
Abstract
Infections caused by carbapenemase-producing, multidrug-resistant (MDR), or extensively drug-resistant (XDR) Gram-negative bacteria constitute a major therapeutic challenge. Whether combination antibiotic therapy is superior to monotherapy remains unknown. In this systematic review and meta-analysis OVID MEDLINE, EMBASE, PubMed, The Cochrane Library, and Scopus databases were searched for randomized controlled trials (RCTs) and observational studies published by December 2016 comparing mono- with combination antibiotic therapy for infections with carbapenemase-producing, MDR, or XDR Gram-negative bacteria. Mortality and clinical cure rates served as primary and secondary outcome measures, respectively. Of 8847 initially identified studies, 53 studies – covering pneumonia (n = 10 studies), blood stream (n = 15), osteoarticular (n = 1), and mixed infections (n = 27) - were included. 41% (n = 1848) of patients underwent monotherapy, and 59% (n = 2666) combination therapy. In case series/cohort studies (n = 45) mortality was lower with combination- vs. monotherapy (RR 0.83, CI 0.73–0.93, p = 0.002, I2 = 24%). Subgroup analysis revealed lower mortality with combination therapy with at least two in-vitro active antibiotics, in blood stream infections, and carbapenemase-producing Enterobacteriaceae. No mortality difference was seen in case-control studies (n = 6) and RCTs (n = 2). Cure rates did not differ regardless of study type. The two included RCTs had a high and unknown risk of bias, respectively. 16.7% (1/6) of case-control studies and 37.8% (17/45) of cases series/cohort studies were of good quality, whereas quality was poor in the remaining studies. In conclusion, combination antimicrobial therapy of multidrug-resistant Gram-negative bacteria appears to be superior to monotherapy with regard to mortality.
Similar content being viewed by others

Introduction
In an era of increasing antibiotic resistance rates, multidrug-resitant (MDR) Gram-negative bacteria constitute a major problem in the treatment of affected patients all over the world. The discovery void of new antibiotics, in particular antibiotics targeting Gram-negative bacteria, is further contributing to the problem and oftentimes necessitates the use of old drugs like polymyxins (colistin (polymyxin E) or polymyxin B), despite their well known and common serious side effects1. There is controversy on whether or not combination antimicrobial therapy is superior to monotherapy for infections with MDR pathogens. Many physicians prefer combination antimicrobial therapy over monotherapy, inferring superior outcomes mainly from in vitro experiments displaying synergistic effects of various antibiotics2. There are only few clinical studies comparing the effect of combination therapy versus monotherapy, most of them being retrospective cohort studies and case series limited by small study size. To account for the numerous confounding factors would require cohort studies including several hundreds to thousands of patients3. Furthermore, well-powered randomized controlled trials (RCTs) are lacking.
We conducted a systematic review and meta-analysis to investigate the effect of combination antimicrobial therapy versus monotherapy against multi-resistant Gram-negative bacteria on mortality as a primary outcome and cure rate as secondary outcome.
Methods
Data sources and searches
For this systematic review and meta-analysis, an electronic search of OVID MEDLINE, EMBASE, Scopus, The Cochrane Central Register of Controlled Trials (CENTRAL), and PubMed was performed with the help of a librarian with expertise in literature search for systematic reviews and meta-analyses. Studies published by December 2016 were included. For a detailed search strategy see Supplementary Materials (Supplementary Table 1).
Study selection
RCTs, case-control studies, cohort studies and case series comparing outcomes of antibiotic monotherapy versus combination therapy of infections caused by carbapenemase-producing, MDR, XDR and PDR Gram-negative bacteria were included. We retained the definition of MDR and XDR used by respective study authors. Studies including not only carbapenemase-producing, MDR, XDR or PDR Gram-negative bacteria were excluded unless outcome data of infections caused by carbapenemase-producing, MDR, XDR or PDR bacteria were reported separately. Moreover, studies with inclusion of bacteria with resistance mechanisms to carbapenems other than carbapenemase production, studies reporting on patients under the age of 16 years, case series lacking a comparison group or including fewer than ten patients were excluded. No restriction by study site, country, follow-up period, dose, or frequency of drug application was applied. Only studies addressing parenteral and oral drug administration were included; antibiotics that got applied by inhalation or topically were not considered. Only studies published in English were considered eligible.
Titles and abstracts were screened and inclusion criteria applied by one author (AS). Full text articles of potentially relevant publications were obtained and reviewed independently by two out of three authors (AS, AW, SK) who took the decision on final inclusion by consensus. In case no agreement could be reached, the third author was consulted and final unanimous decision was taken after an in-depth discussion.
Data extraction and quality assessment
Data extraction from included trials was performed by two of three authors (AS, AW, SK) using a standardized data collection form. In case of missing data, no attemps were made to contact study authors. Following data were extracted from studies: study design, microorganism and type of resistance, disease, antibiotics used in mono- and combination therapy and outcome measures. All-cause mortality and clinical cure rates, as defined in the individual studies, served as primary and secondary outcome measures, respectively. If the endpoints mortality or cure was only reported as probability, data were extracted as proportions.
In the monotherapy group, only patients treated with a single antibiotic drug were included, whereas in the combination therapy group patients treated with two or more antibiotics given simultaneously were included – regardless of in vitro susceptibility. Beta-lactamase inhibitors (i.e. sulbactam, clavulanic acid) were not considered independent antibiotic substances.
Quality assessment of RCTs with regard to method and risk of bias included: sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other sources of bias. Definitions/criteria were derived from the Cochrane Handbook for Systematic Reviews of Interventions4. Quality assessment and risk of bias of case-control studies comprised following criteria: selection, comparability, and exposure, according to the Newcastle-Ottawa quality assessment scale for case-control studies5. To assess quality and risk of bias of cohort studies, selection, comparability, and outcome was accounted for, using the Newcastle-Ottawa quality assessment scale for cohort studies5. Thresholds for converting the Newcastle-Ottawa scales to Agency for Healthcare Research and Quality (AHRQ) standards (good, fair and poor) were as follows: good quality if three or four stars in selection domain and one or two stars in comparability domain and two or three stars in outcome/exposure domain. Fair quality if two stars in selection domain and one or two stars in comparability domain and two or three stars in outcome/exposure domain. Poor quality if zero or one star in selection domain or zero stars in comparability domain or zero or one star in outcome/exposure domain6.
Data synthesis and analysis
For Data synthesis and analysis, Review Manager (Version 5.3, The Cochrane Collaboration, The Nordic Cochrane Centre, Copenhagen, Denmark) was used. Due to anticipated heterogeneity between studies, random effects models were used for all analyses to obtain a summary estimate (risk ratio (RR)) of the average effect with its 95% confidence interval (CI). P-values ≤ 0.05 were considered statistically significant. Subgroup analyses for various resistance mechanisms, disease entities, antibiotics and quality of studies were performed. Statistical heterogeneity was initially inspected graphically using forest plots. The degree of heterogeneity was quantified by using the I2 statistic with a threshold of I2 > 60% for high heterogeneity. Publication bias was investigated using a funnel plot in which the standard error of the effect estimate of each study was plotted against the estimate.
Results
Study selection
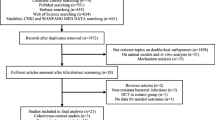
Figure 1 shows the study selection process according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses for Protocols (PRISMA). The initial search yielded 8847 references. After screening titles and abstracts and exclusion of duplicates, 182 articles were selected for full-text screening, after which 53 studies were retained for the analysis. Included studies are depicted in Supplementary Table 2. Addressed infections ranged from pneumonia (n = 10 studies)7,8,9,10,11,12,13,14,15,16, blood stream infections (n = 15 studies)17,18,19,20,21,22,23,24,25,26,27,28,29,30,31, osteoarticular infections (n = 1 study)32, and studies comprising mixed forms of infections (n = 27 studies)33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59. Two of the included studies were RCTs36,43, six case-control studies7,9,15,17,53,55 and forty-five case series/cohort studies8,10,11,12,13,14,16,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,37,38,39,40,41,42,44,45,46,47,48,49,50,51,52,54,56,57,58,59. The studies included a total of 4514 patients: 41% of patients (n = 1848) were treated with monotherapy, 59% (n = 2666) with combination therapy.

Study selection.
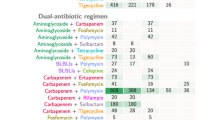
Monotherapies comprised colistin, polymyxin B, minocycline, doxyxycline, carbapenem, tigecycline, beta-lactam/beta-lactamase inhibitor, cephalosporin, aminoglycoside, fosfomycin, nitrofurantoin, and fluoroquinolone. Combination therapy comprised colistin-based combinations, polymyxin B-based combinations, minocycline-based combinations, carbapenem-based combinations, tigecyclin-based combinations, and various other combinations. The following resistant bacteria were addressed by the studies: MDR Pseudomonas aeruginosa, Metallo-Beta-lactamase-producing Pseudomonas aeruginosa, MDR/XDR and pan-drug resistant (PDR) Acinetobacter baumanii, carbapenemase-producing Enterobacteriaceae (incl. KPC), and mixed MDR/XDR Gram-negatives.
Mortality
All studies reporting on mortality totalled 2105 patients (56.3%) with combination therapy and 1633 patients (43.7%) with monotherapy.
Case series and cohort studies
Meta-analysis of all case series and cohort studies included 1813 patients (56.7%) with combination therapy and 1383 patients (43.3%) with monotherapy and demonstrated a lower mortality risk in the combination therapy group (RR: 0.83, 95% CI 0.73–0.93, p = 0.002). Heterogeneity was low (I2 = 24%, p = 0.1).
Subgroup analysis of various bacteria and resistance mechanisms indicated a superior outcome of combination therapy versus monotherapy in the treatment of infections caused by carbapenemase-producing Enterobacteriaceae (RR 0.74, 95% CI 0.59–0.93, p = 0.01; I2 = 26%, p = 0.17). In infections caused by other resistant bacteria, i.e. MDR Pseudomonas aeruginosa, Metallo-Beta-lactamase-producing Pseudomonas aeruginosa, MDR/XDR Acinetobacter baumanii and mixed MDR/XDR Gram negative bacteria, no difference in mortality was detected (Fig. 2).

Risk ratios for mortality rates of case series and cohort studies stratified by different bacteria. Data markers indicate Risk ratios and error bars indicate 95% CIs.
Subgroup analysis of various diseases revealed an advantage of combination therapy when applied in bloodstream infections (RR 0.78, 95% CI 0.63–0.96; p = 0.02; I2 = 27%, p = 0.17), whereas no difference could be seen in pneumonia or studies including mixed forms of infections. In studies that only included bloodstream infections (n = 14), stratified according to bacteria and resistance mechanism, combination therapy was superior in the group of carbapenemase-producing Enterobacteriaceae (RR: 0.61, CI 95% 0.45–0.85, p = 0.003; I2 = 21%, p = 0.26), with no difference in MDR/XDR Acinetobacter baumanii and mixed MDR/XDR Gram-negative bacteria (Supplementary Fig. 1). Subgroup analysis including only infections due to carbapenemase-producing Enterobacteriaceae, stratified by different disease types, again showed lower mortality rates in bloodstream infections (RR 0.61, CI 0.45–0.85, p = 0.003; I2 = 21%, p = 0.26) with no difference in the non-bloodstream infection group (comprising studies with mixed forms of infections) (Supplementary Fig. 2).
Subgroup analysis of different treatment strategies did not reveal a distinct combination therapy with a superior outcome compared to monotherapy. Analysis of the 12 studies with combination therapies that contained only one in-vitro active substance did not result in better outcomes against monotherapy, nor did subgroup analyses stratified according to bacteria and diseases. Polymyxin combinations performed better than polymyxin monotherapy (n = 1; RR 0.63, CI 95% 0.41–0.96, p = 0.03). Colistin combinations performed better than monotherapies with various antibiotics (n = 1; RR 0.38, CI 0.22–0.65, p = 0.0005).
Meta-analysis of studies with combination therapy including at least two in vitro active substances (n = 24) showed lower mortality with combination therapy versus monotherapy (RR 0.82, CI 0.73–0.93, p = 0.002, I2 = 3%, p = 0.41) (Fig. 3). Subgroup analysis in this group revealed better results with carbapenemase-producing Enterobacteriaceae (RR 0.73, CI 0.59–0.90, p = 0.003; I2 = 15%, p = 0.29) and bloodstream infections (RR 0.70, CI 0.53–0.91, p = 0.009; I2 = 25%, p = 0.22).

Risk ratios for mortality rates of case series and cohort studies stratified by different bacteria. Combination therapy with at least two in vitro active substances. Data markers indicate RRs and error bars indicate 95% CIs.
Subgroup analysis of good and poor quality studies revealed a significant lower mortality risk with combination antibiotic therapy versus monotherapy in good quality studies (RR: 0.78, 95% CI 0.69–0.88, p = 0.0001, I2 = 4%, p = 0.4). Among studies with poor quality, no difference in mortality in the combination therapy vs. the monotherapy group was detected. With regard to the different diseases, a significant difference of combination antibiotic therapy was seen in good quality studies of blood stream infections (RR: 0.75, 95% CI 0.61–0.93, p = 0.009, I2 = 17%, p = 0.3) and good quality studies of mixed infections (RR: 0.77, 95% CI 0.64–0.92, p = 0.004, I2 = 5%, p = 0.38), whereas no advantage of combination therapy could be shown in poor quality studies. Subgroup analysis of different bacteria and quality of studies revealed a significant lower mortality with combination therapy of carbapenemase-producing Enterobacteriaceae in good quality studies (RR: 0.71, 95% CI 0.60–0.84, p < 0.0001, I2 = 0%, p = 0.49) in contrast to poor quality studies.
Case-control studies
Meta-analysis of case-control studies comprising 142 patients (50.4%) with combination therapy and 140 patients (49.6%) with monotherapy did not show a significant difference in mortality between combination therapy and monotherapy. Neither did subgroup analyses of case-control studies comparing different bacteria/resistance mechanisms, diseases and treatments show a difference in mortality between the two groups. In all included case-control studies, either only one in vitro active substance was used in the combination group or it was not clearly stated whether there were several in-vitro active substances in the combination group.
The only study of good quality revealed a lower mortality of combination therapy (RR: 0.22, 95% CI 0.09–0.56, p = 0.001). Poor quality studies did not show any difference between combination therapy and monotherapy.
Randomized controlled trials
Meta-analysis of the two RCTs (150 patients with combination treatment, 110 patients with monotherapy) and various subgroup analyses did not show a beneficial effect of combination therapy over monotherapy. In the combination groups of the included RCTs, two or more in-vitro active substances were used.
Clinical cure rates
For meta-analysis of clinical cure rates, data from 1666 patients were available including case series, cohort and case-control studies. Among these, 1069 patients (64.2%) received combination therapy and 597 patients (35.8%) were treated with a monotherapy.
Case series and cohort studies
Meta-analysis of case series and cohort studies with a total of 958 patients (67.0%) with combination therapy and 472 patients (33.0%) with monotherapy, did not show a difference in clinical cure rates between mono- and combination therapy (Fig. 4).

Risk ratios for clinical cure rates of case series and cohort studies stratified by different bacteria. Data markers indicate Risk ratios and error bars indicate 95% CIs.
Subgroup analysis of different bacteria, resistance mechanisms and quality of studies did not reveal a difference between mono- and combination therapy. A trend to higher cure rates in combination therapy was seen in MDR Pseudomonas aeruginosa, MDR Acinetobacter baumanii and carbapenemase-producing Enterobacteriaceae.
Subgroup analysis of different diseases revealed a difference between mono- and combination therapy in osteoarticular infection (n = 1; RR 0.43, CI 0.21–0.89, p = 0.02) but no difference in other types of infections (pneumonia, bloodstream infections, mixed forms of infection).
No difference in cure rates was seen with different antibiotic therapies, regardless of the number of substances with in-vitro activity in combination treatment groups (Fig. 5).

Risk ratios for clinical cure rates of case series and cohort studies stratified by different bacteria. Combination therapy with at least two in vitro active substances. Data markers indicate Risk ratios and error bars indicate 95% CIs.
Case-control studies
Meta-analysis of case-control studies, including 125 patients (53.0%) with mono- and 111 patients (47.0%) with combination therapy, did not show any difference of monotherapy vs. combination therapy with regard to clinical cure rates. Subgroup analyses looking at different bacteria/resistance mechanisms, diseases (pneumonia, mixed) and treatments did not show any difference in clinical cure rates.
Study quality
The quality of included studies was variable. Two of the included studies were RCTs, one of which was un-blinded and the other one did not report on blinding leading to potential performance bias. One RCT showed an overall high risk of bias and the second one an overall unknown risk of bias (Supplementary Table 3). Only one out of six included case-control studies (16.7%) and 17 out of 45 (37.8%) included cases series and cohort studies showed an overall good quality with good comparability of cases and controls. The remaining studies were prone to confounding factors resulting in poor quality (Supplementary Table 4 and Supplementary Table 5). Funnel plots did not suggest publication bias (data not shown).
Discussion
In this large meta-analysis including 53 studies with a total of 4514 patients, overall mortality in case series and cohort studies was lower in patients treated with antibiotic combination therapy. Specifically, lower mortality rates were detected in patients with bloodstream infections and in infections caused by carbapenemase-producing Enterobacteriacae if combination therapy entailed at least two substances with in-vitro activity. There was no difference in mortality rates if combination therapy comprised only one in-vitro active substance, in RCTs (2 studies; several in-vitro active substances in combination therapy) and case-control studies (5 studies; only one in-vitro active substance in combination therapy). These effects were confirmed when restricting our analyses to studies of good quality.
Eight19,20,24,25,27,29,31 out of fourteen case series and cohort studies (57%) that included patients with bloodstream infections were due to carbapenemase-producing Enterobacteriaceae. These studies also accounted for 53% (8/15) of all included case series and cohort studies due to carbapenemase-producing Enterobacteriaceae. The mortality rate of patients with bloodstream infections with bacteria other than carbapenemase-producing Enterobacteriaceae did not differ between combination and monotherapy. Likewise, non-bloodstream infections by carbapenemase-producing Enterobacteriaceae did not show a superior effect of combination therapy. Thus, it is likely that the superior effect of combination therapy with infections caused by carbapenemase-producing Enterobacteriaceae and with bloodstream infections is actually one and the same.
Our results are in line with published results by Zusman et al.60, who showed lower mortality with polymyxin/carbapenem or polymyxin/tigecycline, aminoglycosides or fosfomycin combination therapy compared to polymyxin monotherapy in carbapenem-resistant bacteria and could also show a benefit of combined treatment in bloodstream infections. In contrast to our meta-analysis, Zusman et al. included carbapenem-resistant bacteria in general (i.e. also including carbapenem resistance due to porin loss), and regarded betalactamase inhibitors (i.e. sulbactam) as separate antibiotic substances. Furthermore, Zusman et al. only included carbapenem-resistant bacteria and only polymyxin mono- and combination therapy, whereas our analysis comprised different multiresistant bacteria and antimicrobials.
In theory, several facts argue against the application of combination therapy: the possible rise in resistance rates due to an overall increase in selection pressure as a result of a greater release of antibiotics into the environment61, higher rates of adverse effects (such as nephro- and ototoxicity due to colistin or aminoglycosides)61, an increase in Clostridium difficile-associated infections, fungal infections3, higher costs61, and possible antagonism3. On the other hand, several factors argue in favour of combination therapy: a broader antibiotic spectrum, in vitro data showing synergy of antibiotic combinations2, lower efficacy of colistin monotherapy compared to betalactam monotherapy62, lower risk of resistance development (e.g. against colistin)1, lower doses and shorter treatment duration61.
Observational study designs are prone to several limitations, mainly due to unmeasured confounding factors and other risks of bias. The likelihood of inappropriate empirical antibiotic therapy is higher in the monotherapy group and the time to start of appropriate monotherapy after results from susceptibilty testing are known may be longer compared to the combination therapy group, which may result in a bias in favour of combination therapy3. Information about the dosing of colistin was only reported in a minority of the included studies12,27,29,34. As guidance has changed in recent years and a loading dose is now generally recommended, colistin could have been underdosed in a significant proportion of studies, which may constitute a bias against colistin monotherapy3. Furthermore, there is a chance of selection bias in favour of combination therapy, as patients are more likely to receive colistin or tigecyclin monotherapy if bacteria are resistant to all other antibiotics as compared to situations where bacteria are still susceptible to carbapenems, for example, or in patients who suffer from polymicrobial infections with resistant as well as susceptible strains3. Such an effect could result in a perceived lower overall mortality in the combination treatment group at least partly due to a subgroup of carbapenem susceptible Gram-negative bacteria20,29,56. Moreover, combination therapy is more likely prescribed to patients with polymicrobial infections in which one does not know for sure whether the resistant bacterium is the main causative agent3. Against the latter argues the fact that an advantage of combination therapy could be shown in bloodstream infections, where one can almost be certain of the main causative agent, in analogy to Zusman and colleagues60. Finally, one could argue that combination therapy is more likely to be prescribed in more serious infections, which would bias the results in favour of monotherapy.
Due to numerous limitations and biases, which is reflected in the quality assessment of included studies, the results of this metaanalysis have to be interpreted with caution. However, by inclusion of a wide variety of cohort studies and case series, including a heterogeneous group of infectious diseases, bacteria, and treatments, we tried to minimize existing biases and limitations and allow for a valid comparison of combination treatment with monotherapy. Moreover, the favourable effect of combination therapy in bloodstream infections due to carbapenmase-producing Enterobacteriaceae has recently been confirmed in a large retrospective cohort for the subset of patients with severe infections63. With regard to RCTs and case-control studies, the validity of the results of our meta-analysis of RCTs and case-control studies is very limited due to the low number and limited power of the included studies.
To reach a final conclusion as to the possible advantage of combination therapy versus monotherapy, well designed and sufficiently powered RCTs are needed. Two RCT’s currently being undertaken could bring some more clarity in this contentious issue64,65. Such trials, however, will always have the problem to be prone to the conclusion that their findings can only be applied to the population under study. Only pragmatic trial designs will help resolve this issue. For the time being and taking into account limiting factors of RCTs, such as problems in reaching sufficient power in the setting of uncommon diseases as well as costs, other forms of study (cohort studies, case series, case-control studies) provide valid and valuable data on the best evidence-based treatment66. Individual patient-data meta-analyses may add further insights when it proves to be difficult to obtain large enough sample sizes for certain study questions.
Based on our results, combination therapy with two antimicrobials that demonstrate in vitro activity should be administered in patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae.
References
Falagas, M. E. & Kasiakou, S. K. Colistin: the revival of polymyxins for the management of multidrug-resistant gram-negative bacterial infections. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 40, 1333–1341, https://doi.org/10.1086/429323 (2005).
Zusman, O. et al. Systematic review and meta-analysis of in vitro synergy of polymyxins and carbapenems. Antimicrobial agents and chemotherapy 57, 5104–5111, https://doi.org/10.1128/aac.01230-13 (2013).
Paul, M. et al. Combination therapy for carbapenem-resistant Gram-negative bacteria. The Journal of antimicrobial chemotherapy 69, 2305–2309, https://doi.org/10.1093/jac/dku168 (2014).
Cochrane Collaboration Cochrane Handbook for Systematic Reviews of Interventions, http://handbook.cochrane.org/
Wells, G. E. A. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available at, http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. (2011).
https://www.ncbi.nlm.nih.gov/books/NBK115843/figure/appe.fm115843/?report=objectonly.
Furtado, G. H. et al. Intravenous polymyxin B for the treatment of nosocomial pneumonia caused by multidrug-resistant Pseudomonas aeruginosa. International journal of antimicrobial agents 30, 315–319, https://doi.org/10.1016/j.ijantimicag.2007.05.017 (2007).
He, H. et al. Tigecycline combination for ventilator-associated pneumonia caused by extensive drug-resistant Acinetobacter baumannii. Journal of thoracic disease 8, 2784–2792, https://doi.org/10.21037/jtd.2016.10.29 (2016).
Jean, S. S. et al. Comparison of the clinical efficacy between tigecycline plus extended-infusion imipenem and sulbactam plus imipenem against ventilator-associated pneumonia with pneumonic extensively drug-resistant Acinetobacter baumannii bacteremia, and correlation of clinical efficacy with in vitro synergy tests. Journal of microbiology, immunology, and infection = Wei mian yu gan ran za zhi 49, 924–933, https://doi.org/10.1016/j.jmii.2015.06.009 (2016).
Parchem, N. L. et al. Colistin combination therapy improves microbiologic cure in critically ill patients with multi-drug resistant gram-negative pneumonia. European journal of clinical microbiology & infectious diseases: official publication of the European Society of Clinical Microbiology 35, 1433–1439, https://doi.org/10.1007/s10096-016-2681-1 (2016).
Tasbakan, M. S. et al. Is tigecyclin a good choice in the treatment of multidrug-resistant Acinetobacter baumannii pneumonia? Journal of chemotherapy (Florence, Italy) 23, 345–349, https://doi.org/10.1179/joc.2011.23.6.345 (2011).
Tsioutis, C. et al. Clinical epidemiology, treatment and prognostic factors of extensively drug-resistant Acinetobacter baumannii ventilator-associated pneumonia in critically ill patients. International journal of antimicrobial agents 48, 492–497, https://doi.org/10.1016/j.ijantimicag.2016.07.007 (2016).
Wood, G. C., Hanes, S. D., Boucher, B. A., Croce, M. A. & Fabian, T. C. Tetracyclines for treating multidrug-resistant Acinetobacter baumannii ventilator-associated pneumonia. Intensive care medicine 29, 2072–2076, https://doi.org/10.1007/s00134-003-1811-2 (2003).
Ye, J. J. et al. The clinical implication and prognostic predictors of tigecycline treatment for pneumonia involving multidrug-resistant Acinetobacter baumannii. The Journal of infection 63, 351–361, https://doi.org/10.1016/j.jinf.2011.08.001 (2011).
Ye, J. J. et al. Tigecycline-based versus sulbactam-based treatment for pneumonia involving multidrug-resistant Acinetobacter calcoaceticus-Acinetobacter baumannii complex. BMC infectious diseases 16, 374, https://doi.org/10.1186/s12879-016-1717-6 (2016).
Yilmaz, G. R. et al. Colistin alone or combined with sulbactam or carbapenem against A. baumannii in ventilator-associated pneumonia. Journal of infection in developing countries 9, 476–485, https://doi.org/10.3855/jidc.6195 (2015).
Balkan, I. I. et al. Blood stream infections due to OXA-48-like carbapenemase-producing Enterobacteriaceae: treatment and survival. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases 26, 51–56, https://doi.org/10.1016/j.ijid.2014.05.012 (2014).
Batirel, A. et al. Comparison of colistin-carbapenem, colistin-sulbactam, and colistin plus other antibacterial agents for the treatment of extremely drug-resistant Acinetobacter baumannii bloodstream infections. European journal of clinical microbiology & infectious diseases: official publication of the European Society of Clinical Microbiology 33, 1311–1322, https://doi.org/10.1007/s10096-014-2070-6 (2014).
Daikos, G. L. et al. Prospective observational study of the impact of VIM-1 metallo-beta-lactamase on the outcome of patients with Klebsiella pneumoniae bloodstream infections. Antimicrobial agents and chemotherapy 53, 1868–1873, https://doi.org/10.1128/aac.00782-08 (2009).
Daikos, G. L. et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections: lowering mortality by antibiotic combination schemes and the role of carbapenems. Antimicrobial agents and chemotherapy 58, 2322–2328, https://doi.org/10.1128/aac.02166-13 (2014).
Freire, M. P. et al. Bloodstream infection caused by extensively drug-resistant Acinetobacter baumannii in cancer patients: high mortality associated with delayed treatment rather than with the degree of neutropenia. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases 22, 352–358, https://doi.org/10.1016/j.cmi.2015.12.010 (2016).
Kuo, L. C. et al. Multidrug-resistant Acinetobacter baumannii bacteraemia: clinical features, antimicrobial therapy and outcome. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases 13, 196–198, https://doi.org/10.1111/j.1469-0691.2006.01601.x (2007).
Lim, S. K. et al. The outcomes of using colistin for treating multidrug resistant Acinetobacter species bloodstream infections. Journal of Korean medical science 26, 325–331, https://doi.org/10.3346/jkms.2011.26.3.325 (2011).
Navarro-San Francisco, C. et al. Bacteraemia due to OXA-48-carbapenemase-producing Enterobacteriaceae: a major clinical challenge. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases 19, E72–79, https://doi.org/10.1111/1469-0691.12091 (2013).
Papadimitriou-Olivgeris, M. et al. Risk factors for infection and predictors of mortality among patients with KPC-producing Klebsiella pneumoniae bloodstream infections in the intensive care unit. Scandinavian journal of infectious diseases 46, 642–648, https://doi.org/10.3109/00365548.2014.923106 (2014).
Qureshi, Z. A. et al. Treatment outcome of bacteremia due to KPC-producing Klebsiella pneumoniae: superiority of combination antimicrobial regimens. Antimicrobial agents and chemotherapy 56, 2108–2113, https://doi.org/10.1128/aac.06268-11 (2012).
Tofas, P. et al. Carbapenemase-producing Klebsiella pneumoniae bloodstream infections in neutropenic patients with haematological malignancies or aplastic anaemia: Analysis of 50 cases. International journal of antimicrobial agents 47, 335–339, https://doi.org/10.1016/j.ijantimicag.2016.01.011 (2016).
Tseng, Y. C. et al. Prognosis of adult patients with bacteremia caused by extensively resistant Acinetobacter baumannii. Diagnostic microbiology and infectious disease 59, 181–190, https://doi.org/10.1016/j.diagmicrobio.2007.04.024 (2007).
Tumbarello, M. et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: importance of combination therapy. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 55, 943–950, https://doi.org/10.1093/cid/cis588 (2012).
Wang, W. et al. Predictors of mortality in bloodstream infections caused by multidrug-resistant gram-negative bacteria: 4 years of collection. American journal of infection control 45, 59–64, https://doi.org/10.1016/j.ajic.2016.08.008 (2017).
Zarkotou, O. et al. Predictors of mortality in patients with bloodstream infections caused by KPC-producing Klebsiella pneumoniae and impact of appropriate antimicrobial treatment. Clinical microbiology and infection: the official publication of the European Society of Clinical Microbiology and Infectious Diseases 17, 1798–1803, https://doi.org/10.1111/j.1469-0691.2011.03514.x (2011).
Ribera, A. et al. Osteoarticular infection caused by MDR Pseudomonas aeruginosa: the benefits of combination therapy with colistin plus beta-lactams. The Journal of antimicrobial chemotherapy 70, 3357–3365, https://doi.org/10.1093/jac/dkv281 (2015).
Bergamasco, M. D. et al. Infection with Klebsiella pneumoniae carbapenemase (KPC)-producing K. pneumoniae in solid organ transplantation. Transplant infectious disease: an official journal of the Transplantation Society 14, 198–205, https://doi.org/10.1111/j.1399-3062.2011.00688.x (2012).
Cai, B. et al. Clinical Efficacy of Polymyxin Monotherapy versus Nonvalidated Polymyxin Combination Therapy versus Validated Polymyxin Combination Therapy in Extensively Drug-Resistant Gram-Negative Bacillus Infections. Antimicrobial agents and chemotherapy 60, 4013–4022, https://doi.org/10.1128/aac.03064-15 (2016).
Cetin, C. B., Ozer Turk, D., Senol, S., Dinc Horasan, G. & Tunger, O. Colistin efficacy in the treatment of multidrug-resistant and extremelydrug-resistant gram-negative bacterial infections. Turkish journal of medical sciences 46, 1379–1384, https://doi.org/10.3906/sag-1506-125 (2016).
Durante-Mangoni, E. et al. Colistin and rifampicin compared with colistin alone for the treatment of serious infections due to extensively drug-resistant Acinetobacter baumannii: a multicenter, randomized clinical trial. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 57, 349–358, https://doi.org/10.1093/cid/cit253 (2013).
Falagas, M. E., Kasiakou, S. K., Kofteridis, D. P., Roditakis, G. & Samonis, G. Effectiveness and nephrotoxicity of intravenous colistin for treatment of patients with infections due to polymyxin-only-susceptible (POS) gram-negative bacteria. European journal of clinical microbiology & infectious diseases: official publication of the European Society of Clinical Microbiology 25, 596–599, https://doi.org/10.1007/s10096-006-0191-2 (2006).
Falagas, M. E. et al. Colistin therapy for microbiologically documented multidrug-resistant Gram-negative bacterial infections: a retrospective cohort study of 258 patients. International journal of antimicrobial agents 35, 194–199, https://doi.org/10.1016/j.ijantimicag.2009.10.005 (2010).
Goff, D. A., Bauer, K. A. & Mangino, J. E. Bad bugs need old drugs: a stewardship program’s evaluation of minocycline for multidrug-resistant Acinetobacter baumannii infections. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 59(Suppl 6), S381–387, https://doi.org/10.1093/cid/ciu593 (2014).
Gonzalez-Padilla, M. et al. Gentamicin therapy for sepsis due to carbapenem-resistant and colistin-resistant Klebsiella pneumoniae. The Journal of antimicrobial chemotherapy 70, 905–913, https://doi.org/10.1093/jac/dku432 (2015).
Hachem, R. Y. et al. Colistin is effective in treatment of infections caused by multidrug-resistant Pseudomonas aeruginosa in cancer patients. Antimicrobial agents and chemotherapy 51, 1905–1911, https://doi.org/10.1128/aac.01015-06 (2007).
Hernandez-Torres, A. et al. Multidrug and carbapenem-resistant Acinetobacter baumannii infections: Factors associated with mortality. Medicina clinica 138, 650–655, https://doi.org/10.1016/j.medcli.2011.06.024 (2012).
Ji, S. et al. Cefepime combined with amoxicillin/clavulanic acid: a new choice for the KPC-producing K. pneumoniae infection. International journal of infectious diseases: IJID: official publication of the International Society for Infectious Diseases 38, 108–114, https://doi.org/10.1016/j.ijid.2015.07.024 (2015).
Katsiari, M. et al. Carbapenem-resistant Klebsiella pneumoniae infections in a Greek intensive care unit: Molecular characterisation and treatment challenges. Journal of global antimicrobial resistance 3, 123–127, https://doi.org/10.1016/j.jgar.2015.01.006 (2015).
Lee, C. M., Lim, H. K., Liu, C. P. & Tseng, H. K. Treatment of pan-drug resistant Acinetobacter baumannii. Scandinavian journal of infectious diseases 37, 195–199, https://doi.org/10.1080/00365540510026869 (2005).
Linden, P. K. et al. Use of parenteral colistin for the treatment of serious infection due to antimicrobial-resistant Pseudomonas aeruginosa. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 37, e154–160, https://doi.org/10.1086/379611 (2003).
Lopez-Cortes, L. E. et al. Monotherapy versus combination therapy for sepsis due to multidrug-resistant Acinetobacter baumannii: analysis of a multicentre prospective cohort. The Journal of antimicrobial chemotherapy 69, 3119–3126, https://doi.org/10.1093/jac/dku233 (2014).
Rigatto, M. H. et al. Polymyxin B in Combination with Antimicrobials Lacking In Vitro Activity versus Polymyxin B in Monotherapy in Critically Ill Patients with Acinetobacter baumannii or Pseudomonas aeruginosa Infections. Antimicrobial agents and chemotherapy 59, 6575–6580, https://doi.org/10.1128/aac.00494-15 (2015).
Rihani, D. S. et al. Over-treatment of carbapenemase-producing Enterobacteriaceae. Scandinavian journal of infectious diseases 44, 325–329, https://doi.org/10.3109/00365548.2011.638318 (2012).
Sanchez-Romero, I. et al. Nosocomial outbreak of VIM-1-producing Klebsiella pneumoniae isolates of multilocus sequence type 15: molecular basis, clinical risk factors, and outcome. Antimicrobial agents and chemotherapy 56, 420–427, https://doi.org/10.1128/aac.05036-11 (2012).
Schafer, J. J., Goff, D. A., Stevenson, K. B. & Mangino, J. E. Early experience with tigecycline for ventilator-associated pneumonia and bacteremia caused by multidrug-resistant Acinetobacter baumannii. Pharmacotherapy 27, 980–987, https://doi.org/10.1592/phco.27.7.980 (2007).
Shields, R. K. et al. Epidemiology, clinical characteristics and outcomes of extensively drug-resistant Acinetobacter baumannii infections among solid organ transplant recipients. PloS one 7, e52349, https://doi.org/10.1371/journal.pone.0052349 (2012).
Simsek, F. et al. Colistin against colistin-only-susceptible Acinetobacter baumannii-related infections: Monotherapy or combination therapy? Indian journal of medical microbiology 30, 448–452, https://doi.org/10.4103/0255-0857.103767 (2012).
Souli, M. et al. Clinical experience of serious infections caused by Enterobacteriaceae producing VIM-1 metallo-beta-lactamase in a Greek University Hospital. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 46, 847–854, https://doi.org/10.1086/528719 (2008).
Torres-Gonzalez, P. et al. Associated factors and outcomes for OXA-232 Carbapenem-resistant Enterobacteriaceae infections in a tertiary care centre in Mexico City: A case-control-control study. Diagnostic microbiology and infectious disease 86, 243–248, https://doi.org/10.1016/j.diagmicrobio.2016.07.002 (2016).
Tumbarello, M. et al. Infections caused by KPC-producing Klebsiella pneumoniae: differences in therapy and mortality in a multicentre study. The Journal of antimicrobial chemotherapy 70, 2133–2143, https://doi.org/10.1093/jac/dkv086 (2015).
Vergara-Lopez, S., Dominguez, M. C., Conejo, M. C., Pascual, A. & Rodriguez-Bano, J. Lessons from an outbreak of metallo-beta-lactamase-producing Klebsiella oxytoca in an intensive care unit: the importance of time at risk and combination therapy. The Journal of hospital infection 89, 123–131, https://doi.org/10.1016/j.jhin.2013.12.008 (2015).
Wu, M. T. et al. Clinical evaluation of tigecycline in the treatment of nosocomial infection in a hospital in Taiwan. International journal of clinical pharmacology and therapeutics 52, 1030–1036, https://doi.org/10.5414/cp202220 (2014).
Zavascki, A. P. et al. The influence of metallo-beta-lactamase production on mortality in nosocomial Pseudomonas aeruginosa infections. The Journal of antimicrobial chemotherapy 58, 387–392, https://doi.org/10.1093/jac/dkl239 (2006).
Zusman, O. et al. Polymyxin monotherapy or in combination against carbapenem-resistant bacteria: systematic review and meta-analysis. The Journal of antimicrobial chemotherapy 72, 29–39, https://doi.org/10.1093/jac/dkw377 (2017).
Tamma, P. D., Cosgrove, S. E. & Maragakis, L. L. Combination therapy for treatment of infections with gram-negative bacteria. Clinical microbiology reviews 25, 450–470, https://doi.org/10.1128/cmr.05041-11 (2012).
Paul, M. et al. Effectiveness and safety of colistin: prospective comparative cohort study. The Journal of antimicrobial chemotherapy 65, 1019–1027, https://doi.org/10.1093/jac/dkq069 (2010).
Gutierrez-Gutierrez, B. et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae (INCREMENT): a retrospective cohort study. The Lancet. Infectious diseases 17, 726–734, https://doi.org/10.1016/s1473-3099(17)30228-1 (2017).
Anon. Trial for the Treatment of Extensively Drug-Resistant Gram-negative Bacilli, https://clinicaltrials.gov/ct2/show/NCT01597973.
Anon. Multicenter Open-label Randomized Controlled Trial (RCT) to Compare Colistin Alone Versus Colistin Plus Meropenem, https://clinicaltrials.gov/ct2/show/NCT01732250.
Frieden, T. R. Evidence for Health Decision Making - Beyond Randomized, Controlled Trials. The New England journal of medicine 377, 465–475, https://doi.org/10.1056/NEJMra1614394 (2017).
Author information
Authors and Affiliations
Contributions
Contributions to the conception or design of the work: A.S., J.N. and S.P.K. Acquisition, analysis, or interpretation of data: A.S., A.W., P.W.S., J.N., H.S. and S.P.K. Drafted the work or substantively revised it: A.S., A.W., P.W.S., J.N., H.S. and S.P.K.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schmid, A., Wolfensberger, A., Nemeth, J. et al. Monotherapy versus combination therapy for multidrug-resistant Gram-negative infections: Systematic Review and Meta-Analysis. Sci Rep 9, 15290 (2019). https://doi.org/10.1038/s41598-019-51711-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-51711-x
- Springer Nature Limited
This article is cited by
-
The impact of colistin-based regimens on mortality compared to other antimicrobials in patients with carbapenem-resistant Enterobacterales bacteremia in South African hospitals: a cross-sectional study
BMC Infectious Diseases (2024)
-
Green synthesis of zinc oxide nanoparticles (ZnO-NPs) by Streptomyces baarnensis and its active metabolite (Ka): a promising combination against multidrug-resistant ESKAPE pathogens and cytotoxicity
BMC Microbiology (2024)
-
Optimal effective concentration combinations (OPECCs) for binary application of membrane-targeting antiseptics and TMPyP-mediated antimicrobial photodynamic therapy
Photochemical & Photobiological Sciences (2024)
-
Key summary of German national guideline for adult patients with nosocomial pneumonia- Update 2024 Funding number at the Federal Joint Committee (G-BA): 01VSF22007
Infection (2024)
-
Impact of macrolide treatment on long-term mortality in patients admitted to the ICU due to CAP: a targeted maximum likelihood estimation and survival analysis
Critical Care (2023)