
Abstract
Tidal volume at peak exercise and vital capacity ratio (VTpeak/VC) and VTpeak/inspiratory capacity (IC) were used to differentiate lung expansion in subjects with normal health and chronic obstructive pulmonary disease (COPD) from that in subjects with restrictive ventilation. However, VC and IC variably change due to pseudorestriction of lung volumes. Thus, these variables are currently not recommended. In contrast, total lung capacity (TLC) does little change during exercise. The aims of the study investigated whether VTpeak/TLC is more significantly correlated with static air trapping and lung hyperinflation in patients with COPD than VTpeak/IC, VTpeak/FVC, and VTpeak/SVC (study 1), and developed a marker to replace dynamic IC maneuvers by evaluation of the relationship between end-expiratory lung volume (EELV) and VTpeak/TLC and identification of a cutoff value for VTpeak/TLC (study 2). One hundred adults with COPD (study 1) and 23 with COPD and 19 controls (study 2) were analyzed. Spirometry, lung volume, diffusing capacity, incremental cardiopulmonary exercise tests with dynamic IC maneuvers were compared between groups. An ROC curve was generated to identify a cut off value for VTpeak/TLC. In study 1, VTpeak/TLC was more significantly associated with airflow obstruction, static air trapping and hyperinflation. In study 2, VTpeak/TLC was highly correlated with EELV in the patients (r = −0.83), and VTpeak/TLC ≥ 0.27 predicted that 18% of the patients with static air trapping and hyperinflation can expand their VT equivalent to the controls. In conclusions, VTpeak/TLC was superior to other VTpeak/capacities. VTpeak/TLC may be a marker of dynamic hyperinflation in subjects with COPD, thereby avoiding the need for dynamic IC maneuvers. VTpeak/TLC < 0.27 identified approximately 82% of subjects with COPD who could not adequately expand their tidal volume. As most of our participants were male, further studies are required to elucidate whether the results of this study can be applied to female patients with COPD.
Similar content being viewed by others

Introduction
In normal healthy subjects, tidal volume (VT) rapidly expands at the start of rapid incremental exercise and gradually reaches a plateau after reaching approximately 55% of vital capacity (VC)1. VT/VC and VT and inspiratory capacity ratio (VT/IC) have been reported to range from 0.55 ± 0.09 to 0.63 ± 0.19 and from ≤0.7 ± 0.11 to 0.79 ± 0.041,2,3,4,5,6, respectively. VT/IC values in subjects with restrictive ventilatory impairment usually reach 1, up to the limit of IC1.
Reduced dynamic inspiratory reserve volume (IRV) or O’Donnell’s threshold7 combined with elevated end-expiratory lung volume (EELV) can substantially constrain expansion of operating VT in patients with chronic obstructive pulmonary disease (COPD). Furthermore, VT/VC tends to be more variable because of variations in SVC and FVC in subjects with COPD due to pseudorestriction (i.e., low FVC%pred but normal total lung capacity, TLC). In this context, variations in operating VT at peak exercise and the “false” restriction of FVC (or SVC or IC) lead to inconsistent values of VT/FVC, VT/SVC, and VT/IC. Therefore, these variables are not recommended to differentiate obstructive from restrictive ventilatory limitations8.
Dynamic IC measurements have been reported to be a good way to identify dynamic hyperinflation2,3,4,5,7. However, IC maneuvers have to be standardized and the study subjects have to become familiarized with the maneuvers, and IC measurements and analysis also have to be standardized by researchers9. Nevertheless, dynamic IC measurements are not recommended for ramp-pattern protocols in which VT cannot steadily proceed to perform IC maneuvers9. However, the ramp-pattern protocol is a widely used protocol to test incremental exercise.
TLC does not change or only changes a little during exercise in normal subjects and subjects with lung diseases10,11,12. We hypothesized that VT/TLC at peak exercise (VTpeak/TLC) would be lower in subjects with COPD compared to normal subjects, and that it would be less variable than VTpeak/FVC, /SVC and /IC. As TLC and VTpeak are routinely measured during lung function tests and cardiopulmonary exercise tests (CPET), respectively, VTpeak/TLC may be a convenient new marker of dynamic hyperinflation, thereby avoiding the need for dynamic IC measurements.
The aims of this study were (1) to investigate whether VTpeak/TLC is less variable and more significant in correlation with static air trapping or lung hyperinflation in subjects with COPD than VTpeak/IC, /FVC, and /SVC, and (2) to develop a new marker of dynamic hyperinflation to replace dynamic IC maneuvers by evaluation of the relationship between EELV and VTpeak/TLC and identification of a cutoff value of VTpeak/TLC.
Methods
Study design
This observational cross-sectional study enrolled healthy normal subjects and subjects with COPD at two university teaching hospitals, and analyzed lung function and cardiopulmonary exercise data for aim 1 and aim 2. The Institutional Review Boards of Chung Shan Medical University Hospital (CS16174) and Chang Gung Memorial Hospital (201700899A3) approved this study, which was conducted in compliance with the Declaration of Helsinki.
Subjects
Subjects aged ≥40 years without any chronic diseases including uncontrolled diabetes mellitus, uncontrolled hypertension, anemia (hemoglobin <13 g·dL−1 in males and <12 g·dL−1 in females), and no acute illnesses in the recent 1 month were enrolled. Anthropometric measurements, leisure/sports activities, and cigarette smoking were recorded. Subjects with a body mass index ≤18 kg·m−2 or ≥32 kg·m−2 or with laboratory findings of cardiovascular, hematological, metabolic or neuromuscular diseases were excluded.
Study group
COPD was diagnosed according to the GOLD criteria13. Adult subjects who underwent lung function tests were enrolled only if their FEV1/FVC was <0.7 or the flow volume curve of spirometry revealed typical concavity13, and their forced expired volume in one second (FEV1)% predicted was <80% and had been stable for at least 1 month. A total of 131 subjects in the study group were screened, and 123 were retained for the study (Fig. 1). The reasons for exclusion included not meeting the inclusion criteria (n = 3), meeting the exclusion criteria (n = 2), and declining to participate (n = 2). The study group was divided into two cohorts, one for aim 1 and one for aim 2. To evaluate the bronchodilator effect on the relationship between VTpeak/TLC and static air trapping or lung hyperinflation, the subjects with COPD in study 1 were not allowed to use medications before measurements, whereas the subjects with COPD in study 2 were used medications as normal.

Flow diagram. A total of 131 subjects with chronic obstructive pulmonary disease were screened along with 20 normal healthy controls. After excluding eight subjects with COPD, the remaining 123 were allocated to study 1 (n = 100) and study 2 (n = 23). After excluding one subject, the remaining 19 normal subjects were allocated to study 2.
Control group
Healthy subjects without any of the aforementioned chronic diseases were screened. Twenty such subjects were screened, and 19 were enrolled (one subject did not meet the inclusion criteria) (Fig. 1). All eligible subjects were enrolled after signing informed consent forms.
Definitions
Static and dynamic air trapping and hyperinflation
Definitions of pulmonary hyperinflation and air trapping of the lung in the literature are inconsistent. In this study, static air trapping and hyperinflation were defined as RV/TLC > 0.4514,15, FRC%pred > 120%, or RV%pred > 120%; dynamic air trapping or hyperinflation was defined as VTpeak/TLC < 0.42,3,5.
Measurements
Pulmonary function testing
FEV1, TLC, RV, and diffusing capacity for carbon monoxide were measured using spirometry and body plethysmography (6200 Autobox DL, Yorba Linda, CA, USA or MasterScreen Body™, Carefusion, Wuerzburg, Germany) according to recommended standards16,17,18,19,20,21. VT/TLC, VT/SVC, VT/FVC, and VT/IC were derived when VT was obtained at peak exercise.
CPET
Each subject completed an incremental exercise test to the limit of the symptom (MasterScreen CPX™, Carefusion, Wuerzburg, Germany). Work rate was selected at a rate of 5–20 W/min based on a derived protocol formula according to the oxygen-cost diagram scores22. \(\dot{{\rm{V}}}\)O2 (mL/min), CO2 output (\(\dot{{\rm{V}}}\)CO2) (mL/min), and minute ventilation (\(\dot{{\rm{V}}}\)E) were continuously measured. \(\dot{{\rm{V}}}\)O2peak was symptom-limited and \(\dot{{\rm{V}}}\)O2peak predictions were performed as reported previously22. Cardiovascular stress level or exercise intensity was defined as heart rate at peak exercise/heart rate predicted maximum. The definition of ventilatory limitation was a breathing reserve of either <30% or <11–15 L/min23.
Dynamic inspiratory capacity measurement
The techniques used for performing and accepting IC measurements were as previously reported9. Dynamic IC was measured at the end of a steady-state resting baseline and unloaded cycling, and near the middle of loaded exercise and near end exercise. The middle of the loaded exercise was approximately 5–6 minutes after the start of loaded exercise, when dynamic IC near anaerobic threshold was measured. EELV was calculated as TLC minus dynamic IC. O’Donnell threshold was calculated as dynamic IC minus VT at peak exercise7.
Statistical analysis
Data were summarized as mean ± standard deviation and percentage and 5th and 95th percentiles. The Student’s t test was used for comparisons between two groups. Correlations were based on Pearson’s correlation coefficients. A p value < 0.05 was considered to be significant. An ROC curve was generated to identify a cut off value for VTpeak/TLC by comparisons with dynamic EELV at peak exercise. Statistical analyses were performed using SAS statistical software (SAS Institute Inc., Cary, NC, USA) and Origin v4.1 (Northampton, MA, USA). The sample size of study 2 was estimated to be 23 based on calculations with a 0.1 between-group difference and 0.1 of standard deviation for each group in VTpeak/TLC with a power of 0.9 and significance level of 0.05.
Results
One hundred subjects (97 men) with COPD in study 1 and 23 (23 men) with COPD and 19 healthy subjects (19 men) in study 2 were analyzed (Fig. 1 and Table 1). The majority of the subjects in study 1 had moderate airflow obstruction with hyperinflation and air trapping, and mild exercise hyperventilation and exercise ventilation limitation with mild exercise impairment (Tables 1 and 2). Compared to study 1, most of the subjects with COPD in study 2 had less severe airflow obstruction and hyperinflation and exercise impairment (Tables 1 and 2). VTpeak/TLC and VTpeak/SVC were significantly lower in the subjects in study 1 than in the COPD group in study 2, while VTpeak/FVC and VTpeak/IC were similar between the two COPD groups.
Correlation of VTpeak/TLC, /SVC, /FVC, and /IC with static air trapping and spirometry
VTpeak/TLC was 0.21 ± 0.06 (Table 2) and was most significantly correlated with air trapping or hyperinflation parameters and FEV1/FVC and FEV1%pred compared to the other three variables (Table 3, |r| = 0.45–0.62 vs. 0.001–0.49). Twelve of 99 (12%) subjects had a VTpeak/SVC > 0.63 (mean cut-off value of normal and COPD groups ≤0.631,4,5), 18 of 100 subjects had a VTpeak/FVC > 0.63, and 31 of 97 (32%) subjects had a VTpeak/IC > 0.79 (cut-off value: ≤0.791,2,3,5), while none of 97 subjects had a VTpeak/TLC > 0.4 (re-measured normal value: 0.4–0.422,3,5, Table 4) and only two (2%) had a VTpeak/TLC > 0.33 (Table 2, normal cut-off value in study 2).
Relationship between VTpeak/TLC and static air trapping and airflow obstruction
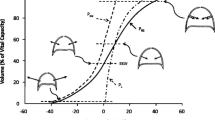
The normal subjects could expand VTpeak/TLC from 0.25 to 0.41 during incremental exercise (Fig. 2). The area under ROC curve was 0.861 and VTpeak/TLC of 0.27 had the highest sensitivity (88%) and specificity (77%) to predict elevated EELV. Nineteen of 112 (17%) subjects with FRC/TLC > 0.59 (Table 1, 95th percentile of the normal subjects in study 2) could expand their lungs to ≥ VTpeak/TLC of 0.27. Sixteen 13 of 97 (13%) subjects with RV/TLC > 0.48 (95th percentile of normal), 28of 119 (24%) subjects with FEV1%pred < 88% (5th percentile of normal), and 21 of 120 (18%) subjects with FEV1/FVC < 0.73 (5th percentile of normal) could expand their lungs to ≥VTpeak/TLC of 0.27.

Tidal volume at peak exercise (VTpeak) and total lung capacity (TLC) ratio as a function of air trapping, hyperinflation and airflow obstruction in the subjects with COPD (n = 97). The hatched areas represent the 5th and 95th percentiles of each corresponding variable of the normal subjects in study 2. The vertical and horizontal dashed lines represent the mean value of each corresponding variable of the normal subjects from the literature. Each symbol represents one subject.
Correlation of VTpeak/TLC and EELV or other variables
In study 2, the levels of EELV at rest, unloading exercise, and near anaerobic threshold and near peak exercise were significantly larger in the subjects with COPD than in the normal subjects (Table 2). VTpeak/TLC was significantly correlated with EELV/TLC in the subjects with COPD but not in the normal subjects (Fig. 3, r = −0.83, p < 0.0001 vs. r = −0.13, p = 0.36). VTpeak/TLC was also significantly correlated with \(\dot{{\rm{V}}}\)O2peak% (r = 0.73, p < 0.0001) in the COPD group but not in the normal group (r = 0.24, p = 0.33). However, VTpeak/TLC was not significantly correlated with Borg score (r = −0.03 vs. −0.03, both p = NS) or O’Donnell threshold (r = −0.43 vs. 0.2, both p = NS) in either groups.

End-expiratory lung volume and total lung capacity ratio (EELV/TLC) at rest, unloading, near anaerobic threshold, and near peak exercise as a function of tidal volume at peak exercise and TLC ratio (VTpeak/TLC) in 23 subjects with COPD and 19 normal subjects. The solid line represents the linear regression line (r = −0.83, p < 0.0001 for the COPD group and r = −0.13, p = 0.36 for the normal subjects) and the curved lines are the 95% CI lines.
Discussion
The key findings of this study were that VTpeak/TLC was the best marker for dynamic expandability of lungs compared to VTpeak/SVC, VTpeak/FVC, and VTpeak/IC in the subjects with COPD (Table 3, |r| = 0.45–0.62 vs. 0.001–0.49). These findings were noted in the subjects with COPD with or without withdrawal of bronchodilators before the test (Table 3 in study 2, |r| = 0.65–0.79 vs. 0.001–0.52). VTpeak/TLC was highly correlated with EELV in the subjects with COPD but not in the normal subjects (Fig. 3, r = −0.83 vs. −0.13). A VTpeak/TLC cutoff value of <0.27 further identified approximately 82% of the subjects with airflow obstruction and static air trapping or hyperinflation who developed dynamic air trapping during incremental exercise (Fig. 2). As VTpeak/TLC can easily be obtained without the need for any maneuvers during exercise, the need for dynamic IC maneuvers during exercise test may be avoided.
VTpeak/TLC, /SVC, /FVC, and /IC
VTpeak/SVC and /IC have been used to differentiate normal and obstructive ventilation from restrictive ventilation during CPET24,25. VTpeak/FVC has also been used as an alternative due to the ease of obtaining FVC. However, these variables are not recommended by the American Thoracic Society for such purposes8. In this study, VTpeak/SVC, /FVC, and /IC showed much higher variability than VTpeak/TLC in the correlation with static air trapping (Table 3). This may be because TLC changes little during exercise in normal subjects and those with airflow obstruction and interstitial lung disease10,11,12. As dynamic air trapping develops, VT is restricted and air cannot be removed sufficiently, thereby limiting the increase in VTpeak/TLC. In contrast, static SVC, FVC, and IC may be variable due to pseudorestriction of lung volume even in subjects with the same TLC, so that dynamic hyperinflation cannot be precisely predicted by VTpeak/SVC, /FVC, and /IC. Pseudorestriction is not uncommon in subjects with airflow obstruction, small airway obstruction and emphysema.
O’Donnell et al. reported that changes in dynamic IC were larger (−14%) during exercise in subjects with airflow obstruction than in normal subjects (4%, p < 0.0005)4, meaning that VTpeak/dynamic IC was larger than VTpeak/static IC (74% vs. 65%)4. However, in the current study, VTpeak/dynamic IC was smaller but not significantly smaller than VTpeak/static IC (71% vs. 77%) in the subjects with COPD, suggesting that dynamic IC was larger than static IC. This was also noted in the normal subjects in study 2 (i.e., 0.72 vs. 0.65; Table 2). This may be due to different severities of COPD in these two studies. In O’Donnell’s study4, the patients with COPD had 37%pred FEV1 in contrast to study 2 where the subjects with COPD had 55–68%pred FEV1.
VTpeak/TLC ratio and EELV or other variables
EELV is calculated as TLC minus dynamic IC. As TLC changes little during exercise10,11,12, changes in EELV must be inversely associated with changes in IC4. As mentioned, VTpeak/TLC changed in line with dynamic IC, and was thus inversely related to EELV (Fig. 4, r = −0.83, p < 0.0001). The area under ROC curve was high (0.861) and the sensitivity (88%) and specificity (77%) of VTpeak/TLC of 0.27 to predict elevated EELV in the current study were acceptable. The importance of VTpeak/TLC has not previously been addressed or reported, and our findings seem to suggest that VTpeak/TLC could be used as a substitute for dynamic IC maneuvers performed during exercise. One reason is that VTpeak/TLC is easily obtainable, and another is that in the ramp pattern exercise protocol but not a steady state protocol, dynamic IC maneuvers are not recommended9. Moreover, dynamic VT represents the difference between dynamic end-inspiratory lung volume (EILV) and EELV, and while measuring VTpeak/TLC is straightforward, measuring EILV and EELV is more complex5. Interestingly, in the current study VTpeak/TLC was correlated with \(\dot{{\rm{V}}}\)O2peak in the COPD group rather than in the normal group. This suggests that dynamic lung expansion played a role in the exercise capacity in patients with COPD but not in health. However, both groups reached a similar level of Borg dyspnea score (COPD vs. normal, 6 ± 3 vs. 6 ± 2, p = 0.83) but different levels of O’Donnell threshold/TLC (COPD vs. normal, 0.11 ± 0.07 vs. 0.19 ± 0.12, p = 0.02) at peak exercise. However, VTpeak/TLC was not correlated with either variable. We speculate that Borg dyspnea score and O’Donnell threshold are more related to the plateau portion of the pressure-volume curve for the lungs and chest wall whereas VTpeak/TLC involves lung volumes not only expanding to the plateau portion of the curve but also encroaching downward to expiratory reserve volume.
VTpeak/TLC ratio in this study and previous reports
Table 4 reveals that VTpeak/TLC was 0.21 ± 0.06–0.24 ± 0.07 in study 1 and 2, which is larger than in our previous report on patients with COPD (0.14–0.2)26 and reports on COPD from other researchers (0.15–0.24, the values were not reported in their studies but were re-calculated by the current authors)2,5,27,28. This may be due to differences in the severity of COPD and preconditioning strategy before the measurements in these studies. We re-measured VTpeak/TLC from the figures of the previous studies, and found values of 0.31–0.42 in patients with interstitial lung disease3,10 and 0.3–0.42 in normal healthy subjects2,3,5,28. In the normal subjects of this study, the VTpeak/TLC was 0.31 ± 0.06. However, it is difficult to compare this value between our study and studies in the literature as the level of VTpeak/TLC has not been reported.
Study limitations
The normal subjects had significant cigarette consumption despite having normal spirometry. In addition, subjects with restrictive ventilation were not included as interstitial lung disease is rare in our institutions. However, VTpeak/TLC in patients with interstitial lung disease as re-measured from the figures of previous studies was 0.31–0.422,3,10. These values are quite different from those reported in the subjects with COPD in this study and in the literature. The number of participants in study 2 was small and the findings may not be generalizable to all populations. However, the sample size of study 2 was estimated to be 23 based on standard calculations. The cohort was all men because the incidence of COPD in women is very low in Taiwan (37:1 in our previous report29). Dynamic IC measurements are recommended for subjects who can achieve a steady state of exercise. The exercise protocol in this study was the ramp pattern, and the relationship between VTpeak/TLC and EELV may be different between two-minute incremental and ramp-pattern exercise. However, it can be difficult to reach a steady state in each stage of exercise despite using the two-minute incremental exercise protocol2,3,4,5. Lastly, the subjects did not undergo pre-test exercise testing including dynamic IC maneuvers to allow them to become familiar with the whole protocol. However, this may more accurately reflect cardiopulmonary exercise testing in the real world.
Conclusion
VTpeak/TLC may be a potential marker of dynamic hyperinflation in subjects with COPD, and its use may avoid the need for dynamic IC maneuvers during incremental exercise. This marker is simple to derive and more stable than other VTpeak-capacity ratios regarding the relationship with static air trapping or hyperinflation, and it was significantly associated with EELV. A cut-off value of VTpeak/TLC < 0.27 identified approximately 82% of the subjects with COPD who had static hyperinflation and air trapping but could not expand their tidal volume to the same extent as the normal subjects. Further large-scale studies are warranted to investigate whether VTpeak/TLC can replace dynamic IC maneuver and whether it can be used to identify the VTpeak/TLC cut-off value. As most of our participants were male, further studies are required to elucidate whether the results of this study can be applied to female patients with COPD.
References
Wasserman, K., Hansen, J. E., Sue, D. Y, Stringer, W. W. & Whipp, B. J. Normal values in Principles of exercise testing and interpretation (ed. Wasserman, K.) (Lippicott Williams & Wilkins) (Philadelphia, 2005).
Faisal, A. et al. Common Mechanisms of Dyspnea in Chronic Interstitial and Obstructive Lung Disorders. Am. J. Respir. Crit. Care Med. 193, 299–309 (2016).
O’Donnell, D. E., Chau, L. K. & Webb, K. A. Qualitative aspects of exertional dyspnea in patients with interstitial lung disease. J. Appl. Physiol. 84, 2000–9 (1998).
O’Donnell, D. E., Revill, S. M. & Webb, K. A. Dynamic hyperinflation and exercise intolerance in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 164, 770–7 (2001).
O’Donnell, D. E. & Webb, K. A. Exertional breathlessness in patients with chronic airflow limitation. The role of lung hyperinflation. Am. Rev. Respir. Dis. 148, 1351–7 (1993).
Spiro, S. G., Dowdeswell, I. R. & Clark, T. J. An analysis of submaximal exercise responses in patients with sarcoidosis and fibrosing alveolitis. Br. J. Dis. Chest. 75, 169–80 (1981).
Casaburi, R. & Rennard, S. I. Exercise limitation in chronic obstructive pulmonary disease. The O’Donnell threshold. Am. J. Respir. Crit. Care Med. 191, 873–5 (2015).
The Committee. This Joint Statement of the ATS and the ACCP was adopted by the ATS Board of Directors, March 1, 2002 and by the ACCP Health Science Policy Committee, November 1, 2001. ATS/ACCP Statement on cardiopulmonary exercise testing. Am. J. Respir. Crit. Care Med. 167, 211–77 (2003).
Guenette, J. A., Chin, R. C., Cory, J. M., Webb, K. A. & O’Donnell, D. E. Inspiratory Capacity during Exercise: Measurement, Analysis, and Interpretation. Pulm. Med. 2013, 956081 (2013).
Marciniuk, D. D., Sridhar, G., Clemens, R. E., Zintel, T. A. & Gallagher, C. G. Lung volumes and expiratory flow limitation during exercise in interstitial lung disease. J. Appl. Physiol. 77, 263–73 (1994).
Stubbing, D. G., Pengelly, L. D., Morse, J. L. & Jones, N. L. Pulmonary mechanics during exercise in normal males. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 49, 506–510 (1980).
Stubbing, D. G., Pengelly, L. D., Morse, J. L. & Jones, N. L. Pulmonary mechanics during exercise in subjects with chronic airflow obstruction. J. Appl. Physiol. Respir. Environ. Exerc. Physiol. 49, 511–515 (1980).
GOLD Committees. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (revised 2015). Disclosure forms for GOLD Committees are posted on the GOLD Website, www.goldcopd.org (2017).
Ruppel, G. L. What is the clinical value of lung volumes? Respir. Care. 57, 26–35 (2012).
Stocks, J. & Quanjer, P. H. Reference values for residual volume, functional residual capacity and total lung capacity. Eur. Respir. J. 8, 492–506 (1995).
ATS/ERS S. ATS/ERS Statement on respiratory muscle testing. Am. J. Respir. Crit. Care Med. 166, 518–624 (2002).
GINA Committees. Global Initiative for Asthma (UPDATED 2017) Disclosure forms for GINA Committees are posted on the GINA Website, www.ginasthma.org, 1–156 (2017)
Macintyre, N. et al. Standardisation of the single-breath determination of carbon monoxide uptake in the lung. Eur. Respir. J. 26, 720–35 (2005).
Miller, M. R. et al. General considerations for lung function testing. Eur. Respir. J. 26, 153–61 (2005).
Miller, M. R. et al. Standardisation of spirometry. Eur Respir J. 26, 319–38 (2005).
Wanger, J. et al. Standardisation of the measurement of lung volumes. Eur. Respir. J. 26, 511–22 (2005).
Chuang, M. L., Lee, C. H. & Lin, I. F. Using the oxygen-cost diagram in ramp-slope selection for dyspneic patients. Intern. Med. 49, 1325–32 (2010).
McNicholl, D. M., Megarry, J., McGarvey, L. P., Riley, M. S. & Heaney, L. G. The utility of cardiopulmonary exercise testing in difficult asthma. Chest. 139, 1117–1123 (2011).
Wasserman, K., Hansen, J. E., Sue, D. Y., Casaburi, R. & Whipp, B. J. Normal Values in Principles of exercise testing and interpretation p.112–131 (ed. Wasserman, K.) (Lea & Febiger) (Philadelphia, 1994).
Wasserman, K., Hansen, J. E., Sue, D. Y., Casaburi, R. & Whipp, B. J. Measurements during integrative cardiopulmonary exercise testing in Principles of exercise testing and interpretation (ed. Wasserman, K.) (Lea & Febiger) (Philadelphia, 1994).
Chuang, M. L., Huang, S. F. & Su, C. H. Cardiovascular and respiratory dysfunction in chronic obstructive pulmonary disease complicated by impaired peripheral oxygenation. Int. J. Chron. Obstruct. Pulmon. Dis. 10, 329–337 (2015).
Ciavaglia, C. E. et al. Differences in respiratory muscle activity during cycling and walking do not influence dyspnea perception in obese patients with COPD. J. Appl. Physiol. 117, 1292–301 (2014).
Amann, M. et al. Impact of pulmonary system limitations on locomotor muscle fatigue in patients with COPD. Am. J. Physiol. Regul. Integr. Comp. Physiol. 299, R314–24 (2010).
Chuang, M. L. et al. Adjunctive Treatment with Rhodiola Crenulata in Patients with Chronic Obstructive Pulmonary Disease - A Randomized Placebo Controlled Double Blind Clinical Trial. PLoS One. 10, e0128142 (2015).
Acknowledgements
This study was supported by grants from the Ministry of Science and Technology, Taiwan (MOST 106-2314-B-040-025), the National Science Council, Taiwan (NSC92-2314-B-303-019), and the Chang Gung Medical Research Program (CMRP No. 443). The study was supported in part by Minister of Science and technology, Taiwan (MOST 106-2314-B-040-025).
Author information
Authors and Affiliations
Contributions
M.L.C. guarantor of the paper, initiated and designed the study, analyzed and interpreted the data, wrote the manuscript, and approved the version to be published. M.J.H. prepared and interpreted the data, reviewed the manuscript, and approved the version to be published. T.C.W. interpreted the data, reviewed the manuscript, and approved the version to be published. I.F.L. conducted statistical analysis, reviewed the manuscript, and approved the version to be published.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chuang, ML., Hsieh, MJ., Wu, TC. et al. Developing a New Marker of Dynamic Hyperinflation in Patients with Obstructive Airway Disease - an observational study. Sci Rep 9, 7514 (2019). https://doi.org/10.1038/s41598-019-43893-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-43893-1
- Springer Nature Limited