
Abstract
Mitochondria contain many copies of a circular DNA molecule (mtDNA), which has been observed as a mixture of normal and mutated states known as heteroplasmy. Elevated heteroplasmy at a single mtDNA site, m.3243A > G, leads to neurologic, sensory, movement, metabolic, and cardiopulmonary impairments. We measured leukocyte mtDNA m.3243A > G heteroplasmy in 789 elderly men and women from the bi-racial, population-based Health, Aging, and Body Composition Study to identify associations with age-related functioning and mortality. Mutation burden for the m.3243A > G ranged from 0–19% and elevated heteroplasmy was associated with reduced strength, cognitive, metabolic, and cardiovascular functioning. Risk of all-cause, dementia and stroke mortality was significantly elevated for participants in the highest tertiles of m.3243A > G heteroplasmy. These results indicate that the accumulation of a rare genetic disease mutation, m.3243A > G, manifests as several aging outcomes and that some diseases of aging may be attributed to the accumulation of mtDNA damage.
Similar content being viewed by others


Introduction
Within each mitochondrion there are thousands of maternally inherited circular mtDNA molecules coding for mitochondrial genes critical to oxidative phosphorylation (or OXPHOS). These populations of mtDNA molecules can contain either normal or mutated DNA in a mixture known as heteroplasmy1. Studies of elderly populations demonstrate an age-related increase in heteroplasmic load due to mtDNA mutations and rearrangements in post-mitotic tissues including: heart, central nervous system, brain and skeletal muscle2,3,4,5,6,7. An increased heteroplasmic load leads to reduced OXPHOS enzymatic activity and may be responsible for age-related functional decline3,4. The greatest impact of this bioenergetics defect has been shown in organs with high energy requirements such as skeletal muscle, retina, auditory neuroepithelia, brain and heart5,6,7,8,9.
Because mitochondrial function is cell-type specific, a single mtDNA mutation may lead to a variety of mitochondrial diseases, depending on the tissue in which the mutation is expressed10. Bioenergetic impairment of mitochondria through high heteroplasmic load (>80% burden of a pathogenic mtDNA mutation) may play a large role in disease initiation or progression11,12. We previously reported associations between elevated mtDNA heteroplasmy levels and reduced neurosensory and mobility function in older persons13. Average heteroplasmy levels among 20 candidate mutations detected in this earlier study of elderly participants ranged from 5–32%13.
Mitochondrial diseases resulting from mtDNA mutations often involve dysfunctions across multiple functional domains, including: neurologic, sensory, movement, metabolic, and cardiopulmonary outcomes14. Among the most thoroughly studied and best characterized of these pathogenic mutations is m.3243A > G, which causes several mitochondrial diseases and physiological dysfunctions, including: Mitochondrial Encephalopathy, Lactic Acidosis, Stroke-like episodes (MELAS), Mitochondrial Myopathy, Leigh syndrome, Chronic Progressive External Ophthalmoplegia (CPEO), Maternally Inherited Deafness and Diabetes (MIDD), hypertrophic cardiomyopathy (HCM), kidney dysfunction, migraine, bowel dysmotility, muscle stiffness, and diabetes14. Heterogeneity in the phenotypic expression related to m.3243A > G mutation ranges from mild to severe symptoms (e.g. mild deafness to stroke-like episodes)15,16.
To date, m.3243A > G heteroplasmy has not been examined for clinical associations in an aging population. In the current study we quantified m.3243A > G heteroplasmy in a community-based cohort of men and women over age 70 years old and tested associations with age-related functioning and mortality.
Results
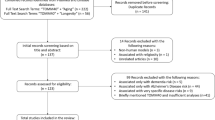
A total of 789 Health ABC participants of African and European ancestry yielded complete mtDNA sequences for analysis, analysis including 371 men and 418 women aged 74.1 (mean) ±2.9 (SD) years. Baseline values for measures of strength, movement, and cognitive, metabolic, and cardiovascular function are detailed in Table 1. Numbers for mortality events are also detailed in Table 1. Mean sequencing coverage for m.3243A > G was 961X with a lower limit of 82X. Heteroplasmy at m.3243A > G ranged from 0–19% with a mean (SD) of 5.55% (3.6) and a median of 5.11%. Heteroplasmy detected in this study is comparable to that from previous chip-17 and NGS-based18 platforms.
We identified statistically significant cross-sectional associations with one measurement from each of the subsets of 9 phenotypes examined (Table 2). The linear associations presented herein achieved nominal significance (p < 0.05): Digit Symbol Substitution Test (DSST) (p = 0.04), fasting insulin (p = 0.04), pulse wave velocity (PWV) (p = 0.008), and grip strength (p = 0.02). No statistically significant associations with other phenotypes examined in this study: 400 meter (m) walk (p = 0.94), Modified Mini-Mental State Examination (3MS) (p = 0.49), fasting glucose (p = 0.90), Systolic blood pressure (SBP) (p = 0.30), and resting heart rate (RHR) (p = 0.13).
We further examined tertiles of m.3243A > G heteroplasmy for associations with DSST score, fasting insulin levels, PWV, and grip strength, (Table 2 and Fig. 1). A total of 263 participants were in each tertile of m.3243A > G heteroplasmy (%) with the following values: low (0.0–≤4%), middle (>4–≤6%), and high (>6–≤19%). DSST score (p = 0.009) was significantly higher for participants in the lowest tertile when compared with those in the middle and high tertiles. Fasting insulin levels were significantly lower (p = 0.006) for participants in the lowest tertile when compared with those in the middle and highest tertiles. PWV was significantly lower (p = 0.032) for participants in the lowest tertile when compared with those in the highest tertile. Grip strength (p = 0.027) was significantly higher for participants in the lowest tertile when compared with those in the middle and high tertiles.

Mitochondrial m.3243A > G associations with digit symbol substitution test score (linear regression p = 0.04), fasting insulin (linear regression p = 0.04), pulse wave velocity (PWV, linear regression p = 0.008), and grip strength (linear regression p = 0.018) compared across tertiles of m.3243A > G heteroplasmy. A total of 263 participants were included in each tertile of m.3243A > G heteroplasmy. Bars indicate tertiles that were combined for analyses comparing phenotypes among low, middle, and high heteroplasmy levels. Asterisks (*) indicate statistically significant differences among individual and/or combined tertiles with p-values reported. Values and analyses adjusted for age, sex, race, and clinic site.
Significantly increased risks of mortality were observed for participants in the highest tertile of heteroplasmy when compared with those in the lowest tertile for all-cause (Hazard Ratio [HR] = 1.25, 95% confidence interval [CI] = 1.01–1.56, p = 0.046), dementia (HR = 1.96, 95% CI = 1.11–3.44, p = 0.02), and stroke (HR = 2.43, 95% CI = 1.00–5.97, p = 0.05) mortality (Table 3). Kaplan-Meier curves demonstrate the cumulative incidence of all-cause (Fig. 2), dementia (Fig. 3), and stroke (Fig. 4) mortality. No statistically significant associations with cardiovascular (p = 0.32) and cancer (p = 0.16) mortality were identified (Supplementary Figs 1, 2).

Mitochondrial m.3243A > G association with all-cause mortality. Survival was compared across tertiles of m.3243A > G heteroplasmy with a total of 263 participants included in each tertile. A significantly increased risk of all-cause mortality was observed for participants in the highest tertile of heteroplasmy when compared with those in the lowest tertile (Hazard Ratio [HR] = 1.25, 95% confidence interval [CI] = 1.01–1.56, p = 0.046). Analyses adjusted for age, sex, race, and clinic site.

Mitochondrial m.3243A > G association with dementia-related mortality. Survival was compared across tertiles of m.3243A > G heteroplasmy with a total of 263 participants included in each tertile. A significantly increased risk of dementia mortality was observed for participants in the highest tertile of heteroplasmy when compared with those in the lowest tertile (HR = 1.96, 95% CI = 1.11–3.44, p = 0.02). Analyses adjusted for age, sex, race, and clinic site.

Mitochondrial m.3243A > G association with stroke-related mortality. Survival was compared across tertiles of m.3243A > G heteroplasmy with a total of 263 participants included in each tertile. A significantly increased risk stroke mortality was observed for participants in the highest tertile of heteroplasmy when compared with those in the lowest tertile (HR = 2.43, 95% CI = 1.00–5.97, p = 0.05). Analyses adjusted for age, sex, race, and clinic site.
Discussion
Here we present novel findings on the role of sub-clinical levels of m.3243A > G heteroplasmy in an elderly population. Elevated m.3243A > G levels were associated with significantly impaired strength, cognition, cardiovascular, metabolic function, and mortality consistent with the diverse mitochondrial diseases and phenotypes typically associated with the m.3243A > G heteroplasmic load14,15,16,19,20. In the present study of non-disease presenting participants, circulating m.3243A > G heteroplasmy ranged from 0–19% with clear impairment at the highest tertiles.
In the context of mitochondrial diseases where the clinically relevant m.3243A > G mutation burden can reach levels over 90%, disease severity typically increases with elevated mutation burden21,22. Previous research has shown that m.3243A > G heteroplasmy levels of 10–30% are associated with type I and type II diabetes23 and autism24; heteroplasmy levels of 50–90% are associated with encephalomyopathies including MELAS25; and heteroplasmy levels of 90–100% lead to Leigh Syndrome or perinatal lethality21. In a large MELAS pedigree, 26 out of 27 living family members were m.3243A > G mutation positive26. Eighteen symptomatic m.3243A > G mutation carriers were identified without traditionally recognized stroke-like episodes but were diagnosed with diabetes, nephropathy, mild myopathy, cardiomyopathy, sensorineural hearing loss, cerebellar disease, and mental retardation. By contrast, eight m.3243A > G mutation carriers in this pedigree were asymptomatic demonstrating incomplete penetrance sometimes observed among mutation carriers. The clinical spectrum of heteroplasmic diseases has also been examined among twins both concordant and discordant for levels of mutation burden. Among monozygotic male twins carrying near-identical heteroplasmy levels of the pathogenic m.14487 T > C in different tissues, both were diagnosed with ptosis, optic atrophy, and myoclonic epilepsy27. By contrast, among monozygotic twins harboring a single large-scale mtDNA deletion, one brother harbored a high level of deleted mtDNA in muscle and exhibited ptosis, progressive external ophthalmoplegia, and proximal weakness while his twin brother had scarcely detectable deleted mtDNA molecules and was asymptomatic28. Among a set of dizygotic twins carrying the m.8344A > G mutation, one twin carried a high mutation load and was diagnosed with typical myoclonic epilepsy with ragged-red fibers (MERRF) while the other twin showed minimal mutation burden and was asymptomatic29.
Both in vitro and in vivo experiments have identified the molecular, structural, biochemical, and physiological impacts of m.3243A > G across the mutational spectrum and in multiple tissues. The m.3243A > G mutation located in the tRNAleu gene produces quantitative differences in processing and steady state amounts of the tRNAleu leading to amino acid misincorporation and impaired mitochondrial protein synthesis and assembly resulting in electron transport chain deficiency30,31,32. Biochemical studies of muscle in MELAS have also shown functional impairments of mtDNA-encoded complexes I, III, and IV33,34,35,36. In addition, widespread cellular dysfunction observed with elevated m.3243A > G mutation burden in MELAS impacts skeletal muscle, cerebral vasculature, and neuronal, endothelial, smooth muscle cells33,34,35,36,37,38. The consequences of the m.3243A > G mutation have been extensively examined using cytoplasmic hybrid (cybrid) models containing mtDNA from different sources placed in a uniform nuclear DNA background39 but have largely focused on on mtDNA sourced from clinically symptomatic MELAS patients carrying high m.3243A > G loads, > 90%21,30. However, MELAS patients often exhibit lower, tissue-specific m.3243A > G mutation loads40,41 and cybrids harboring ~20% m.3243A > G mutation loads exhibit reductions in cell surface area and elevated mtDNA density when compared with cybrids carrying only wild-type mtDNAs21. Respiratory chain dysfunction has also been reported in skeletal muscle42 and brain43 samples carrying m.3243A > G mutation levels under 10%.
A low-level of mtDNA heteroplasmy is commonly found in human populations1,13,17,44,45. Despite protective maternal mechanisms intended to minimize the transmission of mutated mtDNA46,47, heteroplasmy has been measured both in young children and during early adulthood. It remains uncertain whether the presence of heteroplasmy early in life is due to maternally transmitted mtDNA mutations1 or mutation acquisition during development44,48,49. Within the same individual, specific tissues may vary considerably with respect to their heteroplasmy and mutation loads45,50,51,52,53,54,55,56,57,58,59. Mutation load may accrue in post-mitotic tissues until a tissue-dependent threshold in the proportion of normal to mutated mtDNA is exceeded and the cells become bioenergetically deficient60. In general, mutation levels detected in blood are significantly lower than in other affected tissues including muscle, brain, liver, buccal mucosa, hair follicles, and urinary epithelium26,27,45,57,59,61. For example, similar levels of heteroplasmy were previously identified in two brain regions from the same individual while no heteroplasmy was detected in the blood59. Large studies examining mitochondrial genome-wide heteroplasmy across multiple tissues have demonstrated that heteroplasmy is extensive in nonsymptomatic subjects. For example, Naue et al.45 identified significant heteroplasmy in 88 out of 100 participants and detected the highest mutation levels in muscle and liver (69–79%), followed by brain, hair, and heart (30–37%), with the lowest levels in bone, blood, lung, and buccal cells (16–20%). Another study of 152 individuals examined heteroplasmy across twelve tissues obtained at autopsy and demonstrated that mutation burden at ten different mtDNA sites varied by tissue suggesting that both mutation- and tissue-driven processes have a role in driving mutation burden61. With regard to the m.3243A > G mutation, a study examining 61 individuals from 22 mutation-positive families demonstrated that mutation loads varied widely among five tissues57. Overall, urinary sediment exhibited the highest mutation burden followed by fibroblasts, cheek mucosa and hair roots, with blood showing the lowest proportion of mutant genomes57. The relationship between mtDNA mutation load and clinical phenotypes in humans has been a persistent subject for clinical diagnostics and recent studies have shown a superiority of urine epithelial cells over blood and muscle as a preferred non-invasive tissue for mtDNA mutation analysis50,51,52,53,57. The mechanisms responsible for inconsistent loading of mitochondrial heteroplasmy among specific cells44,48,49 and tissues is unknown; possibly genetic drift62 or selection against a particular mutation63,64 play significant roles. A better understanding of the mechanisms driving the expansion of mtDNA mutations and increased heteroplasmy load will further the development of interventions targeted to improved mitochondrial health65,66,67,68,69,70,71.
The current study has a number of strengths including the use of NGS sequencing and a platform designed specifically for complete mtDNA sequencing, and a large, community-based, well-characterized, biracial, longitudinal, cohort. Additionally, we were able to test our specific hypothesis that increased mtDNA heteroplasmy at the m.3234 > G mutation would be associated with impaired function across multiple phenotypes consistent with known mitochondrial disease impairments previously associated with this single mutation.
Although the rate of mitochondrial heteroplasmy accumulation is unknown in this population, we associated the measurements taken in the clinic with the mtDNA collected on a same-day visit thus ensuring that mortality was prospective and that the associations reported here are cross-sectional. Although the observed effect sizes for individual clinical measures associated with heteroplasmy are only moderately clinically significant, the ability to identify predictors of functional decline is critical to refining the associations between future disease onset and these clinical measures (e.g. of strength with disability or DSST with dementia). A limitation to this study is its absence of independent replication; the lack of associations for a number of phenotypes may be attributed to a limitation of sample size and tissue types (e.g. phenotypic examination may not have included all relevant tissues for mutation analysis). In order to confirm these findings, further population-level research including appropriate phenotypes, biospecimens, and design is necessary.
The Health ABC Study cohort is well-characterized and specifically designed for studies of aging-related impairments. Participants were generally healthy at the start of the study and it is likely that results from a single population may not be applied to all possible populations. These results indicate that the accumulation of a rare genetic disease mutation manifests as several aging outcomes and that some diseases of aging may be attributed to the accumulation of mtDNA damage. With further validation, measures of circulating mtDNA heteroplasmy may prove to be a valuable biomarker for identifying at-risk individuals who may benefit from early mitochondrial health interventions as well as for monitoring patients receiving mitochondrial therapies.
Methods
Participants
The Health, Aging, and Body Composition (Health ABC) Study is a prospective cohort of 3,075 community-dwelling men and women aged 70–79 years at recruitment in 1996–1997 and living in Memphis, TN, or Pittsburgh, PA. Participants were recruited within designated zip code areas from a random sample of white and black Medicare-eligible individuals. Participants had to be free of life-threatening cancer diagnoses and report no difficulty with the following activities of daily living: climbing 10 steps without resting or walking a quarter of a mile. Of the 3,075 participants, 51% were female and 41% were black. All participants signed written informed consents approved by the institutional review boards at the clinical sites (University of Tennessee Health Science Center, Memphis and University of Pittsburgh) and the coordinating center (University of California, San Francisco). All research and experimental protocols including participant recruitment, in-clinic assessments, blood collection and metabolic assays, and DNA sequencing were performed in accordance with relevant guidelines and regulations of the National Institute of Aging, the Health ABC Executive and Steering Committees, and the institutional review boards at the clinical sites (University of Tennessee Health Science Center, Memphis and University of Pittsburgh) and the coordinating center (University of California, San Francisco). All research and experimental protocols were also approved by the National Institute of Aging, the Health ABC Executive and Steering Committees, and the institutional review boards at the clinical sites (University of Tennessee Health Science Center, Memphis and University of Pittsburgh) and the coordinating center (University of California, San Francisco).
Mitochondrial DNA sequencing
A total of 794 Health ABC participants were identified for mtDNA sequencing. Genomic DNA was extracted from buffy coat collected using PUREGENE® DNA Purification Kit from samples collected at the baseline visit (1997–1998). The entire mtDNA was sequenced using the Ovation® Human Mitochondrion Target Enrichment System (NuGEN, San Carlos, CA) on the Illumina MiSeq NGS platform. Briefly, DNA samples are first fragmented and end-repaired.
Barcoded sequencing adaptors are next ligated to the 5′ ends of the fragmented DNA and samples are combined for probe annealing and extension. Target enrichment prior to sequencing is accomplished with probes designed to independently target each strand of the mtDNA resulting in an enriched mtDNA library. After NGS sequencing, the FASTQ files were aligned with BWA72 to the Revised Cambridge Reference Sequence (rCRS, NC_012920.1). From the resulting BAM-files73, the bases for position 3243 relative to the rCRS were extracted and only bases with a PHRED-score ≥ 30 and a mapping quality ≥30 were used for the heteroplasmy detection. Heteroplasmy was derived for each m.3243A > G allele by counting the number of reads for each of the ‘G’ minor allele (MA) and ‘A’ reference allele (RA) and calculated as MA/(MA + RA).
Strength and Mobility
Grip strength measured by handheld Jamar dynamometer74 and a timed walk of 400 meter (m) were assessed at the first clinical visit.
Cognitive Function Testing
Two cognitive function tests were assessed among participants at the baseline clinical visit: Digit Symbol Substitution Test (DSST) and Modified Mini-Mental State Examination (3MS). DSST measures executive cognitive function75,76 and is calculated as the total number of items correctly coded in 90 seconds. 3MS is a general cognitive battery77 with possible scores ranging from 0 to 100. Higher DSST and 3MS scores indicate better cognitive functioning.
Metabolic Measures
Fasting insulin and glucose were measured at the first clinical visit. Fasting insulin (uIU/mL) was measured via Microparticle Enzyme Immunoassay; Abbott Laboratories Diagnostics Division, South Pasadena, CA. Fasting glucose (mg/dL) was measured using Vitros Glucose; Johnson & Johnson; Rochester, NY USA.
Cardiovascular Measures
Systolic blood pressure (SBP), resting heart rate (RHR), and pulse wave velocity (PWV) were measured at the first clinical visit. Sitting SBP was computed as the average of 2 measurements in millimeters of mercury. RHR (beats/minute) was automatically measured using a 12‐lead electrocardiogram. PWV (cm/s), a measure of arterial stiffness, was assessed transcutaneous Doppler flow probes; Parks Medical Electronics, Aloha, OR.
Statistical analyses
Associations between m.3243A > G heteroplasmy and cognitive, movement and strength, cardiovascular, and metabolic function were examined using linear regression. Nominally significant linear associations (p < 0.05) among continuous predictor and outcome variables were further compared among tertiles of m.3243A > G heteroplasmy using ANOVA and general linear models were used to test differences among tertiles of heteroplasmy.
Vital status and cause of death were confirmed according to death certificates and hospital discharge summaries (when available) over an average of 12.7 years of follow-up. Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals [CIs] among tertiles of heteroplasmy for all-cause and cause-specific mortality. Kaplan-Meier curves were used to assess the cumulative incidence of all-cause and cause-specific mortality. All association and survival analyses were adjusted for age, sex, race, and clinic site using SAS version 9.4 (SAS Institute Inc, Cary, NC).
References
Payne, B. A. et al. Universal heteroplasmy of human mitochondrial DNA. Human molecular genetics 22, 384–390 (2013).
Linnane, A. W., Marzuki, S., Ozawa, T. & Tanaka, M. Mitochondrial DNA mutations as an important contributor to ageing and degenerative diseases. Lancet 1, 642–645 (1989).
Arnheim, N. & Cortopassi, G. Deleterious mitochondrial DNA mutations accumulate in aging human tissues. Mutation research 275, 157–167 (1992).
Trounce, I., Byrne, E. & Marzuki, S. Decline in skeletal muscle mitochondrial respiratory chain function: possible factor in ageing. Lancet 1, 637–639 (1989).
Tyrrell, D. J. et al. Respirometric Profiling of Muscle Mitochondria and Blood Cells Are Associated With Differences in Gait Speed Among Community-Dwelling Older Adults. The journals of gerontology. Series A, Biological sciences and medical sciences, https://doi.org/10.1093/gerona/glu096 (2014).
Figueiredo, P. A., Powers, S. K., Ferreira, R. M., Appell, H. J. & Duarte, J. A. Aging impairs skeletal muscle mitochondrial bioenergetic function. The journals of gerontology. Series A, Biological sciences and medical sciences 64, 21–33, https://doi.org/10.1093/gerona/gln048 (2009).
Menshikova, E. V. et al. Effects of exercise on mitochondrial content and function in aging human skeletal muscle. The journals of gerontology. Series A, Biological sciences and medical sciences 61, 534–540 (2006).
Van Remmen, H. & Jones, D. P. Current thoughts on the role of mitochondria and free radicals in the biology of aging. The journals of gerontology. Series A, Biological sciences and medical sciences 64, 171–174, https://doi.org/10.1093/gerona/gln058 (2009).
Horan, M. P., Pichaud, N. & Ballard, J. W. Review: quantifying mitochondrial dysfunction in complex diseases of aging. The journals of gerontology. Series A, Biological sciences and medical sciences 67, 1022–1035, https://doi.org/10.1093/gerona/glr263 (2012).
Naviaux, R. K. Mitochondrial DNA disorders. Eur J Pediatr 159(Suppl 3), S219–226 (2000).
Jeppesen, T. D., Schwartz, M., Olsen, D. B. & Vissing, J. Oxidative capacity correlates with muscle mutation load in mitochondrial myopathy. Annals of neurology 54, 86–92 (2003).
Rossignol, R., Malgat, M., Mazat, J. P. & Letellier, T. Threshold effect and tissue specificity. Implication for mitochondrial cytopathies. The. Journal of biological chemistry 274, 33426–33432 (1999).
Tranah, G. J. et al. Mitochondrial DNA Heteroplasmy Associations With Neurosensory and Mobility Function in Elderly Adults. The journals of gerontology. Series A, Biological sciences and medical sciences 70, 1418–1424, https://doi.org/10.1093/gerona/glv097 (2015).
Moraes, C. T. et al. Atypical clinical presentations associated with the MELAS mutation at position 3243 of human mitochondrial DNA. Neuromuscular disorders: NMD 3, 43–50 (1993).
Jean-Francois, M. J. et al. Heterogeneity in the phenotypic expression of the mutation in the mitochondrial tRNA(Leu) (UUR) gene generally associated with the MELAS subset of mitochondrial encephalomyopathies. Australian and New Zealand journal of medicine 24, 188–193 (1994).
Coon, K. D. et al. Quantitation of heteroplasmy of mtDNA sequence variants identified in a population of AD patients and controls by array-based resequencing. Mitochondrion 6, 194–210 (2006).
Ye, K., Lu, J., Ma, F., Keinan, A. & Gu, Z. Extensive pathogenicity of mitochondrial heteroplasmy in healthy human individuals. Proceedings of the National Academy of Sciences of the United States of America 111, 10654–10659, https://doi.org/10.1073/pnas.1403521111 (2014).
Wallace, D. C., Lott, M. T., Shoffner, J. M. & Brown, M. D. Diseases resulting from mitochondrial DNA point mutations. Journal of inherited metabolic disease 15, 472–479 (1992).
Martinuzzi, A. et al. Correlation between clinical and molecular features in two MELAS families. Journal of the neurological sciences 113, 222–229 (1992).
Picard, M. et al. Progressive increase in mtDNA 3243A > G heteroplasmy causes abrupt transcriptional reprogramming. Proceedings of the National Academy of Sciences of the United States of America, https://doi.org/10.1073/pnas.1414028111 (2014).
Hammans, S. R. et al. The mitochondrial DNA transfer RNALeu(UUR) A– > G(3243) mutation. A clinical and genetic study. Brain: a journal of neurology 118(Pt 3), 721–734 (1995).
van den Ouweland, J. M. et al. Mutation in mitochondrial tRNA(Leu)(UUR) gene in a large pedigree with maternally transmitted type II diabetes mellitus and deafness. Nature genetics 1, 368–371, https://doi.org/10.1038/ng0892-368 (1992).
Pons, R. et al. Mitochondrial DNA abnormalities and autistic spectrum disorders. The Journal of pediatrics 144, 81–85, https://doi.org/10.1016/j.jpeds.2003.10.023 (2004).
Goto, Y., Nonaka, I. & Horai, S. A mutation in the tRNA(Leu)(UUR) gene associated with the MELAS subgroup of mitochondrial encephalomyopathies. Nature 348, 651–653, https://doi.org/10.1038/348651a0 (1990).
Damian, M. S. et al. Clinical spectrum of the MELAS mutation in a large pedigree. Acta neurologica Scandinavica 92, 409–415 (1995).
Spyropoulos, A. et al. Near-identical segregation of mtDNA heteroplasmy in blood, muscle, urinary epithelium, and hair follicles in twins with optic atrophy, ptosis, and intractable epilepsy. JAMA neurology 70, 1552–1555, https://doi.org/10.1001/jamaneurol.2013.4111 (2013).
Blakely, E. L. et al. Mitochondrial DNA deletion in “identical” twin brothers. Journal of medical genetics 41, e19 (2004).
Penisson-Besnier, I. et al. Uneven distribution of mitochondrial DNA mutation in MERRF dizygotic twins. Journal of the neurological sciences 110, 144–148 (1992).
King, M. P., Koga, Y., Davidson, M. & Schon, E. A. Defects in mitochondrial protein synthesis and respiratory chain activity segregate with the tRNA(Leu(UUR)) mutation associated with mitochondrial myopathy, encephalopathy, lactic acidosis, and strokelike episodes. Molecular and cellular biology 12, 480–490 (1992).
Sasarman, F., Antonicka, H. & Shoubridge, E. A. The A3243G tRNALeu(UUR) MELAS mutation causes amino acid misincorporation and a combined respiratory chain assembly defect partially suppressed by overexpression of EFTu and EFG2. Human molecular genetics 17, 3697–3707, https://doi.org/10.1093/hmg/ddn265 (2008).
Yasukawa, T., Suzuki, T., Ueda, T., Ohta, S. & Watanabe, K. Modification defect at anticodon wobble nucleotide of mitochondrial tRNAs(Leu)(UUR) with pathogenic mutations of mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes. The Journal of biological chemistry 275, 4251–4257 (2000).
Koga, Y., Nonaka, I., Kobayashi, M., Tojyo, M. & Nihei, K. Findings in muscle in complex I (NADH coenzyme Q reductase) deficiency. Annals of neurology 24, 749–756, https://doi.org/10.1002/ana.410240609 (1988).
Goto, Y. et al. Mitochondrial myopathy, encephalopathy, lactic acidosis, and stroke-like episodes (MELAS): a correlative study of the clinical features and mitochondrial DNA mutation. Neurology 42, 545–550 (1992).
Ciafaloni, E. et al. MELAS: clinical features, biochemistry, and molecular genetics. Annals of neurology 31, 391–398, https://doi.org/10.1002/ana.410310408 (1992).
Fayet, G. et al. Ageing muscle: clonal expansions of mitochondrial DNA point mutations and deletions cause focal impairment of mitochondrial function. Neuromuscular disorders: NMD 12, 484–493 (2002).
Karppa, M., Mahjneh, I., Karttunen, A., Tolonen, U. & Majamaa, K. Muscle computed tomography patterns in patients with the mitochondrial DNA mutation 3243A > G. Journal of neurology 251, 556–563, https://doi.org/10.1007/s00415-004-0363-x (2004).
Gilchrist, J. M., Sikirica, M., Stopa, E. & Shanske, S. Adult-onset MELAS. Evidence for involvement of neurons as well as cerebral vasculature in strokelike episodes. Stroke; a journal of cerebral circulation 27, 1420–1423 (1996).
King, M. P. & Attardi, G. Human cells lacking mtDNA: repopulation with exogenous mitochondria by complementation. Science 246, 500–503 (1989).
Chinnery, P. F., Howell, N., Lightowlers, R. N. & Turnbull, D. M. Molecular pathology of MELAS and MERRF. The relationship between mutation load and clinical phenotypes. Brain: a journal of neurology 120(Pt10), 1713–1721 (1997).
van den Ouweland, J. M., Maechler, P., Wollheim, C. B., Attardi, G. & Maassen, J. A. Functional and morphological abnormalities of mitochondria harbouring the tRNA(Leu)(UUR) mutation in mitochondrial DNA derived from patients with maternally inherited diabetes and deafness (MIDD) and progressive kidney disease. Diabetologia 42, 485–492, https://doi.org/10.1007/s001250051183 (1999).
Chinnery, P. F. et al. Very low levels of the mtDNA A3243G mutation associated with mitochondrial dysfunction in vivo. Annals of neurology 47, 381–384 (2000).
Dubeau, F., De Stefano, N., Zifkin, B. G., Arnold, D. L. & Shoubridge, E. A. Oxidative phosphorylation defect in the brains of carriers of the tRNAleu(UUR) A3243G mutation in a MELAS pedigree. Annals of neurology 47, 179–185 (2000).
Khrapko, K., Nekhaeva, E., Kraytsberg, Y. & Kunz, W. Clonal expansions of mitochondrial genomes: implications for in vivo mutational spectra. Mutation research 522, 13–19 (2003).
Naue, J. et al. Evidence for frequent and tissue-specific sequence heteroplasmy in human mitochondrial DNA. Mitochondrion 20, 82–94, https://doi.org/10.1016/j.mito.2014.12.002 (2015).
Stewart, J. B. et al. Strong purifying selection in transmission of mammalian mitochondrial DNA. PLoS biology 6, e10 (2008).
Fan, W. et al. A mouse model of mitochondrial disease reveals germline selection against severe mtDNA mutations. Science 319, 958–962 (2008).
Ross, J. M. et al. Germline mitochondrial DNA mutations aggravate ageing and can impair brain development. Nature (2013).
Elson, J. L., Samuels, D. C., Turnbull, D. M. & Chinnery, P. F. Random intracellular drift explains the clonal expansion of mitochondrial DNA mutations with age. American journal of human genetics 68, 802–806 (2001).
Frederiksen, A. L. et al. Tissue specific distribution of the 3243A- > G mtDNA mutation. Journal of medical genetics 43, 671–677, https://doi.org/10.1136/jmg.2005.039339 (2006).
Ma, Y. et al. The study of mitochondrial A3243G mutation in different samples. Mitochondrion 9, 139–143, https://doi.org/10.1016/j.mito.2009.01.004 (2009).
Marotta, R. et al. Association of the MELAS m.3243A > G mutation with myositis and the superiority of urine over muscle, blood and hair for mutation detection. Journal of clinical neuroscience: official journal of the Neurosurgical Society of Australasia 16, 1223–1225, https://doi.org/10.1016/j.jocn.2008.11.012 (2009).
Whittaker, R. G. et al. Urine heteroplasmy is the best predictor of clinical outcome in the m.3243A > G mtDNA mutation. Neurology 72, 568–569, https://doi.org/10.1212/01.wnl.0000342121.91336.4d (2009).
McFarland, R. et al. De novo mutations in the mitochondrial ND3 gene as a cause of infantile mitochondrial encephalopathy and complex I deficiency. Annals of neurology 55, 58–64 (2004).
Crimi, M. et al. A new mitochondrial DNA mutation in ND3 gene causing severe Leigh syndrome with early lethality. Pediatr Res 55, 842–846 (2004).
Lebon, S. et al. Recurrent de novo mitochondrial DNA mutations in respiratory chain deficiency. Journal of medical genetics 40, 896–899 (2003).
Shanske, S. et al. Varying loads of the mitochondrial DNA A3243G mutation in different tissues: implications for diagnosis. American journal of medical genetics. Part A 130A, 134–137, https://doi.org/10.1002/ajmg.a.30220 (2004).
Kirches, E. et al. Heterogeneous tissue distribution of a mitochondrial DNA polymorphism in heteroplasmic subjects without mitochondrial disorders. Journal of medical genetics 38, 312–317 (2001).
Jazin, E. E., Cavelier, L., Eriksson, I., Oreland, L. & Gyllensten, U. Human brain contains high levels of heteroplasmy in the noncoding regions of mitochondrial DNA. Proceedings of the National Academy of Sciences of the United States of America 93, 12382–12387 (1996).
Ozawa, T. Mechanism of somatic mitochondrial DNA mutations associated with age and diseases. Biochimica et biophysica acta 1271, 177–189 (1995).
Li, M., Schroder, R., Ni, S., Madea, B. & Stoneking, M. Extensive tissue-related and allele-related mtDNA heteroplasmy suggests positive selection for somatic mutations. Proceedings of the National Academy of Sciences of the United States of America 112, 2491–2496, https://doi.org/10.1073/pnas.1419651112 (2015).
Chinnery, P. F. & Samuels, D. C. Relaxed replication of mtDNA: A model with implications for the expression of disease. American journal of human genetics 64, 1158–1165 (1999).
Pyle, A. et al. Depletion of mitochondrial DNA in leucocytes harbouring the 3243A- > G mtDNA mutation. Journal of medical genetics 44, 69–74 (2007).
Dai, Y. et al. Rapamycin drives selection against a pathogenic heteroplasmic mitochondrial DNA mutation. Human molecular genetics 23, 637–647 (2013).
Russell, O. & Turnbull, D. Mitochondrial DNA disease-molecular insights and potential routes to a cure. Exp Cell Res 325, 38–43, https://doi.org/10.1016/j.yexcr.2014.03.012 (2014).
Taylor, R. W., Chinnery, P. F., Turnbull, D. M. & Lightowlers, R. N. Selective inhibition of mutant human mitochondrial DNA replication in vitro by peptide nucleic acids. Nat Genet 15, 212–215, https://doi.org/10.1038/ng0297-212 (1997).
Minczuk, M., Papworth, M. A., Miller, J. C., Murphy, M. P. & Klug, A. Development of a single-chain, quasi-dimeric zinc-finger nuclease for the selective degradation of mutated human mitochondrial DNA. Nucleic Acids Res 36, 3926–3938, https://doi.org/10.1093/nar/gkn313 (2008).
Comte, C. et al. Mitochondrial targeting of recombinant RNAs modulates the level of a heteroplasmic mutation in human mitochondrial DNA associated with Kearns Sayre Syndrome. Nucleic Acids Res 41, 418–433, https://doi.org/10.1093/nar/gks965 (2013).
Boch, J. et al. Breaking the code of DNA binding specificity of TAL-type III effectors. Science 326, 1509–1512, https://doi.org/10.1126/science.1178811 (2009).
Hao, H., Morrison, L. E. & Moraes, C. T. Suppression of a mitochondrial tRNA gene mutation phenotype associated with changes in the nuclear background. Hum Mol Genet 8, 1117–1124 (1999).
Rorbach, J. et al. Overexpression of human mitochondrial valyl tRNA synthetase can partially restore levels of cognate mt-tRNAVal carrying the pathogenic C25U mutation. Nucleic Acids Res 36, 3065–3074, https://doi.org/10.1093/nar/gkn147 (2008).
Li, H. & Durbin, R. Fast and accurate long-read alignment with Burrows-Wheeler transform. Bioinformatics 26, 589–595, https://doi.org/10.1093/bioinformatics/btp698 (2010).
Li, H. et al. The Sequence Alignment/Map format and SAMtools. Bioinformatics 25, 2078–2079, https://doi.org/10.1093/bioinformatics/btp352 (2009).
Roberts, H. C. et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age and ageing 40, 423–429, https://doi.org/10.1093/ageing/afr051 (2011).
Wechsler, D. Wechsler Adult Intelligence Scale - Revised. San Antonio, Psychological Corporation (1981).
Beres, C. A. & Baron, A. Improved digit symbol substitution by older women as a result of extended practice. Journal of gerontology 36, 591–597 (1981).
Teng, E. L. & Chui, H. C. The Modified Mini-Mental State (3MS) examination. The Journal of clinical psychiatry 48, 314–318 (1987).
Acknowledgements
This research was supported in part by the Intramural Research Program of the NIH, National Institute on Aging, Contracts N01-AG-6-2101, N01-AG-6-2103, and N01-AG-6-2106; National Institutes of Health grants R01-AG028050, R03-AG032498, R01-NR012459, Z01A6000932, R01-HL121023. Foundation grants from the Research and Education Leadership Committee of the CPMC Foundation and the L. K. Whittier Foundation also supported this research. We are grateful to the Health, Aging and Body Composition Study participants and researchers.
Author information
Authors and Affiliations
Contributions
G.J.T. had full access to study data and takes responsibility for data integrity and accuracy of data analysis. conception and design G.J.T., K.Y., S.K., A.B.N., T.B.H., S.R.C.; collection of DNA sequence data K.L., G.J.T.; analysis and interpretation G.J.T., S.M.K., K.Y., S.K., A.B.N., T.B.H., S.R.C.; and drafting the manuscript for intellectual content G.J.T., S.M.K., T.M.M., S.K., A.B.N., T.B.H., S.R.C. All authors approved the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tranah, G.J., Katzman, S.M., Lauterjung, K. et al. Mitochondrial DNA m.3243A > G heteroplasmy affects multiple aging phenotypes and risk of mortality. Sci Rep 8, 11887 (2018). https://doi.org/10.1038/s41598-018-30255-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-30255-6
- Springer Nature Limited
This article is cited by
-
In utero particulate matter exposure in association with newborn mitochondrial ND4L10550A>G heteroplasmy and its role in overweight during early childhood
Environmental Health (2022)
-
Molecular damage in aging
Nature Aging (2021)
-
Distant hybrids of Heliocidaris crassispina (♀) and Strongylocentrotus intermedius (♂): identification and mtDNA heteroplasmy analysis
BMC Evolutionary Biology (2020)
-
New Frontiers in IVF: mtDNA and autologous germline mitochondrial energy transfer
Reproductive Biology and Endocrinology (2019)