
Abstract
SIX1 and SIX6 are glaucoma susceptibility genes. Previous reports indicate that the single nucleotide polymorphism (SNP) rs33912345 in SIX6 is associated with inferior circumpapillary retinal nerve fibre layer (cpRNFL) thickness (cpRNFLT). Although the region of visual field defect in glaucoma patients is directly related to cpRNFL thinning, a detailed sector analysis has not been performed in genetic association studies. In the present study, we evaluated 26 tagging SNPs in the SIX1/SIX6 locus ±50 kb region in a population of 2,306 Japanese subjects with 4- and 32-sector cpRNFLT analysis. While no SNPs showed a significant association with cpRNFLT in the 4-sectored analysis, the finer 32-sector assessment clearly showed a significant association between rs33912345 in the SIX1/SIX6 locus with inferior cpRNFL thinning at 292.5–303.8° (β = −4.55, P = 3.0 × 10−5). Furthermore, the fine-sectored cpRNFLT analysis indicated that SIX1/SIX6 polymorphisms would affect cpRNFL thinning at 281.3–303.8°, which corresponds to parafoveal scotoma in a visual field test of glaucoma patients.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Glaucoma is a complex vision-threatening disorder with a multifactorial aetiology that includes both genetic and environmental factors1,2,3, and it is one of the most prevalent causes of irreversible blindness worldwide4. To date, various glaucoma susceptibility genes have been identified by genome-wide association studies (GWAS)5,6,7,8,9,10,11,12,13. While the majority of associated genes have been characterized5,6,7,8, GWAS for glaucoma endophenotypes—such as vertical cup-to-disc ratio (VCDR)9, 10 and intraocular pressure (IOP)11,12,13—have also contributed to the discovery of glaucoma susceptibility genes, indicative of endophenotype-specific genetic associations. Of the known glaucoma susceptibility genes, several have been shown to exhibit associations with race14, sex15, 16, and the location of the visual field defect (VFD)17,18,19,20.
Although glaucomatous VFD generally occurs in the upper hemifield, early involvement of the inferior hemifield and/or the paracentral VFD has been observed in certain subgroups with low-tension glaucoma or myopia, resulting in severely impaired quality of vision (QOV) from the initial stages of disease21,22,23,24,25. Therefore, the ability to predict the risk of these QOV-threatening VFD patterns using specific genetic associations to the locations of the VFD would be highly beneficial. However, current visual field testing is based on subjective patient responses and can be susceptible to various extraneous factors, such as cataract, dementia, concentration, and physical conditions, thus preventing an accurate evaluation of the associations between susceptibility genes and VFD patterns.
Recent advances in optical coherence tomography (OCT) have allowed ophthalmologists to perform quantitative evaluations of circumpapillary retinal nerve fibre layer thickness (cpRNFLT), which represents glaucomatous optic neuropathy (GON) with high reproducibility and reliability. This morphological testing method generates objective data less influenced by the problems listed above26. The association between cpRNFLT and VFD pattern is highly correlative27,28,29, suggesting that cpRNFLT would be a better measure to evaluate the genetic contribution to GON endophenotype than visual field testing.
To date, genetic studies on cpRNFLT have shown consistent contributions of the single nucleotide polymorphisms (SNPs) rs33912345 and rs10483727 located within the SIX1/SIX6 loci to cpRNFL thinning in the superior and inferior sectors, but not in the temporal, nasal, and global sectors30,31,32. The significance of the SIX1/SIX6 locus in glaucoma was initially discovered by GWAS for VCDR and primary open-angle glaucoma (POAG), and subsequent studies confirmed the association of polymorphisms in this region with glaucoma onset.9, 33, 34 According to previous GON structure-function correlations27,28,29, a finer cpRNFLT analysis with >4 sectors would be better suited to fully evaluate the risk of QOV-threatening VFD patterns. Therefore, the present study examined genetic associations of the SIX1/SIX6 locus with cpRNFLT using 4- and 32-sector analyses.
Results
Study population
Participants were excluded due to prior intraocular surgery (N = 125), axial length ≥26 mm (N = 258), presence of other ocular disease (N = 64), and cpRNFL image quality (N = 54) as described in the Methods section. A total of 2,306 subjects passed the exclusion criteria and the participant demographics are shown in Table 1. The average age was 57.6 ± 13.6 years (mean ± SD; range, 34–80 years). Mean axial length of the right eye was 23.78 ± 1.04 mm (range, 16.46–25.99 mm). Two-thirds of the participants (68.9%) were females; however, this did not affect global cpRNFLT after the adjustment for age and axial length. The mean global cpRNFLT was 101.6 ± 12.0 μm, and 122.4 ± 20.0 μm, 132.1 ± 20.8 μm, 76.3 ± 13.9 μm, and 75.5 ± 14.3 μm in the superior, inferior, temporal, and nasal sectors, respectively.
Association of SIX1/SIX6 polymorphisms with regional cpRNFLT
Association of the 26 tagging SNPs along the 4 cpRNFLT sectors are shown in Table 2. Only rs12147345 showed a marginal association with cpRNFLT in the temporal region (β = 1.08; 95% confidential interval [CI], 0.26–1.90; P = 0.010). On the other hand, a finer assessment with 32 sectors found 5 additional SIX1/SIX6 SNPs, including rs33912345, to be significantly or marginally associated with a cpRNFLT region, mostly in inferior sectors (Table 3). Among these 6 SNPs, only rs148908311 showed a marginal association with cpRNFLT in the superior region, whereas the other 5 SNPs showed significant or marginal associations with cpRNFLT in the inferior regions. The strongest and only significant association (P < 6.0 × 10−5; 0.05/26 SNPs/32 sectors) was observed between rs33912345 and cpRNFLT in the inferior region at 292.5–303.8° (β = −4.55; 95% CI, −2.42–−6.69), P = 3.0 × 10−5). For all SNPs that were significantly or marginally associated with regional cpRNFLTs, we confirmed identical effect directions of the genetic variances to the regional cpRNFLT as to the global cpRNFLT.
We observed that rs10483727—the only SIX1/SIX6 SNP previously associated with glaucoma susceptibility by GWAS—was in close linkage disequilibrium (LD) with rs33912345 (R-sq = 0.99 in the JPT 1000 genomes dataset). Although rs10483727 was not included in the tagging SNPs in the present study, the C risk allele of rs33912345 (corresponding to the T risk allele of rs10483727) resulted in both regional and global cpRNFL thinning.
Discussion
Our study used a tagging SNP approach to show that polymorphisms in the SIX1/SIX6 region was significantly associated with inferior cpRNFLT and marginally associated with superior cpRNFLT in a community-based Japanese cohort. These results were consistent with previous candidate SNP evaluations on rs3391234530,31,32. In addition, our findings suggest that the 32-sector region-based approach for cpRNFLT enables the detection of underpowered and undermined genetic associations in 4-sector analyses.
The importance of the SIX1/SIX6 locus in glaucoma was initially discovered by a GWAS for VCDR, and subsequent GWAS for POAG confirmed the association between polymorphisms in this locus with glaucoma onset9, 33, 34. This is the only locus where an association with cpRNFLT has been established30,31,32. In this study, our detailed analysis further specified the cpRNFL region of association, and revealed that SIX1/SIX6 affects cpRNFL thinning at 281.3–303.8° among the inferior region, which may have clinical and biological relevance since retinal nerve fibre layer defects also occur in this region. In addition, according to the Garway-Heath map27, RNFL thinning of this region would lead to upper mid-peripheral VFD and so-called early upper nasal step35. Because VFD in this region typically results from early-stage glaucoma, SIX1/SIX6 could be associated with initial changes in GON; however, optic fissure closures—known as colobomas—also present in this area. While eyes with apparent colobomas were excluded from our analysis, subclinical cases would likely influence the statistical data. Moreover, since PAX6 mutations are associated with coloboma formation36 and correlate with SIX6 activation during eye development37, SIX1/SIX6 polymorphisms could be involved in the pathophysiology of cpRNFL thinning in the inferior region. Although previous reports have not shown a connection between SIX6 SNPs and coloboma formation38, 39, further genetic studies with 32-sector cpRNFLT analysis would likely lead to the identification of other genes with key roles in glaucomatous VFD development.
Our findings would suggest that we should evaluate genetic associations to cpRNFLT by dividing it into 32 sectors rather than dividing it into 4 sectors or evaluating cpRNFLT as a whole. Notably, we found a significant association between rs33912345 and inferior region cpRNFLT at 292.5–303.8° (P = 0.025 after Bonferroni correction) in the 32-sectored cpRNFLT analysis, whereas rs33912345 was not significantly associated with the inferior region (225–315°) in the 4-sectored analysis (P = 1.0 after Bonferroni correction). Furthermore, all SNPs with marginal P-values at 292.5–303.8 and 281.3–292.5° showed an equivalent contribution to cpRNFL thinning to that observed with rs33912345. In addition, rs10483727—a RNFLT-susceptible SNP not included in our analysis—showed a significant association with inferior region cpRNFLT at 281.3-303.8° (P = 0.016 and P = 0.016 after Bonferroni correction, respectively) in the 32-sector analysis, but not in the 4-sector analysis (225–315°; P = 1.0 after Bonferroni correction) (Supplementary Tables 1 and 2).
Based on a previous study, cpRNFL thinning at 281.3–303.8° should correspond to mid-peripheral scotoma since central VFD is associated with cpRNFL thinning at 311–40° 27. VFD is usually classified as central/mid-peripheral/peripheral scotoma, superior/inferior altitudinal defect, or temporal/nasal hemianopia that shared features of the clinically observed visual field patterns40. The altitudinal boundary is separated at 12° around optic nerve head (ONH)41; thus, cpRNFL should be evaluated at 12° interval or less (at least 30 sectors) to fully evaluate its correspondence to VFD patterns. To our knowledge, this is the first study evaluating the applicability of a region-based approach for GON analysis by examining the genetic contributions of glaucoma susceptibility genes with regional cpRNFLT. Therefore, genetic studies using 32-sectored cpRNFLT might reveal further associations to clinically important glaucoma phenotypes.
To date, three studies have reported significant associations of SIX1/SIX6 polymorphisms to cpRNFL thinning in the upper and lower sectors—but not the nasal and temporal sectors—in 30 POAG cases32, 1,243 population controls31, and 231 other participants consisting of 20% normal, 44% of suspected glaucoma, and 36% confirmed glaucoma cases30. In contrast, our analyses used 2,306 population controls and showed that rs33912345 had the strongest association with cpRNFLT at 292.5–303.8° and a marginal association at 78.8–90.0°. RNFL thinning at 281.3–303.8° would lead to upper mid-peripheral VFDs that could lead to an early upper nasal step27, 35. However, further genetic studies on visual field testing are necessary to confirm whether the SIX1/SIX6 locus would be an appropriate locus to determine the genetic factors underlying GON in the upper visual fields.
There are several limitations to this study. First, the VFD data was not obtained in our cohort. As the clinical importance of VFD has been widely accepted in GON studies, further confirmation analyses on VFD are needed. Nevertheless, we believe that cpRNFLT is an objective value with high reliability and repeatability and can facilitate the identification of hidden genetic associations for VFD. Second, only data from the right eye of subjects were analysed due to the time constraints placed on OCT acquisition; however, because both eyes are equally affected by genotype, analyses on the left eyes should yield similar findings. Third, the number of participants analysed was rather small compared to the large sample size of the Nagahama cohort. This is mainly because only subjects with genome-wide SNP data and an axial length <26 mm were included in the study. A larger sample analysis might further elucidate its associations to other regions. Fourth, population-based study methods are best evaluated with disease-free subjects. Despite the known association between SIX1/SIX6 SNPs and glaucoma development, these patients were not specifically excluded from the study population since we did not perform visual field testing or slit lamp biomicroscopy required for this diagnosis. Thus, a subsequent study of only healthy subjects will be necessary to confirm the clinical impact of our findings. Lastly, an optimization of sector number may be beneficial in future cpRNFLT studies and it is possible that wider sectors would be sufficient to yield the same result, whereas a finer sector analysis might be able to find other associations.
In conclusion, we confirmed that rs33912345 and rs10483727—the only known cpRNFLT susceptibility SNPs—showed the strongest association with cpRNFLT of those within the SIX1/SIX6 locus. Notably, only the 32-sector cpRNFLT analysis was capable of detecting the significant associations these SNPs with inferior cpRNFL thinning at 292.5–303.8° and 281.3–303.8°, respectively, as the results of 4-sector cpRNFLT analysis were insignificant. Collectively, this suggests that fine regional association analyses are a more effective strategy to assess glaucoma endophenotype in genomic studies and may facilitate the identification of novel genetic associations in disease pathogenesis.
Methods
Ethical considerations
Written informed consent was obtained from all participants. Study procedures adhered to the tenets of the Declaration of Helsinki and were approved by the ethics committee of Kyoto University Graduate School of Medicine and the Nagahama Municipal Review Board.
Study participants
The study population consisted of healthy Japanese volunteers enrolled in the Nagahama Prospective Cohort for Comprehensive Human Bioscience (the Nagahama Study). Participants were recruited between 2008 and 2010 from the general population of Nagahama City, a rural city of 125,000 inhabitants located in central Japan. Community residents from 30–74 years of age, living independently and without physical impairment or dysfunction were eligible. Of the 9,804 included participants, nine withdrew consent to participate, and 26 were excluded because genetic analysis showed an ethnic background other than Japanese. Participants were offered a follow-up assessment 5 years after the baseline evaluation, and 8,294 of the original 9,769 cohort members participated (84.9%).
In the present study, we used a dataset of the follow-up measurement. Study subjects consisted of 2,807 individuals with genome-wide SNP genotyping, axial length, phakic status, and OCT data available by April 2016. Other exclusion criteria included prior intraocular surgery (except for cataract surgery), high myopia (axial length ≥26 mm), and presence of other ocular diseases affecting retinal nerve fibre layer thickness based on fundus photography—such as optic atrophy, anterior ischemic optic neuropathy, optic disc coloboma, retinal vein occlusion, proliferative or severe non-proliferative diabetic retinopathy, retinitis pigmentosa, and other optic neuropathies. Subjects outside of the Japanese ethnic cluster or with poor quality cpRNFL images, which could result from cataracts or small pupils, were also excluded. Glaucomatous status did not serve as exclusion criteria since visual field information was unavailable at the time of analysis. Ultimately, a total of 2,306 subjects with a ≤ 0.9 sample call rate and estimated relatedness (PI-HAT) >0.35 were included in the study population
All subjects were assessed by standardized ophthalmic examination, including an objective determination of the refractive error and corneal curvature (Autorefractor ARK-530; Nidek, Gamagori, Aichi, Japan), fundus imaging (CR-DG10; Canon, Tokyo, Japan), and axial length measurements by partial coherence interferometry (IOL Master; Carl Zeiss Meditec, Inc., Dublin, California, USA). The cpRNFL in the right eye was imaged by spectral-domain optical coherence tomography (SD-OCT) (RS-3000 advanced; Nidek, Gamagori, Aichi, Japan).
Circumpapillary retinal nerve fibre layer thickness
The RS-3000 advanced OCT (Nidek) was used to obtain circular B-scans 11.5° in diameter (3.45 mm in the Gullstrand’s eye) centred on the optic disc, i.e., a circumpapillary scan. Each B-scan was obtained by averaging 50 images in “Regular mode” to reduce speckle noise. The cpRNFL thickness was defined as the distance between the inner border of the internal limiting membrane (ILM) and the outer border of the RNFL in B-scan images, measured automatically with built-in software, and then manually corrected for all images. We excluded eyes with extensive peripapillary atrophy (affecting cpRNFL scans), RNFL schisis, peripapillary epiretinal membrane, or thickened posterior vitreous membrane that affected segmentation, and low quality or other RNFL segmentation errors.
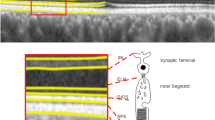
RNFL thickness was measured at 1,024 points along the 360° OCT circle scan, which were subsequently sectioned into 4 or 32 sectors (Fig. 1). Data for each sector were averaged and the associations between the SIX1/SIX6 SNPs and mean cpRNFLT in each region were analysed.

Illustration of the 32 sectors along the RS-3000 advanced (Nidek) optical coherence tomographic (OCT) circular image used for circumpapillary retinal nerve fibre layer thicknesses (cpRNFLT) analysis. (A,B) Circular B-scans 11.5° in diameter (3.45 mm in the Gullstrand’s eye) centred on the optic disc were obtained from the right eye of each participant. (C) cpRNFLT was measured at 1,024 points along the 360° OCT circle scan and divided into 4 or 32 sectors.
Genotyping and imputation
DNA samples were prepared and genotyped as described previously42. Briefly, 3,712 baseline samples were genotyped using at least one of the three genotyping platforms, HumanHap610K Quad Arrays, HumanOmni2.5 M Arrays, or HumanExome Arrays (Illumina, Inc., San Diego, CA). To ensure high-quality genotype data, a series of quality control (QC) filters, including sample success rate (>95%), individual call rate (>99%), minor allele frequency (MAF) cut-off (>0.01), Hardy-Weinberg equilibrium p-values (>1 × 10−6), and estimated relatedness (PI-HAT < 0.35) were applied to the data from each platform. In addition, seven ancestry outliers were identified by principal component analysis with the HapMap Phase 2 release 28 with the Japanese in Tokyo, Japan (JPT) reference dataset using EIGENSTRAT ver. 2.0. QC in PLINK39, 43 (ver.1.07; available at http://pngu.mgh.harvard.edu/~purcell/plink/). As a result, 3,267 baseline and 2,807 follow-up samples passed the QC filters. SNP genotype imputation was performed for the Japanese samples using MaCH44. Genotypes of 89 JPT samples from the 1000 Genomes Project (May 2011 release) were used as reference sequences. Imputed SNPs with an R-squared value less than 0.5 were excluded from the following association analyses.
Our dataset contained 488 SNPs within ±50 kb of the SIX1/SIX6 locus (chr14: 60925938–61166155; NCBI build 37). The Tagger program in Haploview45 was used to identify 26 tagging-SNPs encompassing the 242 known SNPs with an MAF > 0.05 (mean R-sq = 0.962). Since rs33912345 was previously reported as a cpRNFLT-susceptible SNP, it was selected as a tagging SNP for a positive control. The location of these 26 SNPs within the SIX1/SIX6 locus and a linkage disequilibrium plot of this genetic region are shown in Fig. 2.

Construction of the SIX1/SIX6 region and tagging SNPs. (A) Location of the 26 tagging SNPs within the SIX1/SIX6 locus are shown relative to NCBI build 37 of the human genome. (B) A linkage disequilibrium map of the SIX1/SIX6 locus ±50 kb region encompassing the 242 SNPs examined in our analysis was plotted with Haploview 4.2 software. A total of 16 haplotype blocks could be distinguished and 10 SNPs were not included in any of the blocks.
Statistical analysis
Linear regression analyses were performed to determine the associations between regional cpRNFLT and the 26 SNP genotypes assuming additive regression models for a per-minor-allele with an adjustment for age, sex, and axial length. We evaluated regional cpRNFLT associations using 4 divided sectors and finer 32 sectors with Bonferroni corrections. P values < 6.0 × 10−5 (0.05/26 SNPs/32 sectors) and <4.8 × 10−4 (0.05/26 SNPs/4 sectors) were considered statistically significant for cpRNFL in the 32-sector and 4-sectors analyses, respectively, whereas P-values < 0.0016 (0.05/32 sectors) and <0.0125 (0.05/4 sectors) were considered marginally significant, respectively.
References
Tielsch, J. M., Katz, J., Sommer, A., Quigley, H. A. & Javitt, J. C. Family history and risk of primary open angle glaucoma. The Baltimore Eye Survey. Arch. Ophthalmol. 112, 69–73 (1994).
van Koolwijk, L. M. E. et al. Common genetic determinants of intraocular pressure and primary open-angle glaucoma. PLoS Genet. 8, 1002611, doi:10.1371/journal.pgen.1002611 (2012).
Wiggs, J. L. Genetic Etiologies of Glaucoma. Arch. Ophthalmol. 125, 30 (2007).
Tham, Y. C. et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology 121, 2081–2090 (2014).
Burdon, K. P. et al. Genome-wide association study identifies susceptibility loci for open angle glaucoma at TMCO1 and CDKN2B-AS1. Nat. Genet. 43, 574–578 (2011).
Thorleifsson, G. et al. Common variants near CAV1 and CAV2 are associated with primary open-angle glaucoma. Nat. Genet. 42, 906–909 (2010).
Wiggs, J. L. et al. Common variants at 9p21 and 8q22 are associated with increased susceptibility to optic nerve degeneration in glaucoma. PLoS Genet. 8, 1002654, doi:10.1371/journal.pgen.1002654 (2012).
Chen, Y. et al. Common variants near ABCA1 and in PMM2 are associated with primary open-angle glaucoma. Nat. Genet. 46, 1115–1119 (2014).
Ramdas, W. D. et al. A genome-wide association study of optic disc parameters. PLoS Genet. 6, 1000978, doi:10.1371/journal.pgen.1000978 (2010).
Springelkamp, H. et al. Meta-analysis of genome-wide association studies identifies novel loci that influence cupping and the glaucomatous process. Nat. Commun. 5, 4883 (2014).
Blue Mountains Eye Study (BMES) & Wellcome Trust Case Control Consortium 2 (WTCCC2). Genome-wide association study of intraocular pressure identifies the GLCCI1/ICA1 region as a glaucoma susceptibility locus. Hum. Mol. Genet. 22, 4653–4660 (2013).
Hysi, P. G. et al. Genome-wide analysis of multi-ancestry cohorts identifies new loci influencing intraocular pressure and susceptibility to glaucoma. Nat. Genet. 46, 1126–1130 (2014).
van Koolwijk, L. M. E. et al. Common genetic determinants of intraocular pressure and primary open-angle glaucoma. PLoS Genet. 8, 1002611, doi:10.1371/journal.pgen.1002611 (2012).
Rong, S. S. et al. Ethnic specific association of the CAV1/CAV2 locus with primary open-angle glaucoma. Sci. Rep. 6, 27837, doi:10.1038/srep27837 (2016).
Ng, S. K. et al. Genetic Association at the 9p21 Glaucoma Locus Contributes to Sex Bias in Normal-Tension Glaucoma. Invest. Ophthalmol. Vis. Sci. 57, 3416–3421 (2016).
Loomis, S. J. et al. Association of CAV1/CAV2 genomic variants with primary open-angle glaucoma overall and by gender and pattern of visual field loss. Ophthalmology 121, 508–16 (2014).
Loomis, S. J. et al. Association of CAV1/CAV2 genomic variants with primary open-angle glaucoma overall and by gender and pattern of visual field loss. Ophthalmology 121, 508–16 (2014).
Buys, E. S. et al. Soluble guanylate cyclase α1-deficient mice: a novel murine model for primary open angle glaucoma. PLoS One 8, 60156, doi:10.1371/journal.pone.0060156 (2013).
Wiggs, J. L. et al. The p53 codon 72 PRO/PRO genotype may be associated with initial central visual field defects in caucasians with primary open angle glaucoma. PLoS One 7, 45613, doi:10.1371/journal.pone.0045613 (2012).
Pasquale, L. R. et al. CDKN2B-AS1 genotype-glaucoma feature correlations in primary open-angle glaucoma patients from the United States. Am. J. Ophthalmol. 155, 342–353.e5 (2013).
Caprioli, J. & Spaeth, G. L. Comparison of visual field defects in the low-tension glaucomas with those in the high-tension glaucomas. Am. J. Ophthalmol. 97, 730–737 (1984).
Hitchings, R. A. & Anderton, S. A. A comparative study of visual field defects seen in patients with low-tension glaucoma and chronic simple glaucoma. Br. J. Ophthalmol. 67, 818–821 (1983).
Kim, J. M., Kyung, H., Shim, S. H., Azarbod, P. & Caprioli, J. Location of Initial Visual Field Defects in Glaucoma and Their Modes of Deterioration. Invest. Ophthalmol. Vis. Sci. 56, 7956–7962 (2015).
Park, S. C. et al. Initial parafoveal versus peripheral scotomas in glaucoma: risk factors and visual field characteristics. Ophthalmology 118, 1782–1789 (2011).
Sun, Y. et al. The Impact of Visual Field Clusters on Performance-based Measures and Vision-Related Quality of Life in Patients With Glaucoma. Am. J. Ophthalmol. 163, 45–52 (2016).
Nukada, M. et al. Detection of localized retinal nerve fiber layer defects in glaucoma using enhanced spectral-domain optical coherence tomography. Ophthalmology 118, 1038–1048 (2011).
Garway-Heath, D. F., Poinoosawmy, D., Fitzke, F. W. & Hitchings, R. A. Mapping the visual field to the optic disc in normal tension glaucoma eyes. Ophthalmology 107, 1809–1815 (2000).
Hood, D. C., Raza, A. S., de Moraes, C. G. V., Liebmann, J. M. & Ritch, R. Glaucomatous damage of the macula. Prog. Retin. Eye Res. 32, 1–21 (2013).
Nakanishi, H. et al. Clustering of Combined 24-2 and 10-2 Visual Field Grids and Their Relationship With Circumpapillary Retinal Nerve Fiber Layer Thickness. Invest. Ophthalmol. Vis. Sci. 57, 3203–3210 (2016).
Kuo, J. Z. et al. Quantitative Trait Locus Analysis of SIX1-SIX6 With Retinal Nerve Fiber Layer Thickness in Individuals of European Descent. Am. J. Ophthalmol. 160, 123–130.e1 (2015).
Cheng, C. Y. et al. Association of common SIX6 polymorphisms with peripapillary retinal nerve fiber layer thickness: the Singapore Chinese Eye Study. Invest. Ophthalmol. Vis. Sci. 56, 478–483 (2015).
Carnes, M. U. et al. Discovery and functional annotation of SIX6 variants in primary open-angle glaucoma. PLoS Genet. 10, 1004372, doi:10.1371/journal.pgen.1004372 (2014).
Osman, W., Low, S.-K., Takahashi, A., Kubo, M. & Nakamura, Y. A genome-wide association study in the Japanese population confirms 9p21 and 14q23 as susceptibility loci for primary open angle glaucoma. Hum. Mol. Genet. 21, 2836–2842 (2012).
Ramdas, W. D. et al. Common genetic variants associated with open-angle glaucoma. Hum. Mol. Genet. 20, 2464–2471 (2011).
Mizoue, S., Iwase, A., Matsumoto, S. & Yoshikawa, K. [Initial scotomas in normal tension glaucoma]. Nihon Ganka Gakkai Zasshi 118, 826–830 (2014).
Tétreault, N., Champagne, M. P. & Bernier, G. The LIM homeobox transcription factor Lhx2 is required to specify the retina field and synergistically cooperates with Pax6 for Six6 trans-activation. Dev. Biol. 327, 541–550 (2009).
Grindley, J. C., Davidson, D. R. & Hill, R. E. The role of Pax-6 in eye and nasal development. Development 121, 1433–42 (1995).
Zhang, X. et al. Mutational screening of 10 genes in Chinese patients with microphthalmia and/or coloboma. Mol. Vis. 15, 2911–8 (2009).
Aijaz, S. et al. Absence of SIX6 Mutations in Microphthalmia, Anophthalmia, and Coloboma. Investig. Opthalmol. Vis. Sci. 45, 3871 (2004).
Cai, S. et al. Clinical Correlates of Computationally Derived Visual Field Defect Archetypes in Patients from a Glaucoma Clinic. Curr. Eye Res. 1205630, doi:10.1080/02713683.2016.1205630 (2016).
Hood, D. C. & Raza, A. S. On improving the use of OCT imaging for detecting glaucomatous damage. Br. J. Ophthalmol. 98(Suppl 2), ii1–9 (2014).
Oishi, M. et al. Association between ZIC2, RASGRF1, and SHISA6 genes and high myopia in Japanese subjects. Invest. Ophthalmol. Vis. Sci. 54, 7492–7497 (2013).
Purcell, S. et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 81, 559–575 (2007).
Li, Y., Willer, C. J., Ding, J., Scheet, P. & Abecasis, G. R. MaCH: using sequence and genotype data to estimate haplotypes and unobserved genotypes. Genet. Epidemiol. 34, 816–834 (2010).
Barrett, J. C., Fry, B., Maller, J. & Daly, M. J. Haploview: analysis and visualization of LD and haplotype maps. Bioinformatics 21, 263–265 (2005).
Acknowledgements
This work was partly supported by an internal grant from Kyoto University, a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science & Technology in Japan, a Grant-in-Aid for scientific research from the Japan Society for the Promotion of Science, Tokyo (No. 24592624), and Comprehensive Research on Aging and Health Science Research Grants for Dementia R&D from Japan Agency for Medical Research and Development (AMED). Additional support was provided by the Centre of Innovation Program, the Global University Project from Japan Science and Technology Agency, the Practical Research Project for Rare/Intractable Diseases, and the Japan National Society for the Prevention of Blindness, Tokyo, Japan. The authors also thank the Nagahama City Office and non-profit organization Zeroji Club for their help in conducting the Nagahama study.
Author information
Authors and Affiliations
Author notes
A comprehensive list of consortium members appears at the end of the paper
Consortia
Contributions
K.Y. and M. Miyake proposed study concept and design, M.Y., M. Miyata, M. Miyake, Y.H., the Nagahama Study Group, Y.T., and F.M. participated in data acquisition, M.Y., K.Y., Y.T., and N.Y. analysed or interpreted the data, M.Y., K.Y., H.N., and Y.T. wrote the manuscript, and K.Y., Y.T., F.M., and N.Y. revised the manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
Nagahisa Yoshimura has received financial support from Topcon Corporation (Tokyo, Japan), Nidek (Aichi, Japan), and Canon (Tokyo, Japan). All other authors have no financial disclosures.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Consortia The Nagahama Study GroupTakahisa Kawaguchi3, Kazuya Setoh3, Yoshimitsu Takahashi4, Shinji Kosugi5 & Takeo Nakayama4
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yoshikawa, M., Yamashiro, K., Nakanishi, H. et al. Association of SIX1/SIX6 locus polymorphisms with regional circumpapillary retinal nerve fibre layer thickness: The Nagahama study. Sci Rep 7, 4393 (2017). https://doi.org/10.1038/s41598-017-02299-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-02299-7
- Springer Nature Limited
This article is cited by
-
Age-dependent regional retinal nerve fibre changes in SIX1/SIX6 polymorphism
Scientific Reports (2020)