
Abstract
Pancreatic cancer (PDAC) is still lacking of reliable markers to monitor tumor response. CA 19-9 is the only biomarker approved, despite it has several limitations in sensitivity and specificity. Since mutations of KRAS occur in more than 90% of tumors, its detection in circulating free tumor DNA (cftDNA) could represent a biomarker to monitor chemotherapy response. Twenty-seven advanced PDAC patients given first-line 5-fluorouracil, irinotecan and oxaliplatin or gemcitabine and nab-paclitaxel were enrolled. Three ml of plasma were collected: 1) before starting chemotherapy (baseline); 2) at day 15 of treatment; and 3) at each clinical follow-up. cftDNA was extracted and analysed for KRAS mutations (mutKRAS) by digital droplet PCR. Nineteen patients displayed a mutKRAS in baseline plasma samples. There was a statistically significant difference in progression-free survival (PFS) and overall survival (OS) in patients with increase vs. stability/reduction of cftDNA in the sample collected at day 15 (median PFS 2.5 vs 7.5 months, p = 0.03; median OS 6.5 vs 11.5 months, p = 0.009). The results of this study demonstrate that cftDNA mutKRAS changes are associated with tumor response to chemotherapy and support the evidence that mutKRAS in plasma may be used as a new marker for monitoring treatment outcome and disease progression in PDAC.
Similar content being viewed by others

Introduction
Pancreatic adenocarcinoma (PDAC) represents the fourth leading cause of cancer-related deaths in Western countries and only 10–20% of patients are diagnosed with a resectable disease1. Chemotherapy represents the milestone of treatment of advanced disease; indeed, among the combinations developed in recent years, 5-fluorouracil, irinotecan and oxaliplatin (FOLFIRINOX), and the association of gemcitabine and nab-paclitaxel (GEMnPAC) have demonstrated improved survival and represent now the standard of care in first-line treatment2, 3.
However, since pancreatic tumor tissue is surrounded by a dense fibrotic stroma, the evaluation of tumor response to therapy is particularly challenging and imaging techniques do not always provide an accurate estimate, despite the significant costs4, 5. For this reason, the monitoring of these tumors by blood markers is a valuable alternative and is based on the evaluation of the Carbohydrate Antigen 19-9 (CA 19-9) levels, the standard serum marker for pancreatic cancer. Although CA 19-9 has been approved to monitor tumor response, it has several limitations including: (1) low sensitivity and specificity (estimated to be around 79% and 82%, respectively); (2) occurrence of unspecific changes in serum samples; (3) poor accuracy in the identification of small tumors6, 7. These issues limit the utility of CA 19-9 as a biomarker and highlight the need for new biomarkers to complement the imaging in order to obtain a more effective monitoring of these patients and improve the clinical outcome. Alternative approaches for PDAC monitoring are represented by circulating tumor cells (CTCs), which may predict poor disease outcome8, though their use is limited by false negative tests and high costs.
The majority of pancreatic cancers (from 75 to 95%) harbor a KRAS mutation at codon 129 and a significant difference in survival was observed in patients with detectable or undetectable KRAS mutations (mutKRAS) in circulating free tumor DNA (cftDNA)10. Moreover, the presence of mutKRAS in plasma samples after surgical resection of PDAC has been associated with poor survival11, 12. In addition, looking at the specific type of mutation, the presence of KRAS p.G12V seems to be associated with a decrease in survival of pancreatic cancer patients13.
Tissue availability is recognized as a crucial issue, as there are several limitations to obtain repeated biopsies (i.e. invasiveness) and to capture tumor heterogeneity due to the practical constraints to collect multiple samples. In contrast, the detection of somatic mutations in cftDNA released in plasma from apoptotic and necrotic tumor cells both from primary tumor and metastatic lesions is feasible and affordable in terms of costs14. Thus, cftDNA may reflect the tumor burden in cancer patients and is a valuable option for a better monitoring of response; it may complement imaging in order to obtain a more effective management of patients, identify early resistance and improve clinical outcome15.
Therefore, the aim of the present study was to monitor the allelic burden of mutKRAS in patients with advanced PDAC undergoing first-line combination chemotherapy. In particular, the correlation between early variations of cftDNA mutKRAS after 15 days of treatment with response to therapy was explored, in order to provide an effective tool to predict the effectiveness of therapy early after its beginning.
Results
Study population
A total of 27 patients with locally advanced (n = 4; 15%) and metastatic (n = 23; 85%) PDAC were included in this biomarker study (Table 1). Median age was 68 years (range 49–77).
At a median follow up of 7.6 months, 13 patients (54%) underwent disease progression and 6 (22%) died. Median progression-free survival (PFS) and overall survival (OS) were 7.4 and 11.5 months, respectively. Response rate was 38% and disease control rate (DCR) defined as the sum of partial response (PR) and stable disease (SD) was 73%.
Analysis of mutKRAS cftDNA at baseline
At baseline, 19 out of 27 patients (70.4%) were carriers of one mutKRAS allele; 14 subjects were carriers of p.G12D, while 2 patients had the p.G12V, 2 subjects the p.G12R and another the p.G13D. In mutKRAS patients, the amount of cftDNA ranged from 80 to 64800 copies/ml (Table 1). Eight patients were negative for cftDNA mutKRAS at baseline (3 patients were stage III and 5 were stage IV); one of them turned to positivity at day 15 and another one at the first radiological evaluation (2 months after treatment start). There was no statistically significant difference in mutKRAS cftDNA positivity at baseline in patients with metastatic vs. locally advanced disease (p = 0.065). Besides, there was no statistically significant difference in mutKRAS positivity by stratifying patients by gender (p = 0.103), age (p = 0.087), performance status (PS) (p = 1), disease site (p = 0.103), and stage (p = 0.065).
No statistically significant differences in median PFS and OS in patients with baseline positive or negative cftDNA mutKRAS were found (PFS: 7.4 months vs. not reached, p = 0.24; OS: 11.5 months vs. not reached, p = 0.16; Table 2).
On the contrary, there was a statistically significant difference between cftDNA mutKRAS positivity at baseline and the presence of liver metastasis (p = 0.008) or abnormal CA 19-9 levels (p = 0.011).
Monitoring mutKRAS cftDNA during treatment and correlation with outcome
Twenty-five out of 27 patients (17 positive cftDNA mutKRAS and 8 wild type) had more than one blood sample drawn. One patient died within a month of study entry and another one withdrew the consent to participate in the study.
There was a statistically significant difference in PFS between patients displaying an increase vs. stability/reduction of mutKRAS cftDNA at the 15 day-sample (median PFS 2.5 vs. 7.5 months, p = 0.03, Fig. 1). In particular, according to the radiological evaluation 2 months after the beginning of treatment, all patients displaying cftDNA increase at the 15th day (3 baseline mutKRAS and 1 wild type that became mutKRAS) had disease progression.

PFS according to early mutKRAS cftDNA variation (increase vs. reduction).
Interestingly, a statistically significant difference was also observed in median OS (6.5 vs. 11.5 months, p = 0.009) in patients displaying an increase vs. reduction of mutKRAS cftDNA, respectively. None of the other parameters (sex, age, stage, PS, primary tumor location, baseline CA 19-9) was significantly correlated with PFS and/or OS (Table 2).
The early mutKRAS cftDNA variation did not correlate with tumor response (Fisher’s exact test p = 0.09; Mann-Whitney test p = 0.156) even if a trend toward better DCR in patients with early mutKRAS cftDNA decrease was found (Fisher’s exact test p = 0.08; Mann-Whitney test p = 0.059, Fig. 2).

Plot showing early mutKRAS cftDNA variations (% change in number of copies) in patients with PR or SD vs. PD.
Noteworthy, the comparison of mutKRAS cftDNA changes in samples taken at baseline and after 2 months (at the time of first radiological evaluation) demonstrated that median PFS was 7.5 months for patients whose cftDNA mutKRAS decreased vs 2.8 months of subjects with increasing cftDNA mutKRAS levels (p = 0.028). Figure 3 reports the results of 3 representative patients as an example of PR (Fig. 3a), early PD (Fig. 3b) and early disease response followed by progression (Fig. 3c), while on the other hand, Fig. 4 reports the same patients comparing the cftDNA mutKRAS to the CA 19-9 monitoring.

Representative ddPCR plots showing mutKRAS cftDNA variations during follow up of patients. The mutKRAS cftDNA are the blue dots circled in red. Upper panel: metastatic patient who developed PR to first-line FOLFIRINOX. (1) Baseline detection of KRAS p.G12D (11600 copies/ml); (2) p.G12D declined after 15 days (900 copies/ml); (3) p.G12D still reduced after 2 months (130 copies/ml); (4) pG12D is undetectable after 7 months of chemotherapy (0 copies/ml). Middle panel: patient with local recurrence who developed early PD during first-line FOLFIRINOX. (1) Baseline detection of KRAS p.G12D (240 copies/ml); (2) slight increase of p.G12D (245 copies/ml) after 15 days; (3) p.G12D increase (2700 copies/ml) after 2 months. This patient died due to PD two weeks after radiological re-evaluation at 2 months. Lower panel: metastatic patient who developed PR and subsequent early PD to GEMnPAC. (1) Baseline detection of KRAS p.G12D (3200 copies/ml); (2) undetectable cftDNA at day 15 (0 copies/ml); (3) increase of p.G12D (900 copies/ml) after 2 months; (4) further increase of p.G12D (2800 copies/ml) corresponding to radiologically-confirmed PD at 4 months. Clinical condition progressively deteriorated and patients died because of PD 5 months after diagnosis.

Changes in cftDNA mutKRAS levels compred to CA 19-9 in a case of early PD (upper panel), PR (middle panel) and early PR followed by PD (lower panel).
Discussion
The present study provides the evidence that the change of mutKRAS cftDNA levels between baseline vs. day 15 is an early predictor of clinical outcome. To the best of our knowledge, the present study shows for the first time that cftDNA mutKRAS variation is an early marker of response to treatment in PDAC. In our pilot study, all patients having an early increase in cftDNA mutKRAS underwent rapid disease progression, supporting the hypothesis that cftDNA mutKRAS changes are associated with tumor dynamics. Experimental evidences demonstrate that cftDNA is a valuable biomarker to predict the response or resistance to treatment not only with targeted therapies, but also with chemotherapy16.
While previous studies demonstrated that pancreatic cancer patients with detectable mutKRAS cftDNA before or after initiation of chemotherapy have a shorter survival time13, 17, 18, our results did not find a statistically significant difference in median PFS and OS in patients with baseline positive or negative mutKRAS cftDNA (median PFS 7.4 months vs. not reached, p = 0.24; median OS 11.5 months vs. not reached, p = 0.16, respectively). Despite enrolling also patients with locally advanced disease, we did not find any difference between mutKRAS cftDNA positivity in locally advanced vs. metastatic patients. The lack of difference in OS between mutKRAS cftDNA positive and negative patients could be explained by the relatively low number of survival events - at the time of analysis 22% of the patients were deceased - and by differences in the cftDNA mutKRAS detection method used in our study. Of note, the technique used in the present study is characterized by a high sensitivity, as it is able to detect small amounts of cftDNA (median baseline KRAS copies/ml: 2100; range: 80–64800 copies/ml). In fact, in the present study, 70.4% of patients had detectable mutKRAS cftDNA prior to treatment, whereas in previously published studies detectability ranged from 0% to 62.2%13, 17,18,19,20. This high positivity rate may be dependent on the sensitivity of the method used for the analysis being digital droplet PCR (ddPCR) the most sensitive compared to other techniques.
Two out of 6 mutKRAS cftDNA negative patients became positive during treatment, one after 15 days and another after 8 weeks, respectively. It is unclear if this is simply due to one or more of the following reasons: (1) increase in tumor burden; (2) molecular heterogeneity within the primary tumor; (3) changes in dynamics of mutKRAS cftDNA released from cells; or (4) the emergence of metastases or CTCs with different molecular clones contributing to the cftDNA pool released. It would be extremely interesting, in the future, to analyze tumor biopsies from these patients to confirm the proportion of mutKRAS.
The present study was aimed to explore whether early changes in cftDNA levels might be useful to monitor treatment response. We observed a trend towards better DCR in patients with early mutKRAS cftDNA decrease during treatment. Recently, an article on this topic has been published10, demonstrating that changes in cftDNA levels were related to the radiological response. However, our study has been conducted on a larger and more homogeneous cohort of patients, treated with improved first-line combination regimens, and investigated the role of early variations mutKRAS cftDNA, at variance with other publications in the field.
Under this point of view, future studies should focus on this issue also by comparing paired tumor biopsies and plasma from these patients, to confirm the correlation between mutKRAS cftDNA and treatment outcome. Indeed, the use of cftDNA approach and of a sensitive method, such as ddPCR, allow the detection of very small amounts of mutated clones in a large background of wild type DNA, minimizing the false negative data. In this context, monitoring the amount or the appearance of tumor molecular alterations (i.e. KRAS or other mutations like TP53, SMAD4) in cftDNA during treatment is a promising and reliable tool to monitor treatment resistance or response, as it reflects the tumor dynamics and tissue heterogeneity. In conclusion, although the present study examines a small cohort of patients, the results are in support of the hypothesis that cftDNA may be used as a new marker to monitor treatment outcome and disease progression in PDAC potentially earlier than radiological findings, suggesting that cftDNA mutKRAS changes are associated with tumor dynamics.
Patients and Methods
Patients
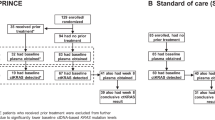
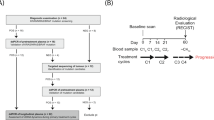
The study enrolled 27 consecutive patients with histologically proven advanced PDAC undergoing first-line chemotherapy with FOLFIRINOX or GEMnPAC as per standard practice. Patients were accrued from November 2015 to December 2016 at the Medical Oncology Unit of the University Hospital of Pisa. Treatment was administered until PD, unacceptable toxicity or patient refusal. Patients underwent standard disease evaluation by imaging according to RECIST 1.1 criteria: computed tomography (CT) of abdomen and chest was performed at baseline and every 8 weeks until PD. Disease control rate (DCR) was estimated as the percentage of patients who have achieved PR and SD during treatment. CA 19-9 was determined at every radiological evaluation. Data on PS, adverse events, serum chemistry, hematology and concomitant medications were collected at every chemotherapy cycle in a prospective database. Blood samples were drawn by venous puncture as follows: (1) baseline (immediately before chemotherapy administration); (2) after 15 days (before the second cycle of FOLFIRINOX or on day 15 of cycle 1 of GEMnPAC); and (3) at first radiological evaluation.
The study was approved by the Ethics Committee of Pisa University Hospital and conducted in accordance to the principles of the Declaration of Helsinki; all patients gave their signed informed consent before blood collection and cftDNA analysis.
Plasma collection, cftDNA extraction and KRAS analysis
Six ml of blood were collected in tubes containing EDTA and centrifuged at 3000 rpm for 10 min at 4 °C within 2 hours after blood drawing; plasma samples were stored at −80 °C until analysis. cftDNA was extracted using a QIAamp Circulating nucleic acid kit (Qiagen®, Valencia, CA, USA) from 3 ml of plasma following the manufacturer’s protocol and cftDNA was eluted with 50 μl of elution buffer.
The analysis was performed with a ddPCR KRAS Screening Multiplex Kit (BioRad®, Hercules, CA) and the results were confirmed using single mutation assays (BioRad®, Hercules, CA) to detect p.G12D, p.G12V, p.G12R, p.G13D. Based on the information reported in the technical annex, the MiQE Context Sequence is ATTATTTTTATTATAAGGCCTGCTGAAAATGACTGAATATAAACTTGTGGTAGTTGGAGCT[G/C]GTGGCGTAGGCAAGAGTGCCTTGACGATACAGCTAATTCAGAATCATTTTGTGGACGAATA (Entrez Gene ID 3845, RefSeq accessions NM_004985, NM_033360; Ensemble Accessions ENST00000311936, ENST00000256078, ENST00000556131, ENST00000557334).
Briefly, PCR reactions were assembled as per manufacturer instruction and the amplification protocol was standardized for all mutations to the following conditions: 95 °C × 10 min, 94 °C × 30 s and 55 °C × 60 s (35 cycles), 98 °C × 10 min, and 4 °C hold. As a positive control for mutKRAS, the cftDNA from 30 patients with known mutKRAS colorectal cancer was used, while the DNA extracted from plasma of 43 healthy blood donors was used as negative control. The droplet-reader was used for fluorescence signal quantification; the QuantaSoft (BioRad®, Hercules, CA) software measured the number of positive vs. negative droplets for both fluorophores (FAM/HEX) and their ratio was fitted to a Poisson distribution to determine the copy number/ml of the target molecule in the input reaction. A fluorescence intensity threshold of 3000 was set as a cut-off point and all droplets above this threshold were scored as positive for mutKRAS. The sample was considered as KRAS positive when at least 3 positive HEX droplets were identified above the threshold level.
Statistical analyses
OS was measured from the date of the first cycle of chemotherapy to death or last follow-up visit. PFS was measured from the date of the first cycle of chemotherapy to disease progression or death, whichever occurred first. PFS and OS were estimated using the Kaplan-Meier product-limit method. Shapiro-Wilk test was performed to verify normality of distributions of cftDNA mutKRAS variations; the latter were correlated with tumor response by Mann-Whitney test and Fisher’s exact test and with OS and PFS by log-rank test. Significance was set at p < 0.05 for two-tailed tests. Characteristics of patients, including and KRAS status and CA 19-9, were compared by the Fisher’s exact test. Univariate analysis was performed to correlate PFS and OS with demographics and clinical status of patients, i.e., ECOG PS, stage of disease, primary tumor location, chemotherapy regimen, site of disease, liver metastases, CA 19-9 levels and mutKRAS. Cut-off data of the analyses was January 2017. The cftDNA mutKRAS variation was evaluated both as a categorical variable (increase vs. no increase) and as a continuous variable considered as the percentage decreasing with respect to the baseline amount. Statistical analyses were carried out using the statistical software package SPSS 19.0 (SPSS, Chicago, IL, USA).
References
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2016. CA Cancer J Clin 66, 7–30, doi:10.3322/caac.21332 (2016).
Conroy, T. et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 364, 1817–1825, doi:10.1056/NEJMoa1011923 (2011).
Goldstein, D. et al. nab-Paclitaxel plus gemcitabine for metastatic pancreatic cancer: long-term survival from a phase III trial. J Natl Cancer Inst 107, doi:10.1093/jnci/dju413 (2015).
Duffy, M. J. et al. Tumor markers in pancreatic cancer: a European Group on Tumor Markers (EGTM) status report. Ann Oncol 21, 441–447, doi:10.1093/annonc/mdp332 (2010).
Rothenberg, M. L. et al. A rationale for expanding the endpoints for clinical trials in advanced pancreatic carcinoma. Cancer 78, 627–632, doi:10.1002/(SICI)1097-0142 (1996).
Ballehaninna, U. K. & Chamberlain, R. S. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J Gastrointest Oncol 3, 105–119, doi:10.3978/j.issn.2078-6891.2011.021 (2012).
Ballehaninna, U. K. & Chamberlain, R. S. Serum CA 19-9 as a Biomarker for Pancreatic Cancer-A Comprehensive Review. Indian J Surg Oncol 2, 88–100, doi:10.1007/s13193-011-0042-1 (2011).
Tjensvoll, K., Nordgard, O. & Smaaland, R. Circulating tumor cells in pancreatic cancer patients: methods of detection and clinical implications. Int J Cancer 134, 1–8, doi:10.1002/ijc.28134 (2014).
Hidalgo, M. Pancreatic cancer. N Engl J Med 362, 1605–1617, doi:10.1056/NEJMra0901557 (2010).
Tjensvoll, K. et al. Clinical relevance of circulating KRAS mutated DNA in plasma from patients with advanced pancreatic cancer. Mol Oncol 10, 635–643, doi:10.1016/j.molonc.2015.11.012 (2016).
Hadano, N. et al. Prognostic value of circulating tumour DNA in patients undergoing curative resection for pancreatic cancer. Br J Cancer 115, 59–65, doi:10.1038/bjc.2016.175 (2016).
Earl, J. et al. Circulating tumor cells (Ctc) and kras mutant circulating free Dna (cfdna) detection in peripheral blood as biomarkers in patients diagnosed with exocrine pancreatic cancer. BMC Cancer 15, 797, doi:10.1186/s12885-015-1779-7 (2015).
Kinugasa, H. et al. Detection of K-ras gene mutation by liquid biopsy in patients with pancreatic cancer. Cancer 121, 2271–2280, doi:10.1002/cncr.29364 (2015).
Imamura, T. et al. Liquid biopsy in patients with pancreatic cancer: Circulating tumor cells and cell-free nucleic acids. World J Gastroenterol 22, 5627–5641, doi:10.3748/wjg.v22.i25.5627 (2016).
Dabritz, J., Preston, R., Hanfler, J. & Oettle, H. K-ras mutations in the plasma correspond to computed tomographic findings in patients with pancreatic cancer. Pancreas 41, 323–325, doi:10.1097/MPA.0b013e3182289118 (2012).
Lebofsky, R. et al. Circulating tumor DNA as a non-invasive substitute to metastasis biopsy for tumor genotyping and personalized medicine in a prospective trial across all tumor types. Mol Oncol 9, 783–790, doi:10.1016/j.molonc.2014.12.003 (2015).
Castells, A. et al. K-ras mutations in DNA extracted from the plasma of patients with pancreatic carcinoma: diagnostic utility and prognostic significance. J Clin Oncol 17, 578–584, doi:10.1200/jco.1999.17.2.578 (1999).
Chen, H. et al. K-ras mutational status predicts poor prognosis in unresectable pancreatic cancer. Eur J Surg Oncol 36, 657–662, doi:10.1016/j.ejso.2010.05.014 (2010).
Marchese, R. et al. Low correspondence between K-ras mutations in pancreatic cancer tissue and detection of K-ras mutations in circulating DNA. Pancreas 32, 171–177, doi:10.1097/01.mpa.0000202938.63084.e3 (2006).
Maire, F. et al. Differential diagnosis between chronic pancreatitis and pancreatic cancer: value of the detection of KRAS2 mutations in circulating DNA. Br J Cancer 87, 551–554, doi:10.1038/sj.bjc.6600475 (2002).
Acknowledgements
The authors wish to thank Dr. Joanne Spataro for language revision. This work was funded by Fondazione Cassa Risparmio di Lucca, Lucca (Italy), Istituto Toscano Tumori, Firenze (Italy), and University of Pisa (Italy) to RD.
Author information
Authors and Affiliations
Contributions
Study concept and design: Del Re, Vivaldi. Acquisition of data: Del Re, Vivaldi, Rofi, Vasile, Fornaro, Caparello, d’Arienzo. Analysis and interpretation of data: Del Re, Vivaldi, Rofi, Danesi. Drafting of the manuscript: Del Re, Vivaldi, Rofi, Danesi. Critical revision of the manuscript for important intellectual content: Danesi, Falcone, Vasile, Fornaro. Statistical analysis: Del Re, Vivaldi, Miccoli. Obtaining funding: Danesi. Administrative, technical, or material support: Del Re, Vivaldi, Rofi. Supervision: Danesi, Falcone. Other (specify): None.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Del Re, M., Vivaldi, C., Rofi, E. et al. Early changes in plasma DNA levels of mutant KRAS as a sensitive marker of response to chemotherapy in pancreatic cancer. Sci Rep 7, 7931 (2017). https://doi.org/10.1038/s41598-017-08297-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-08297-z
- Springer Nature Limited
This article is cited by
-
High somatic mutations in circulating tumor DNA predict response of metastatic pancreatic ductal adenocarcinoma to first-line nab-paclitaxel plus S-1: prospective study
Journal of Translational Medicine (2024)
-
Circulating tumor DNA in molecular assessment feasibly predicts early progression of pancreatic cancer that cannot be identified via initial imaging
Scientific Reports (2023)
-
Prognostic value of circulating tumour DNA in metastatic pancreatic cancer patients: post-hoc analyses of two clinical trials
British Journal of Cancer (2022)
-
Current and Emerging Applications of Droplet Digital PCR in Oncology: An Updated Review
Molecular Diagnosis & Therapy (2022)
-
Prognostic Value of KRAS Mutations in the Peripheral Blood of Patients with Pancreatic Cancer: a Systematic Review and Meta-analysis
Indian Journal of Surgery (2022)