
Abstract
Background
Childhood obesity is a complex multifaceted condition, which is influenced by genetics, environmental factors, and their interaction. However, these interactions have mainly been studied in twin studies and evidence from population-based cohorts is limited. Here, we analyze the interaction of an obesity-related genome-wide polygenic risk score (PRS) with sociodemographic and lifestyle factors for BMI and waist circumference (WC) in European children and adolescents.
Methods
The analyses are based on 8609 repeated observations from 3098 participants aged 2–16 years from the IDEFICS/I.Family cohort. A genome-wide polygenic risk score (PRS) was calculated using summary statistics from independent genome-wide association studies of BMI. Associations were estimated using generalized linear mixed models adjusted for sex, age, region of residence, parental education, dietary intake, relatedness, and population stratification.
Results
The PRS was associated with BMI (beta estimate [95% confidence interval (95%—CI)] = 0.33 [0.30, 0.37], r2 = 0.11, p value = 7.9 × 10−81) and WC (beta [95%—CI] = 0.36 [0.32, 0.40], r2 = 0.09, p value = 1.8 × 10−71). We observed significant interactions with demographic and lifestyle factors for BMI as well as WC. Children from Southern Europe showed increased genetic liability to obesity (BMI: beta [95%—CI] = 0.40 [0.34, 0.45]) in comparison to children from central Europe (beta [95%—CI] = 0.29 [0.23, 0.34]), p-interaction = 0.0066). Children of parents with a low level of education showed an increased genetic liability to obesity (BMI: beta [95%—CI] = 0.48 [0.38, 0.59]) in comparison to children of parents with a high level of education (beta [95%—CI] = 0.30 [0.26, 0.34]), p-interaction = 0.0012). Furthermore, the genetic liability to obesity was attenuated by a higher intake of fiber (BMI: beta [95%—CI] interaction = −0.02 [−0.04,−0.01]) and shorter screen times (beta [95%—CI] interaction = 0.02 [0.00, 0.03]).
Conclusions
Our results highlight that a healthy childhood environment might partly offset a genetic predisposition to obesity during childhood and adolescence.
Similar content being viewed by others
Introduction
Obesity is a complex multifaceted condition and its prevalence has been increasing continuously over previous decades most likely due to adverse changes of environmental and demographic factors [1]. Studies in twins have suggested that genetic factors explain ~40–80% of the variation in obesity susceptibility [2]. Twin studies have further suggested that obesity-predisposing genes are not deterministic, but they rather interact with a variety of environmental and lifestyle factors. In particular, the heritability of BMI has been shown to be higher among children living in obesogenic home environments [3,4,5,6], children whose parents have lower education levels [7] and young adults with a sedentary lifestyle [8, 9]. An alternative to the traditional twin study design is genome-wide associations studies (GWAS), which have revolutionized the field of complex disease genetics over the past decade, providing numerous compelling associations for obesity [10, 11] and other human complex traits and diseases [12]. GWAS have identified 751 genetic variants (single-nucleotide polymorphisms (SNPs)) in association with BMI [10, 11] and a subset of them has been used in gene–environment (G×E) interaction analyses to show that the genetic predisposition to obesity is attenuated by a healthy lifestyle including physical activity [13, 14] and adherence to healthy dietary patterns [14,15,16,17,18,19,20]. However, these genome-wide significant variants only account for a small portion of BMI variation (up to 6%) [10, 11], while genome-wide estimates suggest that common variation accounts for >20% of BMI variation [10]. Therefore, the polygenic nature of BMI is not reflected in the current literature of BMI-related G×E interactions, which could have decreased the statistical power to detect interactions. Khera et al. suggest that the power to predict BMI can be improved by using polygenic risk scores (PRSs) that include SNPs that do not reach the threshold for genome-wide significance and by using genome-wide approaches [21]. We hypothesize that using a PRS that captures the polygenic nature of BMI will enable us to validate the interactions that were found in twin studies [3,4,5,6,7,8,9] and possibly detect new G×E interactions that have not been found by previous studies.
Another gap in knowledge is that most previous G×E interaction studies primarily involved adults [8, 9, 13,14,15,16,17,18,19,20, 22, 23], so that little is known whether the inherited susceptibility to obesity is modified by environmental factors already during childhood and adolescence. Given that the weight trajectories of individuals in different PRS deciles start to diverge in early childhood [21], the identification of robust G×E interactions in children is particularly important to facilitate targeted strategies for obesity prevention early in life.
In this study, we will calculate the most recent PRS for BMI [21] and (1) show the variance explained by the PRS for BMI as well as for waist circumference of European children and adolescents and (2) analyze its interaction with parental education, region of residence, selected dietary variables, and physical activity to investigate to which degree the inherited susceptibility to obesity in children is modified by these sociodemographic and lifestyle factors. The analyses are based on 8609 repeated observations from 3098 children and adolescents aged 2–16 years from the pan-European IDEFICS/I.Family cohort.
Methods
Study population
The pan-European IDEFICS/I.Family cohort [24, 25] is a multi-center, prospective study on the association of social, environmental, and behavioral factors with children’s health status. Children were recruited through kindergarten or school settings in Belgium, Cyprus, Estonia, Germany, Hungary, Italy, Spain, and Sweden. In 2007/2008, 16,229 children aged between 2 and 9.9 years participated in the baseline survey. Follow-up surveys were conducted after 2 (FU1, N = 11,043 plus 2543 newcomers) and 6 years (FU2, N = 7117 plus 2512 newly recruited siblings). Questionnaires were completed by parents. In the second follow-up (FU2), adolescents of 12 years of age or older reported for themselves. The study was conducted in agreement with the Declaration of Helsinki; all procedures were approved by the local ethics committees and written and oral informed consents were obtained. Children were selected for a whole-genome scan based on their participation in the individual study modules. Children from Cyprus were not included in this initial genotyping to minimize population stratification.
Assessment of BMI and waist circumference
BMI was calculated as weight divided by height squared [kg/m²]. Height was measured to the nearest 0.1 cm by a SECA 225 Stadiometer (Seca GmbH & Co. KG., Hamburg, Germany) and body weight was measured in fasting state in light underwear on a calibrated scale accurate to 0.1 kg by a Tanita BC 420 SMA scale (TANITA, Tokyo, Japan). Waist circumference was measured in upright position with relaxed abdomen and feet together using an inelastic tape (Seca 200, Birmingham, UK), precision 0.1 cm, midway between the iliac crest and the lowest rib margin to the nearest 0.1 cm [26]. Age- and sex-specific BMI and waist circumference z-scores for children and adolescents were calculated using reference data from the International Obesity Task Force [27] and from British children [28], respectively. In addition, we proceeded as follows to dichotomize BMI and waist circumference (binary outcomes): As recommended by the International Obesity Task Force [27], we used age- and sex-specific cutoff values for obesity based on the raw BMI values, e.g., 6.0-year-old boys and girls with a BMI of at least 19.76 and 19.62 were considered as obese, respectively. The age- and sex-specific cutoff values for waist circumference were based on the top quartile of the reference data from the National Health and Nutrition Examination Survey [29], e.g., 6.0 year old boys and girls with a waist circumference of at least 58.3 and 57.2 cm were in the top quartile of waist circumference, respectively.
Genotyping and quality control
DNA was extracted from saliva or blood samples using established procedures. Genotyping of 3515 children was performed on the UK Biobank Axiom array (Santa Clara, USA) in two batches (2015 and 2017). Following the recommendations of ref. [30], sample and genotype quality control measures were applied (see Supplementary materials for details), resulting in 3099 children and 3424,677 genotypes after imputation. A genetic relatedness matrix was calculated by using the program EMMAX (https://genome.sph.umich.edu/wiki/EMMAX) to account for the degree of relatedness within the study sample and to adjust for population stratification [31, 32] (see “Statistical analyses”).
Polygenic risk score calculation
We calculated PRS based on genome-wide summary statistics for BMI from European ancestry populations. The PRS (called PRS-Khera) was proposed and validated in Khera et al. [21]. It consists of 2,100,302 SNPs and is based on summary statistics from the first large-scale GWAS of BMI (~300,000 samples) [10]. PRS-Khera was calculated in Khera et al. [21] using a computational algorithm called LDPred, which is a Bayesian approach to calculate a posterior mean effect for all variants using external weights with subsequent shrinkage based on linkage disequilibrium [33]. Using LDPred, each variant was reweighted according to the prior GWAS [10], the degree of correlation between a variant and others nearby, and a tuning parameter that denotes the proportion of variants with non-zero effect.
In sensitivity analyses, the performance of PRS-Khera was compared to PRS calculated with PRSice [34] and PRS based on only genome-wide significant SNPs from two discovery samples (same discovery sample as for PRS-Khera (~300,000 samples) [10] and the largest published GWAS study of BMI to date (~700,000 samples) [11]). More details on the different PRS are given in the Supplementary methods and Figs. S1–S3.
Assessment of dietary intake
We used long-term and short-term dietary measurements assessed by food frequency questionnaires (FFQs) and repeated 24-h dietary recalls, respectively [35]. A fruit and vegetable score was calculated from FFQs (for more details on the FFQs and calculation of the fruit and vegetable score, see Supplementary material). We expressed the fruit and vegetable consumption as the relative frequency in relation to all foods reported in the FFQs [36]. Energy and dietary fiber intake was assessed by repeated 24-h dietary recalls in a subset of the IDEFICS/I.Family cohort (see Table 1 for the actual numbers) [37, 38]. Fiber intake was expressed in relation to total energy intake in mg/kcal. See Supplementary material for more details.
Assessment of physical activity
Physical activity was objectively measured by using Actigraph’s uniaxial or three-axial accelerometers [39, 40]. At baseline and FU1, children were asked to wear the accelerometer for 3 days (including 1 weekend day) and at FU2 for a full week during waking hours (except when swimming or showering). The daily average cumulative duration of time spent performing moderate-to-vigorous physical activity (MVPA) was expressed as hours per day according to the cutoff value by Evenson et al. [41]. Time spent in MVPA is based on cleaned accelerometer data that only contain measurements that have passed the minimum wear time criteria of at least 3 measurement days and at least 360 min of valid time per day. The accelerometers were attached to the right hip with an elastic belt. See Supplementary material for more details.
Assessment of screen time
Screen time was assessed by asking how many hours per day the child/adolescent usually spends watching television (including videos or DVDs) and by another question on the time sitting in front of a computer and game console [42, 43]. Responses were weighted and summed across weekdays and weekend days and the quantified frequencies from both questions were added to create a continuous variable of total screen time in hours per day. See Supplementary material for more details.
Assessment of sociodemographic variables
Parental education was retrieved from questionnaires and coded according to the International Standard Classification of Education (ISCED) [44]. For the analyses, the highest parental education of both parents was coded as low (ISCED levels 1 and 2; ≤9 years of education), medium (ISCED levels 3 and 4), and high (ISCED levels 5 and 6; ≥2 years of education after high school). The region of residence was coded as Northern Europe (Estonia, Sweden), Central Europe (Belgium, Germany, and Hungary), and Southern Europe (Italy, Spain).
Statistical analyses
Our data consist of up to three repeated measurements of individuals, some of whom were siblings. We estimated associations between the PRS and obesity outcomes (BMI and waist circumference) as well as interactions between the PRS and demographic and lifestyle factors using generalized linear mixed models where the covariance matrix of the random intercept is proportional to a genetic relatedness matrix. We applied the generalized linear mixed model approach of Chen et al. [31] that jointly controls for relatedness and population stratification. Such a model can be formulated in slightly simplified notation as:
where g() is the link function, E() the expectation, y is the dependent variable, X the covariate matrix, β a vector of the fixed effects, and γ the intercept-only random effect, which is assumed to be normally distributed with expectation 0 and covariance according to the genetic relatedness matrix V.
In addition, we conducted the following analyses for the main effects of the PRS for easier interpretation and comparison with the results from Khera et al. [21]. (1) We used logistic mixed models (logit link) to estimate associations between the PRS and obesity and the top quartile of waist circumference (binary outcomes) and (2) we estimated associations between being in the top decile of the PRS (binary variable) and the obesity outcomes.
All models were adjusted for confounding factors that are assumed to be associated with lifestyle and obesity (sex, age, region of residence, parental education, and dietary intake (fruit and vegetable score as proxy for healthy dietary intake)). Models that investigated the interaction between PRS and fiber intake were not additionally adjusted for the fruit and vegetable score because both variables are used as proxy variables for healthy dietary intake. The response and confounding variables showed only small percentage of missing values while we had more missing values of some exposure variables such as fiber intake and MVPA (Table 1). We compared BMI and waist circumference of children with and without missing values in exposure variables (fiber, fruit and vegetable score, MVPA, screen time) to evaluate if they were missing at random. As we conducted a repeated measurement analysis, we retained all children in the analysis that had at least one observed measurement of each variable and performed listwise deletion of incomplete cases. When testing associations with categorical variables (sex, region of residence, and parental education), we used the category with the largest sample size as reference category.
All p values from the G×E interaction analyses were adjusted according to the number of tested environmental factors using the false-discovery rate (FDR, FDR-adjusted p values are called q values). We reported 95% CI and two-sided p values, and considered p values <0.05 statistically significant. We used R 3.5.1 [45] for all statistical analyses.
Results
Study description
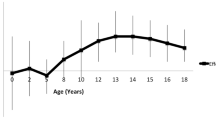
The study sample included 8609 repeated BMI measurements from at maximum three time points (baseline, FU1, FU2) of 3098 children aged 2–16 years (Table 1). The number of participants decreased between the follow-up investigations from n = 3016 at baseline (mean age 6 years) to n = 2656 at FU2 (mean age 12 years). Half of the children were girls, most children came from families with a medium or high level of parental education and the majority lived in Central European countries. The distributions of the dietary variables (fruit and vegetable score and fiber intake) and time spent in MVPA were similar between baseline and the two follow-up samples, whereas children and adolescents spent more time in front of screens at FU1 and FU2 as compared to baseline. For the variables with the most missing values (MVPA, fiber intake, the fruit and vegetable score, and screen time), we observed at least one of three repeated measurements for 90%, 95%, >99%, and >99% of the children, respectively. We found no substantial differences between children with no measurements at any visit and children with at least one observed measurement with BMI, waist circumference, and the PRS score (see Fig. S4).
Variance explained by PRS
We found that the PRS-Khera provided the best prediction of BMI (r2 = 0.11) and the second-best prediction of obesity (AUC = 0.74, see Table S1 for details on the characteristics of the other PRS). PRS-Khera was associated with BMI (r2 = 0.11, p value = 7.9 × 10−81) and waist circumference (r2 = 0.09, 1.8 × 10−71) in our study population (Table 2) and these correlations increased with age (see Tables S2, S3 and Fig. S5). Being in the top decile of the distribution of PRS-Khera was associated with 3.63 times higher odds for obesity (95% CI: [2.57, 5.14]) and with 3.09 (95% CI: [2.37, 4.03]) higher odds for being in the top quartile of waist circumference.
G×E interactions
We found a significant G×E interaction of PRS-Khera with parental education (low vs. high) as well as with the European region of residence (Central vs. Southern) for BMI as well as for waist circumference (Fig. 1 and Table S4). Children and adolescents from families with a low level of parental education were at a higher risk of having obesity among those with higher genetic susceptibility than children from families with a high level of parental education (low: beta estimate from education-stratified analysis for association between PRS-Khera and BMI = 0.48; 95% CI: [0.38, 0.59], high: beta estimate = 0.30; 95% CI: [0.26, 0.34], q value interaction = 0.0106, Fig. 1 and Table S4). Furthermore, children and adolescents from Southern European countries showed an increased genetic susceptibility to a high BMI in comparison to children and adolescents from Central Europe (Central Europeans: beta estimate from region-stratified analysis for association between PRS-Khera and BMI = 0.29; 95% CI: [0.23, 0.34], Southern Europeans: beta estimate = 0.40; 95% CI: [0.34, 0.45], q value interaction = 0.0246, Fig. 1 and Table S4). Interactions were confirmed in our sensitivity analyses using other genome-wide PRS (Fig. S6 and Table S6). We did not find significant interactions between PRS-Khera and sex, the comparison of low vs. medium parental education, nor the comparison of Central vs. Northern European region of residence (Fig. 1 and Table S4).

Associations between PRS and BMI/waist circumference are shown in different strata (beta estimates and 95% CIs) as well as in the whole study population (red line). Raw p values (p) and FDR-adjusted p values (q values, q) are given for the test of deviations of the association between PRS and obesity in one subgroup in comparison to the reference category (interaction). The category without p values is the reference category. The gray boxes show the distribution of the sociodemographic factors.
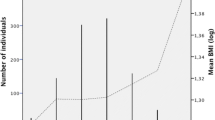
The genetic susceptibility to a high BMI was further modified by intake of dietary fiber and screen time (Fig. 2 and Table S5). Children and adolescents with a higher fiber intake showed an attenuated risk of having obesity despite their genetic susceptibility (BMI: beta estimates and 95% CI for interaction terms: −0.02 [−0.04, −0.01], q values interaction = 0.025; waist circumference: −0.03 [−0.06, −0.01], q values interaction = 0.023). Furthermore, the more time the children and adolescents spent in front of screens, the higher was their risk of having obesity among those with higher genetic susceptibility (significant for BMI: beta estimates and 95% CI for interaction terms: 0.02 [0.00, 0.03], q value interaction = 0.042). Interactions between PRS-Khera and the fruit and vegetable score or MVPA were not significant (beta estimates and 95% CI for interaction terms: −0.01 [−0.21, 0.19] for fruit and vegetable score and −0.01 [−0.07, 0.04] for MVPA). Interaction results with other PRS for obesity were similar, but not significant (Fig. S7 and Table S7).

Associations between PRS and obesity are shown in dependence of the PRS (beta estimates and 95% CIs) as well as in the whole study population (red line). The distributions of the lifestyle factors are shown in histograms. Raw p values (p) and FDR-adjusted p values (q values, q) are given for the interaction terms. The distributions of the lifestyle factors are shown in histograms.
Discussion
In our pan-European cohort of children aged 2–16 years, we found significant interactions between PRS-Khera and sociodemographic as well as lifestyle factors for BMI and waist circumference: we observed G×E interactions with (1) the European region of residence, which most likely reflect cultural lifestyle differences, (2) parental education, (3) dietary fiber intake, and (4) the time children spent in front of screens. Of note, all of these interactions would have remained undetected in this sample of children when only focusing on genome-wide significant variants as was done in previous studies (compare Figs. S6 and S7) [13,14,15,16,17,18,19,20].
Comparison with previous studies
Interactions with socioeconomic status [7, 14], physical activity [8, 9, 13, 14], and dietary factors [14,15,16] have been reported previously. However, previous interaction results were mainly estimated in twin studies, which might not be representative of the general population [46], and cohort studies including only <100 genome-wide significant SNPs, which do not account for the polygenic nature of BMI [21]. Thus, our study confirms previous interaction findings and demonstrates that genome-wide PRSs are a powerful approach to detect interactions and a good alternative to the traditional twin study design. Genome-wide PRSs have the advantage that they can be applied to cohort studies, while explaining a much larger part of the genetic variance of BMI than studies restricted to genome-wide significant variants. In addition, previous G×E interaction studies were mainly based on adult populations whereas in our study we analyzed data from children and adolescents aged 2–16 years, i.e., in the key developmental transition phases of human life.
We identified children from families with low level of parental education as being about 61% more susceptible to the polygenic burden of obesity than children from families with a high level of parental education. In addition, we found that children from Southern Europe had a higher genetic susceptibility to obesity in comparison to children from Central Europe. Parental education and region of residence reflect a variety of social and cultural differences and many of them are difficult to be captured by questionnaires. Since a previous analysis of the same cohort showed that low parental education was associated with higher intakes of unhealthy food among children, e.g., sugar-rich and fatty foods [47, 48], part of the effect modification might be due to dietary habits. The differences in the risk of having obesity among children with a higher genetic susceptibility across different European regions might be explained by differences in dietary or cultural habits [49, 50].
Furthermore, we found an interaction between PRS-Khera and dietary fiber intake, where children with a higher intake of fiber have a reduced risk for obesity despite their genetic susceptibility. This finding is in line with many other studies that have shown that a healthy diet can attenuate the genetic burden of obesity [14,15,16,17,18,19,20].
Interactions between PRS-Khera and physical activity (MVPA) were not significant, but the direction of interaction effect was in line with previous studies [13, 14]. An explanation for this might be that MVPA was only assessed in ~40% of our analysis group (Table 1), which reduced the statistical power to detect interactions between MVPA and PRS.
Strengths and limitations of this study
Important strengths of this study include: detailed and repeated phenotyping of participants in this cohort with partly objective measures (MVPA), inclusion of thousands of children from diverse regions in Europe and the longitudinal approach across key developmental periods [25]. Dietary assessment in children is a challenging task, and different dietary assessment methods have different strengths and limitations. We used two different methods—a fruit and vegetable score derived from FFQs and fiber intake calculated from the more detailed 24-h dietary recalls. The harmonized protocol in all countries that was enforced by a central quality control and a central data management ensures comparability of measurements across study centers. Another major strength of our study is the application of genome-wide PRS for obesity, which has an almost five times higher prediction accuracy than previously used PRS [14,15,16,17,18,19,20] and with which we identified interactions that would have remained undetected when restricting to only genome-wide significant variants (compare Figs. S5 and S6). In addition, although the PRS-Khera was derived for BMI we also assessed its association with waist circumference. The strength of this association was only slightly smaller than the association with BMI. This is plausible, because PRS-Khera is known to be a strong risk factor for severe obesity and associated health outcomes [21].
A limitation of our study is that measurement errors of self-reported lifestyle behaviors are inevitable. However, measurement error in environmental exposure typically biases the interaction effect toward the null [51], which does not increase the risk for false-positive findings but reduces the statistical power to detect modest interactions. In addition, we used a complete-case analysis strategy, which might bias the estimates toward null [52].
Conclusions
Our study showed significant interactions between the polygenic risk for an increased BMI and sociodemographic and lifestyle factors that affect BMI as well as waist circumference. Among children with a high genetic risk, we identified children from Southern Europe, children from families with a low level of parental education, children with a low dietary fiber intake and children who spend more time in front of screens as being particularly susceptible to obesity. These results suggest that the risk for obesity among children with a high genetic susceptibility varies by environmental and sociodemographic factors during childhood. While all children benefit from an environment that supports a healthy lifestyle, our findings suggest that this is particularly important for children with a high genetic risk for obesity. Although it is unlikely that genetic screening for obesity will be implemented in clinical practice anytime soon, our findings emphasize the importance of obesity prevention in early childhood by showing that there are synergistic effects of genetics and sociodemographic and lifestyle factors that could affect a substantial part of the general population. The interactions between parental education, region, and genetic heritability indicate that system-level interventions might be better suited than individual intervention strategies.
References
GBD 2015 Obesity Collaborators, Afshin A, Forouzanfar MH, Reitsma MB, Sur P, Estep K, et al. Health effects of overweight and obesity in 195 countries over 25 years. N Engl J Med. 2017;377:13–27.
Silventoinen K, Jelenkovic A, Sund R, Hur YM, Yokoyama Y, Honda C, et al. Genetic and environmental effects on body mass index from infancy to the onset of adulthood: an individual-based pooled analysis of 45 twin cohorts participating in the COllaborative project of Development of Anthropometrical measures in Twins (CODATwins). Am J Clin Nutr. 2016;104:371–9.
Min J, Chiu DT, Wang Y. Variation in the heritability of body mass index based on diverse twin studies: a systematic review. Obes Rev. 2013;14:871–82.
Rokholm B, Silventoinen K, Tynelius P, Gamborg M, Sørensen TIA, Rasmussen F. Increasing genetic variance of body mass index during the Swedish obesity epidemic. PLoS ONE. 2011;6:e27135.
Dinescu D, Horn EE, Duncan G, Turkheimer E. Socioeconomic modifiers of genetic and environmental influences on body mass index in adult twins. Heal Psychol. 2016;35:157–66.
Schrempft S, Van Jaarsveld CHM, Fisher A, Herle M, Smith AD, Fildes A, et al. Variation in the heritability of child body mass index by obesogenic home environment. JAMA Pediatr. 2018;172:1153–60.
Silventoinen K, Jelenkovic A, Latvala A, Yokoyama Y, Sund R, Sugawara M, et al. Parental education and genetics of BMI from infancy to old age: a pooled analysis of 29 twin cohorts. Obesity. 2019;27:855–65.
Karnehed N, Tynelius P, Heitmann BL, Rasmussen F. Physical activity, diet and gene-environment interactions in relation to body mass index and waist circumference: the Swedish Young Male Twins Study. Public Health Nutr. 2006;9:851–8.
Mustelin L, Silventoinen K, Pietiläinen K, Rissanen A, Kaprio J. Physical activity reduces the influence of genetic effects on BMI and waist circumference: a study in young adult twins. Int J Obes. 2009;33:29–36.
Locke AE, Kahali B, Berndt SI, Justice AE, Pers TH, Day FR, et al. Genetic studies of body mass index yield new insights for obesity biology. Nature. 2015;518:197–206.
Yengo L, Sidorenko J, Kemper KE, Zheng Z, Wood AR, Weedon MN, et al. Meta-analysis of genome-wide association studies for height and body mass index in ~700 000 individuals of European ancestry. Hum Mol Genet. 2018;27:3641–9.
Tam V, Patel N, Turcotte M, Bossé Y, Paré G, Meyre D. Benefits and limitations of genome-wide association studies. Nat Rev Genet. 2019;20:467–84.
Li S, Zhao JH, Luan J, Ekelund U, Luben RN, Khaw KT, et al. Physical activity attenuates the genetic predisposition to obesity in 20,000 men and women from EPIC-Norfolk prospective population study. PLoS Med. 2010;7:1–9.
Rask-Andersen M, Karlsson T, Ek WE, Johansson Å. Gene-environment interaction study for BMI reveals interactions between genetic factors and physical activity, alcohol consumption and socioeconomic status. PLoS Genet. 2017;13:1–20.
Wang T, Heianza Y, Sun D, Huang T, Ma W, Rimm EB, et al. Improving adherence to healthy dietary patterns, genetic risk, and long term weight gain: gene-diet interaction analysis in two prospective cohort studies. BMJ. 2018;360:1–9.
Wang T, Heianza Y, Sun D, Zheng Y, Huang T, Ma W, et al. Improving fruit and vegetable intake attenuates the genetic association with long-term weight gain. Am J Clin Nutr. 2019;110:759–68.
Qi Q, Chu AY, Kang JH, Huang J, Rose LM, Jensen MK, et al. Fried food consumption, genetic risk, and body mass index: gene-diet interaction analysis in three US cohort studies. BMJ. 2014;348:g1610.
Ding M, Ellervik C, Huang T, Jensen MK, Curhan GC, Pasquale LR, et al. Diet quality and genetic association with body mass index: Results from 3 observational studies. Am J Clin Nutr. 2018;108:1291–300.
Casas-Agustench P, Arnett DK, Smith CE, Lai C-Q, Parnell LD, Borecki IB, et al. Saturated fat intake modulates the association between a genetic risk score of obesity and BMI in two US populations Patricia. J Acad Nutr Diet. 2013;18:1199–216.
Wang T, Huang T, Kang JH, Zheng Y, Jensen MK, Wiggs JL, et al. Habitual coffee consumption and genetic predisposition to obesity: Gene-diet interaction analyses in three US prospective studies. BMC Med. 2017;15:1–9.
Khera AV, Chaffin M, Wade KH, Zahid S, Brancale J, Xia R, et al. Polygenic prediction of weight and obesity trajectories from birth to adulthood. Cell. 2019;177:587–596.e9.
Silventoinen K, Jelenkovic A, Sund R, Yokoyama Y, Hur YM, Cozen W, et al. Differences in genetic and environmental variation in adult BMI by sex, age, time period, and region: an individual-based pooled analysis of 40 twin cohorts. Am J Clin Nutr. 2017;106:457–66.
Ordoñana JR, Rebollo-Mesa I, González-Javier F, Pérez-Riquelme F, Martínez-Selva JM, Willemsen G, et al. Heritability of body mass index: a comparison between the Netherlands and Spain. Twin Res Hum Genet. 2007;10:749–56.
Ahrens W, Bammann K, Siani A, Buchecker K, De Henauw S, Iacoviello L, et al. The IDEFICS cohort: design, characteristics and participation in the baseline survey. Int J Obes. 2011;35:3–15.
Ahrens W, Siani A, Adan R, De Henauw S, Eiben G, Gwozdz W, et al. Cohort profile: the transition from childhood to adolescence in European children-how I.Family extends the IDEFICS cohort. Int J Epidemiol. 2017;46:1394–5.
Ahrens W, Pigeot I, Pohlabeln H, De Henauw S, Lissner L, Molnár D, et al. Prevalence of overweight and obesity in European children below the age of 10. Int J Obes. 2014;38:S99–S107.
Cole TJ, Lobstein T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr Obes. 2012;7:284–94.
McCarthy H, Jarrett K, Crawley H. The development of waist circumference percentiles in British. Eur J Clin Nutr. 2001;55:902–7.
McDowell MA, Fryar CD, Hirsch R, Ogden CL. Anthropometric reference data for children and adults: U.S. population, 1999–2002. Adv Data. 2005;361:1–5.
Weale ME. Quality control for genome-wide association studies. Methods Mol Biol. 2010;628:341–72.
Chen H, Wang C, Conomos MP, Stilp AM, Li Z, Sofer T, et al. Control for population structure and relatedness for binary traits in genetic association studies via logistic mixed models. Am J Hum Genet. 2016;98:653–66.
Wang K, Hu X, Peng Y. An analytical comparison of the principal component method and the mixed effects model for association studies in the presence of cryptic relatedness and population stratification. Hum Hered. 2013;76:1–9.
Vilhjálmsson BJ, Yang J, Finucane HK, Gusev A, Lindström S, Ripke S, et al. Modeling linkage disequilibrium increases accuracy of polygenic risk scores. Am J Hum Genet. 2015;97:576–92.
Euesden J, Lewis CM, O’Reilly PF. PRSice: Polygenic Risk Score software. Bioinformatics. 2015;31:1466–8.
Illner AK, Freisling H, Boeing H, Huybrechts I, Crispim SP, Slimani N. Review and evaluation of innovative technologies for measuring diet in nutritional epidemiology. Int J Epidemiol. 2012;41:1187–203.
Arvidsson L, Bogl LH, Eiben G, Hebestreit A, Nagy P, Tornaritis M, et al. Fat, sugar and water intakes among families from the IDEFICS intervention and control groups: first observations from I.Family. Obes Rev. 2015;16:127–37.
Intemann T, Pigeot I, De Henauw S, Eiben G, Lissner L, Krogh V, et al. Urinary sucrose and fructose to validate self-reported sugar intake in children and adolescents: results from the I.Family study. Eur J Nutr. 2019;58:1247–58.
Bogl LH, Silventoinen K, Hebestreit A, Intemann T, Williams G, Michels N, et al. Familial resemblance in dietary intakes of children, adolescents, and parents: does dietary quality play a role? Nutrients. 2017;9. https://doi.org/10.3390/nu9080892.
Konstabel K, Chopra S, Ojiambo R, Muñiz-Pardos B, Pitsiladis Y. Accelerometry-Based Physical Activity Assessment for Children and Adolescents. In: Bammann K, Lissner L, Pigeot I, Ahrens W. (eds) Instruments for Health Surveys in Children and Adolescents. Springer Series on Epidemiology and Public Health. Springer, Cham. (2019) https://doi.org/10.1007/978-3-319-98857-3_7.
Konstabel K, Veidebaum T, Verbestel V, Moreno LA, Bammann K, Tornaritis M, et al. Objectively measured physical activity in European children: the IDEFICS study. Int J Obes. 2014;38:135–43.
Evenson KR, Catellier DJ, Gill K, Ondrak KS, McMurray RG. Calibration of two objective measures of physical activity for children. J Sports Sci. 2008;26:1557–65.
Olafsdottir S, Berg C, Eiben G, Lanfer A, Reisch L, Ahrens W, et al. Young children’s screen activities, sweet drink consumption and anthropometry: results from a prospective European study. Eur J Clin Nutr. 2014;68:223–8.
Bogl LH, Mehlig K, Intemann T, Masip G, Keski-Rahkonen A, Russo P, et al. A within-sibling pair analysis of lifestyle behaviours and BMI z-score in the multi-centre I.Family study. Nutr Metab Cardiovasc Dis. 2019;29:580–9.
UNESCO. International Standard Classification of education ISCED 2011. Montreal, QC: UNESCO; 2012.
R Core Team. R: a language and environment for statistical computing. 2018. https://www.r-project.org/.
Sahu M, Prasuna JG. Twin studies: a unique epidemiological tool. Indian J Community Med. 2016;41:177–82.
Fernandez-Alvira JM, Mouratidou T, Bammann K, Ferna JM, Hebestreit A, Barba G, et al. Parental education and frequency of food consumption in European children: the IDEFICS study. Public Health Nutr. 2012;16:487–98.
Fernández-Alvira JM, Bammann K, Pala V, Krogh V, Barba G, Eiben G, et al. Country-specific dietary patterns and associations with socioeconomic status in European children: the IDEFICS study. Eur J Clin Nutr. 2014;68:811–21.
Tognon G, Hebestreit A, Lanfer A, Moreno LA, Pala V, Siani A, et al. Mediterranean diet, overweight and body composition in children from eight European countries: cross-sectional and prospective results from the IDEFICS study. Nutr Metab Cardiovasc Dis. 2014;24:205–13.
Lissner L, Lanfer A, Gwozdz W, Olafsdottir S, Eiben G, Moreno LA, et al. Television habits in relation to overweight, diet and taste preferences in European children: the IDEFICS study. Eur J Epidemiol. 2012;27:705–15.
Paeratakul S, Popkin BM, Kohlmeier L, Hertz-Picciotto I, Guo X, Edwards LJ. Measurement error in dietary data: implications for the epidemiologic study of the diet-disease relationship. Eur J Clin Nutr. 1998;52:722–7.
White IR, Carlin JB. Bias and efficiency of multiple imputation compared with complete-case analysis for missing covariate values. Stat Med. 2010;29:2920–31.
Acknowledgements
This research was done on behalf of the IDEFICS/I.Family consortia. The authors wish to thank the children and their parents for participating in this extensive examination. We are grateful for the support of school boards, head teachers, and communities, and for the effort of the study nurses, interviewers, laboratory technicians, and data managers, especially Claudia Brünings-Kuppe. We thank the anonymous reviewers whose comments and suggestions helped to improve and clarify this manuscript.
Funding
The IDEFICS study was financially supported by the European Commission within the Sixth RTD Framework Programme Contract No. 016181 (FOOD); the I.Family study was funded by the European Commission within the Seventh RTD Framework Programme Contract No. 266044 (KBBE 2010-14). Participating partners have contributed their own resources to the genotyping of children. AH was supported by a research fellowship from the Deutsche Forschungsgemeinschaft (DFG; HU 2731/1-1) and by the HERCULES Center (NIEHS P30ES019776). Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hüls, A., Wright, M.N., Bogl, L.H. et al. Polygenic risk for obesity and its interaction with lifestyle and sociodemographic factors in European children and adolescents. Int J Obes 45, 1321–1330 (2021). https://doi.org/10.1038/s41366-021-00795-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41366-021-00795-5
- Springer Nature Limited
This article is cited by
-
A genomics perspective of personalized prevention and management of obesity
Human Genomics (2024)
-
Variability of polygenic prediction for body mass index in Africa
Genome Medicine (2024)
-
Future implications of polygenic risk scores for life insurance underwriting
npj Genomic Medicine (2024)
-
Associations between polygenic risk scores for cardiometabolic phenotypes and adolescent depression and body dissatisfaction
Pediatric Research (2024)
-
Socio-economic differences in body mass index: the contribution of genetic factors
International Journal of Obesity (2024)