
Abstract
Adding supraphysiologic doses of levothyroxine (L-T4) to standard treatment for bipolar depression shows promise, but the mechanisms underlying clinical improvement are unknown. In a previous pilot study, L-T4 treatment reduced depression scores and activity within the anterior limbic network. Here we extended this work in a randomized, double-blind, placebo-controlled study of patients with bipolar depression. Cerebral glucose metabolism was assessed with positron emission tomography and [F-18]fluorodeoxyglucose before and after 6 weeks of treatment with L-T4 (n=15) or placebo (n=10) in 12 volumes of interest (VOIs): the bilateral thalamus, amygdala, hippocampus, dorsal striatum and ventral striatum, and midline cerebellar vermis and subgenual cingulate cortex. Radioactivity in the VOIs, normalized to whole-brain radioactivity was taken as a surrogate index of glucose metabolism, and markers of thyroid function were assayed. Changes in brain activity and their association with clinical response were assessed using statistical parametric mapping. Adjunctive L-T4 treatment produced a significant decline in depression scores during the 6-week treatment. In patients treated with L-T4, we found a significant decrease in regional activity at P<0.05 after Bonferroni correction in the left thalamus, right amygdala, right hippocampus, left ventral striatum and the right dorsal striatum. Decreases in the left thalamus, left dorsal striatum and the subgenual cingulate were correlated with a reduction in depression scores (P<0.05 after Bonferroni correction). Placebo treatment was associated with a significant decrease in activity only in the right amygdala, and no region had a change in activity that was correlated with change in depression scores. The groups differed significantly in the relationship between the changes in depression scores and in activity in the thalamus bilaterally and the left ventral striatum. The findings provide evidence that administration of supraphysiologic thyroid hormone improves depressive symptoms in patients with bipolar disorder by modulating function in components of the anterior limbic network.
Similar content being viewed by others


Introduction
For most patients with bipolar disorder, depression is the most difficult phase of the illness to treat.1 The overall evidence from treatment trials in bipolar depression is sparse, and the role of antidepressants and their efficacy remains controversial.2, 3, 4, 5 Adjunctive treatment with thyroid hormone is one approach for treatment-refractory bipolar disorders. Such use of levothyroxine (L-T4) at supraphysiologic doses has offered promise in several open-label studies, including rapid cycling,6 prophylaxis-resistant bipolar patients7 and for patients with refractory uni- or bipolar depression.8
The hypothesis driving these studies was that increasing the availability of thyroid hormones to the brain changes the phenotypic expression of the disorder and is associated with improvement of mood and cognition.9 Supporting this hypothesis are observations that suboptimal thyroid hormone levels have been associated with an unfavorable acute and longer-term treatment outcome in patients with bipolar disorders.10, 11, 12 In a pilot study of women with bipolar depression, the decline in depression in those treated with L-T4 was significantly associated with changes in regional cerebral glucose metabolism in limbic and subcortical circuits, brain areas that are integral to the regulation of affect and cognition.13 Specifically, treatment with supraphysiologic doses of L-T4 decreased relative activity in the subgenual cingulate cortex, thalamus, amygdala, hippocampus, dorsal and ventral striatum, and the cerebellar vermis. Furthermore, it was demonstrated that the decrease in relative activity in the latter brain regions was significantly correlated with reduction in depression scores.13
The aims of this randomized, placebo-controlled double-blind study of euthyroid bipolar depressed patients were to test the hypotheses that treatment with adjunctive supraphysiologic doses of L-T4 would be more effective than placebo treatment (reduction in depressive symptoms), and that clinical improvement would be more associated with reduction in relative regional cerebral metabolism in pre-defined limbic and subcortical regions, as compared with the corresponding changes in placebo-treated patients. A secondary hypothesis was that there would be a greater reduction in relative brain activity in these pre-defined regions after L-T4 as compared with placebo treatment.
Materials and methods
Study design
This 6-week, double-blind, randomized, placebo-controlled study assessed the efficacy of L-T4 (300 mcg per day, fixed dose) in bipolar depressed patients who had failed a course of treatment with mood stabilizer and/or antidepressant medication. The study was part of a larger multisite clinical trial (registered with ClinicalTrials.gov, identifier: NCT01528839).14 Participants in the study reported here (n=25; 15 with bipolar disorder type I and 10 with bipolar disorder type II) were recruited from a single site in Berlin, where positron emission tomography (PET) technology was available. Image analyses were performed at the Laboratory of Molecular Imaging, Semel Institute for Neuroscience and Human Behavior, University of California Los Angeles.
Clinical response was measured by the change in Hamilton Rating Scale for Depression (HamD17) total score from randomization to completion of treatment. Brain function was inferred from normalized, decay-corrected raw counts from the radiotracer [F-18]fluorodeoxyglucose (FDG) as a surrogate index of glucose metabolism. Relative activity, as used in this report, refers to this measure.
The study was approved by the local institutional review board (Ethical Committee at Charité–Universitätsmedizin Berlin) and performed in accordance with the current amendment of the Declaration of Helsinki and the International Conference on Harmonization/Good Clinical Practice guidelines. Written informed consent was obtained from all subjects.
Subjects
Research participants were 18–65 years of age and diagnosed with bipolar disorder, type I or II, according to the DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, Fourth EditionIV). The patients in this study had failed to respond to at least 6 weeks of treatment with a mood stabilizer and/or antidepressant (see below) at standard doses according to an international guideline.15 They were required at both the screening and randomization assessments to have an overall score ⩾14 on the HamD17,16 a HamD item 1 (depressed mood) score⩾2 and a Young Mania Rating Scale17 score ⩽12. Serum levels of lithium were required to be within therapeutic ranges (0.5–0.8 mmol l−1) for at least 2 weeks before enrollment in this study of adjunctive thyroid hormone treatment.
Patients who met any of the following criteria were excluded: (1) an axis I disorder other than bipolar disorder, (2) ultra-rapid cycling, defined as ⩾12 episodes in the previous year, (3) psychotic features, (4) a diagnosis of substance dependence or substance use (except for nicotine) over the previous year, (5) a clinically significant current medical illness, or (6) current or past thyroid disease or thyroid hormone treatment. Serum thyroid hormone (free thyroxine (fT4) and free triiodothyronine (fT3)) and thyroid-stimulating hormone (TSH) levels were required to fall within the normal reference range of the laboratory (fT4: 0.9–1.9 ng dl−1; fT3: 2.6–5.1 ng l−1; TSH 0.27–4.2 mU l−1) in order to exclude subthreshold thyroid disease.
Procedures
Following a screening interview, subjects meeting preliminary entry criteria were invited to participate. After providing written informed consent, participants received a psychiatric interview supplemented by the Structured Clinical Interview for DSM-IV Axis I Disorders,18 to confirm the diagnosis of bipolar disorder, a complete medical and physical examination, a routine laboratory evaluation (thyroid function tests, blood count, blood chemistry and urine drug screen), vital signs and a 12-lead electrocardiogram. Affective symptoms were assessed with the HamD17 and Young Mania Rating Scale. Participants were reassessed 1 week after the qualifying examination and, on still fulfilling study criteria, were randomized to receive adjunctive L-T4 (n=15) or placebo (n=10) for a double-blind 6-week period. L-T4 or placebo was administered orally each day before breakfast. L-T4 was administered at 100 mcg per day during week 1,200 mcg per day during week 2 and 300 mcg per day during weeks 3–6. Placebo and active tablet packaging were identical in appearance.
At study entry, patients in both groups were receiving a variety of psychotropic medications (there were no significant group differences); all 25 patients received at least one mood stabilizer (lithium, carbamazepine, valproate, lamotrigine or an atypical antipsychotic approved for bipolar disorder), except for two bipolar II patients who received only one antidepressant (duloxetine or nortriptyline). Fifteen patients received two psychotropic medications, seven received three and one patient received four. The medications in the group that received adjunctive L-T4 treatment were as follows: buproprione, n=1 (300 mg per day); carbamazepine, n=2 (400–600 mg per day); citalopram, n=1 (60 mg per day); duloxetine, n=1 (120 mg per day); lamotrigine, n=3 (100–150 mg per day); lithium carbonate, n=7 (600–1200 mg per day); mirtazapine, n=1 (30 mg per day); nortriptyline, n=1 (100 mg per day); olanzapine, n=1 (10 mg per day); pregabaline, n=1 (500 mg per day); risperidone, n=1 (4 mg per day); sertraline, n=2 (100–150 mg per day); tranylcypromine, n=1 (20 mg per day); venlafaxine, n=2 (150–375 mg per day); valproate, n=1 (800 mg per day).
The medications in the group that received placebo treatment were as follows: amisulpride, n=1 (200 mg per day); amitriptyline, n=1 (750 mg per day); carbamazepine, n=1 (600 mg per day); citalopram, n=1 (40 mg per day); lamotrigine, n=4 (25–200 mg per day); lithium carbonate, n=4 (200–1200 mg per day); mirtazapine, n=1 (45 mg per day); olanzapine, n=1 (10 mg per day); quetiapine, n=1 (700 mg per day); venlafaxine, n=2 (225 g per day); valproate, n=2 (1200–1500 mg per day); ziprasidone, n=1 (80 mg per day). There was no change in treatment with any of these medications in either group 2 weeks prior randomization and throughout the study.
Zolpidem tartrate (5–10 mg per day at bedtime for insomnia) and lorazepam (1–3 mg per day for severe anxiety) were permitted at the discretion of the study physician during the first 3 weeks, but withheld within 8 h before any assessment was conducted. No other psychotropic drug (except the prescribed mood stabilizers and/or antidepressants listed above) was allowed during the study.
Clinical assessments were conducted at screening, baseline and at the end of each week in the 6-week treatment period. The measure of treatment efficacy was the mean change from baseline in HamD17 score. Adverse events were assessed from spontaneous self-reports. The clinician asked the subject whether any events, independent of any causal relationship, had come to attention, using the Thyroid Symptom List, a specific assessment of thyroid system-related side effects.19 Vital signs, weight, blood pressure and heart rate were obtained at each assessment. Electrocardiogram, clinical chemistry, hematology and thyroid function tests were conducted at screening and treatment weeks 2, 4 and 6.
Magnetic resonance imaging
T1 volumetric structural magnetic resonance imaging scans (3-T, General Electric, Fairfield, CT, USA) were acquired (spoiled-gradient-recalled acquisition, 256 × 256 matrix, TE=3.2 ms, TR=8 ms, angle=20 °, 2-mm slice thickness) for co-registration with PET data.
PET imaging
Each subject participated in two PET scanning sessions with FDG.20, 21 The first PET scan was acquired before treatment and the second after 6 weeks of L-T4 or placebo treatment. Thyroid status and psychiatric ratings were assessed on the morning of each PET scan. Before each PET measurement, a catheter was inserted into the antecubital vein for FDG infusion. Measured blood glucose levels were<5.6 mmol l−1 in all cases.
To provide a consistent, affectively neutral cognitive set during measurement of cerebral activity and to control for variance optimally, all participants performed an auditory continuous performance task (CPT) during the radiotracer uptake period. The CPT required discrimination of rare higher-pitched ‘target’ tones presented within a sequence (inter-tone interval=2 s) of more frequent lower-pitched distracting tones. A button was pressed to signify hearing a target tone.
Subjects performed the CPT while seated. Approximately 15 min after the CPT began, FDG (300 MBq) was administered as an intravenous bolus, followed by a 20-ml saline flush. Thirty minutes after the injection, the CPT was stopped and the subject was positioned in the scanner gantry. Brain images were acquired for 30 min (six 5-min frames), beginning 50 min after FDG injection.
Static PET brain images of 11 participants (L-T4 n=7 and placebo n=4) were acquired with a Siemens ECAT EXACT 47 tomograph (Siemens, Erlangen, Germany) in 33 planes in three-dimensional mode. Image reconstruction was performed by filtered back projection using a Hanning filter (cut-off 0.4) into a 128 × 128 matrix using a zoom of 2. A 10-min transmission scan using a 68Ge/68Ga rod source was performed for attenuation correction.
PET images of the other 14 participants (L-T4 n=8 and placebo n=6) were obtained in three-dimensional mode using a hybrid PET/computed tomography (CT) system consisting of a multislice CT and a full-ring PET system (Biograph 16, Siemens). The crystal and block dimensions were equal to those of the ECAT EXACT detectors, but different detector materials were used (LSO vs BGO). Intrinsic spatial resolution was comparable. Pre- and posttreatment PET scans were always acquired with the same PET scanner for a given patient. An unenhanced CT image (detector collimation 16 × 1.5 mm2, tube current 100 mA, tube voltage 120 kV and gantry rotation time 0.8 s) covering the entire head was performed for attenuation correction. PET emission data were reconstructed iteratively (OSEM algorithm, 6 iterations, 16 subsets) using a 128 × 128 matrix and a zoom of 2.
Data analysis
Differences between the treatment groups in demographic characteristics and baseline depressive symptoms (HamD17 score) were assessed using two-tailed Student’s t-test. The hypothesis that depressive symptoms would improve more after L-T4 than placebo treatment was assessed through a general linear mixed model. The first analysis modeled the effect of treatment group (two levels), treatment week (six levels) and their interaction on the difference scores resulting from subtracting each subject’s HamD17 score before treatment from the weekly HamD17 scores during treatment. A second general linear mixed model dropped the insignificant interaction term. Both models were corrected for age. Statistical significance for all analyses was set at α=0.05.
Relative activity, reflecting regional glucose metabolism, was compared between groups and between pre- and posttreatment assessments using Statistical Parametric Mapping 5 (refs 22, 23). Each reconstructed PET image was co-registered to the corresponding magnetic resonance imaging using Automated Image Registration.24 The magnetic resonance images were then used to normalize each subject’s PET data spatially by linear and nonlinear transformations,22 which warped the images into a standard coordinate system developed at the Montreal Neurological Institute space using a study-specific template. Normalized images were then smoothed with an 8-mm (full width at half maximum) isotropic Gaussian kernel. The effects of global activity were removed from consideration by proportional scaling.
On the basis of our previous study of L-T4-treated patients with bipolar depression,13 we identified 12 volumes of interest (VOI) where we expected decreases in relative activity after L-T4 treatment, and the decreases being proportional to improvement in depressive symptoms. These regions were the thalamus, amygdala, hippocampus, dorsal striatum and the ventral striatum, measured in each cerebral hemisphere, subgenual cingulate cortex and the midline cerebellar vermis. The VOIs were drawn on the structural magnetic resonance template provided in Statistical Parametric Mapping 5, using MEDx software (Sensor Systems, Sterling, VA, USA) aided by use of the Talairach and Tournaux atlas25 and the Human Brain atlas of Duvernoy.26 In combination, the 12 VOIs constituted 7,349 voxels representing 3.9% of the analyzed whole brain volume.
We used the Statistical Parametric Mapping 5 small volume correction. The voxel height threshold for inclusion in statistical parametric maps was P=0.05 (uncorrected). A VOI was considered to show a significant effect only if the probability of obtaining the peak voxel height was P<0.05 after family-wise error correction for the number of voxels in the VOI.
The first SPM analysis explored the effects of treatment on relative brain activity. The interaction of treatment group (L-T4 vs placebo) with treatment session (pre vs post) was evaluated. A second SPM analysis split each treatment group into responders and non-responders, as defined by a ⩾50% reduction in HamD17 scores after treatment.
A third SPM analysis assessed the degree to which change in relative activity after treatment was correlated with change in depressed depressive symptoms (HamD17). In each analysis, age and gender were modeled as covariates of no interest. Separate contrasts for each group assessed the differences in relative activity between sessions and the relationship of these changes to depressive symptoms.
We also noted which effects maintained statistical significance after applying the Bonferroni correction for the number of regions assessed (five bilateral regions and two midline volumes). This evidentiary criterion (0.05/12=0.0042) is overly conservative, because it assumes tests of the individual VOIs are independent of one another, which is highly unlikely in this type of data.
Results
Characteristics of participants
The treatment groups did not differ significantly in gender (female vs male: L-T4 group n=8 vs n=7; placebo group n=4 vs n=6), type of bipolar disorder (type I and II), education, ethnicity or handedness. HamD17 scores before initiation of treatment (L-T4: 21.7±3.2; placebo: 20.3±6.3) were also equivalent between the groups as assessed by two-tailed t-test (P=0.48). However, participants in the placebo group were older than those in the L-T4 group (mean 51.8±11.4 years vs 41.3±12.4; t (two-tailed t=2.15, P=0.042). All subsequent analyses were corrected for age.
Treatment outcome
Figure 1 demonstrates the change in HamD17 total score from randomization over time (6 weeks). General linear mixed model analysis revealed a significant effect of treatment group (F1,117=9.98, P=0.002) and treatment week (F5,43=4.71, P=0.002), but no significant Group × Week interaction (F5,43=0.93, P=0.469) or effect of age (F1,79=0.31, P=0.581). A second general linear mixed model without the interaction term retained significant effects of treatment group (F1,83=6.30, P=0.014) and treatment week (F5,44=5.47, P=0.001).

Change in Hamilton Rating Scale for Depression (HamD17) total score from randomization over time (6 weeks). Baseline (week 0) HamD17 score: levothyroxine (L-T4) vs placebo: 21.7 vs 20.3, at week 6: difference between groups 3.7 (L-T4 vs placebo: 12.6 vs 16.3).
At baseline, all thyroid axis hormone levels (fT4, fT3 and TSH) fell in the normal range of the laboratory. With L-T4 treatment (300 mcg per day), thyroid hormone levels increased significantly (free T4: from 1.11±0.26 to 2.53±0.67 ng dl−1, P<0.01; free T3: from 2.80±0.77 to 5.62±1.05 ng dl−1, P<0.01) and basal TSH levels decreased significantly (from 2.35±0.94 to 0.02±0.15 mU l−1; P<0.001), but not with placebo treatment (fT4: from 1.14±0.14 to 1.09±0.19 ng dl−1; fT3: from 3.39±1.07 to 3.23±0.41 ng dl−1; and basal TSH: from 1.34±0.61 to 1.53±0.76 mU l−1). Blood pressure, heart rate and body weight did not change significantly with either treatment. L-T4 treatment was well tolerated, with no serious adverse events or side effects that warranted discontinuation of treatment (data not shown).
Change in relative brain metabolism after treatment
Table 1 presents and Figure 2 depicts changes in relative regional activity of the preselected VOIs from the pre- to posttreatment session for each treatment group. At the 0.05 α-level, there were no areas where relative activity increased after treatment in either group. In patients treated with L-T4, activity decreased after treatment in a large part of all the preselected regions-of-interest areas (see Materials and methods) comprising 65% of the total assessed voxels. There were significant decreases in 10 of the 12 VOIs. Effects in the left thalamus, right amygdala, right hippocampus, left ventral striatum and the right dorsal striatum retained significance after Bonferroni correction for the number of regions assessed (0.05/12=0.0042).

Brain areas where relative activity changed after levothyroxine (L-T4) treatment or placebo. Colors superimposed on a gray-scale structural magnetic resonance template indicate areas where relative metabolism decreased after, as compared with that before treatment (t⩾1.69; P<0.05), in bipolar disorder patients treated with L-T4 (top row), placebo (center row), or where the decrease was greater in the L-T4 than placebo group (bottom row). Coordinates are in Montreal Neurological Institute (MNI) space depicted in neurological orientation. PLA, placebo.
Activity decreased significantly after placebo treatment in 11% of the assessed voxels, with a significant regional decrease in the right amygdala. Table 1 and Figure 2 show that parts of some VOIs, particularly within the right thalamus, appeared to decrease more in activity after treatment in the L-T4 as compared with the placebo group, but formal comparisons of group differences (interaction of PET session with group) attained the α-level in only 6% of assessed voxels and no VOI showed a significant effect after volume correction.
When the groups were split into responders and non-responders, there were seven non-responders in the placebo group (mean HamD decrease=16%, s.d.=61%) and three responders (mean HamD decrease=70%, s.d.=11%). There were eight non-responders in the L-T4 group (mean HamD decrease=32%, s.d.=15%) and seven responders (mean HamD decrease=67%, s.d.=13%).
The group of three was too small for meaningful statistical comparison but decreases in relative cerebral activity after treatments were quantified separately in the other three groups. In placebo-treated non-responders, 10% of the total assessed voxels were decreased at P<0.05, but no VOIs retained significant decreases after volume correction. In L-T4-treated non-responders, 24% of the total voxels decreased at P<0.05, and there were significant decreases in 4 of 12 VOIs (right amygdala P=0.016, right hippocampus P=0.019, right ventral striatum P=0.028, right dorsal striatum P=0.025). In L-T4-treated responders, 60% of the voxels decreased at P<0.05, with significant decreases in 8 of 12 VOIs (left thalamus P=0.001, right thalamus P=0.007, left amygdala P=0.040, right amygdala P=0.027, right hippocampus P=0.040, left ventral striatum P=0.017, left dorsal striatum P=0.014 and cerebellar vermis P=0.015). Comparing L-T4-treated responders and non-responders revealed a larger decrease after treatment in the right thalamus of responders (P=0.037). There were no significant differences in metabolic change between non-responders treated with L-T4 and with placebo.
Symptom-related change in relative brain metabolism after treatment
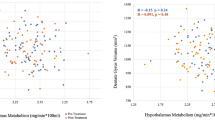
To test the primary hypothesis, symptom-related changes in relative metabolism after treatment were examined. Table 2 presents and Figure 3 depicts VOIs with significant correlation between changes from the pre- to posttreatment session in relative regional activity and depressive symptoms assessed with the HamD17 score. There were no areas with inverse correlation between change in depressive symptoms and brain activity change. In the L-T4 group, relative activity decreased as depressive symptoms improved (for example, positive correlation, as lower HamD17 scores indicate better mood) in all VOIs (P-values range from 0.04 to<0.0005). In the left thalamus, left dorsal striatum and the midline subgenual cingulate, the volume-corrected effects retained significance after Bonferroni correction for the number of regions assessed. In contrast, change in depressive symptoms after treatment was not correlated with activity change in any VOI of the placebo group.

Brain areas where change in relative activity after treatment was correlated with change in depressed mood (Hamilton Rating Scale for Depression (HamD17)). Colors superimposed on a gray-scale structural magnetic resonance template indicate areas from whole-brain analysis of patients with bipolar disorder where change in relative metabolism from before to after treatment was directly correlated (t≥1.69; P<0.05) with change in HamD17 scores in the levothyroxine (L-T4 group; top row), placebo group (center row), or where the correlation was greater in L-T4 than placebo-treated patients (bottom row). Coordinates are in Montreal Neurological Institute (MNI) space depicted in neurological orientation. There were no areas where change in activity was inversely correlated with change in HamD17 scores. PLA, placebo.
Table 2 and Figure 3 suggest that portions of several VOIs featured more positive correlation of pre- to posttreatment changes between cerebral activity and depressive symptoms after L-T4 as compared with placebo treatment. Formal comparisons were significant in the right thalamus, left thalamus and the left ventral striatum. Across all VOI voxels, 86% showed P<0.05 correlations in the L-T4 group, but only 2% showed such correlations in the placebo group; 28% showed correlations that were larger in the L-T4 than the placebo group.
Discussion
This report is the first randomized, placebo-controlled study in euthyroid bipolar patients with refractory depression employing functional brain imaging (FDG–PET) to investigate the effects of adjunctive L-T4 treatment on regional brain metabolism. The addition of supraphysiologic doses of L-T4 (300 mcg per day) to an otherwise stable medication regimen of standard treatments resulted in a significant decline in depression scores during the 6-week, double-blind treatment phase. At endpoint (week 6), the mean HamD score showed a group difference of 3.7 points in favor of L-T4. Such difference is generally considered to be clinically meaningful in a short-term treatment trial for major depression. NICE used a 3.0-point difference in HamD change scores as a criterion of clinical significance.27
The major biological findings of this study are that L-T4, as compared with placebo, yields greater clinical improvement in depression, and that this improvement is strongly correlated with metabolic changes in areas of the anterior limbic network, with pronounced effects in the thalamus, striatum and the subgenual cortex.
Functional brain imaging studies (functional magnetic resonance imaging and PET studies) in depression have provided evidence for a dysfunctional interaction between frontal lobe activity and the anterior limbic network, specifically those interconnected prefrontal, limbic and the striatal regions essential for emotional homeostasis. These regions include the amygdala, hippocampus, thalamus, anterior cingulate cortex, orbitofrontal, ventrolateral and dorsolateral prefrontal cortex, and the striatum.28 In our previous pilot study of L-T4 in patients with bipolar depression, which was conducted without a patient control group,13 it was not possible to differentiate to what degree changes in depression and related change in brain metabolic activity were directly in response to L-T4, or occurred during the natural course of the disorder. This study employing a placebo–control group differentiates that the changes observed are in high probability directly related to the adjunctive L-T4.
The most pronounced differences between effects of L-T4 treatment and placebo on brain metabolic activity were the correlations between clinical and metabolic changes in the thalamus and the ventral striatum. These changes in the active L-T4 treatment group appear associated with improved depressive symptoms.
Both the thalamus and ventral striatum have been shown previously to have abnormally high glucose metabolism in depressed bipolar patients compared with healthy controls,13, 29, 30 which normalized after effective treatment with L-T4 (ref. 13). A recent review of functional magnetic resonance imaging investigations of bipolar disorder concluded that the most consistent abnormalities are activation of the thalamus and the striatum. It has been hypothesized that excessive activation of an anterior limbic network may disturb emotional homeostasis and lead to dysregulation of positive and negative feedback loops in patients with bipolar disorder.28
One limitation of this study is that it was a necessary subset of a larger multi-center clinical study, because PET imaging was only available at the Berlin site. This sample of convenience had the downside of yielding both unequal sample sizes (15 vs 10) and also age differences between the groups. The relatively small sample sizes precluded the quantification of gender effects. Despite these limitations, for the first time, in this randomized, placebo-controlled trial of depressed bipolar patients, cerebral metabolic changes are demonstrated with the use of adjunctive L-T4 treatment.
As in previous studies, the hyperthyroxinemia induced by L-T4 treatment was well tolerated and led to a doubling of fT4 and fT3 levels (with both hormones being slightly above the reference range), while TSH was suppressed as expected after 6 weeks of L-T4 treatment. Even in bipolar patients treated with supraphysiologic doses of L-T4 for extended periods, no serious effects, including loss of bone mineral density, were observed in those previous studies.31, 32 The low incidence of adverse effects and high tolerability reported by patients with bipolar disorders, who are receiving high-dose thyroid hormone therapy, contrasts with that typically seen in patients with primary thyroid disease or healthy controls. As part of an ongoing effort to define tolerability and safety parameters of supraphysiologic L-T4, we found that under comparable conditions and doses healthy subjects and depressed patients respond differently to L-T4: depressed patients exhibit less elevation in the serum levels of thyroid hormones and show fewer side effects.33 However, in spite of overall good tolerability, treatment with supraphysiologic L-T4 requires selection of adequate patients with a good general physical health status (especially the absence of severe cardiac disease, arrhythmia in particular) and close (cardiac) monitoring. Given the overall lack of placebo-controlled data in this area of bipolar depression, we recommend to use adjunctive L-T4 at a dose of up to 300 mcg per day (depending on individual tolerability) as one option in difficult-to-treat depressed patients and in non-responders to standard treatment approaches, respectively.
Although we are only beginning to understand the mechanisms through which thyroid hormones exert their behavioral effects, such as those demonstrated in this paper, the brain’s independence of peripheral thyroid metabolism suggests that an understanding of their therapeutic efficacy requires further central nervous system investigation. As part of the nuclear superfamily of ligand-modulated transcription factors, thyroid hormones bind to nuclear receptors34 where they control, and usually increase, gene expression influencing a broad array of metabolic processes.35 Genes that are regulated by thyroid hormones are known to encode for proteins essential for important brain function such as myelin and neurotrophines. Non-genomic actions after binding to cytoplasmic thyroid hormone receptors include rapid activation of the phosphatidylinositol-3-protein kinase pathway and thereby achievement of vasodilatory and neuroprotective effects.36
Thyroid hormone receptors are widely distributed in the brain with high concentrations in the cerebral cortex, hippocampus and the amygdala,37 the latter being limbic structures that are implicated in the pathogenesis of mood disorders. The regulation of thyroid hormone homeostasis in the brain underlies a complex interaction of different mechanisms, some of which overlap with mechanisms involved in affect regulation.
The activity of specific thyroid hormone transporters (for example, monocarboxylate transporter 8) as clarified in recent research38, and the carrier transthyretin, are involved in determining intracellular concentrations of thyroid hormones via mediating their cellular influx and efflux.39 Deiodinases control regional effectivity of T3 in concert with other mechanisms,40 that is, the local distribution of the different nuclear thyroid hormone receptors TRα and TRβ.37 Deficits in any one, or several, of these mechanisms may result in reduced bioavailability of thyroid hormones at cerebral target regions despite normal peripheral serum levels of thyroid hormones. This condition has been conceptualized as ‘central hypothyroidism’. Compensation for this putative ‘central hypothyroidism’ might be one reason why a proportion of euthyroid depressed patients benefit from administration of supraphysiologic doses of L-T4. Interestingly, mice suffering from central hypothyroidism caused by a mutation of the TRα1 gene,41 showed reduced neuronal density, resulting in reduced cortical thickness in the hippocampal CA1 region.42 Behaviorally, these mice show increases in surrogate animal markers for depression and anxiety, as well as an increased startle response. Both the behavioral and neural density measures normalized with thyroid hormone administration.41, 43
As noted earlier, limbic system structures where thyroid hormone receptors are prevalent have been implicated in the pathogenesis of mood disorders. However, the functional pathways through which thyroid hormones modulate such depressive symptoms are poorly understood. Interactions of the thyroid and neurotransmitter systems, primarily norepinephrine and serotonin, which are generally believed to have a major role in the regulation of mood and behavior, may contribute to the mechanism of action in the developing and mature brain.33, 44 In particular, there is robust evidence from animal research that thyroid hormones have a modulatory effect leading to an increase in serotonergic neurotransmission.33 Thyroid hormones also interact with other neurotransmitter systems involved in mood regulation, including dopamine postreceptor and signal-transducing processes, as well as gene regulatory mechanisms.45
Further research is clearly warranted. Despite the clinical evidence of a close relationship between low thyroid status and behavioral disturbance, known for more than 100 years, metabolic effects of thyroid hormones in the adult mammalian brain have rarely been investigated in vivo.46 In part, this lack of curiosity may be traced to reports in the 1950s and 1960s, which suggested that oxygen consumption in the mature human brain did not change with thyroid status. However, the absence of a technology capable of direct in vivo measurement of brain thyroid metabolism is also responsible. Such definitive technology still does not exist. The evaluation of cerebral blood flow and metabolism by functional brain imaging techniques, employing selective radioligand binding to receptors of interest in the brain, however, offers a starting point. This study demonstrates that further metabolic study of the adjunctive use of thyroid hormones in mood disorder offers promising insights into the thyroid–brain relationship.
References
Judd LL, Akiskal HS, Schettler PJ, Endicott J, Maser J, Solomon DA et al. The long-term natural history of the weekly symptomatic status of bipolar I disorder. Arch Gen Psychiatry 2002; 59: 530–537.
Sidor MM, MacQueen GM . Antidepressants for the acute treatment of bipolar depression: a systematic review and meta-analysis. J Clin Psychiatry 2011; 72: 156–167.
Bauer M, Ritter P, Grunze H, Pfennig A . Treatment options for acute depression in bipolar disorder. Bipolar Disord 2012; 14: 37–50.
Pacchiarotti I, Bond DJ, Baldessarini RJ, Nolen WA, Grunze H, Licht RW et al. The International Society for Bipolar Disorders (ISBD) task force report on antidepressant use in bipolar disorders. Am J Psychiatry 2013; 170: 1249–1262.
Cerullo MA, Strakowski SM . A systematic review of the evidence for the treatment of acute depression in bipolar I disorder. CNS Spectr 2013; 18: 199–208.
Bauer MS, Whybrow PC . Rapid cycling bipolar affective disorder. II. Treatment of refractory rapid cycling with high-dose levothyroxine: a preliminary study. Arch Gen Psychiatry 1990; 47: 435–440.
Bauer M, Berghofer A, Bschor T, Baumgartner A, Kiesslinger U, Hellweg R et al. Supraphysiological doses of L-thyroxine in the maintenance treatment of prophylaxis-resistant affective disorders. Neuropsychopharmacology 2002; 27: 620–628.
Bauer M, Hellweg R, Graf KJ, Baumgartner A . Treatment of refractory depression with high-dose thyroxine. Neuropsychopharmacology 1998; 18: 444–455.
Bauer M, Goetz T, Glenn T, Whybrow PC . The thyroid-brain interaction in thyroid disorders and mood disorders. J Neuroendocrinol 2008; 20: 1101–1114.
Frye MA, Denicoff KD, Bryan AL, Smith-Jackson EE, Ali SO, Luckenbaugh D et al. Association between lower serum free T4 and greater mood instability and depression in lithium-maintained bipolar patients. Am J Psychiatry 1999; 156: 1909–1914.
Cole DP, Thase ME, Mallinger AG, Soares JC, Luther JF, Kupfer DJ et al. Slower treatment response in bipolar depression predicted by lower pretreatment thyroid function. Am J Psychiatry 2002; 159: 116–121.
Frye MA, Yatham L, Ketter TA, Goldberg J, Suppes T, Calabrese JR et al. Depressive relapse during lithium treatment associated with increased serum thyroid-stimulating hormone: results from two placebo-controlled bipolar I maintenance studies. Acta Psychiatr Scand 2009; 120: 10–13.
Bauer M, London ED, Rasgon N, Berman SM, Frye MA, Altshuler LL et al. Supraphysiological doses of levothyroxine alter regional cerebral metabolism and improve mood in bipolar depression. Mol Psychiatry 2005; 10: 456–469.
Stamm TJ, Lewitzka U, Sauer C, Pilhatsch M, Smolka MN, Koeberle U et al. Supraphysiologic doses of levothyroxine as adjunctive therapy in bipolar depression: a randomized, double-blind, placebo-controlled study. J Clin Psychiatry 2014; 75: 162–168.
Bauer M, Bschor T, Pfennig A, Whybrow PC, Angst J, Versiani M et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological Treatment of Unipolar Depressive Disorders in Primary Care. World J Biol Psychiatry 2007; 8: 67–104.
Hamilton M . A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23: 56–62.
Young RC, Biggs JT, Ziegler VE, Meyer DA . A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry 1978; 133: 429–435.
First MB, Spitzer RL, Gibbon M, Williams JBW . Structured Clinical Interview for DSM-IV Axis I Disorders (SCID), Clinician Version American Psychiatric Press: Washington, DC, 1996.
Bauer M, Baur H, Berghofer A, Strohle A, Hellweg R, Muller-Oerlinghausen B et al. Effects of supraphysiological thyroxine administration in healthy controls and patients with depressive disorders. J Affect Disord 2002; 68: 285–294.
Reivich M, Kuhl D, Wolf A, Greenberg J, Phelps M, Ido T et al. The [18 F]fluorodeoxyglucose method for the measurement of local cerebral glucose utilization in man. Circ Res 1979; 44: 127–137.
Phelps ME, Huang SC, Hoffman EJ, Selin C, Sokoloff L, Kuhl DE . Tomographic measurement of local cerebral glucose metabolic rate in humans with (F-18)2-fluoro-2-deoxy-D-glucose: validation of method. Ann Neurol 1979; 6: 371–388.
Friston KJ, Ashburner J, Poline JB, Frith CD, Heather JD, Frackowiak RS . Spatial registration and normalization of images. Hum Brain Mapp 1995; 2: 165–189.
Friston KJ, Holmes AP, Worsley KJ, Poline JB, Frith CD, Frackowiak RS . Statistical parametric maps in functional imaging: a general linear approach. Hum Brain Mapp 1995; 2: 189–210.
Woods RP, Mazziotta JC, Cherry SR . MRI-PET registration with automated algorithm. J Comput Assist Tomogr 1993; 17: 536–546.
Talairach J, Tournoux P . Co-Planar Stereotaxic Atlas of the Human Brain. Thieme: New York, 1988.
Duvernoy HM . The Human Brain. Surface, Three-Dimensional Sectional Anatomy with MRI, and Blood Supply2nd ednSpringer: Wien, 1999.
NICE Depression: Management of Depression in Primary and Secondary Care. Clinical Practice Guideline Number 23.. National Institute for Clinical Excellence: London, 2004.
Cerullo MA, Adler CM, DelBello MP, Strakowski SM . The functional neuroanatomy of bipolar disorder. Int Rev Psychiatry 2009; 21: 314–322.
Baxter LR Jr ., Schwartz JM, Phelps ME, Mazziotta JC, Guze BH, Selin CE et al. Reduction of prefrontal cortex glucose metabolism common to three types of depression. Arch Gen Psychiatry 1989; 46: 243–250.
Ketter TA, Kimbrell TA, George MS, Dunn RT, Speer AM, Benson BE et al. Effects of mood and subtype on cerebral glucose metabolism in treatment-resistant bipolar disorder. Biol Psychiatry 2001; 49: 97–109.
Bauer M, Fairbanks L, Berghofer A, Hierholzer J, Bschor T, Baethge C et al. Bone mineral density during maintenance treatment with supraphysiological doses of levothyroxine in affective disorders: a longitudinal study. J Affect Disord 2004; 83: 183–190.
Ricken R, Bermpohl F, Schlattmann P, Bschor T, Adli M, Monter N et al. Long-term treatment with supraphysiological doses of thyroid hormone in affective disorders - effects on bone mineral density. J Affect Disord 2012; 136: e89–e94.
Bauer M, Heinz A, Whybrow PC . Thyroid hormones, serotonin and mood: of synergy and significance in the adult brain. Mol Psychiatry 2002; 7: 140–156.
Lechan RM, Toni R . Thyroid hormones in neural tissue. In: Pfaff DW, Arnold AP, Etgen AM, Fahrbach SE, Rubin RT eds Hormones, Brain and Behavior. Academic Press: San Diego, 2002; pp 157–238.
Bernal J . Action of thyroid hormone in brain. J Endocrinol Invest 2002; 25: 268–288.
Hiroi Y, Kim HH, Ying H, Furuya F, Huang Z, Simoncini T et al. Rapid nongenomic actions of thyroid hormone. Proc Natl Acad Sci USA 2006; 103: 14104–14109.
Williams GR . Neurodevelopmental and neurophysiological actions of thyroid hormone. J Neuroendocrinol 2008; 20: 784–794.
Friesema EC, Grueters A, Biebermann H, Krude H, von Moers A, Reeser M et al. Association between mutations in a thyroid hormone transporter and severe X-linked psychomotor retardation. Lancet 2004; 364: 1435–1437.
Hennemann G, Docter R, Friesema EC, de Jong M, Krenning EP, Visser TJ . Plasma membrane transport of thyroid hormones and its role in thyroid hormone metabolism and bioavailability. Endocr Rev 2001; 22: 451–476.
Visser TJ . Thyroid hormone transporters. Horm Res 2007; 68: 28–30.
Venero C, Guadano-Ferraz A, Herrero AI, Nordstrom K, Manzano J, de Escobar GM et al. Anxiety, memory impairment, and locomotor dysfunction caused by a mutant thyroid hormone receptor alpha1 can be ameliorated by T3 treatment. Genes Dev 2005; 19: 2152–2163.
Alva-Sanchez C, Ortiz-Butron R, Pacheco-Rosado J . Kainic acid does not affect CA3 hippocampal region pyramidal cells in hypothyroid rats. Brain Res Bull 2004; 63: 167–171.
Pilhatsch M, Winter C, Nordstrom K, Vennstrom B, Bauer M, Juckel G . Increased depressive behaviour in mice harboring the mutant thyroid hormone receptor alpha 1. Behav Brain Res 2010; 214: 187–192.
Whybrow PC, Prange AJ Jr . A hypothesis of thyroid-catecholamine-receptor interaction. Its relevance to affective illness. Arch Gen Psychiatry 1981; 38: 106–113.
Yen PM, Brent GA . Genomic and nongenomic actions of thyroid hormones. In: Braverman LE, Cooper DS eds Werner & Ingbar’s The Thyroid. A Fundamental and Clinical Text10th ednWilliams & Wilkins: Philadelphia, 2013 p 127–138.
Bauer M, Whybrow PC . Thyroid hormone, brain, and behavior. In: Pfaff DW, Arnold AP, Etgen AM, Fahrbach SE, Rubin RT eds Hormones, Brain and Behavior. Academic Press: San Diego, 2002 p 238–264.
Acknowledgements
The study was sponsored by the Stanley Medical Research Institute (grant 02T-238 to MB) and the National Alliance for Research on Schizophrenia and Depression (NARSAD) Independent Investigator Award (to MB).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Preliminary reports were presented at the 50th Annual Meeting of the American College of Neuropsychopharmacology (4–8 December 2011, Waikoloa, HI, USA).
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Bauer, M., Berman, S., Stamm, T. et al. Levothyroxine effects on depressive symptoms and limbic glucose metabolism in bipolar disorder: a randomized, placebo-controlled positron emission tomography study. Mol Psychiatry 21, 229–236 (2016). https://doi.org/10.1038/mp.2014.186
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/mp.2014.186
- Springer Nature Limited
This article is cited by
-
Changes in regulators of lipid metabolism in the brain: a study of animal models of depression and hypothyroidism
Pharmacological Reports (2022)
-
Role of thyroid hormone therapy in depressive disorders
Journal of Endocrinological Investigation (2021)
-
Targeting Hormones for Improving Cognition in Major Mood Disorders and Schizophrenia: Thyroid Hormones and Prolactin
Clinical Drug Investigation (2020)
-
Treatment of bipolar depression with supraphysiologic doses of levothyroxine: a randomized, placebo-controlled study of comorbid anxiety symptoms
International Journal of Bipolar Disorders (2019)
-
Thyroid Hormone Treatment of Mood Disorders
Current Treatment Options in Psychiatry (2018)