
Abstract
Several trials have shown preliminary evidence for the efficacy of transcranial magnetic stimulation (TMS) as a treatment for negative symptoms in schizophrenia. Here, we synthesize this literature in a systematic review and quantitative meta-analysis of double-blind randomized controlled trials of TMS in patients with schizophrenia. Specifically, MEDLINE, EMBASE, Web of Science, and PsycINFO were searched for sham-controlled, randomized trials of TMS among patients with schizophrenia. The effect of TMS vs. sham on negative symptoms in each study was quantified by the standardized mean difference (SMD, Cohen’s d) with 95% confidence intervals (95%CI) and pooled across studies using an inverse variance random effects model. We identified 57 studies with a total of 2633 participants that were included in the meta-analysis. The pooled analysis showed statistically significant superiority of TMS (SMD = 0.41, 95%CI: 0.26; 0.56, p-value < 0.001), corresponding to a number needed to treat of 5. Furthermore, stratified analyses suggested that TMS targeting the left dorsolateral prefrontal cortex and using a stimulation frequency >1 Hz was most efficacious. There was, however, substantial heterogeneity and high risk of bias among the included studies. In conclusion, TMS appears to be an efficacious treatment option for patients with schizophrenia suffering from negative symptoms, but the optimal TMS parameters are yet to be established.
Similar content being viewed by others


Introduction
Pharmacological treatment is the cornerstone of care in schizophrenia and other psychotic disorders1. Though positive symptoms (e.g., delusions and hallucinations) respond relatively well to pharmacological treatment, negative symptoms often do not respond to the same degree2,3,4. The negative symptoms of schizophrenia are those representing absence/lessening of normal functions and include affective flattening, alogia, apathy and social withdrawal5. Patients with predominantly negative symptoms are more resistant to treatment than patients with primarily positive symptoms, and negative symptoms are strongly associated with low daily functioning and poor long-term prognosis6,7,8. Therefore, identification and development of efficacious treatments of negative symptoms is a priority3,9.
Transcranial magnetic stimulation (TMS) is a non-invasive neuromodulation technique in which a localized electrical field is elicited in underlying brain parenchyma through electromagnetic induction, generally limited to superficial cortical regions10,11. Whether TMS increases or decreases the activity of the targeted neurons depends on the frequency of the magnetic pulses with 1 Hz and below (low frequency) being inhibitory and >1 Hz being excitatory (high frequency)12. Repetitive TMS (rTMS) is the most widely used modality with a single session lasting 20–40 min, typically delivering between 1200-3000 magnetic pulses13. Other types include deep TMS in which the magnetic field reaches deeper subcortical regions of the brain as well as theta burst stimulation (TBS) in which the frequency of stimulation is 50 Hz administered five times per second to mimic endogenous theta waves either continuously or intermittently14.
TMS is approved for the treatment of major depression (https://www.accessdata.fda.gov/cdrh_docs/pdf6/K061053.pdf) and since the negative symptoms of schizophrenia and the symptoms of major depression both represent deficits of normal functions, TMS has also been explored as a potential treatment of negative symptoms among patients with schizophrenia15,16,17,18. Since the most recent reviews of the literature on TMS for treatment of negative symptoms15,16,17,18, several trials have been conducted—some using novel stimulation parameters as well as neuronavigation to improve targeting19,20,21,22,23,24,25,26,27. Due to these developments in the field, an updated synthesis would be of relevance. Therefore, we conducted a systematic review and quantitative meta-analysis of randomized controlled trials reporting on the efficacy of rTMS in the treatment of negative symptoms among patients with schizophrenia.
Methods
Protocol and registration
The study protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO, ID: CRD42021238828) (https://www.crd.york.ac.uk/PROSPERO) and carried out in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines28.
Information sources and screening
MEDLINE (PubMed), PsycINFO, Web of Science and EMBASE were searched for relevant studies. Earlier reviews on the subject, clinicaltrials.gov, as well as citations of included studies were reviewed in order to find further eligible studies. The search was carried out on May 1st 2021 using the following search string in MEDLINE: (“schizophreni*” OR “schizoaffective disorder” OR “schizophreniform disorder” OR “schizophrenia”[MeSH Terms] OR “negative symptom*” OR “CHR” OR “Clinical High Risk” OR “Ultra High Risk” OR “UHR” OR “Psychotic Disorders”[MeSH Terms] OR “Psychotic Disorder*“) AND (“transcranial magnetic stimulation” OR “TMS” OR “rTMS” OR “theta burst” OR “iTBS” OR “cTBS” OR Transcranial Magnetic Stimulation*[MeSH Terms]). The analogue search strings used for the other databases are available in the Supplementary Material. Titles and abstracts of studies identified via the search strategy described above were screened independently by two authors (RL and TDN) assisted by Covidence29. Full text versions of the studies deemed relevant after initial screening were subsequently assessed for eligibility.
Eligibility criteria
In line with earlier reviews in the field, the following inclusion criteria were employed15,17,18. Notably, no language restrictions were employed:
-
Randomized, sham-controlled trials of transcranial magnetic stimulation (e.g., rTMS or theta burst stimulation)
-
Participants with a primary diagnosis of schizophrenia, schizoaffective disorder or another psychotic disorder (e.g., acute/transient/brief psychotic disorder or persistent delusional disorder), according to the DSM-IV, DSM-5, or ICD-10.
-
Adult participants (≥18 years)
-
Outcome measured using an established psychometric scale for negative symptoms in schizophrenia (e.g., the negative subscale of the Positive and Negative Syndromes Scale (PANSS-N)30 or the Scale for Assessment of Negative Symptoms (SANS)31).
The following exclusion criterion was employed:
-
Co-initiation of other treatments, e.g., pharmacological treatment, as the results of such studies could be affected by an interaction effect between TMS and the co-initiated treatment.
Data extraction
The following items were extracted from each included study: Author name, publication year, country, study type (cross-over or parallel), analysis-type (per protocol or intention-to-treat (ITT)), number of participants, drop-out rates, mean age of participants, sex distribution of participants, diagnostic distribution, whether samples were selected for predominantly negative symptoms, frequency and intensity of TMS including the total number of stimuli and number of treatments, TMS target, nature of the sham intervention, outcome measure (rating scale), post treatment scores, follow-up scores and post treatment depression scores (if available). If these data were not reported, the authors were contacted by e-mail with a request to provide the data. If authors did not reply, data from graphs (if available) were extracted using the GetData Graph Digitizer (http://getdata-graph-digitizer.com/). Previous meta-analyses were screened for post-treatment outcome data required to compute effect sizes. Studies where data was not available upon request, via graphs or through previous meta-analyses, were excluded from the analyses.
Evaluation of risk of bias
The included studies were evaluated according to five domains of bias (articles in non-English languages were not evaluated) using the Cochrane Risk of Bias Tool 2.0:(https://methods.cochrane.org/risk-bias-2) (A) Randomization process (allocation sequence generation and concealment), (B) Deviations from intended interventions (bias arising from non-protocol interventions), (C) Missing outcome data (dropouts), (D) Measurement of the outcome (using a validated tool), and (E) Selection of the reported result (alignment with protocol and method section). In accordance with the instructions for the Cochrane Risk of Bias Tool 2.0, the highest risk score assigned in one of these domains defined the overall risk of bias score for each study (https://methods.cochrane.org/risk-bias-2). Furthermore, potential publication bias was explored via a funnel plot and Egger’s regression test.
Statistical analysis
The effect of TMS vs. sham on negative symptoms in each included study was quantified by the standardized mean difference (SMD, Cohen’s d) with 95% confidence intervals (95%CI) based on endpoint scores or change scores (with endpoint scores being preferred). If multiple outcome measures were used, PANSS-N was preferred to improve methodological homogeneity because it was used in 89% (51/57) of the included studies. If a study did not provide standard deviations (SD) or data that could be used to calculate SD (e.g., standard error), the mean standard deviation across all studies of the same outcome measure was used. For cross-over studies, data was extracted after the first treatment phase (before cross-over) to exclude possible carry-over effects of treatment and thus regarded as a parallel design study.
SMDs were pooled using the inverse variance random effects model in Review Manager 5.332. This model takes into account both in-study and between-study variability. For the primary analysis, number needed to treat (NNT) was estimated using the method proposed by Kraemer and Kupfer33. Heterogeneity was assessed using the I²-test with I²-values ≥50% suggesting considerable heterogeneity. For multi-arm studies, data from different active TMS treatment arms were pooled in the calculation of overall efficacy as to not duplicate data from the sham group, using the formulas provided in table 6.5a in the Cochrane Handbook (https://training.cochrane.org/handbook/current/chapter-06#section-6-5-2-10).
Following the main analysis, the following secondary/subgroup analyses (yielding effect sizes) were carried out: (i) focusing on long term effect using data from at least four weeks after the last treatment (the last follow up in each study was used), (ii) focusing on patients with predominantly negative symptoms, (iii) focusing on the effect size of TMS for depressive symptoms (all depression measures allowed with a preference for the Calgary Depression Scale in Schizophrenia34), (iv) after stratifying by target site (v) after stratifying by type of TMS, (vi) after stratifying by stimulation frequency, (vii) after stratifying by stimulation intensity, and (viii) after stratifying by age. Finally, the following sensitivity analyses (yielding effect sizes) were conducted: (I) after excluding studies with data extracted from graphs, (II) after excluding studies with high risk of bias, (III) after excluding studies reporting change-from-baseline scores, (IV) after excluding studies with data extracted from other reviews, and (V) after stepwise exclusion of the 10 most outlying studies compared to the overall efficacy estimate.
Results
Study selection
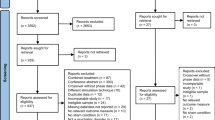
The search yielded 3287 articles of which 1573 were duplicates, resulting in 1714 studies that underwent title- and abstract screening (Fig. 1). Following this screening, 1565 were excluded. This left 149 articles to be assessed in full text, of which 80 studies did not meet the eligibility criteria. The most common reason for exclusion in this final step was “not randomized sham-controlled trials” (31 studies), which included non-blinded studies, studies with no sham-treated group and studies, which were not clinical trials. The second most common reason for exclusion was “did not include eligible outcome measure” (14 studies), which included studies that did not measure negative symptoms, but had other primary endpoints such as biomarkers/neuroimaging or cognitive function. Of the 69 eligible studies, 35 reported insufficient data and thus the authors were contacted by e-mail requesting additional data. The means and standard deviations of PANSS-N was the most common missing piece of information (i.e., from studies where only the total PANSS scores were reported). From these 35 studies, three author groups provided data21,26,35, and data were extracted from graphs in an additional eight studies27,36,37,38,39,40,41,42. Hence, 24 articles were excluded due to non-available data43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66. In total, the search yielded 45 includable studies, with 51 comparisons as a result of studies including multiple interventions19,20,21,22,23,24,25,26,27,35,36,37,38,39,40,41,42,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94. No additional studies were found in citations or in the database of clinicaltrials.gov. Summary data was available from 15 studies reviewed by Wang and colleagues18 from non-English reports90,91,92,95,96,97,98,99,100,101,102,103,104,105,106, of which 3 were also identified by the database search, leaving a total of 57 studies and 63 comparisons19,20,21,22,23,24,25,26,27,35,36,37,38,39,40,41,42,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106.

*Authors were contacted by e-mail. If data was not provided and data could not be taken from graphs, the study was excluded.
Study characteristics
Table 1 shows the characteristics of the 57 included studies.
The 57 studies included 2633 participants, of whom 1481 received active treatment and 1152 sham treatment. In the 55 studies (n = 2525) that reported the specific diagnoses of the participants, 98.9% had schizophrenia and 1.1% had schizoaffective disorder. The two remaining studies reported that the participants had either schizophrenia or schizoaffective disorder, without providing the distribution between the two. The studies were conducted in 15 different countries, of which China was the most common (n = 25). Almost all included studies reported the outcome using PANSS-N or SANS with only one study using the Brief Psychiatric Rating Scale – Negative/Disorganized factor (BPRS-N/D)69.
Several different active TMS modalities were used in the included trials, with some testing more than one active modality against sham treatment: rTMS (48 studies, 10 used ≤1 Hz, 39 used >1 Hz, 42 used unilateral treatment, and eight bilateral or midline treatment), theta burst stimulation (TBS) (9 studies, 5 used intermittent TBS (iTBS), 1 used continuous TBS (cTBS), and 3 used unspecified TBS), and deep-TMS (2 studies). The mean total number of TMS pulses per trial was 25,684 varying from 1200 to 80,000 with an average of 1455 pulses per treatment. The majority of the studies (n = 39) had the left dorsolateral prefrontal cortex (L-DLPFC) as the primary stimulation target.
Risk of bias of individual studies
Eight studies were regarded as having low risk of bias, 10 studies with “some concerns”, and 23 studies with high risk of bias (Supplementary Table 1). The most common reason for “some concerns” was insufficient reporting whether the randomization sequence was concealed adequately (domain A). Improper analysis (e.g. “per protocol” analysis, domain B) and missing outcome data (domain C) were the most common reasons (n = 12 and n = 21, respectively, with n = 11 having both) for a study being regarded as having high risk of bias.
Results of individual studies
Standardized mean differences for the included studies are shown in Fig. 2. Eighteen studies showed a statistically significant superior effect of TMS compared to sham treatment21,22,38,78,79,81,82,88,89,90,95,96,100,101,102,103,105,106 and one study found a statistically significant superior effect of sham treatment36. The remaining studies did not show a statistically significant difference between the treatment groups. There was considerable heterogeneity between the included studies (I2 = 67%).

Forest plot of standardized mean differences (effect size) of TMS on negative symptoms.
Synthesis of results
As evident from the forest plot in Fig. 2, the overall SMD was 0.41 (95%CI: 0.26; 0.56, p < 0.001) in favour of TMS, corresponding to a NNT of 5. The results of the subgroup analyses are available in Table 2A and the results of sensitivity analyses I–IV in Table 2B. Using follow-up data from at least four weeks after end of treatment (see Supplementary Table 2 for further details) yielded an SMD of 0.27 (95%CI: 0.05; 0.49). The effect in participants with predominantly negative symptoms was substantial (SMD = 0.50, 95%CI: 0.25; 0.74), while no effect on depressive symptoms was observed (SMD = 0.02, 95%CI: −0.17; 0.20) (see Supplementary Table 3). Stimulation of the L-DLPFC had a statistically significant (p = 0.0002) larger effect than other sites (SMD = 0.55, 95%CI: 0.38; 0.72 vs. SMD = 0.04, 95%CI: −0.18; 0.25), however, there was considerable methodological heterogeneity in the “other sites” category. The SMD of different types of TMS did not statistically significantly differ (p = 0.28) (SMD = 0.49, 95%CI: 0.03; 0.95 for TBS, SMD = 0.43, 95%CI: 0.27; 0.59 for rTMS and SMD = −0.32, 95%CI: −1.24; 0.61 for deep-TMS). For forest plots of these subgroup analyses, see Supplementary Figs. 1–5. The sensitivity analyses following exclusion of (I) studies with data taken from graphs (SMD = 0.43, 95%CI: 0.27; 0.59), (II) studies with a high risk of bias (SMD = 0.42, 95%CI: 0.14; 0.73), (III) studies using change-from-baseline scores (SMD = 0.43, 95%CI: 0.28; 0.57), or (IV) studies with data extracted from other reviews (SMD = 0.32, 95%CI: 0.15; 0.49), did not impact the effect estimate substantially. A separate forest plot of the standardized mean differences (effect sizes) of the TMS studies targeting the left dorsolateral prefrontal cortex (L-DLPFC) at >1 Hz is shown in Fig. 3.

Forest plot of standardized mean differences (effect sizes) of TMS targeting negative symptoms via stimulation of the left dorsolateral prefrontal cortex (L-DLPFC) at > 1 Hz.
Risk of bias across studies
Based on the funnel plot examining study precision versus effect size (Fig. 4), we saw no qualitative evidence of asymmetry and this was confirmed with Egger’s regression (p = 0.9498). There were, however, outlying studies on both sides of the confidence interval. Notably in this regard, the sensitivity analysis (no. V) involving stepwise exclusion of the 10 most outlying studies yielded no substantial change in the efficacy estimate (see Supplementary Table 4).

SE Standard error, SMD Standardized mean difference.
Discussion
Based on meta-analysis of 57 studies with a total of 2633 participants with schizophrenia (the vast majority) or schizoaffective disorder, we found a superior effect of active TMS on negative symptoms compared to sham treatment. The SMD was 0.41 (95%CI: 0.26; 0.56) in favour of active TMS, translating to a NNT of 5. This result aligns with those from prior meta-analyses on the subject, as Aleman et al.15 found an SMD of 0.64 (95%CI: 0.32; 0.96), He et al.16 an SMD of 0.41 (95%CI: −0.35; 1.16), Wang et al.18 an SMD of 0.40 (95%CI: 0.18; 0.62), and Osoegawa et al.17 an SMD of 0.19 (95%CI: 0.07; 0.32). The superiority of active TMS on negative symptoms remained statistically significant in sensitivity analyses following (a) exclusion of data extracted from graphs, (b) exclusion of studies deemed to be at high risk of bias, and (c) exclusion of studies reporting change-from-baseline scores, respectively. Subgroup analyses suggested that using >1 Hz stimulation (SMD = 0.51 vs. SMD = 0.05, p = 0.003) and targeting the L-DLPFC (SMD = 0.55 vs. SMD = 0.04, p = 0.0002) may be more effective. However, there was considerable heterogeneity across the included studies and these results should therefore be considered tentative. In contrast to the meta-analysis by Aleman et al.15, we found no support for the suggestion that TMS should have a particularly beneficial effect upon negative symptoms among younger patients (SMD = 0.34 vs. SMD = 0.46, p = 0.43). The meta-analysis by Aleman et al. was, however, based on data from a much smaller number of studies/participating patients compared to the present work. Indeed, while there are prior meta-analysis on the effect of TMS on negative symptoms, our updated version covers substantially more studies and participants (138% more studies and 219% more participants than Aleman et al.15, 714% more studies and 539% more participants than He et al.16, 97% more studies and 83% more participants than Wang et al.18, and 138% more studies and 142% more participants than Osoegawa et al.17) and should therefore be more representative of the state-of-the-art.
Several different brain areas were targeted by TMS in the studies included in this synthesis, in which subgroup analyses suggested that stimulation of the L-DLPFC may be particularly beneficial (SMD = 0.55). These results align with earlier studies that have found an inverse correlation between frontal lobe size and glucose metabolism, and negative symptom severity107,108. Together with small sample size, this variability in target could in part explain why only eighteen studies found statistically significant effects of TMS since 17 of these targeted L-DLPFC. Hence, increased activity in the L-DLPFC due to magnetic stimulation could be the mechanism of action underlying the effect on negative symptoms of TMS as proposed in several of the largest included studies25,87,88. Moreover, there is an increasing body of data suggesting that the DLPFC has a privileged relationship with other structures implicated in negative symptoms, including the midline cerebellum109. For these reasons, circuitries involving the DLPFC will likely receive substantial attention in future efforts to relieve negative symptoms of schizophrenia and related psychotic disorders. Conversely, TMS of “other targets” than the L-DLPFC yielded no positive effect compared to sham treatment (SMD = 0.06). While there is considerable methodological heterogeneity among these studies, the quantitative synthesis converged on a null effect with low statistical heterogeneity. Furthermore, several of the studies targeting other sites than the L-DLPFC had other primary endpoints such as the severity of auditory hallucinations (the temporo-parietal cortex as target) with negative symptom severity as a secondary outcome36,40,67,71,77,84, which likely contributes to the lack of effect compared to sham treatment.
There are limitations to this study, which should be acknowledged by the readers. First, as there are phenomenological overlaps between negative and depressive symptoms and since depression responds well to TMS110,111, the relief of depressive symptoms during treatment could potentially confound the estimation of the effect on negative symptoms. However, the results from our analysis of data from studies measuring depressive symptoms in the context of schizophrenia (no effect of TMS) do not support this explanation. Second, 56% of the evaluated studies were regarded as having “high risk of bias”, which is a substantially larger proportion compared to the 13% reported in the review by Wang et al.18. This difference, however, is predominantly a consequence of classification as we used the Cochrane Risk of Bias Tool 2.0, while Wang et al. used the Cochrane Risk of Bias Tool 1.0. The most common reason for studies being considered as “high risk” in the context of the present review was missing data. We employed a relatively conservative 10% cut-off for missing data, but there is no agreed upon threshold (https://training.cochrane.org/handbook/current/chapter-08#section-8-5) and the proportion of studies classified as “high risk of bias” can thus vary considerably between reviews. Also, publication bias seems unlikely as Egger’s regression test showed non-significant results (p = 0.9498), but cannot be ruled out. The two most outlying studies88,103 did not differ substantially in their treatment parameters as both targeted the L-DLPFC with >1 Hz over 20 days of treatment, however, the stimulation intensity (percent of MT) was not described for Zhang 2015. Third, we used a broad search strategy, but relevant studies may have been missed nevertheless. However, assuming that such potential misses occur at random, it should not have affected the reported efficacy estimates. Fourth, the inclusion of data drawn from reviews and graphs is suboptimal. However, the analyses excluding these data yielded results equivalent to those from the primary analysis. Fifth, there was significant heterogeneity in outcome across the included studies, with I2-assessments at 50% or above in all but seven cases (66% in the primary analysis; Fig. 2). While this is likely partly due to the considerable heterogeneity of the TMS treatment provided across the included studies, other sources of heterogeneity, such as differences in sham conditions, patient populations, outcome measures, or random chance, are also likely contributors. Relatedly, in the review by He et al.16, a univariate meta-regression of stimulation frequency, total simulation, motor threshold, stimulation site, study design, and type of coil was conducted. None of these factors were shown to be the main source of heterogeneity. Seventh, 24 studies could not be included due to unavailable data. These studies were, however, generally smaller, which reduces the impact of this limitation.
In conclusion, this systematic review and meta-analysis of data from sham-controlled studies suggests that TMS is efficacious in the treatment of negative symptoms of schizophrenia. Although it appears that targeting the L-DLPFC and using a stimulation frequency >1 Hz are the most efficacious settings, the optimal treatment parameters are yet to be established.
Data availability
All data are available in the manuscript, figures, tables, and supplementary files.
References
The American Psychiatric Association Practice Guideline for the Treatment ofPatients With Schizophrenia. Am. J. Psychiatry. 177, 868–872 (2020).
Fusar-Poli, P. et al. Treatments of negative symptoms in schizophrenia: meta-analysis of 168 randomized placebo-controlled trials. Schizophr. Bull. 41, 892–899 (2015).
Buchanan, R. W. et al. The 2009 schizophrenia PORT psychopharmacological treatment recommendations and summary statements. Schizophr. Bull. 36, 71–93 (2010).
Hieronymus, F. et al. Antipsychotic-placebo separation on the PANSS-6 subscale as compared to the PANSS-30: a pooled participant-level analysis. NPJ Schizophr. 7, 41 (2021).
Strauss, G. P. et al. Deconstructing negative symptoms of schizophrenia: avolition-apathy and diminished expression clusters predict clinical presentation and functional outcome. J. Psychiatr. Res. 47, 783–790 (2013).
Strauss, G. P. et al. Periods of recovery in deficit syndrome schizophrenia: a 20-year multi-follow-up longitudinal study. Schizophr. Bull. 36, 788–799 (2010).
Fenton, W. S. & McGlashan, T. H. Antecedents, symptom progression, and long-term outcome of the deficit syndrome in schizophrenia. Am. J. Psychiatry 151, 351–356 (1994).
Leucht, S. et al. Sixty years of placebo-controlled antipsychotic drug trials in acute schizophrenia: systematic review, bayesian meta-analysis, and meta-regression of efficacy predictors. Am. J. Psychiatry 174, 927–942 (2017).
Kirkpatrick, B. et al. Assessing the efficacy of treatments for the deficit syndrome of schizophrenia. Neuropsychopharmacology 22, 303–310 (2000).
George, M. S. et al. Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: a sham-controlled randomized trial. Arch. Gen. Psychiatry 67, 507–516 (2010).
Allan, C. et al. Transcranial stimulation in depression. Br. J. Psychiatry 200, 10–11 (2012).
Wassermann, E. M. Risk and safety of repetitive transcranial magnetic stimulation: report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation, June 5-7, 1996. Electroencephalogr. Clin. Neurophysiol. 108, 1–16 (1998).
Lisanby, S. H. Update on magnetic seizure therapy: a novel form of convulsive therapy. J. ECT 18, 182–188 (2002).
Blumberger, D. M. et al. Effectiveness of theta burst versus high-frequency repetitive transcranial magnetic stimulation in patients with depression (THREE-D): a randomised non-inferiority trial. Lancet 391, 1683–1692 (2018).
Aleman, A. et al. Moderate effects of noninvasive brain stimulation of the frontal cortex for improving negative symptoms in schizophrenia: meta-analysis of controlled trials. Neurosci. Biobehav. Rev. 89, 111–118 (2018).
He, H. et al. Repetitive transcranial magnetic stimulation for treating the symptoms of schizophrenia: a PRISMA compliant meta-analysis. Clin. Neurophysiol. 128, 716–724 (2017).
Osoegawa, C. et al. Non-invasive brain stimulation for negative symptoms in schizophrenia: an updated systematic review and meta-analysis. Schizophr. Res. 197, 34–44 (2018).
Wang, J. et al. Efficacy towards negative symptoms and safety of repetitive transcranial magnetic stimulation treatment for patients with schizophrenia: a systematic review. Shanghai Arch Psychiatry 29, 61–76 (2017).
Chauhan, P. et al. Efficacy of intensive cerebellar intermittent theta burst stimulation (iCiTBS) in treatment-resistant schizophrenia: a randomized placebocontrolled study. Cerebellum 20, 116–123 (2020).
Guan, H. Y. et al. High-frequency neuronavigated rTMS effect on clinical symptoms and cognitive dysfunction: a pilot double-blind, randomized controlled study in veterans with schizophrenia. Transl. Psychiatry 10, 79 (2020).
Güleken, M. D. et al. The effect of bilateral high frequency repetitive transcranial magnetic stimulation on cognitive functions in schizophrenia. Schizophr. Res. Cogn. 22, 100183 (2020).
Kumar, N. et al. A randomized, double blind, sham-controlled trial of repetitive transcranial magnetic stimulation (rTMS) in the treatment of negative symptoms in schizophrenia. Brain Stimul. 13, 840–849 (2020).
Singh, S. et al. The safety and efficacy of adjunctive 20-Hz repetitive transcranial magnetic stimulation for treatment of negative symptoms in patients with schizophrenia: a double-blinded, randomized, sham-controlled study. Indian J. Psychiatry 62, 21–29 (2020).
Wang, L. et al. Intermittent theta burst stimulation (iTBS) adjustment effects of schizophrenia: results from an exploratory outcome of a randomized double-blind controlled study. Schizophr. Res. 216, 550–553 (2020).
Xiu, M. H. et al. Cognitive enhancing effect of high-frequency neuronavigated rTMS in chronic schizophrenia patients with predominant negative symptoms: a double-blind controlled 32-week follow-up study. Schizophr. Bull. 46, 1219–1230 (2020).
Bation, R. et al. Intermittent theta burst stimulation for negative symptoms of schizophrenia-A double-blind, sham-controlled pilot study. NPJ Schizophr. 7, 10 (2021).
Pan, Z. et al. The effects of repetitive transcranial magnetic stimulation in patients with chronic schizophrenia: insights from EEG microstates. Psychiatry Res. 299, 113866 (2021).
Liberati, A. et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ 339, b2700 (2009).
Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org
Kay, S. R., Fiszbein, A. & Opler, L. A. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr. Bull. 13, 261–276 (1987).
Andreasen, N. C. The scale for the assessment of negative symptoms (SANS): conceptual and theoretical foundations. Br. J. Psychiatry Suppl. 7, 49–58 (1989).
Review Manager (RevMan) [Computer program]. Version 5.4, The Cochrane Collaboration, (2020). https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman.
Kraemer, H. C. & Kupfer, D. J. Size of treatment effects and their importance to clinical research and practice. Biol. Psychiatry 59, 990–996 (2006).
Addington, D., Addington, J. & Maticka-Tyndale, E. Assessing depression in schizophrenia: the Calgary Depression Scale. Br. J. Psychiatry Suppl. 22, 39–44 (1993).
Novák, T. et al. The double-blind sham-controlled study of high-frequency rTMS (20 Hz) for negative symptoms in schizophrenia: negative results. Neuro. Endocrinol. Lett. 27, 209–213 (2006).
Chibbaro, G. et al. Repetitive transcranial magnetic stimulation in schizophrenic patients reporting auditory hallucinations. Neurosci. Lett. 383, 54–57 (2005).
Goyal, N., Nizamie, S. H. & Desarkar, P. Efficacy of adjuvant high frequency repetitive transcranial magnetic stimulation on negative and positive symptoms of schizophrenia: preliminary results of a double-blind sham-controlled study. J. Neuropsychiatry Clin. Neurosci. 19, 464–467 (2007).
Hajak, G. et al. High-frequency repetitive transcranial magnetic stimulation in schizophrenia: a combined treatment and neuroimaging study. Psychol. Med. 34, 1157–1163 (2004).
Mogg, A. et al. Repetitive transcranial magnetic stimulation for negative symptoms of schizophrenia: a randomized controlled pilot study. Schizophr. Res. 93, 221–228 (2007).
Rosenberg, O. et al. Deep transcranial magnetic stimulation add-on for the treatment of auditory hallucinations: a double-blind study. Ann. Gen. Psychiatry, 13 (2012). https://pubmed.ncbi.nlm.nih.gov/22559192/.
Schneider, A. L., Schneider, T. L. & Stark, H. Repetitive transcranial magnetic stimulation (rTMS) as an augmentation treatment for the negative symptoms of schizophrenia: a 4-week randomized placebo controlled study. Brain Stimul. 1, 106–111 (2008).
Cordes, J. et al. Effects of 10 Hz repetitive transcranial magnetic stimulation (rTMS) on clinical global impression in chronic schizophrenia. Psychiatry Res. 177, 32–36 (2010).
Blumberger, D. M. et al. MRI-targeted repetitive transcranial magnetic stimulation of Heschl’s gyrus for refractory auditory hallucinations. Brain Stimul. 5, 577–585 (2012).
Fitzgerald, P. B. et al. A double-blind sham-controlled trial of repetitive transcranial magnetic stimulation in the treatment of refractory auditory hallucinations. J. Clin. Psychopharmacol. 25, 358–362 (2005).
Koops, S. et al. Theta burst transcranial magnetic stimulation for auditory verbal hallucinations: negative findings from a double-blind-randomized trial. Schizophr. Bull. 42, 250–257 (2016).
Langguth, B. et al. Repetitive transkranielle Magnetstimulation bei Schizophrenie: Vorläufige Ergebnisse. Nervenheilkunde: Zeitschrift für interdisziplinaere Fortbildung 22, 350–353 (2003).
Lee, S. H. et al. A double blind study showing that two weeks of daily repetitive TMS over the left or right temporoparietal cortex reduces symptoms in patients with schizophrenia who are having treatment-refractory auditory hallucinations. Neurosci. Lett. 376, 177–181 (2005).
Lin, X. D. et al. Effects of repetitive transcranial magnetic stimulation treatment on event-related potentials in schizophrenia. Chin. Med. J. 131, 301–306 (2018).
Maïza, O. et al. Impact of repetitive transcranial magnetic stimulation (rTMS) on brain functional marker of auditory hallucinations in schizophrenia patients. Brain Sci. 3, 728–743 (2013).
Voineskos, A. N. et al. Effects of repetitive transcranial magnetic stimulation on working memory performance and brain structure in people with schizophrenia spectrum disorders: a double-blind, randomized, sham-controlled trial. Biol. Psychiatry Cogn. Neurosci. Neuroimaging (2020). https://pubmed.ncbi.nlm.nih.gov/33551284/.
Wing, V. C. et al. High frequency repetitive transcranial magnetic stimulation reduces tobacco craving in schizophrenia. Schizophr. Res. 139, 264–266 (2012).
Kim, E.-J. et al. Bilateral repetitive transcranial magnetic stimulation for auditory hallucinations in patients with schizophrenia: a randomized controlled, cross-over study. Clin. Psychopharmacol. Neurosci. 12, 222–228 (2014).
Klirova, M. et al. Individualized rTMS neuronavigated according to regional brain metabolism (18FGD PET) has better treatment effects on auditory hallucinations than standard positioning of rTMS: a double-blind, sham-controlled study. Eur. Arch. Psychiatry Clin. Neurosci. 263, 475–484 (2013).
McIntosh, A. M. et al. Transcranial magnetic stimulation for auditory hallucinations in schizophrenia. Psychiatry Res. 127, 9–17 (2004).
Vercammen, A. et al. Effects of bilateral repetitive transcranial magnetic stimulation on treatment resistant auditory–verbal hallucinations in schizophrenia: a randomized controlled trial. Schizophr. Res. 114, 172–179 (2009).
Jandl, M. et al. Treating auditory hallucinations by transcranial magnetic stimulation: a randomized controlled cross-over trial. Neuropsychobiology 53, 63–69 (2006).
Kimura, H. et al. A randomized, sham-controlled study of high frequency rTMS for auditory hallucination in schizophrenia. Psychiatry Res. 241, 190–194 (2016).
Mendes-Filho, V. A. et al. Effects of repetitive transcranial magnetic stimulation over supplementary motor area in patients with schizophrenia with obsessive-compulsive-symptoms: a pilot study. Psychiatry Res. 242, 34–38 (2016).
Rollnik, J. D. et al. High frequency repetitive transcranial magnetic stimulation (rTMS) of the dorsolateral prefrontal cortex in schizophrenic patients. Neuroreport 11, 4013–4015 (2000).
Hoffman, R. E. et al. Transcranial magnetic stimulation of left temporoparietal cortex in three patients reporting hallucinated “voices”. Biol. Psychiatry 46, 130–132 (1999).
Hoffman, R. E. et al. Transcranial magnetic stimulation and auditory hallucinations in schizophrenia. Lancet 355, 1073–1075 (2000).
Hoffman, R. E. et al. Transcranial magnetic stimulation of left temporoparietal cortex and medication-resistant auditory hallucinations. Arch. Gen. Psychiatry 60, 49–56 (2003).
Hoffman, R. E. et al. Temporoparietal transcranial magnetic stimulation for auditory hallucinations: safety, efficacy and moderators in a fifty patient sample. Biol. Psychiatry 58, 97–104 (2005).
Hoffman, R. E. et al. Transcranial magnetic stimulation of Wernicke’s and Right homologous sites to curtail “voices”: a randomized trial. Biol. Psychiatry 73, 1008–1014 (2013).
Jin, Y. et al. Alpha EEG guided TMS in schizophrenia. Brain Stimul. 5, 560–568 (2012).
Jin, Y. et al. Therapeutic effects of individualized alpha frequency transcranial magnetic stimulation (αTMS) on the negative symptoms of schizophrenia. Schizophr. Bull. 32, 556–561 (2006).
Bais, L. et al. Short and long term effects of left and bilateral repetitive transcranial magnetic stimulation in schizophrenia patients with auditory verbal hallucinations: a randomized controlled trial. PLoS ONE 9, e108828 (2014).
Barr, M. S. et al. A randomized controlled trial of sequentially bilateral prefrontal cortex repetitive transcranial magnetic stimulation in the treatment of negative symptoms in schizophrenia. Brain Stimul. 5, 337–346 (2012).
de Jesus, D. R. et al. A pilot double-blind sham-controlled trial of repetitive transcranial magnetic stimulation for patients with refractory schizophrenia treated with clozapine. Psychiatry Res. 188, 203–207 (2011).
Dlabac-de Lange, J. J. et al. Efficacy of bilateral repetitive transcranial magnetic stimulation for negative symptoms of schizophrenia: results of a multicenter double-blind randomized controlled trial. Psychol. Med. 45, 1263–1275 (2015).
Dollfus, S. et al. High-frequency neuronavigated rTMS in auditory verbal hallucinations: a pilot double-blind controlled study in patients with schizophrenia. Schizophr. Bull. 44, 505–514 (2018).
Fitzgerald, P. B. et al. A study of the effectiveness of bilateral transcranial magnetic stimulation in the treatment of the negative symptoms of schizophrenia. Brain Stimul. 1, 27–32 (2008).
Garg, S. et al. The efficacy of cerebellar vermal deep high frequency (theta range) repetitive transcranial magnetic stimulation (rTMS) in schizophrenia: a randomized rater blind-sham controlled study. Psychiatry Res. 243, 413–420 (2016).
Holi, M. M. et al. Left prefrontal repetitive transcranial magnetic stimulation in schizophrenia. Schizophr. Bull. 30, 429–434 (2004).
Huang, W. et al. Effect of repetitive transcranial magnetic stimulation on cigarette smoking in patients with schizophrenia. Shanghai Arch. Psychiatry 28, 309–317 (2016).
Klein, E. et al. Right prefrontal slow repetitive transcranial magnetic stimulation in schizophrenia: a double-blind sham-controlled pilot study. Biol. Psychiatry 46, 1451–1454 (1999).
Paillère-Martinot, M. L. et al. Active and placebo transcranial magnetic stimulation effects on external and internal auditory hallucinations of schizophrenia. Acta Psychiatr. Scand. 135, 228–238 (2017).
Prikryl, R. et al. Treatment of negative symptoms of schizophrenia using repetitive transcranial magnetic stimulation in a double-blind, randomized controlled study. Schizophr. Res. 95, 151–157 (2007).
Prikryl, R. et al. Does repetitive transcranial magnetic stimulation have a positive effect on working memory and neuronal activation in treatment of negative symptoms of schizophrenia?. Neuroendocrinol. Lett. 33, 90–97 (2012).
Prikryl, R. et al. Repetitive transcranial magnetic stimulation reduces cigarette consumption in schizophrenia patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 49, 30–35 (2014).
Prikryl, R. et al. A detailed analysis of the effect of repetitive transcranial magnetic stimulation on negative symptoms of schizophrenia: a double-blind trial. Schizophr. Res. 149, 167–173 (2013).
Quan, W. X. et al. The effects of high-frequency repetitive transcranial magnetic stimulation (rTMS) on negative symptoms of schizophrenia and the follow-up study. Neurosci. Lett. 584, 197–201 (2015).
Rabany, L., Deutsch, L. & Levkovitz, Y. Double-blind, randomized sham controlled study of deep-TMS add-on treatment for negative symptoms and cognitive deficits in schizophrenia. J. Psychopharmacol. 28, 686–690 (2014).
Rosa, M. O. et al. Effects of repetitive transcranial magnetic stimulation on auditory hallucinations refractory to clozapine. J. Clin. Psychiatry 68, 1528–1532 (2007). p.
Saba, G., Schurhoff, F. & Leboyer, M. Therapeutic and neurophysiologic aspects of transcranial magnetic stimulation in schizophrenia. Neurophysiologie Clinique 36, 185–194 (2006).
Tikka, S. K. et al. Safety and efficacy of adjunctive T burst repetitive transcranial magnetic stimulation to right inferior parietal lobule in schizophrenia patients with first-rank symptoms a pilot, exploratory study. J. ECT 33, 43–51 (2017).
Wobrock, T. et al. Left prefrontal high-frequency repetitive transcranial magnetic stimulation for the treatment of schizophrenia with predominant negative symptoms: a sham-controlled, randomized multicenter trial. Biol. Psychiatry 77, 979–988 (2015).
Zhao, S. et al. Randomized controlled trial of four protocols of repetitive transcranial magnetic stimulation for treating the negative symptoms of schizophrenia. Shanghai Arch. Psychiatry 26, 15–21 (2014).
Zhuo, K. et al. Repetitive transcranial magnetic stimulation as an adjunctive treatment for negative symptoms and cognitive impairment in patients with schizophrenia: a randomized, double-blind, sham-controlled trial. Neuropsychiatr. Dis. Treat. 15, 1141–1150 (2019).
Gan, J. et al. Effectiveness and safety of high dose transcranial magnetic stimulation in schizophrenia with refractory negative symptoms: a randomized controlled study. Zhonghua Yi Xue Za Zhi 95, 3808–3812 (2015).
Ren, Y.-P. et al. Effects of high frequency repetitive transcranial magnetic stimulation on refractory negative symptom of schizophrenia: a double blind, randomized controlled trial. Chin. Mental Health Journal 25, 89–92 (2011).
Xu, W. J. et al. Double-blind control trial of alpha electroencephalogram-guided transcranial magnetic stimulation treatment for schizophrenia. Chin. J. Clin. Rehabil. 10, 22–24 (2006).
Wen-Xiang, Q. et al. Effects of low frequency repetitive transcranial magnetic stimulation on auditory hallucination in patients with schizophrenia. Chin. Mental Health J. 26, 204–208 (2012).
Li, Z. et al. Delayed effect of repetitive transcranial magnetic stimulation (rTMS) on negative symptoms of schizophrenia: findings from a randomized controlled trial. Psychiatry Res. 240, 333–335 (2016).
Chen, H. Y. et al. Effect of adjunctive treatment with repetitive transcranial magnetic stimulation on exploratory eye movements and negative symptoms in schizophrenic patients: a randomized, double-blind, sham-controlled study. Shanghai Arch. Psychiatry 23, 200–206 (2011).
Duan, H. F. et al. Therapeutic effect of repetitive transcranial magnetic stimulation for refractor y negative symptom of schizophrenia. Xinxiang Yi Xue Yuan Xue Bao 30 (2013).
Gan, J. L. et al. A randomized controlled trial of a short pulsed transcranial magnetic stimulation in the treatment of refractory negative symptoms of schizophrenia. Zhong Hua Jing Shen Ke Za Zhi. 191–192 (2014).
Gan, J. L. et al. Effects of repetitive transcranial magnetic stimulation on schizophrenia with refractory negative symptoms and brain-derived neurotrophic factor. Zhongguo Shen Jing Jing Shen Ji Bing Za Zhi. 2014 (2014).
LiuH, L. H., Liu, R. & Wang J. J. The analysis of curative effect of negative symptoms in schizophrenic patients after the treatment of repetitive transcranial magnetic stimu-lation (rTMS). Xian Dai Dian Sheng Li XueZaZhi. (2008).
Ma, S. J., W, Z., Huang, Y. Q., Lin, L. B. & Gao, Z. S. Clinical efficacy of repetitive transcranial magnetic stimulation on first episode schizophrenia patients. Zhong Hua Lin Chuang Yi Shi Za Zhi (Dian Zi Ban) (2016).
Xu, Q., Z, Y. & Cheng, Z. H. Efficacy and safety of repetitive transcranial magnetic stimulation in the treatment of negative symptoms of chronic schizophrenia. Zhong Hua Yi Xue Hui Di Shi Qi Ci Quan Guo Xin Wei Yi Xue Xue Shu Hui Yi Lun Wen Ji (2015).
Zhang, J. J. et al. Double-blind randomized controlled trial of repetitive transcranial magnetic stimulation in the treatment of the negative symptoms of schizophrenia. Shanghai Arch Psychiatry (2010).
Zhang, C. H., Y, Z., Zhang, G. & Yang, G. H. Study on effect of repetitive transcranial magnetic stimulation combined with ziprasidone in the treatment of the negative symptoms of schizophrenia. Zhongguo Xian Dai Yi Yao Za Zhi (2015).
Zheng, L. N., G, Q., Li, H., Li, C. B. & Wang, J. J., Effects of repetitive transcranial magnetic stimulation with different paradigms on the cognitive function and psychotic symptoms of schizophrenia patients. Beijing Da Xue Xue Bao (Yi Xue Ban). (2012).
Bai, L. I., G, J., Xuejun, L., Huifeng, D. & Cunyou, G. Effects of repetitive transcranial magnetic stimulation on diffusion tensor imaging and negative symptoms in patients with schizophrenia. Chin. J. Health Psychol. 23, 649–653 (2015).
Wang, Y. F., L, B., Teng, J. B. & Xia, Y. Efficacy and safety of repetitive transcranial magnetic stimulation in the treatment of schizophrenia with negative symptoms. Zhejiang Zhong Xi Yi Jie He Za Zhi 4, 331–333+340 (2015).
Tamminga, C. A. et al. Limbic system abnormalities identified in schizophrenia using positron emission tomography with fluorodeoxyglucose and neocortical alterations with deficit syndrome. Arch. General Psychiatry 49, 522–530 (1992).
Wible, C. G. et al. Prefrontal cortex, negative symptoms, and schizophrenia: an MRI study. Psychiatry Res.: Neuroimaging 108, 65–78 (2001).
Brady, R. O. Jr et al. Cerebellar-prefrontal network connectivity and negative symptoms in schizophrenia. Am. J. Psychiatry 176, 512–520 (2019).
Brunoni, A. R. et al. Repetitive transcranial magnetic stimulation for the acute treatment of major depressive episodes: a systematic review with network meta-analysis. JAMA Psychiatry 74, 143–152 (2017).
Nguyen, T. D. et al. The efficacy of repetitive transcranial magnetic stimulation (rTMS) for bipolar depression: a systematic review and meta-analysis. J. Affect. Disord. 279, 250–255 (2021).
Author information
Authors and Affiliations
Contributions
The study was designed by all authors. The screening and selection of articles was carried out by R.L. and T.D.N. The data extraction was performed by R.L. and F.H. The assessment of bias was carried out by R.L. The statistical analyses were conducted by R.L. and F.H. The results were interpreted by all authors. The manuscript was drafted by R.L. and S.D.Ø. T.D.N., A.M. and F.H. revised the manuscript for important intellectual content. The final manuscript was approved by all authors prior to submission.
Corresponding author
Ethics declarations
Competing interests
A.M. has served as an advisor for Allergan Canada. S.D.Ø. received the 2020 Lundbeck Foundation Young Investigator Prize. Furthermore, S.D.Ø. owns units of mutual funds with stock tickers DKIGI and WEKAFKI, as well as units of exchange-traded funds with stock tickers TRET, QDVE, QDVH, EUNL and SADM.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lorentzen, R., Nguyen, T.D., McGirr, A. et al. The efficacy of transcranial magnetic stimulation (TMS) for negative symptoms in schizophrenia: a systematic review and meta-analysis. Schizophr 8, 35 (2022). https://doi.org/10.1038/s41537-022-00248-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41537-022-00248-6
- Springer Nature Limited
This article is cited by
-
Prolonged intermittent theta burst stimulation targeting the left prefrontal cortex and cerebellum does not affect executive functions in healthy individuals
Scientific Reports (2024)
-
Prefrontal cortical dopamine deficit may cause impaired glucose metabolism in schizophrenia
Translational Psychiatry (2024)
-
Psychosis superspectrum II: neurobiology, treatment, and implications
Molecular Psychiatry (2024)
-
A pilot study to examine the association between COX-2 rs5275 polymorphism and the response to repetitive transcranial stimulation in schizophrenia
Schizophrenia (2023)
-
Transcranial Magnetic Stimulation in the Treatment of Positive, Negative, and Cognitive Symptoms of Psychosis
Current Behavioral Neuroscience Reports (2023)