
Abstract
Several previous studies have noted benefits of maintaining continuity of care (COC), including improved patient compliance, decreased health care cost, and decreased incidence of hospitalization. However, the association of COC in hypertension patients with subsequent cardiovascular disease (CVD) risk is yet unclear. Therefore, we aimed to investigate the impact of COC on CVD risk among newly-diagnosed hypertension patients. We conducted a cohort with a study population consisted of 244,187 newly-diagnosed hypertension patients in 2004 from the Korean National Health Insurance Service database. The participants were then divided into approximate quartiles of COC index, and followed from 1 January 2007 until 31 December 2017. Cox proportional hazards models were used to evaluate the adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) for CVD risk according to quartiles. Compared to patients within the lowest quartile of COC index, those within the highest quartile of COC index had reduced risk for CVD (aHR 0.76, 95% confidence interval; CI 0.73–0.79), CHD (aHR 0.66, 95% CI 0.62–0.69) and stroke (aHR 0.84, 95% CI 0.80–0.88). COC among hypertension patients was associated with improved medication compliance and reduced risk of stroke and CVD. The importance of maintaining COC should be emphasized to reduce the risk of CVD among hypertension patients.
Similar content being viewed by others

Introduction
Hypertension is known to be a major modifiable risk factor for cardiovascular disease (CVD)1, and it is also one of the leading causes of a preventable death2. In 2017, the American College of Cardiology/American Heart Association released an updated guideline. According to the new criteria for hypertension, 46% of the United State adults are affected by high blood pressure3. However, approximately 30% of those who affected are not aware of the disease, and less than 60% are adequately controlled worldwide4. Since CVD is also recognized as the leading cause of death5, it is important to emphasize proper management of hypertension to reduce the risk of CVD and mortality.
Meanwhile, previous studies have noted poor care coordination on chronic diseases has been associated with increase in medical expense6,7. Continuity of care (COC), which generally refers to the relationship between patient and their physician overtime8, is known to improve quality of care and patient compliance9,10. Despite these benefits, not having COC on patients with chronic disease is common, especially in Asian countries where primary care physician is not established commonly11. Although it is likely that COC among chronic diseases patients such as hypertension would benefit from their comprehensive care, the impact of COC on clinical outcomes are relatively less studied. Previous studies investigated the effect of COC among hypertension patients focused on the outcomes of blood pressure control12, medication compliance13, health care cost7, and incidence of hospital admission14. However, the association of COC with CVD is still unexplored especially among hypertension patients.
Therefore, we aimed to investigate the impact of COC on cardiovascular risk among newly-diagnosed hypertension patients by using nationwide health claim database from Korean National Health Insurance Service (NHIS). Also, we evaluated the association of COC with medication compliance as a secondary outcome as well.
Methods
Study population
The study population was derived from NHIS database. Nearly all South Korean citizens are ensured under the NHIS, with an enrollment rate of 97%. The NHIS provides mandatory health care covering most forms of health services, and the data from insured health services including hospital use inpatient and outpatient, pharmaceutic drug prescriptions are collected in the NHIS database15,16. Additionally, NHIS provides biannual national health screening examinations for enrollees. The results of health examinations are also collected by the NHIS and provided for research purposes. These data include anthropometric measurements, a self-reported questionnaire on participants’ health behaviors, and laboratory tests for blood15. The NHIS database has been used for multiple previous epidemiological studies, and its validity is described detail elsewhere17,18.
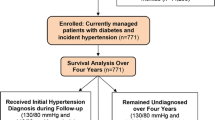
Among 295,594 newly-diagnosed hypertension patients in 2004, we excluded 8 participants who were aged less than 20 years. Then, 25,240 participants with missing values for covariates were further excluded. Finally, 1878 and 24,281 participants who died or diagnosed with CVD prior to the index date of 1 January 2007 were excluded, respectively. The final study population consisted of 244,187 participants who underwent health examinations before index date. All participants were followed-up from 1 January 2007 until the event of CVD, death, or 31 December 2017, whichever came earliest. Figure 1 presents the flow diagram of selecting study participants.

Flow diagram of selection of study participant.
Key variables
Hypertension was defined as the prescription of anti-hypertensive medication under the diagnosis code for hypertension (I10) under the International Classification of Diseases Tenth Edition (ICD-10). Participants with less than 4 visits within the first 2 years of diagnosis were not included in the newly-diagnosed hypertension patients. The rationale of this exclusion criteria was based on previous studies that investigated the COC19,20. It was noted that continuity cannot be assessed well with few visits, since it’s relatively easy to attain its maximum (1) or minimum (0) value with few visits19. Previous studies have adopted 2-year exposure periods to ensure longitudinal continuity20, and analyzed participants who had 4 or more visits19. COC was measured by the COC index and the number of medical institutions utilized21,22. COC index is a widely used measure of continuity that reflects both the frequency of visits to each provider and the dispersion of visits between providers23,24. Hospital use for hypertensive medication prescriptions in South Korea requires the medical records for Korean National Health Insurance reimbursement. Therefore, almost every hospital uses including outpatient and inpatient for hypertension is recorded in NHIS, which makes the COC index calculated by claim data of NHIS valid and accurate. COC index and the number of medical institutions a person visited within first 2 year of diagnosis, which was 2005–2006, according to all outpatient visit. The participants were then divided into approximate quartiles, with participants among the first quartile having lowest COC index or the number of medical institutions utilized.
The event of CVD was defined when a participant was hospitalized more than 2 days under diagnosis code for CHD (ICD-10 codes for I20-I21) or stroke (ICD-10 codes for I60-I69)25. Medication compliance was determined by medication possession ratio (MPR). MPR was calculated by the proportion of the hypertensive medication prescriptions days during the first 2 years of follow-up period (2007–2008). High medication compliance was defined when a participant had an MPR value of 0.8 or higher26,27.
The considered covariates included age (continuous, years), sex (categorical, men and women), household income (categorical, 1st , 2nd , 3rd , and 4th quartiles), smoking status (categorical, never, past, and current smokers) alcohol consumption (categorical, 0, 0–1, 1–2, 3–4, and 5 or more times per week), physical activity (categorical, 0, 1–2, 3–4, 5–6, and 7 times per week), body mass index (continuous, kg/m2), fasting serum glucose (continuous, mg/dL), and Charlson comorbidity index (continuous). Smoking status, alcohol consumption and physical activity were assessed by a self-reported questionnaire during the health examination. Household income was derived from the insurance premium and the Charlson comorbidity index was calculated with an algorithm adopted form a previous study28,29.
Statistical analysis
Chi-square test for categorical variables and analysis of variance for continuous variables were conducted to compare the difference in distributions of covariates according to the quartiles of COC index. Multivariate Cox proportional hazard regression analyses were conducted to evaluated adjusted hazard ratios (aHRs) and 95% confidence intervals (CIs) for CVD, CHR and stroke risk according to the COC index and the number of medical institutions utilization quartile groups. The proportionality assumption of the Cox proportional hazards regression has been visually tested and validated using the Schoenfeld residual method. We also conducted multivariate logistic regression to determine the adjusted odds ratios (aORs) and 95% CIs for hypertensive medication compliance according to the quartiles of COC index. Stratified analyses on the association of COC index with CVD were conducted according to the subgroups of age, sex, smoking status, alcohol consumption, physical activity, Charlson comorbidity index, medication compliance, and pre-diagnosis blood pressure. (Fig. 2) Additionally, analyses using the usual provider continuity (UPC) score and the modified modified continuity index (MMCI) as other measures of COC were conducted21. The methods of calculating theses indices are well established and noted in multiple previous studies23,24,30,31.


Stratified analysis on the association of continuity of care with cardiovascular disease according to subgroups of age, smoking, alcohol intake, physical activity, Charlson comorbidity index, and medication compliance. (A) Adjusted hazard ratio for cardiovascular disease of participants in 2nd quartile compared to those of 1st quartile. (B) Adjusted hazard ratio for cardiovascular disease of participants in 3rd quartile compared to those of 1st quartile. (C) Adjusted hazard ratio for cardiovascular disease of participants in 4th quartile compared to those of 1st quartile. HR adjusted hazard ratio, CI confidence interval, MPR medication possession ratio, BP blood pressure.
Statistical significance was defined as a two-side p value of less than 0.05. All data collection and statistical analyses were conducted using SAS Enterprise Guide 7.1 (SAS Institute, Cary, USA).
Ethical considerations
This study was approved by the Seoul National University Hospital Institutional Review Board (IRB number: E-1812-041-993) and the analyses were performed in accordance with relevant guidelines and regulations. The requirement for informed consent was waived as the NHIS database was constructed after anonymization according to strict confidentiality guidelines.
Results
The descriptive characteristics of the study population according to COC index quartiles are depicted in Table 1. The range of COC index were 0.00–0.23, 0.23–0.36, 0.36–0.56, and 0.57–1.00 for the 1st, 2nd, 3rd, and 4th quartiles groups. Participants with higher COC index tended to be young age, men, have lower household income, smoke often, consume more alcohol, had higher pre-diagnosis blood pressure, obese, and have less comorbidities.
Table 2 shows the risk of CVD, CHD, and stroke according to quartiles of the COC index. Compared to the participants with the lowest COC index, those with the highest COC index had 24% lower risk for CVD, 34% lower risk for CHD, and 15% lower risk for stroke. Furthermore, the risk reduction of CVD, CHD, and stroke tended to be higher according to the higher quartiles of the COC index (all p for trend < 0.001).
Similarly, Table 3 depicts the risk of CVD, CHD, and stroke according to the number of medical institutions utilized. Participants who visited the greatest number of medical institutions (> 9 institutions) had 33% increased risk for CVD, 63% increased risk for CHD, and 14% increased risk for stroke, compared to those with the least number of medical institutions (1–3 institutions). As the number of medical institutions utilized increased, statistically significant increased risk of developing CVD, CHD, and stroke were observed (all p for trend < 0.001).
The association of COC with hypertensive medication compliance is shown in Table 4. While 44.8% of participants with the lowest COC index maintained high medication compliance of MPR more than 0.8, 61.9% of those with the highest COC index maintained high medication compliance among the first 2 years of hypertension diagnosis. Compared to the patients with the lowest COC, those with the highest COC had higher odds (aOR 1.76, 95% CI 1.71–1.79) for having high medication compliance.
Figure 2 shows the results from stratified analyses of the impact of COC on CVD according to the subgroups of age, sex, smoking status, alcohol consumption, physical activity, Charlson comorbidity index, medication compliance, and pre-diagnosis blood pressure. The risk reduction of CVD among the high COC index group was preserved among the subgroups mentioned above, particularly regardless of medication compliance. This result from the stratified analysis demonstrates that COC has a benefit in reducing the risk of CVD independent of medication compliance.
The risk of CVD, CHD, and stroke according to other measures of COC is shown in Supplementary Table S1. The results were consistent with those of Table 2, showing that maintaining higher UPC score and MMCI was associated with reduced risk for CVD, CHD and stroke.
Discussion
In this nationwide population-based study among 244,187 newly-diagnosed hypertension patients, we have shown that COC was associated with reduced risk of CVD. We have also applied an intuitive measure of COC, the number of medical institutions utilized, to evaluate the CVD risk associated with COC. The increasing number of utilized medical institutes, which represents lower COC, was associated with a higher risk for CVD compared to those who visited fewer hospitals. Furthermore, we have demonstrated that higher COC was associated with higher medication compliance. While several previous studies have investigated the benefits of COC among hypertension patients7,12,13,14, none of these focused on the risk of developing CVD.
Several possible mechanisms could explain the association of COC with decreased risk of cardiovascular diseases observed in this study. It is noted that higher COC among hypertension patients is associated with higher health-related quality of life32, which reflects both physical function and mental health. Likewise, patients with high COC are more likely to receive a higher quality of care and improve lifestyle behaviors as noted in the previous studies9,33. Moreover, patients with higher COC are associated with a higher level of trust in physicians along with higher patient satisfaction34,35, which is directly linked to medication compliance as shown in this study as well36,37. Particularly among hypertension patients, some studies noted that the higher COC is also associated with the higher rate of controlled blood pressure12, which is also directly associated with the risk reduction of cardiovascular disease.
Previous studies have evaluated the positive effect of COC on the concept of health care expense. These studies reported that maintaining COC is associated with the decreased number of emergency department visits24, hospitalizations10, and health care costs7,24. Other studies investigated the effect of COC among chronic diseases mainly focused on diabetic patients. These studies demonstrated that higher COC is associated with medication adherence31, better glycemic control37, and decreased mortality22,38. Similarly, a few recent studies evaluated the direct impact of COC on clinical outcomes, mostly focused on the mortality39,40,41.
Although numerous studies noted the benefits of maintaining COC, relatively few studies evaluated the effect of COC among hypertension patients. McClellan and colleagues evaluated 4688 hypertension patients and reported that COC was associated with better blood pressure control12. In 2011, a study investigated 5590 individuals aged more than 67 years and noted that COC may not increase adherence to hypertensive medication. Most recently, Ye and colleagues demonstrated higher COC among hypertension patients improved health-related quality of life32, and Nam and his colleagues reported the association of higher COC and decreased the risk of hospital admission in hypertension patients. However, the association of COC with the risk of disease development among hypertension patients was not noted in these studies. The result of this study further expands the concept of previous studies and demonstrated that COC is associated with reduced risk of CVD among newly-diagnosed hypertension patients.
There are several limitations to be considered in this study. First, COC was only measured by the pattern of clinical visits, which could not reflect some aspects of COC such as the interpersonal relationship between patient and physicians21,30. COC after the index date was not followed and therefore the effect of possible changes was not considered. Third, the study population was restricted to those newly-diagnosed hypertension patients. Hence, long-term complications of hypertension might be underestimated under eleven years of follow-up. Also, other possible complications of hypertension such as heart failure, hypertensive nephropathy, and hypertensive retinopathy were not assessed. Therefore, future studies with a longer follow-up period and assessment of various complications of hypertension are merited. Finally, hypertension medications or dietary intake that participants used were not reflected in our analysis. These factors indirectly reflect the severity of hypertension and might be associated with subsequent CVD. Although we tried to take into account the grade of hypertension and conducted the stratified analysis based on pre-diagnosis blood pressure (Fig. 2), further studies with considering the medications or dietary intake to control hypertension will be merited.
In spite of the limitations mentioned above, our study has some advantages. First, we investigated a large number of study population adjusting a wide range of covariates, which has not done previously. Extensive subgroup analyses of potential confounders also enhance the reliability of our results. Particularly, higher COC was associated with decreased risk of CVD even among those with high medication compliance, implying that COC has a benefit in reducing the risk of CVD independent of medication compliance. Second, we took account for multiple commonly used different measures of COC which led the similar results. Especially, the number of utilized medical institutes, which is an intuitive and simple measure reflects the non-continuity of care also demonstrated our main result effectively. Although the number of medical institutes utilized is an easier way to reflect COC, it has a limitation that it might be associated with severity and progression of hypertension, and therefore further studies on this index will be merited as well. Third, we attempted to clarify the possible mechanisms for the association of COC and reduced CVD risk by investigating medication compliance as an intermediate outcome.
In conclusion, we have shown that the COC was associated with decreased risk for CVD, CHD, and stroke among newly-diagnosed hypertension patients. Higher COC was also associated with improved hypertensive medication compliance. Therefore, the importance of COC should be emphasized to reduce the risk of cardiovascular complications of hypertension.
Data availability
This study is based on Korean National Health Insurance Service Database. These data do not belong to the authors but to the Korean National Health Insurance Service, and the authors are not permitted to share them, except in aggregate form.
References
Global Burden of Disease Study, C. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 386, 743–800. https://doi.org/10.1016/S0140-6736(15)60692-4 (2015).
Danaei, G. et al. The preventable causes of death in the United States: comparative risk assessment of dietary, lifestyle, and metabolic risk factors. PLoS Med 6, e1000058. https://doi.org/10.1371/journal.pmed.1000058 (2009).
Whelton, P. K. et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart association task force on clinical practice guidelines. Hypertension 71, 1269–1324. https://doi.org/10.1161/HYP.0000000000000066 (2018).
Collaboration, N. C. D. R. F. Long-term and recent trends in hypertension awareness, treatment, and control in 12 high-income countries: an analysis of 123 nationally representative surveys. Lancet 394, 639–651. https://doi.org/10.1016/S0140-6736(19)31145-6 (2019).
Roth, G. A. et al. Global and regional patterns in cardiovascular mortality from 1990 to 2013. Circulation 132, 1667–1678. https://doi.org/10.1161/CIRCULATIONAHA.114.008720 (2015).
Hussey, P. S. et al. Continuity and the costs of care for chronic disease. JAMA Intern. Med. 174, 742–748. https://doi.org/10.1001/jamainternmed.2014.245 (2014).
Hong, J. S., Kang, H. C. & Kim, J. Continuity of care for elderly patients with diabetes mellitus, hypertension, asthma, and chronic obstructive pulmonary disease in Korea. J. Korean Med. Sci. 25, 1259–1271. https://doi.org/10.3346/jkms.2010.25.9.1259 (2010).
Gulliford, M., Naithani, S. & Morgan, M. What is “continuity of care”?. J. Health Serv. Res. Policy 11, 248–250. https://doi.org/10.1258/135581906778476490 (2006).
Cabana, M. D. & Jee, S. H. Does continuity of care improve patient outcomes?. J. Fam. Pract. 53, 974–980 (2004).
van Walraven, C., Oake, N., Jennings, A. & Forster, A. J. The association between continuity of care and outcomes: a systematic and critical review. J. Eval. Clin. Pract. 16, 947–956. https://doi.org/10.1111/j.1365-2753.2009.01235.x (2010).
Sato, T., Takeichi, M., Shirahama, M., Fukui, T. & Gude, J. K. Doctor-shopping patients and users of alternative medicine among Japanese primary care patients. Gen. Hosp. Psychiatry 17, 115–125 (1995).
McClellan, W. M., Hall, W. D., Brogan, D., Miles, C. & Wilber, J. A. Continuity of care in hypertension. An important correlate of blood pressure control among aware hypertensives. Arch. Intern. Med. 148, 525–528. https://doi.org/10.1001/archinte.148.3.525 (1988).
Robles, S. & Anderson, G. F. Continuity of care and its effect on prescription drug use among Medicare beneficiaries with hypertension. Med. Care 49, 516–521. https://doi.org/10.1097/MLR.0b013e31820fb10c (2011).
Nam, Y. S., Cho, K. H., Kang, H. C., Lee, K. S. & Park, E. C. Greater continuity of care reduces hospital admissions in patients with hypertension: an analysis of nationwide health insurance data in Korea, 2011–2013. Health Policy 120, 604–611. https://doi.org/10.1016/j.healthpol.2016.04.012 (2016).
Seong, S. C. et al. Cohort profile: the national health insurance service-national health screening cohort (NHIS-HEALS) in Korea. BMJ Open 7, e016640. https://doi.org/10.1136/bmjopen-2017-016640 (2017).
Cheol Seong, S. et al. Data resource profile: the national health information database of the national health insurance service in South Korea. Int. J. Epidemiol. 46, 799–800. https://doi.org/10.1093/ije/dyw253 (2017).
Son, J. S. et al. Association of blood pressure classification in Korean Young adults according to the 2017 American College of Cardiology/American Heart association guidelines with subsequent cardiovascular disease events. JAMA 320, 1783–1792. https://doi.org/10.1001/jama.2018.16501 (2018).
Choi, S. et al. Association of obesity or weight change with coronary heart disease among young adults in South Korea. JAMA Intern. Med. 178, 1060–1068. https://doi.org/10.1001/jamainternmed.2018.2310 (2018).
Nyweide, D. J. et al. Continuity of care and the risk of preventable hospitalization in older adults. JAMA Intern. Med. 173, 1879–1885. https://doi.org/10.1001/jamainternmed.2013.10059 (2013).
Wolinsky, F. D. et al. Continuity of care with a primary care physician and mortality in older adults. J. Gerontol. A Biol. Sci. Med. Sci. 65, 421–428. https://doi.org/10.1093/gerona/glp188 (2010).
Saultz, J. W. Defining and measuring interpersonal continuity of care. Ann. Fam. Med. 1, 134–143 (2003).
Kim, J. H. & Park, E. C. Can diabetes patients seeking a second hospital get better care? Results from nested case-control study. PLoS ONE 14, e0210809. https://doi.org/10.1371/journal.pone.0210809 (2019).
Chan, C. L., You, H. J., Huang, H. T. & Ting, H. W. Using an integrated COC index and multilevel measurements to verify the care outcome of patients with multiple chronic conditions. BMC Health Serv. Res. 12, 405. https://doi.org/10.1186/1472-6963-12-405 (2012).
Dreiher, J. et al. The association between continuity of care in the community and health outcomes: a population-based study. Isr. J. Health Policy Res. 1, 21. https://doi.org/10.1186/2045-4015-1-21 (2012).
Writing Group, M. et al. Heart disease and stroke statistics-2016 update: a report from the american heart association. Circulation 133, e38–360. https://doi.org/10.1161/CIR.0000000000000350 (2016).
Friedman, O. et al. Antihypertensive drug persistence and compliance among newly treated elderly hypertensives in ontario. Am. J. Med. 123, 173–181. https://doi.org/10.1016/j.amjmed.2009.08.008 (2010).
Laliberte, F. et al. Impact of daily dosing frequency on adherence to chronic medications among nonvalvular atrial fibrillation patients. Adv. Ther. 29, 675–690. https://doi.org/10.1007/s12325-012-0040-x (2012).
Sundararajan, V. et al. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 57, 1288–1294. https://doi.org/10.1016/j.jclinepi.2004.03.012 (2004).
Choi, D., Choi, S., Son, J. S., Oh, S. W. & Park, S. M. Impact of discrepancies in general and abdominal obesity on major adverse cardiac events. J. Am. Heart Assoc. 8, e013471. https://doi.org/10.1161/JAHA.119.013471 (2019).
Jee, S. H. & Cabana, M. D. Indices for continuity of care: a systematic review of the literature. Med. Care Res. Rev. 63, 158–188. https://doi.org/10.1177/1077558705285294 (2006).
Chen, C. C., Tseng, C. H. & Cheng, S. H. Continuity of care, medication adherence, and health care outcomes among patients with newly diagnosed type 2 diabetes: a longitudinal analysis. Med. Care 51, 231–237. https://doi.org/10.1097/MLR.0b013e31827da5b9 (2013).
Ye, T. et al. Effect of continuity of care on health-related quality of life in adult patients with hypertension: a cohort study in China. BMC Health Serv. Res. 16, 674. https://doi.org/10.1186/s12913-016-1673-2 (2016).
Parchman, M. L., Pugh, J. A., Noel, P. H. & Larme, A. C. Continuity of care, self-management behaviors, and glucose control in patients with type 2 diabetes. Med. Care 40, 137–144. https://doi.org/10.1097/00005650-200202000-00008 (2002).
Saultz, J. W. & Albedaiwi, W. Interpersonal continuity of care and patient satisfaction: a critical review. Ann. Fam. Med. 2, 445–451 (2004).
Beattie, P., Dowda, M., Turner, C., Michener, L. & Nelson, R. Longitudinal continuity of care is associated with high patient satisfaction with physical therapy. Phys. Ther. 85, 1046–1052 (2005).
Brookhart, M. A. et al. Physician follow-up and provider continuity are associated with long-term medication adherence: a study of the dynamics of statin use. Arch. Intern. Med. 167, 847–852. https://doi.org/10.1001/archinte.167.8.847 (2007).
Mainous, A. G. 3rd., Baker, R., Love, M. M., Gray, D. P. & Gill, J. M. Continuity of care and trust in one’s physician: evidence from primary care in the United States and the United Kingdom. Fam. Med. 33, 22–27 (2001).
Worrall, G. & Knight, J. Continuity of care is good for elderly people with diabetes: retrospective cohort study of mortality and hospitalization. Can. Fam. Phys. 57, e16-20 (2011).
Maarsingh, O. R., Henry, Y., van de Ven, P. M. & Deeg, D. J. Continuity of care in primary care and association with survival in older people: a 17-year prospective cohort study. Br. J. Gen. Pract. 66, e531-539. https://doi.org/10.3399/bjgp16X686101 (2016).
Pereira Gray, D. J., Sidaway-Lee, K., White, E., Thorne, A. & Evans, P. H. Continuity of care with doctors-a matter of life and death? A systematic review of continuity of care and mortality. BMJ Open 8, e021161. https://doi.org/10.1136/bmjopen-2017-021161 (2018).
Shin, D. W. et al. Impact of continuity of care on mortality and health care costs: a nationwide cohort study in Korea. Ann. Fam. Med. 12, 534–541. https://doi.org/10.1370/afm.1685 (2014).
Funding
This research was supported by the National Health Insurance Service of Korea. K Kim received Grants from the BK21-Plus Education Program from the National Research Foundation of Korea. The National Health Insurance Service of Korea had no role in the design and conduct of the study, the collection, management, analysis, and interpretation of the data, or the preparation, review, or approval of the manuscript, and decision to submit for publication.
Author information
Authors and Affiliations
Contributions
S.M.P. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: D.C., S.M.P. Acquisition of data: Y.K., S.M.P. Analysis and interpretation of data: D.C., S.C., H.K., K.K., N.K., A.K., K.H.K., J.S.S., J.M.Y., Y.K., S.M.P. Drafting of the manuscript: D.C., S.M.P. Critical revision of the manuscript: D.C., S.C., H.K., K.K., N.K., A.K., K.H.K., J.S.S., J.M.Y., Y.K., S.M.P. Statistical analysis: D.C. Administrative, technical, or material support: Y.K.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Choi, D., Choi, S., Kim, H. et al. Impact of continuity of care on cardiovascular disease risk among newly-diagnosed hypertension patients. Sci Rep 10, 19991 (2020). https://doi.org/10.1038/s41598-020-77131-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-77131-w
- Springer Nature Limited
This article is cited by
-
Fear of recurrence in elderly patients with coronary heart disease: the current situation and influencing factors according to a questionnaire analysis
BMC Cardiovascular Disorders (2022)
-
Impact of continuity of care on risk for major osteoporotic fracture in patients with new onset rheumatoid arthritis
Scientific Reports (2022)
-
Efficacy of Statin Therapy in Patients with Hospital Admission for COVID-19
Cardiovascular Drugs and Therapy (2022)
-
Effects of continuity of care on health outcomes among patients with diabetes mellitus and/or hypertension: a systematic review
BMC Family Practice (2021)