
Abstract
Patients with simple snoring (SS) often complain of poor sleep quality despite a normal apnoea-hypopnoea index (AHI). We aimed to identify the difference in power spectral density of electroencephalography (EEG) between patients with SS and those with obstructive sleep apnoea (OSA). We compared the absolute power spectral density values of standard EEG frequency bands between the SS (n = 42) and OSA (n = 129) groups during the non-rapid eye movement (NREM) sleep period, after controlling for age and sex. We also analysed partial correlation between AHI and the absolute values of the EEG frequency bands. The absolute power spectral density values in the beta and delta bands were higher in the OSA group than in the SS group. AHI also positively correlated with beta power in the OSA group as well as in the combined group (OSA + SS). In conclusion, higher delta and beta power during NREM sleep were found in the OSA group than in the SS group, and beta power was correlated with AHI. These findings are microstructural characteristics of sleep-related breathing disorders.
Similar content being viewed by others

Introduction
Obstructive sleep apnoea (OSA) is the most prevalent manifestation of sleep disordered breathing (SDB) characterised by repeated episodes of complete or partial collapse of upper airway during sleep1. Clinical manifestation of OSA includes snoring, disturbed sleep, fatigue, daytime sleepiness, loss of concentration, memory decline, and neuropsychiatric symptoms2,3,4,5. OSA is diagnosed using overnight polysomnography (PSG) when the apnoea or hypopnoea occurs five or more times per hour (apnoea-hypopnoea index [AHI] ≥ 5)6. In the spectrum of SDB, snorers with AHI < 5 are defined as having simple snoring (SS), which has less pathological and clinical significance7,8,9.
SS is a preclinical condition that requires no treatment. However, patients with SS may suffer from daytime sleepiness, insomnia, and psychiatric symptoms despite a normal AHI10,11. Although SS is differentiated from OSA by AHI on PSG, there is a weak association between AHI and symptomatology in SDB12,13,14,15,16,17,18. Some studies reported that patients with SS have more severe psychiatric symptoms and poorer subjective sleep quality than those with OSA12,19. This paradoxical association between AHI, subjective sleep quality, and psychiatric symptoms suggests that other factors besides AHI influence such symptoms, and it may be necessary to study differences in microstructure in addition to classical PSG measurements (e.g., sleep stage ratio or sleep efficiency) and macrostructures.
Researchers have previously attempted to investigate the microstructure of PSG-derived sleep as well as waking quantitative electroencephalography (qEEG) in SDB20,21,22,23,24. It has been generally accepted that wake EEG slowing is more pronounced in patients with OSA than in good sleepers, and the slowing is associated with daytime sleepiness and attention or vigilance dysfunction25,26,27,28,29,30,31. Studies using sleep EEG derived from PSG have documented significant differences in spectral power or sleep spindles during non-rapid eye movement (NREM) sleep between patients with OSA and controls32,33,34,35. Although previous spectral analysis studies have investigated EEG and oximetric spectral features to improve OSA detection21, little is known about differences in sleep qEEG between patients with SS and those with OSA.
Our goal was to study differences in qEEG between SS and OSA to understand the association between qEEG and AHI in SDB. The aims of this study were 1) to compare the power spectral density of qEEG frequency bands during NREM sleep between the SS and OSA groups and 2) to investigate the correlation between AHI and qEEG power in patients with SDB.
Results
Demographic and PSG characteristics of participants
Among the 171 participants, 129 (75.4%) were classified into the OSA group and 42 (24.6%) were classified into the SS group. Demographic and PSG characteristics of participants are presented in Table 1. There were no significant differences between the groups in terms of age and sex. As expected, the groups differed in body mass index (BMI), AHI, and arousal index and all values were higher in the OSA group than in the SS group. PSG data differed in the ratio of sleep stages N1 and N2 but did not differ in most other PSG measures (the ratio of stage N3 and REM and all sleep and wake time data, including total sleep time and sleep efficiency) between the groups.
Comparison of absolute spectral EEG power between groups
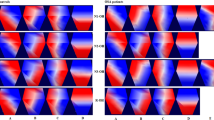
Table 2 and Fig. 1 provide the comparison of the absolute spectral power in central electrodes during NREM sleep between the SS and OSA groups. There were significant differences in the spectral power in the delta and beta frequency bands between the groups after controlling for age and sex. The absolute spectral power in the delta (1–4 Hz, F = 10.54, p = 0.001, p corrected = 0.006) and beta (15–20 Hz, F = 7.64, p = 0.006, p corrected = 0.036) bands during NREM sleep was higher in the OSA group than in the SS group. Comparative results during N2, N3 and REM sleep are presented in Table S1 in the supplementary information.

Comparisons of the absolute power spectral density during NREM sleep between the SS and OSA groups. *p < 0.05 in ANCOVA controlling for age and sex after Bonferroni correction (uncorrected p value × 6) for correction of multiple comparisons. Bars denote mean ± standard deviation. NREM, non-rapid eye movement; SS, simple snoring; OSA, obstructive sleep apnoea; ANCOVA, analysis of covariance.
Table 3 presents results for comparisons of the absolute spectral power in central electrodes among SS, mild OSA (5 ≤ AHI < 15), moderate OSA (15 ≤ AHI < 30), and severe OSA (30 ≤ AHI) groups to reveal differences in the EEG power according to the severity of AHI. There were significant differences in the spectral power of the beta frequency bands between the groups after controlling for age and sex. The absolute spectral power of the beta (F = 4.41, p = 0.005, p corrected = 0.031) band during NREM sleep was higher in the severe OSA group than in the SS group following post-hoc analysis.
Partial correlation analyses between AHI, arousal index and absolute power spectral density
Table 4 presents partial correlation analyses results between AHI and absolute power spectral density after controlling for age and sex in the SS, OSA, and total participants. AHI positively correlated with absolute beta power in the OSA group (r = 0.251, p = 0.004, p corrected = 0.027; Fig. 2a) and total participants (SS + OSA; r = 0.340, p < 0.001, p corrected <0.001; Fig. 2b).

Partial correlations between AHI and absolute beta power during NREM sleep. (a) Partial correlation between AHI and absolute beta power during NREM period controlling for age and sex in the OSA group (r = 0.251, p corr = 0.027). (b) Partial correlation between AHI and absolute beta power during NREM period controlling for age and sex in total participants (r = 0.340, p corr <0.001). AHI, apnoea-hypopnea index; NREM, non-rapid eye movement; OSA, obstructive sleep apnoea; r, Pearson’s r; Log transformation for spectral EEG was performed before Pearson correlation analysis when both variables deviate from the normal distribution. p corr, p value after Bonferroni correction (uncorrected p value × 6) for correction of multiple comparisons.
Table S2 in supplementary information presents partial correlation analyses results between the arousal index and absolute power spectral density after controlling for age and sex in the SS, OSA and total participants. The arousal index positively correlated with absolute beta power in all participants (SS + OSA; r = 0.282, p < 0.001, p corrected <0.001; Fig. S1).
Discussion
We conducted spectral power analysis of sleep EEG derived from PSG in patients with suspected OSA. The major finding of the present study is the spectral power difference in the delta and beta frequency bands of sleep EEG between the SS and OSA groups (Table 2). We found increased delta and beta activity36 in the OSA group compared to the SS group. In addition, the beta power positively correlated with AHI in the OSA group and total participants.
We attribute this seemingly paradoxical result—an increase in delta activity, which predominates in slow wave sleep, in patients with higher AHI—as (1) a compensatory EEG slowing response to arousal or (2) precedence of slow waves over respiratory arousal in patients with OSA. Studies on the hypothesis of compensatory EEG slowing response have been previously published37,38. Previous studies reported that the delta band amplitude increased in patients with OSA starting few seconds after apnoea onset during NREM sleep38. Another study reported that consecutive respiratory events restoring process was related to higher spectral power of the delta band37. These findings may implicate that the slowing of EEG in OSA and slow waves, including the delta band, play a role in recovery from altered respiration and complement arousal event during sleep. On the other hand, there is an opinion that the increase of delta is not compensating for arousal due to respiratory disturbance, but more hypopnea related arousal response occurs after slow wave sleep in OSA patients. Previous studies have shown that arousals in NREM sleep were consistently preceded by increase in the transient delta power in both normal and pathological NREM sleep39.
The lower delta power in the SS group than in the OSA group may be the underlying cause of subjective symptoms in patients with SS or subjective-objective mismatch in sleep perception in SDB, as shown in previous studies10,11,12,13. In other words, reduced delta power in the SS group may induce poor sleep perception and eventually develop poor psychiatric symptoms. Although the severity of SDB continuum is defined as mild form of SS to severe form of OSA9, a weak or no relationship between AHI and accompanying psychiatric symptoms, such as depression and anxiety, has been reported16. We also found increased psychiatric symptoms12 and perception of nocturnal SDB symptoms40 in the SS group compared to those in the OSA group. Bianchi et al. reported subjective-objective mismatch in sleep perception in patients with sleep apnoea and insomnia and concluded that mismatch was not attributable to commonly measured PSG measures and that further insight into the advanced signal processing technique would help explain this mismatch41. Thus, further elaborate investigations into the relationship among sleep EEG spectral power, sleep perception, and psychiatric symptoms in SDB would be necessary.
We found higher beta power in the OSA group than in the SS group (Table 2) and the absolute beta power density positively correlated with the AHI and arousal index in all participants (Table 4 and Table S2). Beta band is associated with emotional and cognitive processes and arousal during sleep42 and is enhanced during the N1 and N2 sleep stages and decreased during deeper sleep36. Higher beta power in patients with OSA in our study can be explained by the higher background brain activity in patients with OSA than in those with SS. This study also showed a significant correlation between the arousal index and beta power, which means sleep disturbance of SDB. Positive correlation between beta power in NREM sleep and AHI is consistent with recent data24. Our result replicated this data and had the same association in the suspected OSA (SS + OSA groups). In addition, we believed that the increase in both beta and delta powers during NREM sleep in the OSA group was due to cyclic alternating patterns, which are considered to be indicators of arousal instability43. The A phase in the cyclic alternating patterns was reported to be associated with increase in beta power and preceding delta power39. Our results exhibiting positive correlation between beta power and the arousal index in NREM sleep may also support this cyclic alternating pattern.
Our study was limited by the small sample size of the SS group. Further, the sample sizes between the SS and OSA groups were unequal owing to the clinical characteristics of the participants. However, as this is the largest investigation of spectral power comparison between the SS and OSA groups to date, this study is meaningful. Future studies with a larger sample size are needed involving patients with SS and OSA as well as normal controls.
Conclusions
In summary, we found that qEEG spectral power in the delta and beta bands of NREM sleep differ between the SS and OSA groups. The higher delta and beta power were found in the OSA group than SS group and beta power was correlated with AHI in combined group. This study reports differences in microstructures of PSG-derived sleep EEG between SS and OSA and how these differences in microstructures may reveal areas that were not previously explained by macrostructure and traditional parameters in PSG. The current finding of the increased delta power in the OSA group might explain previous reports on the lack of an association between the AHI and subjective symptoms in patients with SDB10,11,12,13. Future investigations need to focus on the characterisation of features of SDB in both conventional and microstructural aspects of PSG in order to clarify the neural mechanism of SDB and explain clinical phenomena not explained by conventional PSG.
Methods
Participants
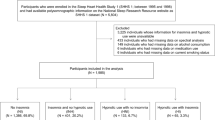
Adults (age: 18–65 years) with suspected OSA were recruited from the sleep clinic of Gil Medical Center from March 2012 to February 2016. Among 205 participants who were recruited through structured clinical interviews and screening scales, 171 participants were finally included in the analyses. All participants had symptoms of SS or OSA, such as frequent snoring, witnessed apnoea, experience of choking during sleep, and daytime sleepiness. They met the breathing-related sleep disorder diagnostic criteria of the Diagnostic and Statistical Manual of Mental Disorders (fourth edition, text revision)44. Subjects were interviewed and evaluated by medical doctors (i.e., board-certified medical doctors in the department of psychiatry, neurology, and Otolaryngology) with over 5 years of experience in OSA and sleep medicine.
The exclusion criteria for participants were as follows: (i) comorbidity of severe medical or surgical conditions; (ii) major psychiatric disorders; (iii) previous diagnosis with OSA; (iv) history of uvulopalatopharyngoplasty; and (v) suspected as having other major sleep disorders such as restless legs syndrome, REM sleep behaviour disorder, circadian rhythm sleep disorder, or narcolepsy.
Written informed consent was obtained from all participants prior to inclusion in the study, and the Institutional Review Board of Gil Medical Center approved all study protocols. All experiments were performed in accordance with relevant guidelines and regulations.
Polysomnography
In-laboratory and monitored nocturnal PSG were conducted for all participants. Standard PSG recordings included six electroencephalogram leads (F3, F4, C3, C4, O1, and O2), one electrocardiography channel, two electrooculogram channels (E1-M2 and E2-M2), and three electromyography channels (chin and both anterior tibialis muscles) and were conducted according to the recommendations of American Academy of Sleep Medicine (AASM)45. PSG was conducted using COMET systems (Grass-Telefactor Corporation), and PSG results were scored based on the criteria in the AASM manual45. We used the recommended rules of hypopnea (≥30% reduction in nasal pressure signal excursions from baseline that lasted ≥10 s and were associated with ≥4% desaturation from the pre-event baseline) during sleep in the AASM manual45 and OSA was defined as an AHI ≥ 5 and SS as AHI < 5. Experienced PSG technologists who completed the interscorer reliability program of the AASM (http://www.aasmnet.org/isr/) scored PSG recordings using the AASM sleep scoring criteria45. All PSG data were confirmed by a sleep specialist medical doctor (K.H.P.).
Spectral analysis
Power spectra were computed for each EEG frequency band: slow oscillation (0.5–1 Hz), delta (1–4 Hz), theta (4–8 Hz), alpha (8–12 Hz), sigma (12–15 Hz), and beta (15–20 Hz). For the present analysis, data derived from stages N2, N3, REM and the average NREM central EEG electrode (i.e., [C3/A2 + C4/A1]/2) were used.
SpectralTrainFig was used for power spectral analysis. This program is an automated open-source Matlab graphic interface for the spectral analysis of sleep EEG in PSG. It detects and deletes epochs with artifact automatically and generates summary figures for visual adjudication46,47. It was developed by the National Sleep Research Resource (https://github.com/nsrr/SpectralTrainFig)48,49. In accordance with Welch’s method, the spectral power density was calculated using 10 overlapping 4-s sub-epochs for each 30-s epoch, with a 50% tapered cosine window. The artifact due to electrocardiogram interference was removed using a template subtraction method50. Manual visual adjudication was performed by a researcher who was blinded to the subject group, and spectra data with significant artifacts were excluded manually. In spectral analysis using the SpectralTrainFig program and visual adjudication, 34 subjects were excluded due to excessive PSG artifacts.
Statistical analysis
G*Power 3.1.9.2 software was used for sample size calculation. The minimum sample size yielded from this program was 134 (34 for group 1 and 100 for group 2). In the power analysis, a medium effect size of 0.5, power of 0.8 and α error probability of 0.05 were applied with group allocation ratio of 3 (OSA:SS = 3:1) based on the previous works12,13.
IBM SPSS for Windows software (version 23.0, IBM Corp, Armonk, NY, USA) was used for data analysis. Chi-square test was used for categorical variables, and independent t-test analysis of variance or analysis of covariance was used to compare the demography, PSG characteristics, and absolute spectral EEG power between the groups. Pearson correlation analysis was used to assess the correlation between AHI, arousal index and absolute spectral EEG power. Log transformation of spectral EEG power was conducted before Pearson correlation analysis when both variables showed deviation from normal distribution. P < 0.05 after Bonferroni correction was considered statistically significant.
References
American Academy of Sleep Medicine. International Classification of Sleep Disorders 3rd ed. (American Academy of Sleep Medicine, 2014).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). (American Psychiatric Publishing, 2013).
Yaffe, K. et al. Sleep-disordered breathing, hypoxia, and risk of mild cognitive impairment and dementia in older women. JAMA 306, 613–619, https://doi.org/10.1001/jama.2011.1115 (2011).
Pillar, G. & Lavie, P. Psychiatric symptoms in sleep apnea syndrome: effects of gender and respiratory disturbance index. Chest 114, 697–703, https://doi.org/10.1378/chest.114.3.697 (1998).
Ohayon, M. M. The effects of breathing-related sleep disorders on mood disturbances in the general population. J Clin Psychiatry 64, 1195–1200; quiz, 1274–6, https://doi.org/10.4088/jcp.v64n1009 (2003).
Greenberg, H., Lakticova, V. & Scharf, S. M. Principles and Practice of Sleep Medicine 1110–1124. e1116 (Elsevier, 2017).
Counter, P. & Wilson, J. A. The management of simple snoring. Sleep Med Rev 8, 433–441, https://doi.org/10.1016/j.smrv.2004.03.007 (2004).
Karakoc, O., Akcam, T., Gerek, M., Genc, H. & Ozgen, F. The upper airway evaluation of habitual snorers and obstructive sleep apnea patients. ORL 74, 136–140, https://doi.org/10.1159/000337134 (2012).
Ekici, M. et al. Risk factors and correlates of snoring and observed apnea. Sleep Med 9, 290–296, https://doi.org/10.1016/j.sleep.2007.04.018 (2008).
Kalchiem‐Dekel, O. et al. Snoring intensity and excessive daytime sleepiness in subjects without obstructive sleep apnea. Laryngoscope 126, 1696–1701, https://doi.org/10.1002/lary.25876 (2016).
Svensson, M., Franklin, K. A., Theorell-Haglöw, J. & Lindberg, E. Daytime sleepiness relates to snoring independent of the apnea-hypopnea index in women from the general population. Chest 134, 919–924, https://doi.org/10.1378/chest.08-0847 (2008).
Kang, J. M. et al. Comparison of psychiatric symptoms in patients with obstructive sleep apnea, simple snoring, and normal controls. Psychosomatic medicine 80, 193–199, https://doi.org/10.1097/PSY.0000000000000541 (2018).
Kang, J. M. et al. The quality of life of suspected obstructive sleep apnea patients is related to their subjective sleep quality rather than the apnea-hypopnea index. Sleep Breath 21, 369–375, https://doi.org/10.1007/s11325-016-1427-8 (2017).
Asghari, A. & Mohammadi, F. Is apnea-hypopnea index a proper measure for obstructive sleep apnea severity? Med J Islam Repub Iran 27, 161–162 (2013).
Sforza, E. et al. Personality, anxiety and mood traits in patients with sleep-related breathing disorders: effect of reduced daytime alertness. Sleep Med 3, 139–145, https://doi.org/10.1016/s1389-9457(01)00128-9 (2002).
Asghari, A., Mohammadi, F., Kamrava, S. K., Tavakoli, S. & Farhadi, M. Severity of depression and anxiety in obstructive sleep apnea syndrome. Eur Arch Otorhinolaryngol 269, 2549–2553, https://doi.org/10.1007/s00405-012-1942-6 (2012).
Lee, S.-A., Han, S.-H. & Ryu, H. U. Anxiety and its relationship to quality of life independent of depression in patients with obstructive sleep apnea. J Psychosom Res 79, 32–36, https://doi.org/10.1016/j.jpsychores.2015.01.012 (2015).
Macey, P. M., Woo, M. A., Kumar, R., Cross, R. L. & Harper, R. M. Relationship between obstructive sleep apnea severity and sleep, depression and anxiety symptoms in newly-diagnosed patients. PLoS One 5, e10211, https://doi.org/10.1371/journal.pone.0010211 (2010).
Ong, J. C., Gress, J. L., San Pedro-Salcedo, M. G. & Manber, R. Frequency and predictors of obstructive sleep apnea among individuals with major depressive disorder and insomnia. J Psychosom Res 67, 135–141, https://doi.org/10.1016/j.jpsychores.2009.03.011 (2009).
Chervin, R. D., Burns, J. W. & Ruzicka, D. L. Electroencephalographic changes during respiratory cycles predict sleepiness in sleep apnea. Am J Respir Crit Care Med 171, 652–658, https://doi.org/10.1164/rccm.200408-1056OC (2005).
Alvarez, D., Hornero, R., Marcos, J., Del Campo, F. & Lopez, M. Spectral analysis of electroencephalogram and oximetric signals in obstructive sleep apnea diagnosis. Conf Proc IEEE Eng Med Biol Soc 2009, 400–403, https://doi.org/10.1109/iembs.2009.5334905 (2009).
Lee, Y. J., Kim, J. W., Lee, Y. J. & Jeong, D. U. Sleep EEG characteristics in young and elderly patients with obstructive sleep apnea syndrome. Psychiatry Investig 13, 217–221, https://doi.org/10.4306/pi.2016.13.2.217 (2016).
Lee, H. K., Park, D. H., Shin, H. S. & Hong, S. C. Comparison of low resolution electromagnetic tomography imaging between subjects with mild and severe obstructive sleep apnea syndrome: a preliminary study. Psychiatry Investig 5, 45–51, https://doi.org/10.4306/pi.2008.5.1.45 (2008).
Appleton, S. L. et al. Quantitative electroencephalography measures in rapid eye movement and nonrapid eye movement sleep are associated with apneahypopnea index and nocturnal hypoxemia in men. Sleep 42, https://doi.org/10.1093/sleep/zsz092 (2019).
Mathieu, A. et al. Does age worsen EEG slowing and attention deficits in obstructive sleep apnea syndrome? Clin Neurophysiol 118, 1538–1544, https://doi.org/10.1016/j.clinph.2007.04.009 (2007).
D’Rozario, A. L. et al. A new EEG biomarker of neurobehavioural impairment and sleepiness in sleep apnea patients and controls during extended wakefulness. Clin Neurophysiol 124, 1605–1614, https://doi.org/10.1016/j.clinph.2013.02.022 (2013).
Sforza, E., Grandin, S., Jouny, C., Rochat, T. & Ibanez, V. Is waking electroencephalographic activity a predictor of daytime sleepiness in sleep-related breathing disorders? Eur Respir J 19, 645–652, https://doi.org/10.1183/09031936.02.00267302 (2002).
Grenèche, J. et al. EEG spectral power and sleepiness during 24h of sustained wakefulness in patients with obstructive sleep apnea syndrome. Clin Neurophysiol 119, 418–428, https://doi.org/10.1016/j.clinph.2007.11.002 (2008).
Xiromeritis, A. G. et al. Quantitative spectral analysis of vigilance EEG in patients with obstructive sleep apnoea syndrome: EEG mapping in OSAS patients. Sleep Breath 15, 121–128, https://doi.org/10.1007/s11325-010-0335-6 (2011).
Morisson, F. et al. Spectral analysis of wakefulness and REM sleep EEG in patients with sleep apnoea syndrome. Eur Respir J 11, 1135–1140, https://doi.org/10.1183/09031936.98.11051135 (1998).
Morisson, F. et al. Daytime sleepiness and EEG spectral analysis in apneic patients before and after treatment with continuous positive airway pressure. Chest 119, 45–52, https://doi.org/10.1378/chest.119.1.45 (2001).
Saunamäki, T., Jehkonen, M., Huupponen, E., Polo, O. & Himanen, S.-L. Visual dysfunction and computational sleep depth changes in obstructive sleep apnea syndrome. Clin EEG Neurosci 40, 162–167, https://doi.org/10.1177/155005940904000308 (2009).
Jones, S. G. et al. Regional reductions in sleep electroencephalography power in obstructive sleep apnea: a high-density EEG study. Sleep 37, 399–407, https://doi.org/10.5665/sleep.3424 (2014).
Dingli, K. et al. Electroencephalographic spectral analysis: detection of cortical activity changes in sleep apnoea patients. Eur Respir J 20, 1246–1253, https://doi.org/10.1183/09031936.02.00288202 (2002).
Himanen, S. L., Virkkala, J., Huupponen, E. & Hasan, J. Spindle frequency remains slow in sleep apnea patients throughout the night. Sleep Med 4, 361–366, https://doi.org/10.1016/s1389-9457(03)00155-2 (2003).
Benbadis, S. R. Introduction to sleep electroencephalography in Sleep: a comprehensive handbook 989–1004 (John Wiley & Sons, 2006).
Huang, S. et al. The correlations between electroencephalogram frequency components and restoration of stable breathing from respiratory events in sleep apnea hypopnea syndrome. Respir Physiol Neurobiol 258, 91–97, https://doi.org/10.1016/j.resp.2018.06.006 (2018).
Svanborg, E. & Guilleminault, C. EEG frequency changes during sleep apneas. Sleep 19, 248–254 (1996).
De Carli, F. et al. Quantitative analysis of sleep EEG microstructure in the time–frequency domain. Brain Res Bull 63, 399–405, https://doi.org/10.1016/j.brainresbull.2003.12.013 (2004).
Lee, S. et al. Comparison of awareness of symptoms and illness between patients with obstructive sleep apnea and simple snoring. Sleep Med Psychophysiol 23, 16–24, https://doi.org/10.14401/KASMED.2016.23.1.16 (2016).
Bianchi, M. T., Williams, K. L., Mckinney, S. & Ellenbogen, J. M. The subjective–objective mismatch in sleep perception among those with insomnia and sleep apnea. J Sleep Res 22, 557–568, https://doi.org/10.1111/jsr.12046 (2013).
Ray, W. J. & Cole, H. W. EEG alpha activity reflects attentional demands, and beta activity reflects emotional and cognitive processes. Science 228, 750–752, https://doi.org/10.1126/science.3992243 (1985).
Terzano, M. G. & Parrino, L. Origin and Significance of the Cyclic Alternating Pattern (CAP): REVIEW ARTICLE. Sleep Med Rev 4, 101–123, https://doi.org/10.1053/smrv.1999.0083 (2000).
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders DSM-IV-TR Fourth Edition (Text Revision). (Amer Psychiatric Publishing, 2000).
Iber, C. American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications. (American Academy of Sleep Medicine, 2007).
Buckelmuller, J., Landolt, H. P., Stassen, H. H. & Achermann, P. Trait-like individual differences in the human sleep electroencephalogram. Neuroscience 138, 351–356, https://doi.org/10.1016/j.neuroscience.2005.11.005 (2006).
Chen, Y., Wang, Z. Y., Yuan, G. & Huang, L. An overview of online based platforms for sharing and analyzing electrophysiology data from big data perspective. WIREs Data Mining Knowl Discov 7, e1206, https://doi.org/10.1002/widm.1206 (2017).
Dean, D. A. II et al. Scaling up scientific discovery in sleep medicine: the national sleep research resource. Sleep 39, 1151–1164, https://doi.org/10.5665/sleep.5774 (2016).
Mariani, S. et al. Evaluation of an automated pipeline for large-scale EEG spectral analysis: the national sleep research resource. Sleep Med 47, 126–136, https://doi.org/10.1016/j.sleep.2017.11.1128 (2018).
Nakamura, M. & Shibasaki, H. Elimination of EKG artifacts from EEG records: a new method of non-cephalic referential EEG recording. Electroencephalogr Clin Neurophysiol 66, 89–92, https://doi.org/10.1016/0013-4694(87)90143-x (1987).
Acknowledgements
It was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health and Welfare, Republic of Korea (grant number: HI17C2665). We thank Dr. Dennis Dean, PhD and National Sleep Research Resource for creating the SpectralTrainFig. We also thank Dr. Kwang-Pil Ko for the statistical assistance.
Author information
Authors and Affiliations
Contributions
J.M.K. and S.T.K. wrote the manuscript. S.G.K and K.H.P. designed and managed the study. S.G.K., K.H.P. and S.T.K. selected the participants through clinical and semi-structured interviews. S.M., S.E.C. and S.G.K. managed the data and performed the spectral and statistical analysis. S.G.K., K.H.P. and J.W.W. conceptualized the study and performed literature review. All authors contributed to and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kang, J.M., Kim, S.T., Mariani, S. et al. Difference in spectral power density of sleep EEG between patients with simple snoring and those with obstructive sleep apnoea. Sci Rep 10, 6135 (2020). https://doi.org/10.1038/s41598-020-62915-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-62915-x
- Springer Nature Limited
This article is cited by
-
Compensatory mechanisms of reduced interhemispheric EEG connectivity during sleep in patients with apnea
Scientific Reports (2023)