack of sufficient family supports is up to integrated care and formal care. Simultaneously, the urban–rural gap exceeds the gap between communities and provinces. Urban elders have more savings, higher educational attainment, less children and more positive attitudes toward nursing homes than rural elders. Besides, they live in communities with more convenient care and health services. Therefore, they are willing to choose integrated care and formal care.
Based on these outcomes, we conclude with the four types of care preferences among older adults. The first type is “habitual care preference”, which refers to the traditional habitual views of elderly people on caregiving behavior, which are deeply influenced by traditional culture and moral judgments. The second type is “relationship dependency care preference”, which means the care preferences of the elderly are influenced by intergenerational relationships, and the strength of intergenerational relationships affects their choice of care preferences. The third type is “structurally restricted care preferences”, which refers to the care preferences of elderly people that are influenced by their social structure. Due to the structural differences in care resources and services caused by the imbalance of economic and social development, their care choices are limited and they are in a state of structural detachment. The last one is “proactively choosing care preferences”, meaning the elderly choose care locations and providers according to their own preferences, without being constrained by intergenerational relationships and care resources.
The unequal utilization of community care services and community health services reflects the structural inequality of distribution care resources in China. Despite the government making considerable efforts to develop the social care system, there is still a lot of space for improvement in rural areas and underdeveloped provinces. Due to the lack of care facilities and income, rural elders are excluded from the national care service system, demonstrating a structural disengagement of care services for rural seniors. Specifically, there are differences in the preferences for formal care, integrated care, and formal care expressed by urban and rural seniors. Unlike health care resources, social care resources for urban elders are diverse and accessible, including public and private nursing homes, cooperatives nursing homes, health care institutions, socialized elderly care services, and hospice care institutions that meet different physical and economic requirements of the elderly. For rural seniors, formal care mainly refers to ensuring priority assistance for groups such as Five-Guarantee elders and particularly disadvantaged older people through public welfare homes and homes for the aged, while private or cooperative nursing homes and socialized care services are relatively rare in rural areas.
Overall, the care preferences of older people in China are influenced by individuals and social structures, with structural embedding characteristics. We argue that due to imbalanced and insufficient development among regions in China, a portion of the elderly have drifted away from the care system, resulting in structural detachment. This is also the content that the country should pay attention to and improve as the next step.
Data availability
This study used survey data from the 2014 China Longitudinal Aging Social Survey (CLASS), which can be downloaded from http://class.ruc.edu.cn/ website. Summary data in the study are from the China Statistical Yearbook 2015.
References
Bengtson, V., Giarrusso, R., Mabry, J. B., & Silverstein, M. (2002). Solidarity, conflict, and ambivalence: complementary or competing perspectives on intergenerational relationships. Journal of Marriage and Family, 3, 568–576. https://doi.org/10.1111/j.1741-3737.2002.00568.x
Blekesaune, M. (2007). Economic conditions and public attitudes to welfare policies. European Sociological Review, 3, 393–403. https://doi.org/10.1093/esr/jcm012
Bolin, K., Lindgren, B., & Lundborg, P. (2008). Informal and formal care among single-living elderly in Europe. Health economics, 17(3), 393–409. https://doi.org/10.1002/hec.1275
Bonsang, E. (2009). Does informal care from children to their elderly parents substitute for formal care in Europe? Journal of Health Economics, 28(1), 143–154. https://doi.org/10.1016/j.jhealeco.2008.09.002
Brody, E. M. (1985). Parent care as a normative family stress. The Gerontologist, 1, 19–29. https://doi.org/10.1093/geront/25.1.19
Carrieri, V., Di Novi, C., & Orso, C. E. (2017). Home sweet home? public financing and inequalities in the use of home care services in Europe. Fiscal Studies, 38(3), 445–468. https://doi.org/10.1111/j.1475-5890.2017.12138
Cheung, C.-K., Kwan, A.Y.-H. & Ng, S.H. (2006). Impacts of filial piety on preference for kinship versus public care. Journal of Community Psychology, 34, 617–634. https://doi.org/10.1002/jcop.20118
Daatland, S. O. (1990). What are families for? On family solidarity and preference for help. Ageing & Society, 1, 1–15. https://doi.org/10.1017/S0144686X00007820
Du, P., & Wang, Y. (2017). Determinants of utilization of social care service for older persons in China. Population Study, 3, 26–37. (in Chinese).
Granovetter, M. (2005). Problems of explanation in economic sociology. In New Developments in Economic Sociology., 1, 29–60. https://doi.org/10.4159/9780674977792-002
Granovetter, M. (2017). Society and economy: Framework and principles. Harvard University Press. https://doi.org/10.2307/j.ctv24w64km
Jiao, K. (2018). Inequality of healthy life expectancy for the Chinese elderly and its future trend. Sociological Studies, 1, 116–141+244245. (in Chinese).
Kane, R. L., & Kane, R. A. (1980). Long-term care: can our society meet the needs of its elderly? Annual Review of Public Health, 1, 227–253. https://doi.org/10.1146/annurev.pu.01.050180.001303
Kemp, L., Ball, M., & Perkins, M. M. (2013). Convoys of care: Theorizing intersections of formal and informal care. Journal of Aging Studies, 1, 15–29. https://doi.org/10.1016/j.jaging.2012.10.002
Kikuzawa, S., Olafsdottir, S., & Pescosolido, B. A. (2008). Similar pressures, different contexts: Public attitudes toward government intervention for health care in 21 nations. Journal of Health and Social Behavior, 4, 385–399. https://doi.org/10.1177/002214650804900402
Ku, L.-J. E., Liu, L. F., & Wen, M. J. (2013). Trends and determinants of informal and formal caregiving in the community for disabled elderly people in Taiwan. Archives of Gerontology and Geriatrics, 56(2), 370–376. https://doi.org/10.1016/j.archger.2012.11.005
Künemund, H., & Rein, M. (1999). There is more to receiving than needing: theoretical arguments and empirical explorations of crowding in and crowding out. Ageing and Society, 19(1), 93–121. https://doi.org/10.1017/S0144686X99007205
Lambotte, D., De, D., Van, R., Fret, B., Dury, S., Smetcoren, A., Dierckx, E., De, W., Verté, D., & Kardol, M. (2018). Frailty differences in older adults’use of informal and formal care. Archives of Gerontology and Geriatrics, 3, 69–77. https://doi.org/10.1016/j.archger.2018.05.018
Lehnert, T., Günther, O. H., Hajek, A., Riedel-Heller, S. G., & König, H. H. (2018). Preferences for home- and community-based long-term care services in Germany: a discrete choice experiment. The European Journal of Health Economics, 19(9), 1213–1223. https://doi.org/10.1007/s10198-018-0968-0
Liu, Y., Zai, X. (2023). The unintended effect of medicaid aging waivers on informal caregiving. MPIDR working papers WP-2023-006, Max Planck Institute for demographic research, rostock, Germany. https://doi.org/10.4054/MPIDR-WP-2023-006
Logan, J. R., Bian, F., & Bian, Y. (1998). Tradition and change in the urban Chinese family: the case of living arrangements. Social Forces, 76(3), 851–882. https://doi.org/10.1093/sf/76.3.851
Lu, J., & Guo, R. (2017). An Empirical study on health and health inequality of Chinese elderly: based on regional and community perspective. Population Journal, 2, 57–67. (in Chinese).
Lu, J., Zhang, L., & Zhang, K. (2021). Care preferences among chinese older adults with daily care needs: Individual and community factors. Research on Aging, 43(3–4), 166–176. https://doi.org/10.1177/0164027520939321
Luo, Y., & Ding, J. (2020). The disparities in nursing institution utilization in the process of welfare socialization: An empirical study using concentration index method. Chinese Journal of Population Science, 5, 79–90+127128 (in Chinese).
Mair, C. A., Quiñones, A. R., & Pasha, M. A. (2016). Care preferences among middle-aged and older adults with chronic disease in Europe: Individual health care needs and national health care infrastructure. The Gerontologist, 4, 687–701. https://doi.org/10.1093/geront/gnu119
Marcum, C., & Treas, J. (2013). The intergenerational social contract revisited: Cross-national perspectives. In M. Silverstein & R. Giarrusso (Eds.), From generation to generation: Continuity and discontinuity in aging families. Oxford: Oxford University Press.
Meng, D., Xu, G., He, L., Zhang, M., & Lin, D. (2017). What determines the preference for future living arrangements of middle-aged and older people in urban China? PLoS One, 12(7), e0180764. https://doi.org/10.1371/journal.pone.0180764
Motel-Klingebiel, A., Tesch-Roemer, C., & Von Kondratowitz, H.-J. (2005). Welfare states do not crowd out the family: evidence for mixed responsibility from comparative analyses. Ageing and Society, 25(6), 863–882. https://doi.org/10.1017/S0144686X05003971
Parsons, T. (1942). Age and sex in the social structure of the United States. American Sociological Review, 7(5), 604–616. https://doi.org/10.2307/2085686
Peng, X., & Hu, Z. (2015). The contemporary transition of the Chinese family and the reconstruction of family policy. Social Sciences in China, 12, 113–132+207 (in Chinese).
Pinquart, M., & Sörensen, S. (2002). Older adults’ preferences for informal, formal, and mixed support for future care needs: a comparison of Germany and the United States. International Journal of Aging & Human Development, 54(4), 291–314. https://doi.org/10.2190/1FVT-24T3-Y1V3-57A5
Ridic, G., Gleason, S., & Ridic, O. (2012). Comparisons of health care systems in the United States. Germany and Canada. Materia Socio-Medica, 24, 112. https://doi.org/10.5455/msm.2012.24.112-120
Rodrigues, R., Ilinca, S., & Schulmann, K. (2018). It’s better together! European perspective on benefits and challenges associated with cross-border health communication campaigns. PLoS One, 13(10), e0204882. https://doi.org/10.1371/journal.pone.0204882
Stoller, E. (1985). Exchange patterns in the informal support networks of the elderly: The impact of reciprocity on morale. Journal of Marriage & the Family, 2, 335–342. https://doi.org/10.2307/352133
Van Houtven, C. H., & Norton, E. C. (2004). Informal care and health care use of older adults. Journal of Health Economics, 23(6), 1159–1180. https://doi.org/10.1016/j.jhealeco.2004.04.008
Wagstaff, A., & van Doorslaer, E. (2000). Measuring and testing for inequity in the delivery of health care. The Journal of Human Resources, 35(4), 716–733. https://doi.org/10.2307/146369
Weaver, R., Roberto, K., & Blieszner, R. (2018). Older adults in rural appalachia: Preference and expectations for future care. International Journal of Aging and Human Development, 4, 364–381. https://doi.org/10.1177/0091415017720891
Wolff, J. L., Kasper, J. D., & Shore, A. D. (2008). Long-term care preferences among older adults: a moving target? Journal of Aging & Social Policy, 20(2), 182–200. https://doi.org/10.1080/08959420801977574
Wu, X. (2020). Problematization of care and its policy choice- a discussion on the perspective of family change. Journal of Hangzhou Normal University (humanities and Social Science), 6, 80–90. (in Chinese).
Yue, X., & Ng, S. H. (1999). Filial obligations and expectations in China: current views from young and old people in Beijing. Asian Journal of Social Psychology, 2(2), 215–226.
Zarit, J. M. (1999). Caring for the caregivers of the elderly: having fun while doing good. Family Relations, 4, 429–431. https://doi.org/10.2307/585251
Zhang, W., Wei, M. (2014). A study on the factors associated with preferences for institutional care of the elderly in urban China: evidences from Xicheng District of Beijing. Population & Economics, 6, 25–37 (in Chinese).
Zhao, L., Hessel, P., Simon Thomas, J., & Beckfield, J. (2021). Inequality in place: effects of exposure to neighborhood-level economic inequality on mortality. Demography, 58(6), 2041–2063. https://doi.org/10.1215/00703370-9463660
Funding
No funding support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Jiehua Lu is the Editorial Board Member of this journal.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zhang, L., Lu, J. A multi-level analysis of older adults’ care preferences in China: from the perspective of regional resource equality. China popul. dev. stud. (2024). https://doi.org/10.1007/s42379-024-00156-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s42379-024-00156-5