
Abstract
Objective
This systematic review examines the impact of COVID-19 on Health-Related Quality of Life (HRQoL) across different populations, focusing on demographic, socio-economic, and COVID-19-related factors.
Methods
A comprehensive search of PubMed from 2020 to 2022 was conducted, identifying 37 studies that met the inclusion criteria. Studies were assessed using the Appraisal Tool for Cross-Sectional Studies, Newcastle–Ottawa Scale, and Consolidated Health Economic Evaluation Reporting Standards tools. Data extraction included study characteristics, HRQoL measures, and health state utility values.
Results
Thirty-seven studies were conducted with a total of 46,709 individuals and 274 HSUVs ranging from 0.224 to 1. Research included Europe (n = 20), North America (n = 4), Asia (n = 11), South America (n = 1), and Africa (n = 1). Utility was measured using 15D (n = 3), EQ-5D-5L (n = 24), EQ-5D-3L (n = 8), VAS (n = 1), and TTO (n = 1). The review found significant decreases in HRQoL among COVID-19 survivors, particularly those with severe symptoms, due to persistent fatigue, breathlessness, and psychological distress. Quarantine and isolation measures also negatively impacted HRQoL, with increased anxiety and depression. Vaccination status influenced HRQoL, with vaccinated individuals reporting better outcomes. Socio-demographic factors such as age, gender, education, employment, marital status, and income significantly affected HRQoL, with older adults, females, and unemployed individuals experiencing lower HRQoL.
Conclusions
COVID-19 has profoundly affected HRQoL, highlighting the need for comprehensive post-recovery rehabilitation programs and targeted public health interventions. Addressing socio-demographic disparities is crucial to mitigate the pandemic’s impact on HRQoL. Policymakers and healthcare providers should implement strategies to support affected populations, emphasizing mental health support, social support systems, and vaccination programs.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
1 Introduction
The coronavirus disease 2019 (COVID-19) has posed a significant threat worldwide, prompting the World Health Organization (WHO) to declare it a public health emergency of international concern on 30 January 2020, and subsequently a pandemic on 11 March 2020 [1]. As of 19 November 2023, COVID-19 has over 772 million confirmed cases, and over six million deaths, with significant implications for public health and Health-Related Quality of Life (HRQoL) [2]. This unprecedented global health crisis has spurred research, with numerous studies investigating the pandemic’s impact on HRQoL. This review aims to examine and synthesize findings related to HRQoL outcomes in various populations affected by the pandemic.
HRQoL is a critical measure that captures the impact of COVID-19 on individuals’ well-being, guiding clinical and policy interventions through utility values ranging from 0 (death) to 1 (perfect health condition) [3]. Utility-based approaches primarily utilize structured vignettes, which are concise depictions of hypothetical health states, to elicit preferences regarding these states from either the general population or specific patient groups. These vignettes are instrumental in gauging how individuals value different aspects of health, offering insights into their health-related priorities and decision-making processes. Typically, this is achieved through established direct and indirect techniques. The direct methods include the EQ Visual Analog Scales (VAS) [4], Time Trade-Off (TTO) [5], and Standard Gamble (SG) [6]. Each method provides a unique way to quantify the value individuals assign to various health states, facilitating the comparison of health outcomes and the prioritization of healthcare interventions.
Conversely, Indirect methods utilize standardized instruments, such as the EQ-5D and SF-6D, which consist of a descriptive system and utility weights derived from population-based studies [7, 8]. These tools measure HRQoL across various dimensions (e.g., mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) and provide consistent and comparable measures across populations, facilitating broader application in clinical and policy-making contexts. Subsequently, the responses are converted into a single summary score using utility weights derived from population-based studies. These weights reflect societal preference for different health states, enabling the calculation of Quality-Adjusted Life Years (QALYs) for economic evaluations and healthcare planning. Indirect methods offer the advantage of providing consistent and comparable HRQoL measures across different populations and conditions, facilitating broader application in clinical and policy-making contexts. In general, direct methods provide individualized evaluations, indirect methods offer broader population-level insights. Together, these methods enrich the toolkit for HRQoL assessment, allowing for comprehensive evaluations.
There has not been an infectious disease outbreak like the COVID-19 pandemic in recent decades. Most previous studies on health status were conducted in social conditions with or without an unexpected pandemic and often focused on specific groups. This review aims to synthesize findings on HRQoL outcomes across diverse populations affected by COVID-19, including survivors, individuals with varying severities of infection, frontline workers, quarantined individuals, and vaccinated groups. By integrating these findings, we aim to identify patterns, risk factors, and protective factors associated with HRQoL outcomes. This review will offer evidence-based recommendations for healthcare providers, policymakers, and practitioners to address the broad health challenges posed by the pandemic, ultimately informing future research and policy decisions.
2 Methods
2.1 Search strategy
A systematic search of PubMed electronic bibliographic databases was conducted from 2020 to May 2022 with the aim of assessing HRQoL utility values using both direct measures (Standard Gamble [SG], Time Trade-Off [TTO], and Visual Analogue Scale [VAS]) and indirect measures (questionnaires such as EQ-5D, SF-6D, and HUI). To improve specificity and minimize the retrieval of non-relevant articles, terms were searched in titles and abstracts, e.g., [SG (abstract/title)]. This approach aimed to focus the search results on studies directly relevant to our research. Additionally, we extended our search to include key terms related to quality-adjusted life years and health state utility, such as ‘preference-based quality of life’, ‘health state utilities’, and ‘health utility’, following the recommendations of health economists [9, 10] (Table 1). Our search aimed to provide a comprehensive global overview, without geographical limitations, to reflect the diverse impact of the pandemic worldwide. The search was limited to publications from 2020 to 2022 for several critical reasons. Firstly, the COVID-19 pandemic began in late 2019, with significant global spread occurring in early 2020. Limiting the search to this timeframe ensures that the studies included are directly relevant to the pandemic and its implications for HRQoL. Studies published during these years are more likely to focus on the unique health challenges and circumstances posed by COVID-19, thus providing the most current and applicable data. Secondly, the pandemic spurred an unprecedented surge in research activity. By focusing on publications from 2020 to 2022, this review captures the most recent and rapidly evolving body of knowledge. This period saw the development and dissemination of numerous studies specifically investigating the effects of COVID-19 on various health aspects, including HRQoL. This ensures the inclusion of the latest findings and emerging trends in the field. Additionally, research conducted prior to 2020 would not encompass data related to the COVID-19 pandemic. Excluding earlier studies guarantees that all included research provides novel insights and findings related to the pandemic’s impact, enhancing the relevance and specificity of the review’s conclusions and recommendations. Moreover, healthcare policies and interventions have significantly evolved in response to emerging data on COVID-19. Studies from 2020 to 2022 reflect the latest understanding of the disease and its management, which is critical for providing evidence-based recommendations for healthcare providers, policymakers, and practitioners. Lastly, focusing on this specific timeframe ensures consistency in the data and context of the studies reviewed. This is crucial for making accurate comparisons and synthesizing findings across different studies, as the healthcare landscape and public health responses were relatively consistent during this period. Thus, this approach provides a comprehensive and relevant analysis of the pandemic’s impact on HRQoL, ensuring that the findings are directly applicable to current healthcare challenges and policy needs. We applied inclusion and exclusion criteria to refine the search results, ensuring they were relevant and focused on our research objectives.
2.1.1 Inclusion and exclusion criteria
Articles were included in our review based on the following criteria: (a) reports presenting health state utility values (HSUVs) related to COVID-19 collected between 2020 and 2022; (b) publications in English in peer-reviewed journals; (c) presentation of original HSUVs data; and (d) use of direct or indirect methods to quantify HRQoL.
2.2 Study selection and data extraction
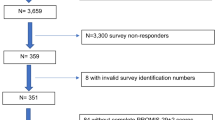
This literature review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, with the study selection process outlined in Fig. 1. The PRISMA flow diagram (Fig. 1) illustrates the selection process, with the initial search yielding 1,052 articles. After de-duplication and screening, 37 studies met the inclusion criteria. One reviewer (Xu) was responsible for the initial study selection, and a second reviewer (BV) checked the quality of the data. The search results were imported into Excel for de-duplication. At the title and abstract screening stage, an inclusive strategy was used to retrieve publications that met the inclusion criteria, including those whose eligibility was uncertain based on their title or abstract alone. These were then fully assessed on the basis of their full text. The selection process consisted of three steps: first, duplicates were removed using Excel; second, titles and abstracts were screened against the inclusion/exclusion criteria using a keyword search, with all excluded articles removed; third, all articles with uncertain eligibility were assessed in their full-text versions against the inclusion/exclusion criteria. An Excel form was prepared for data extraction from articles that passed the second stage.

Flow diagram for HRQoL. the number of records identified, included, and excluded at each stage of the review, and the reasons for exclusions
A pre-designed Excel spreadsheet facilitated systematic data collection, recording key details from each eligible study, including (1) first author, year of publication; (2) country of research; (3) study title; (4) sample characteristics; (5) morbidity; (6) study design; (7) data collection method; (8) survey period; (9) HRQoL instrument(s) or utility measures (e.g., EQ-5D); (10) sample size; (11) health state description; and (12) mean health state utility (with standard deviation). All qualifying studies were identifiable after data compilation in Excel. We extracted directly reported utilities and, where necessary, converted utility scores from a scale of 0 to 100 to a scale of 0 to 1 for consistency. Numerical information was painstakingly extracted from graphical presentations where not directly reported in text or tables. Aggregated utility scores were systematically tabulated and summarized for analysis (Table 2 and Supplementary).
3 Results
3.1 Characteristics of included HRQoL studies
Our initial search of PubMed generated 1,052 articles focusing on the COVID-19 outbreak from 2020 to 2022. Through a detailed process of title and abstract screening, followed by full-text review (Fig. 1), we identified 37 studies [11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47] that met our inclusion criteria. These studies aimed to assess post-discharge persistent symptoms, rehabilitation needs, and HRQoL impacts among the general population, COVID-19 survivors, and specific disease groups. Of these, 31 were cross-sectional studies, four were cohort studies, one was a decision-making study, and one was a longitudinal study. The methodologies employed varied, including twenty studies that used online self-completed questionnaires, six with paper-based self-completed questionnaires, eight conducted via phone interviews (questionnaires), three through private interviews, and three that examined patients’ healthcare records. These studies spanned five continents, including Europe (n = 20), North America (n = 4), Asia (n = 11), South America (n = 1), and Africa (n = 1), reflecting wide geographic diversity. The HRQoL instruments employed included 15D (n = 3), EQ-5D-5L (n = 24), EQ-5D-3L (n = 8), VAS (n = 1), and TTO (n = 1), covering a broad spectrum of health state utility measurements (Table 3).
A significant portion of the research focused on diverse populations, with sample sizes ranging from forty (Spain, Alzheimer’s disease patients) to 15,037 (Germany, intellectual fitness of the general population). Specifically, 14 studies (representing 30.29% of the study population) addressed a broad population of COVID-19 infection cases, while seven studies (representing 5. 89% of the total population) focused on respondents with specific diseases, including Alzheimer’s disease (AD) and amnesic mild cognitive impairment (MCI) [25], cardiovascular disease [26], skin disease [21], total hip (THA) or knee arthroplasty (KA) or partial knee arthroplasty (PKA) [32], cancer [31], bariatric surgery [15], and amyotrophic lateral sclerosis [20]. Each of these conditions was reported in single study (Table 3).
3.2 HRQoL based on EQ-5D dimension responses
Within the review, a total of sixteen out of 37 studies used the EQ-5D instrument for HRQoL domains assessment. Twelve studies utilized the EQ-5D-5L instrument, known for its validity and reliability across five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, to report HRQoL domain performance. Each dimension in the EQ-5D-5L has five levels: no problems, slight problems, moderate problems, severe problems, and extreme problems. The EQ-5D-3L, like the EQ-5D-5L, assesses the same dimensions but with three levels: no problems, some problems, and extreme problems. In this review, four studies used the EQ-5D-3L instrument to assess HRQoL domain performance.
Analysis of the studies using the EQ-5D instrument identified that the self-care domain (14 studies) was consistently reported as the least affected HRQoL domain, with only two studies indicating usual activities as the least affected domain. Conversely, the anxiety/depression domain was identified as the most affected HRQoL domain in eight studies, followed closely by the pain/discomfort domain in seven studies. Mobility and usual activities were also noted as significantly impacted domains. These findings underscore the varied impact of COVID-19 on different HRQoL domains. Detailed outcomes for each HRQoL domain assessment are cataloged in Table 4.
3.3 Analyzing HRQoL utility variations across COVID-19 infection and demographics of selected literature
From the data of 46,709 respondents, we determined 274 health state utility values (HSUVs). Notably, four studies [14, 17, 26, 34] provided comprehensive utilities before and after the COVID-19 pandemic, with HSUVs ranging from 0.823 to 0.95 before the pandemic and 0.802 to 0.861 after. Furthermore, HSUV data were richly detailed across studies, including six studies focusing on population norms [11, 13, 21, 23, 35, 42]. Two articles reported the HSUVs of caregivers before and after lockdown (0.29 to 0.74; 0.31 to 0.72, respectively) and the patients (with HSUVs ranging from 0.5 to 0.66 and 0.6 to 0.62, respectively) [15, 20]. Three studies reported the utility of ICU and ward participants during hospitalization with HSUVs ranging from 0.581 to 0.82, and from 0.72 to 0.86, respectively) [12, 19, 22]. Three studies reported HSUVs in quarantined individuals [13, 21, 43], with HSUVs ranging from 0.86 to 0.96. These findings, collectively summarized in Table 5, underscore the extensive HRQoL challenges posed by the pandemic and highlight the diverse methodologies and populations involved in the current body of research (Table 2).
The pandemic’s uniform risk of infection contrasted with the varying HSUVs observed across different timeframes, locations and geographies. Before the outbreak, higher HSUVs were consistently reported. For example, in Germany, respondents reported a utility of 0.823 before COVID-19, which decreased to 0.803 after the pandemic [14]. Similarly, in Mexico, respondents’ utility was 0.95 before the pandemic and 0.85 after the pandemic [34]. Similar trends were noted in Morocco and Portugal, with pre-restriction HSUVs at 0.91 and 0.887 dropping to 0.86 and 0.861 post-restriction [13, 17]. Young specialists working in the gastroenterology department of designated COVID-19 hospitals were found to have lower utility values than their counterparts. In Romania, the utility of individuals in designated hospitals was 0.957, compared to 0.966 for those working in non-COVID-19 hospitals [41]. Similarly, in Vietnam, the utility of participants in designated hospitals was 0.87 compared with 0.93 for non-designated hospitals [28]. Additionally, examining HSUVs in individuals with and without prior COVID-19 infections revealed nuanced insights into the pandemic’s impact on HRQoL across different geographies. Iran reported the highest overall HSUV among those previously infected, with a value of 0.863 [11]. Conversely, the lowest HSUV, at 0.51, was noted in Belgium and the Netherlands among infected individuals with coexisting health conditions [30] (Table 2 and Supplementary).
Among the 37 included studies, 16 identified various determinants associated with diminished HRQoL during COVID-19. Notably, eight studies reported that older individuals tend to experience lower HRQoL levels. Similarly, seven studies identified a correlation between female gender and reduced HRQoL. COVID-19-related factors, such as history of infection, quarantine status, ICU admission, prolonged mechanical ventilation, or longer ICU stay, were linked to decreased HRQoL in five studies. Furthermore, seven studies demonstrated that individuals with comorbidities reported lower HRQoL compared to those without, indicating the compounded impact of additional health challenges. The detailed associations between these factors and HRQoL are systematically presented in Table 5.
4 Quality assessment of selected studies of HRQoL literature
To evaluate the quality of the studies included in this HRQoL literature review, we utilized three specific tools: the Appraisal Tool for Cross-Sectional Studies (AXIS) (N = 31) [48], Newcastle–Ottawa Scale (NOS) (N = 5) [49], and Consolidated Health Economic Evaluation Reporting Standards (CHEERS) (N = 1) [50] for cross-sectional studies, cohort studies, and decision-analytic model, respectively.
The AXIS tool assesses various aspects of study quality, including clarity of objectives, appropriateness of study design, sample size justification, representativeness of the sample, measurement validity, and consideration of potential biases. The NOS tool evaluates studies based on three domains: selection, comparability, and outcome, with a maximum of nine stars indicating the highest quality. Studies were assessed on the representativeness of the sample, ascertainment of exposure, demonstration that the outcome of interest was not present at the start of the study, comparability of cohorts, and assessment of outcome and adequacy of follow-up. Each domain was rated, and disagreements were resolved through consensus or consultation with a third reviewer. This rigorous process ensured a comprehensive and reliable assessment of the included studies’ quality. The CHEERS tool was utilized for assessing the quality of health economic evaluations. It ensures that studies adhere to standardized reporting practices, evaluating aspects such as the transparency of the economic evaluation, the methodology used, the presentation of results, and the discussion of study limitations. By using the CHEERS tool, we ensured that the health economic evaluations included in our review met high standards of reporting quality and reliability.
The quality of the 31 cross-sectional studies included was evaluated using the AXIS tool, with responses recorded as “Yes” or “No” for specific criteria (Table 6). Our analysis revealed that all 31 studies had clear study objectives and employed appropriate cross-sectional methodologies. Five studies [14, 23, 24, 27, 40] reported justified sample size estimations. All studies clearly defined the reference population and sample frame, ensuring representativeness. Except for one study [22], all studies tested both the validity and reliability of their questionnaires. Regarding the reporting of survey results, most studies presented adequate basic data and addressed concerns about non-response bias, with fifteen studies reporting information about non-responders [12,13,14, 19, 22, 25, 27, 30, 31, 35, 38, 39, 43, 45, 46]. The results were internally consistent, and the analyses described were presented. Discussions and conclusions were justified in all studies, and limitations were transparently discussed. Most studies declared no conflicts of interest, with a few exceptions [30, 41]. Ethical approval or consent was obtained in all studies. Overall, the evaluated studies met most key criteria for rigorous research. Areas for improvement included sample size justification and detailed information about non-responders. The consistent use of validated instruments and clear descriptions of target populations and methods were strengths across most studies. Discussions and conclusions were typically well-justified, and limitations were acknowledged, contributing to transparency and reliability. The quality assessment reveals a generally high level of methodological rigor despite some limitations, providing valuable insights into the diverse effects of the pandemic on different populations and significantly contributing to our understanding of HRQoL during COVID-19.
The quality of five included studies was assessed using the NOS (N = 5) tool, which evaluates studies based on three domains: selection, comparability, and outcome, with a maximum of nine stars indicating the highest quality (Table 7). All studies effectively selected their exposed cohorts, ensuring the representation of their specific populations [18, 26, 39, 44]. Only Ryuichi Ohta and Lorenzo Gamberini [18, 33] included non-exposed cohorts for comparison. All studies confirmed COVID-19 diagnosis and health outcomes through medical records or validated questionnaires like EQ-5D, ensuring that the outcome of interest was not present at the start of the study, thereby clarifying baseline health status. In terms of comparability, all studies adjusted for key covariates such as age, sex, and other relevant factors, enhancing the reliability of their findings [18, 26, 33, 39, 44], and received two stars for comparability, indicating robust adjustment methods. The follow-up periods ranged from three months to one year, ensuring sufficient time to observe outcomes, with high follow-up rates and clear documentation of missing data. Outcomes were assessed using validated instruments such as the EQ-5D-5L and 15D, ensuring consistent and reliable measurement of HRQoL. Ryuichi Ohta and Shir Lynn Lim [26, 33] received eight stars each, indicating high-quality studies with comprehensive selection, comparability, and outcome assessment. M. M. Walle-Hansen and Beatriz Costa Todt [39, 44] received seven stars each, reflecting strong methodologies but lacking a non-exposed cohort. Lorenzo Gamberini [18] received nine stars, indicating a very high-quality study with thorough selection and robust follow-up procedures. Collectively, these studies highlight the importance of clear cohort selection, adjustment for key variables, and the use of validated tools in assessing the impact of COVID-19 on HRQoL, underscoring the diverse impacts of COVID-19 across different populations.
One selected study [36] was assessed using the CHEERS tool and received high marks in all areas. The title, abstract, background, and objectives were clear, with well-defined populations and settings. The methods were robust, using validated tools, and findings were well-discussed. Overall, the study adhered to CHEERS guidelines, indicating high quality (Table 8).
5 Discussion
This systematic review aimed to explore the relationship between demographic, socio-economic, and COVID-19-related characteristics and HRQoL during the pandemic. The review provides a comprehensive overview of how COVID-19 infection, severity of infection, quarantine measures, vaccination status, and socio-demographic factors influenced HRQoL, along with the performance of the EQ-5D domains in assessing these impacts.
The reviewed studies collectively highlight the extensive and persistent symptoms experienced by COVID-19 survivors. COVID-19 infection, particularly with severe symptoms, significantly decreased the HRQoL of participants, emphasizing the need for comprehensive post-recovery rehabilitation programs. For example, a study conducted in Leeds, UK, involving 100 survivors assessed 4 to 8 weeks post-discharge, found fatigue to be the most prevalent symptom, affecting 72% of ICU patients and 60.3% of ward patients. Breathlessness was also significant, reported by 65.6% of ICU patients and 42.6% of ward patients. Psychological distress was common, with 46.9% of ICU patients and 23.5% of ward patients affected. These patients showed a clinically significant drop in EQ-5D-5L scores, indicating a considerable decline in their HRQoL [22]. Similarly, a study from France involving 279 hospitalized COVID-19 patients found that even after a mean of 110.9 days post-admission, fatigue (55%) and dyspnea (42%) were prevalent. Memory loss (34%) and concentration issues (28%) were also notable. The study utilized the EQ-5D-5L questionnaire to assess HRQoL and found that despite these persistent symptoms, the overall HRQoL scores were relatively satisfactory, though patients required ongoing follow-up and rehabilitation [19]. In Mexico, a follow-up study of 115 patients at least 30 days post-COVID-19 revealed a severe decrease in HRQoL in 56% of patients, with 63% experiencing persistent symptoms. The study highlighted alterations in usual activities and anxiety/depression, with restrictive lung impairment being the most common spirometric alteration found in 17% of the patients. This was particularly significant even in those with mild COVID-19, emphasizing the long-term respiratory impact of the virus [34]. Mena Said et al. focused on persistent olfactory dysfunction (OD) related to COVID-19, finding that 89.16% of participants reported parosmia, which significantly affected their health utility values (HUVs) [37]. Cristina Sacristán-Galisteo et al. validated the Spanish version of the Post-COVID-19 Functional Status (PCFS) scale, finding it reliable for assessing functional status and recovery in COVID-19 survivors. This tool showed strong correlations with HRQoL measures and highlighted the importance of continuous monitoring of functional status post-recovery [36]. A study by Morteza Arab-Zozani et al. in Iran highlighted that the mean EQ-5D-5L score for COVID-19 patients was low, indicating poor HRQoL [13]. Finally, the study by Iqbal et al. from Pakistan emphasized the long-term effects of COVID-19, noting that a significant proportion of survivors experienced persistent symptoms such as fatigue and dyspnea, necessitating comprehensive rehabilitation strategies to improve their HRQoL [24].
Studies reported that quarantine and isolation measures, while necessary to control the spread of the virus, had a notable negative impact on HRQoL. Increased levels of anxiety, depression, and stress were observed among quarantined individuals, leading to lower HRQoL scores [13, 14, 35]. Quarantine measures and isolation further contributed to the decline in HRQoL, as noted by Arab-Zozani et al. [12]. The mental health burden of being isolated, the disruption of daily routines, and the uncertainty about health outcomes can significantly diminish HRQoL. The restrictions imposed during quarantine can lead to reduced physical activity, altered eating habits, and changes in sleep patterns, all of which negatively affect physical and mental well-being. Vaccination status is another critical factor influencing HRQoL. Unvaccinated individuals reported lower HRQoL due to ongoing health concerns and heightened anxiety about contracting the virus, as observed by Alinia et al., Zhang et al., and Ferreira et al. [11, 17, 46]. The sense of vulnerability and fear of severe illness among unvaccinated individuals can lead to increased stress and anxiety, further reducing HRQoL. In contrast, vaccinated individuals generally reported better HRQoL, likely due to the perceived protection against severe disease and reduced anxiety about COVID-19.
The use of the EQ-5D instrument across these studies consistently showed significant drops in HRQoL, particularly in the domains such as pain/discomfort and anxiety/depression. Halpin et al. found substantial declines in HRQoL among ICU and ward patients post-discharge, primarily due to persistent symptoms like fatigue and breathlessness [22]. Studies by Weiwei Ping et al. in China and those conducted in Vietnam highlighted that pain/discomfort and anxiety/depression were the most affected domains, pointing to the physical and psychological toll of the pandemic [35, 43]. Navarro et al. and Mena Said et al. emphasized the impact of persistent symptoms such as olfactory dysfunction on HRQoL, showing how ongoing health issues post-COVID can significantly impair daily functioning and overall HRQoL [34, 37].
The COVID-19 pandemic has highlighted the importance of sociodemographic determinants in shaping HRQoL. Age, gender, education, employment status, marital status, and income significantly influence how individuals experience and cope with the pandemic. Addressing these determinants through targeted public health strategies and support systems is essential to mitigate the pandemic’s adverse impact on HRQoL. Studies consistently indicate that older adults report lower HRQoL than younger individuals. This association is evident in the increased problems related to mobility and self-care among older populations and the exacerbation of chronic conditions that further diminish HRQoL [12, 17, 35, 42]. Gender disparities are also evident, with females reporting lower HRQoL and higher levels of anxiety and depression than males. The increased burden of multitasking, such as managing household responsibilities and supporting family members during the lockdown, is a significant stressor contributing to these differences. This trend was evident in multiple studies, including those by Ferreira et al., Nguyen et al., and Arab-Zozani et al., which attributed lower HRQoL in women to higher anxiety levels and the additional burden of domestic responsibilities and caregiving roles during lockdowns [12, 17, 42]. However, Van Rüth et al. did not find significant associations between HRQoL and gender within the homeless population, possibly due to the uniformity of environmental conditions faced by homeless men and women [42]. Marital status influences HRQoL, with single, divorced, or widowed individuals experiencing higher anxiety and lower HRQoL. These individuals often face increased feelings of loneliness and isolation during quarantine periods, exacerbating their mental health challenges. Widowed individuals, in particular, have been shown to have the lowest HRQoL scores among all marital status categories [13]. Ferreira et al. observed that married individuals generally reported better HRQoL than their single, divorced, or widowed counterparts, possibly due to the emotional and practical support provided by partners during lockdowns [17]. Similarly, Hay et al. observed that being married correlated with better HRQoL, while living alone negatively affected it [23]. These findings underscore the importance of social support systems in mitigating the adverse impacts of the pandemic on HRQoL. Higher levels of education were associated with better HRQoL. Educated individuals tend to have better access to information and resources, enabling them to cope more effectively with the challenges of the pandemic. Employment status also plays a critical role, with unemployed individuals reporting lower HRQoL. The stability and social interactions provided by employment significantly contribute to better mental and physical health [12, 17]. The job losses caused by the pandemic exacerbated stress and anxiety levels among the unemployed, as highlighted in the studies by Hay et al. [23]. Economic factors, including income level and financial stability, are crucial determinants of HRQoL. Higher income levels are consistently associated with better HRQoL, as financial resources enable access to healthcare, nutritious food, and a comfortable living environment. Conversely, financial strain during the pandemic has been linked to lower HRQoL. The study by Hay et al. and Ferreira et al. confirmed that increased income correlated with higher HRQoL scores during the pandemic [17, 23].
5.1 Strengths and limitations
The strengths of this systematic review include a comprehensive search strategy and the inclusion of diverse study populations, providing a broad understanding of socio-determinants of HRQoL during the COVID-19. The review considered both physical and psychological health, offering a holistic view of HRQoL. Additionally, the high response rate ensures that the findings are representative of the staff at the institution [16]. However, several limitations must be acknowledged. The heterogeneity among studies in terms of methodologies and populations can introduce biases and affect the generalizability of the findings. Additionally, the reliance on self-reported measures in many studies may lead to underreporting or overreporting of symptoms and HRQoL impacts. Cross-sectional design provides participants’ HRQoL at a single point in time, limiting the ability to infer causality or track changes over time. The voluntary nature of the survey may have led to response bias, as those experiencing higher levels of burnout more likely to participate.
5.2 Recommendations for future research
Future research should focus on longitudinal studies to track changes in HRQoL over time, particularly in COVID-19 survivors. It is also important to explore the long-term impact of vaccination on HRQoL. Additionally, research should aim to understand the socio-demographic disparities in HRQoL outcomes, with a focus on developing targeted interventions for vulnerable populations. Studies should also consider using a combination of direct and indirect HRQoL measurement tools to provide a more comprehensive assessment. Finally, integrating mental health support and rehabilitation programs in the research design will help in understanding their effectiveness in improving HRQoL post-COVID-19.
6 Conclusion
The findings from this review have significant implications for both clinical practice and policymaking. Health professionals should prioritize long-term follow-up of COVID-19 survivors to address persistent symptoms and provide targeted rehabilitation programs. Policymakers should consider socio-demographic disparities in the pandemic’s impact when designing interventions, ensuring that vulnerable populations receive adequate support. Implementing mental health support systems and community-based programs can help mitigate the psychological burden and enhance resilience in affected individuals. In conclusion, this systematic review highlights the substantial and multifaceted impact of COVID-19 on HRQoL. The persistence of physical and psychological symptoms underscores the need for comprehensive long-term support for survivors. Addressing socio-demographic disparities and implementing robust mental health interventions will be essential for promoting resilience and improving the HRQoL in the post-pandemic era.
Data availability
Not applicable.
Code availability
Not applicable.
References
Organization, W.H. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). 2020. https://www.who.int/news-room/detail/30-01-2020-statement-on-the-secondmeeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-ofnovel-coronavirus-(2019-ncov). Accessed date 30 June 2020.
WHO. COVID-19 epidemiological update edition 161 published. Geneva: WHO; 2023.
Romero M, Vivas-Consuelo D, Alvis-Guzman N. Is health related quality of life (HRQoL) a valid indicator for health systems evaluation? Springerplus. 2013;2:1–7.
Green C, Brazier J, Deverill M. Valuing health-related quality of life: a review of health state valuation techniques. Pharmacoeconomics. 2000;17:151–65.
Veenhoven R. Quality of life (QOL), an overview. In: Maggino F, editor. Encyclopedia of quality of life and well-being research. Springer International Publishing: Cham; 2024. p. 5668–71.
McNamee P, et al. Chained time trade-off and standard gamble methods: applications in oesophageal cancer. Europ J Health Econ Formerly HEPAC. 2004;5:81–6.
Al–Sayah F, Johnson JA, Ohinmaa A. Instrument-defined estimates of the minimally important difference for EQ-5D-5L index scores. Value Health. 2017;20(4):644–50. https://doi.org/10.1016/j.jval.2017.01.015.
Ferreira LN, et al. Exploring the consistency of the SF-6D. Value Health. 2013;16(6):1023–31.
Papaioannou D, Brazier J, Paisley S. Systematic searching and selection of health state utility values from the literature. Value Health. 2013;16(4):686–95.
Saeed YA, et al. A systematic review and meta-analysis of health utilities in patients with chronic hepatitis C. Value Health. 2020;23(1):127–37.
Alinia C, et al. The health-related quality of life in Iranian patients with COVID-19. BMC Infect Dis. 2021;21(1):459.
Arab-Zozani M, et al. Health-related quality of life and its associated factors in COVID-19 patients. Osong Public Health Res Perspect. 2020;11(5):296–302.
Azizi A, et al. Health-related quality of life and behavior-related lifestyle changes due to the COVID-19 home confinement: dataset from a Moroccan sample. Data Brief. 2020;32: 106239.
Bauerle A, et al. Mental health burden of the COVID-19 Outbreak in Germany: predictors of mental health impairment. J Prim Care Commu Health. 2020;11:2150132720953682.
Beisani M, et al. Effects of COVID-19 lockdown on a bariatric surgery waiting list cohort and its influence in surgical risk perception. Langenbecks Arch Surg. 2021;406(2):393–400.
Douglas DR, et al. Wellbeing of frontline health care workers after the first SARS-CoV-2 pandemic surge at a neuroscience centre: a cross-sectional survey. J Neurosurg Anesthesiol. 2021. https://doi.org/10.1097/ANA.0000000000000767.
Ferreira LN, et al. Quality of life under the COVID-19 quarantine. Qual Life Res. 2021;30(5):1389–405.
Gamberini L, et al. Quality of life of COVID-19 critically ill survivors after ICU discharge: 90 days follow-up. Qual Life Res. 2021. https://doi.org/10.1007/s11136-021-02865-7.
Garrigues E, et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J Infect. 2020;81(6):e4–6.
Giusiano S, et al. Amyotrophic lateral sclerosis caregiver burden and patients’ quality of life during COVID-19 pandemic. Amyotroph Lateral Scler Frontotemporal Degener. 2021. https://doi.org/10.1080/21678421.2021.1912772.
Guo Y, et al. Association of socioeconomic changes due to the COVID-19 pandemic with health outcomes in patients with skin diseases: cross-sectional survey study. J Med Internet Res. 2020;22(9): e22288.
Halpin SJ, et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: a cross-sectional evaluation. J Med Virol. 2021;93(2):1013–22.
Hay JW, et al. A US population health survey on the impact of COVID-19 using the EQ-5D-5L. J Gen Intern Med. 2021;36(5):1292–301.
Iqbal A, et al. The COVID-19 sequelae: a cross-sectional evaluation of post-recovery symptoms and the need for rehabilitation of COVID-19 survivors. Cureus. 2021;13(2): e13080.
Lara B, et al. Neuropsychiatric symptoms and quality of life in Spanish patients with Alzheimer’s disease during the COVID-19 lockdown. Eur J Neurol. 2020;27(9):1744–7.
Lim SL, et al. Impact of COVID-19 on health-related quality of life in patients with cardiovascular disease: a multi-ethnic Asian study. Health Qual Life Outcomes. 2020;18(1):387.
Machado FVC, et al. Construct validity of the Post-COVID-19 functional status scale in adult subjects with COVID-19. Health Qual Life Outcomes. 2021;19(1):40.
Manh Than H, et al. Mental health and health-related quality-of-life outcomes among frontline health workers during the peak of COVID-19 outbreak in Vietnam: a cross-sectional study. Risk Manag Healthc Policy. 2020;13:2927–36.
Matthew G. Media influence on anxiety, health utility, and health beliefs early in the SARS-CoV-2 pandemic—a survey study. Gen Intern Med. 2021. https://doi.org/10.1007/s11606-020-06554-y.
Meys R, et al. Generic and respiratory-specific quality of life in non-hospitalized patients with COVID-19. J Clin Med. 2020. https://doi.org/10.3390/jcm9123993.
Musche V, et al. COVID-19-related fear and health-related safety behavior in oncological patients. Front Psychol. 2020;11:1984.
Clement ND, Scott CEH, Murray JRD, Howie CR, Deehan DJ. The number of patients “worse than death” while waiting for a hip or knee arthroplasty has nearly doubled during the COVID-19 pandemic. Bone Joint J. 2021. https://doi.org/10.1302/0301-620X.103B.BJJ-2021-0104.R1.
Ohta R, Ryu Y, Sano C. Improvement in quality of life through self-management of mild symptoms during the COVID-19 pandemic: a prospective cohort study. Int J Environ Res Public Health. 2022;19(11):6652.
Ordinola Navarro A, et al. Decreased quality of life and spirometric alterations even after mild-moderate COVID-19. Respir Med. 2021;181: 106391.
Ping W, et al. Evaluation of health-related quality of life using EQ-5D in China during the COVID-19 pandemic. PLoS ONE. 2020;15(6): e0234850.
Sacristán-Galisteo C, et al. Construct validity of the Spanish version of the Post-COVID-19 functional status scale and validation of the web-based form in COVID-19 survivors. PLoS ONE. 2022;17(6): e0269274.
Said M, et al. Clinical factors associated with lower health scores in COVID-19–related persistent olfactory dysfunction. Int Forum Allergy & Rhinol. 2022. https://doi.org/10.1002/alr.22978.
Szabo C, Pukanszky J, Kemeny L. Psychological effects of the COVID-19 pandemic on hungarian adults. Int J Environ Res Public Health. 2020. https://doi.org/10.3390/ijerph17249565.
Todt BC, et al. Clinical outcomes and quality of life of COVID-19 survivors: a follow-up of 3 months post hospital discharge. Respir Med. 2021;184: 106453.
Turcu-Stiolica A, et al. Influence of COVID-19 on health-related quality of life and the perception of being vaccinated to prevent COVID-19: an approach for community pharmacists from Romania and Bulgaria. J Clin Med. 2021. https://doi.org/10.3390/jcm10040864.
Ungureanu BS, et al. Impact of the COVID-19 pandemic on health-related quality of life, anxiety, and training among young gastroenterologists in Romania. Front Psychol. 2020;11: 579177.
van Ruth V, et al. Determinants of health-related quality of life among homeless individuals during the COVID-19 pandemic. Public Health. 2021;194:60–6.
Vu MQ, et al. Health-related quality of life of the Vietnamese during the COVID-19 pandemic. PLoS ONE. 2020;15(12): e0244170.
Walle-Hansen MM, et al. Health-related quality of life, functional decline, and long-term mortality in older patients following hospitalisation due to COVID-19. BMC Geriatr. 2021;21(1):199.
Wong EL-Y, et al. Views on workplace policies and its impact on health-related quality of life during coronavirus disease (COVID-19) pandemic: cross-sectional survey of employees. Int J Health Policy Manag. 2022;11(3):344–53.
Xu Z, et al. Does it matter who you live with during COVID-19 lockdown? association of living arrangements with psychosocial health, life satisfaction, and quality of life: a pilot study. Int J Environ Res Public Health. 2022;19(3):1827.
Zhou CG, et al. Antenatal corticosteroids for pregnant women with COVID-19 infection and preterm prelabor rupture of membranes: a decision analysis. J Matern Fetal Neonatal Med. 2022;35(9):1643–51.
Downes MJ, et al. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open. 2016;6(12): e011458.
Sanderson S, Tatt ID, Higgins JP. Tools for assessing quality and susceptibility to bias in observational studies in epidemiology: a systematic review and annotated bibliography. Int J Epidemiol. 2007;36(3):666–76.
Husereau D, et al. Consolidated health economic evaluation reporting standards (CHEERS) 2022 explanation and elaboration: a report of the ISPOR CHEERS II good practices task force. Value Health. 2022;25(1):10–31.
Funding
Open access funding provided by Corvinus University of Budapest.
Author information
Authors and Affiliations
Contributions
Concept and design: Xu; Acquisition of data: Brodszky and Xu; Analysis and interpretation of data: Brodszky and Xu; Drafting of the manuscript: Xu; Critical revision of the paper for important intellectual content: Brodszky and Xu; Administrative, technical, or logistic support: Brodszky; Supervision: Brodszky.
Corresponding authors
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent to participate
Not applicable.
Competing interest
Not applicable.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Xu, F., Brodszky, V. The impact of COVID-19 on health-related quality of life: a systematic review and evidence-based recommendations. Discov Psychol 4, 90 (2024). https://doi.org/10.1007/s44202-024-00204-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s44202-024-00204-8