
Abstract
We systematically reviewed observational and clinical trials (baseline) studies examining differences in gait parameters between Parkinson’s disease (PD) in on-medication state and healthy control. Four electronic databases were searched (November-2018 and updated in October-2020). Independent researchers identified studies that evaluated gait parameters measured quantitatively during self-selected walking speed. Risk of bias was assessed using an instrument proposed by Downs and Black (1998). Pooled effects were reported as standardized mean differences and 95% confidence intervals using a random-effects model. A total of 72 studies involving 3027 participants (1510 with PD and 1517 health control) met the inclusion criteria. The self-selected walking speed, stride length, swing time and hip excursion were reduced in people with PD compared with healthy control. Additionally, PD subjects presented higher cadence and double support time. Although with a smaller difference for treadmill, walking speed is reduced both on treadmill (.13 m s−1) and on overground (.17 m s−1) in PD. The self-select walking speed, stride length, cadence, double support, swing time and sagittal hip angle were altered in people with PD compared with healthy control. The precise determination of these modifications will be beneficial in determining which intervention elements are most critical in bringing about positive, clinically meaningful changes in individuals with PD (PROSPERO protocol CRD42018113042).
Similar content being viewed by others


Introduction
Parkinson’s disease (PD) is a chronic neurodegenerative condition characterized by decreased dopamine production in the substantia nigra pars compacta1. In addition, impairment in dopamine production resulting in changes on the cortical region is related to the planning and sequencing of the movements2.
In Brazil, the incidence of disease in 2005 was around 16 million, and the projection is that number can double in 20303. Factors such as aging, male gender, and geographic location may be associated with differences in PD incidence. It has been demonstrated that prevalence is higher after 79 years in South American residents4. Although the causes for PD manifestation are unknown, some studies show an association with genetic and environmental factors5,6.
Some motor symptoms such as bradykinesia, postural instability, rest tremor, rigidity, and slowness of movement are present in PD7. These cardinal symptoms promote alteration in gait parameters in subjects with PD8,9,10. The literature has indicated that self-selected walking speed (SSWS) is reduced in people with PD8,9 when compared to a matched healthy control group8.
Notably, individuals with PD walk with higher cadence, shorter stride length, higher time in double limb support phase, greater asymmetry of upper and lower limbs, axial rigidity and reduced range of hip, knee and ankle motions9,10,11,12. The reduced range of motion (ROM) in lower limbs exerts influence on the short stride length at SSWS10,12. Further, PD motor disturbance is characterized by a reduction in walking speed due to a combination of reduced stride length and increased cadence11,12. Kinematic changes may relate to an inability to maintain proper joint excursions.
Although the literature indicates some gait characteristics in PD, several evaluation methods are applied, resulting in different reference values9,10,11. An extensive range of evaluation methods, disease duration, disease stages, phase of medication and aging process may hamper clarity over these biomechanical parameters, generating difficulty in proposing more effective rehabilitation programs.
A recent review showed the gait impairments in PD13, however, they aimed to study the assessment, mechanisms, and interventions to improve gait, and no metanalysis was performed. A systematic review and meta-analysis conducted by Creaby and Cole14 showed spatiotemporal and kinematic characteristics representing the risk of falls in individuals with PD14. The meta-analysis revealed that the likelihood of falls is higher in PD individuals presenting slower walking speed, lower cadence, shorter strides and more mediolateral head and pelvis motion. Still, spatiotemporal and kinematic analyses during walking compared with the healthy control group were not performed. No systematic reviews with meta-analysis were found comparing spatiotemporal and kinematic parameters while walking between PD and healthy control individuals. The quantitative characterization of gait parameters in individuals with PD might help researchers analyze this population data and help professionals observe PD's gait evolution after a rehabilitation program. Therefore, the aim of this study was to systematically review the literature about the spatiotemporal and lower limb angles during walking on people with PD compared with age-matched control subjects and perform meta-analyses. We hypothesized that the SSWS would be deteriorated (reduced speed), accompanied by a reduction in the stride length, swing time and lower limb angles, and higher cadence, step width and double support in individuals with PD compared with healthy controls.
Methods
This systematic review has been reported according to the Guidelines for Meta-Analyses and Systematic Reviews of Observational Studies (MOOSE) (Supplementary material 1.1)15 and followed the recommendations proposed by the Preferred Reporting Items for Systematic review and Meta-Analysis Protocols (PRISMA-P) and Cochrane Collaboration16. The study protocol was pre-registered on the International Prospective Register of Systematic Reviews (PROSPERO protocol CRD42018113042). The present study has been published as a part of MSc dissertation of the first author (http://hdl.handle.net/10183/200663).
Search strategy
The search was conducted in November 2018 and updated in October 2020 by two experienced investigators. The searching electronic bibliographic databases were Cochrane library, Scopus, Pubmed, and EMBASE. Abstracts or extended abstracts published from conferences, theses, dissertations, or studies not yet published in journals were not included. The following terms were used in combination and/or alone: ‘‘Parkinson disease,’’ “kinematics”, “joint kinematic”, “hip angles”, “knee angles”, “ankle angles”, “stride frequency”, “stride length”. Boolean operators ‘‘OR’’ and ‘‘AND’’ were used to search the databases. Details of the PubMed search are shown in Supplementary material 1.2. Also, a manual search of the reference lists of the studies found in the databases was conducted.
Inclusion and exclusion criteria
This review included cross-sectional studies and clinical trials (from which only baseline values were extracted). To be considered eligible, studies should present: (1) straight-line free walking or treadmill walking evaluation with kinematic analysis; (2) people with PD as sample (evaluated in “on” period of medication, regardless of age, sex, and disease stage); (3) an age- and sex-matched healthy control group; (4) values (means and standard deviations) of spatiotemporal outcomes (during SSWS), walking distance, stride length, cadence, step width, double support, single support, swing time, sagittal hip, knee and ankle ROM throughout the gait cycle and at initial contact evaluated in SSWS. Some studies were excluded when (1) the variables of interest were not informed; (2) when subjects presented essential tremor, (3) postural alterations, such as camptocormia and Pisa syndrome; (4) de novo PD; (5) parkinsonism; (6) freezing and (7) differences speeds to both lower limbs; and (8) duplicate data. There were no restrictions on the date of publication for inclusion of studies in the review. Unpublished studies have not been included, and no hand searching was made. Only studies published in English, Portuguese, or Spanish were included. Excluded Studies are in Supplementary material 1.3.
Selection of studies
The selection of studies was conducted independently by two reviewers (A.P.J.Z.; E.S.S.). First, titles and abstracts of studies found through the search strategy were evaluated considering the eligibility criteria. In the second phase, for the selected articles or those in doubt, the same two independent reviewers performed the full-text reading, and the eligibility criteria were followed. Disagreements between reviewers were resolved by consensus, and when necessary, by a third reviewer (R.R.C.).
Data extraction was performed by the same independently two reviewers who conducted the selection of studies. A standardized form containing the information of interest that should be extracted was delivered to each of the reviewers. The data extracted from the studies were: Age (years), mass (kg), height (m), Hoehn and Yahr scale (H&Y), score of the Unified Parkinson's disease Rating Scale (UPDRS), disease duration (years), type of walk test performed (free walking test or treadmill), SSWS (m s−1) and walking distance (m) (Supplementary material 1.4). In addition, means and standard deviations of the outcomes were extracted to the standardized form: SSWS (m s−1), walking distance (m), stride length (m), cadence (step min−1), step width (m), double support (%), single support (%), swing time (%), sagittal hip, knee and ankle ROM (°), ankle, hip, and knee angles (°) at initial contact evaluated in SSWS. The authors of the included studies were contacted by email, aiming to access possible unclear data. If no answer was received, the data in question were excluded from the analysis. In the results presented through figures (graphics), the software Image-J (National Institute of Health, USA) was used to achieve the outcome data. The justification for exclusion is in Supplementary material 1.3.
Assessment of risk of bias (methodological quality)
A customized quality checklist was developed in this review, applying an instrument proposed by Downs and Black17. Other authors have been using this checklist with adequate and customized questions18,19,20. It was originally designed to assess the methodological quality of randomized and non-randomized studies of interventions. In this study, just observational studies were evaluated. Therefore, the instrument was developed by removing items 4, 8, 9, 13, 14, 15, 16, 17, 19, 23, 24, 25 and 26 because they were not relevant to these types of study. The included questions were 1, 2, 3, 5, 6, 7, 10, 11, 12, 18, 20, 21 and 22. The computation of quality of studies was based on Ratcliffe and collaborators21, studies scored as high quality achieve a score > 66.8%, medium quality 33.4–66.7%, and low-quality studies achieving < 33.3%.
Data analysis
The pooled effect estimates were computed from the difference scores between the gait parameters of PD individuals and the healthy controls, their standard deviations, and the number of participants. The authors were contacted through emails for unreported data and, if no answer was returned or the data requested were not available, the studies were excluded. To be included in the meta-analysis study needed to present the mean, standard deviation, standard error, or upper and lower limits of 95% confidence interval.
The results of meta-analyses are exhibited as standardized mean differences and calculations were performed using random-effects models. Statistical heterogeneity of evaluations among studies was evaluated by Cochran’s Q test and the I2 inconsistency test; it was considered that values > 50% indicated high heterogeneity16. Also, sensitivity analyses were conducted to investigate the possible influence of the method selected to assess gait parameters in the included studies on the differences between PD and healthy people, separating the studies using free walking of those using treadmill. Meta-regression analyses were performed to investigate potential moderators: mean age (years), mean H&Y (scores), mean UPDRS (scores) and mean disease duration (years). For descriptive analysis, the mean and standard deviation of each outcome in each group was presented (Supplementary material 2.6). Subgroup (treadmill versus free walking) and meta-regression analyses were not performed for joint kinematic from lower limbs (ROM and angle at initial contact) because there were not enough studies. Also, subgroup analyses were not performed for stride length, step width, double support time, single support time, swing time because there were not enough studies. Furthermore, publication bias was assessed using funnel plots for each outcome (of each trial's effect size against the standard error). Funnel plot asymmetry was evaluated using Begg and Egger tests22 and significant publication bias was considered if the p value < 0.05. Trim-and-fill computation was used to estimate the effect of publication bias on the interpretation of results23.
Forest plots were generated indicating the pooled effects and standardized mean differences, with 95% confidence intervals (CIs) for each outcome. Values of p < 0.05 were considered statistically significant. All analyses were performed using Comprehensive Meta-Analysis software version 3.3.07. All individual data are in Supplementary material 2.7.
Results
Studies selection
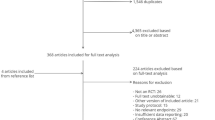
A total of 2398 studies were identified during the literature search. After adjusting for duplicates, 2042 studies remained. No additional articles were included in the present review, resulting from the manual search performed. After reading the abstracts, 1775 were removed, as they did not contain the key concepts of the study question. The full texts of 267 studies were read, and, from this analysis, 194 studies were excluded. Most of these studies were excluded either because (1) the study did not evaluate gait variables, (2) evaluation performed in OFF medication, (3) lack of control group, (4) post-deep brain stimulation (DBS) surgery (5) characteristic of a preliminary study. Thus, 72 studies met the inclusion criteria and were included in the quantitative analysis (Fig. 1). Three trials were included twice because they had met the eligibility criteria for two comparison groups. No other search was performed.

Flowchart of number of articles retrieved during the literature search and study selection.
Characteristics of the included studies
In total, 72 studies and 76 comparison pairs were found. In this review, 3027 participants were included in the meta-analyses. Among these, 1510 and 1517 participants were from PD groups and control groups, respectively. 77% of the studies showed H&Y values, 66% provide UPDRS information, 62% of the studies exhibited the disease duration, 100% informed age of PD group, and 1% did not provide this information about control group. The characteristics of the 72 included studies are available in Supplementary material 1.4.
Methodological quality of the included trials
Of the 72 included studies, 100% showed the hypothesis/aim/objective clearly described, 97% described the primary outcomes, 59% indicated the characteristics of participants clearly, 99% described principal confounders, 100% reported the main findings, 100% showed random variability in the data, 82% described probability values, in 75% of the studies the participants are representative of the population, 93% measured the appropriate statistic, 100% measured the main outcome if accurate methods, 100% recruited the participants of the same population and 8% of the studies recruited the participants of the groups in the same period (Supplementary material 1.5).
Gait Parameters of PD and healthy
Meta-analysis of speed
Data concerning speed were available from 69 studies and 72 combination pairs, which compare the speed of PD versus healthy group, in 2932 participants. Meta-analysis showed that speed is approximately 0.17 m s−1 reduced in people with PD compared with healthy group (ES: − 0.913; 95% CI − 1.100 to − 0.725; p < 0.001; I2: 81%) (Fig. 2). However, the analysis of publication bias for this outcome identified a significant bias (p = 0.003), and thus the adjusted value of the effect size, according to the Duval and Tweedie’s trim and fill test, resulted in − 0.619 (95% CI − 0.809 to − 0.429).

Standardized mean differences on gait speed between Parkinson and healthy individuals. CI confidence interval, Std diff standardized difference.
Subgroup analysis of studies showed that PD participants walked slower than healthy controls both during free (66 studies; 68 combination pairs; ES: − 0.914; 95% CI − 1.113 to − 0.716; p < 0.001; I2: 82%; − 0.17 m s−1) and treadmill walking (3 studies; 4 combination pairs; ES: − 0.919; 95% CI − 1.376 to − 0.462; p < 0.001; I2: 54%; − 0.13 m s−1). More information on these studies is in Supplementary material 1.4. According to the results of meta-regression analysis, mean age, H&Y, UPDRS, and disease duration did not influence the gait speed difference between PD versus the healthy control group (Table 1).
Meta-analysis of stride length
Data concerning stride length were available from 52 studies and 54 combination pairs, which compare stride length of PD versus healthy group, in a total of 2188 participants. Meta-analysis demonstrated that stride length is approximately 0.16 m reduced in PD compared with healthy groups (ES: − 1.032; 95% CI − 1.198 to − 0.866; p < 0.001; I2: 67%) (Fig. 3). However, the analysis of publication bias for this outcome identified a significant bias (p = 0.003), and thus the adjusted value of the effect size, according to the Duval and Tweedie’s trim and fill test, resulted in − 0.836 (95% CI − 1.017 to − 0.655). The meta-regression analysis showed that mean age, H&Y, UPDRS, and disease duration did not influence the stride length difference between individuals with PD and healthy controls (Table 1).

Standardized mean differences on stride length between Parkinson and healthy individuals. CI confidence interval, Std diff standardized difference.
Meta-analysis of cadence
Data concerning cadence were available from 50 studies and 51 combination pairs, which compare cadence of PD versus healthy group, in a total of 1936 participants. Meta-analysis showed that cadence is approximately 1.75 step min−1 higher in PD compared with healthy groups (ES: − 0.212; 95% CI − 0.377 to − 0.048; p = 0.011; I2: 66%) (Fig. 4). The analysis of publication bias for this outcome showed no significant bias (p = 0.074).

Standardized mean differences on gait cadence between Parkinson and healthy individuals. CI confidence interval, Std diff standardized difference.
Subgroup analysis of studies, which evaluated cadence using free (ground) walking or treadmill, evidenced that this criterion influences the gait differences between PD and healthy groups. Studies adopting free walking strategy to evaluate this variable demonstrated that cadence is 1.86 step min−1 higher in PD subjects compared to healthy groups (ES: − 0.228; 95% CI − 0.402 to − 0.054; p < 0.001; I2: 67%). In contrast, studies using the treadmill to evaluate the cadence (3 studies) did not show a difference between the cadence of PD and healthy groups (ES: − 0.023; 95% CI − 0.550 to 0.503; p = 0.931; I2: 52%). Furthermore, the meta-regression analysis results demonstrated that mean age, H&Y, UPDRS, and disease duration do not influence the cadence difference between PD subjects and healthy groups (Table 1).
Meta-analysis of step width
Data concerning step width were available from 18 studies and 19 combination pairs, which compare the step width of PD versus healthy group, in 628 participants. Meta-analysis demonstrated that step width did not differ between PD and healthy groups (ES: 0.104; 95% CI − 0.153 to 0.361; p = 0.426; I2: 59%) (Supplementary material 1.6) The analysis of publication bias for this outcome showed no significant bias (p = 0.327). Besides, the meta-regression analysis showed that mean age, H&Y, UPDRS, and disease duration do not influence the step width difference between individuals with PD and healthy controls (Table 1).
Meta-analysis of double support time
Data concerning double support time were available from 15 studies and 16 combination pairs, which compared the double support time of PD versus control groups, in a total of 562 participants. Meta-analysis showed that double support time is approximately 1.79% longer in PD compared with healthy groups (ES: 0.489; 95% CI 0.137 to 0.841; p < 0.001; I2: 73%) (Supplementary material 1.7). The analysis of publication bias for this outcome showed no significant bias (p = 0.260). The meta-regression analysis showed that mean age, H&Y, UPDRS, and disease duration do not influence the double support time difference between PD subjects and healthy groups (Table 1).
Meta-analysis of single support time
Data concerning single support were available from 10 studies, which compared single support time between individuals with PD versus healthy group, in a total of 366 participants. Meta-analysis demonstrated that single support time did not differ between PD and healthy groups (ES: 0.273; 95% CI − 0.204 to 0.750; p = 0.262; I2: 83%) (Supplementary material 1.8). The analysis of publication bias for this outcome showed no significant bias (p = 0.720). In addition, the meta-regression analysis showed that mean age, H&Y, UPDRS, and disease duration do not influence the single support time difference between PD subjects and healthy groups (Table 1).
Meta-analysis of swing time
Data concerning swing phase time were available from 11 studies, which compare the swing time of PD versus healthy group, in 661 participants. Meta-analysis showed that swing time is 1.76% reduced in PD compared with healthy groups (ES: − 0.715; 95% CI − 1.096 to − 0.334; p < 0.001; I2: 79%) (Supplementary material 1.9). The analysis of publication bias for this outcome showed no significant bias (p = 0.087).
According to the results of meta-regression analysis, mean age and disease duration do not influence the swing time difference between PD subjects and healthy groups. On the other hand, the disease stage evaluated by H&Y plays a significant role in the swing phase time difference between PD and healthy groups (β: 2.535; 95% CI 0.084–4.987 p = 0.042; R2 = 0.57). Therefore, the higher the H&Y values, the higher is the difference between swing phase time in PD compared with healthy groups. Conversely, the UPDRS exert a significant influence on the swing phase difference between PD and healthy groups (β: − 0.149; 95% CI − 0.247 to − 0.052 p = 0.002; R2 = 0.67). The difference between PD and healthy groups decreased with increasing severity of PD (Table 1).
Meta-analysis of hip ROM
Data concerning hip ROM were available from 3 studies, which compare hip ROM of PD versus healthy group in 76 participants. Meta-analysis demonstrated that hip ROM is 5.29 degrees reduced in PD compared with healthy groups (ES: − 0.860; 95% CI − 1.333 to − 0.388 p < 0.001; I2: 0%) (Supplementary material 2.0).
Meta-analysis of knee ROM
Data concerning knee ROM were available from 2 studies, which compare knee ROM of PD versus healthy groups in 52 participants. Meta-analysis showed that knee ROM did not differ between PD and healthy groups (ES: − 1.033; 95% CI − 2.564 to 0.498; p = 0.186; I2: 82%) (Supplementary material 2.1).
Meta-analysis of ankle ROM
Data concerning ankle ROM were available from 3 studies, which compare ankle ROM of PD versus control groups, in a total of 76 participants. Meta-analysis demonstrated that ankle ROM did not differ between PD and healthy groups (ES: − 0.216; 95% CI − 0.896 to 465; p = 0.534; I2: 53%) (Supplementary material 2.2).
Meta-analysis of hip angle at initial contact
Data concerning hip angle at initial contact were available from 3 studies, which compared hip angle at initial contact of PD versus control groups in a total of 70 participants. Meta-analysis demonstrated that hip angle at initial contact did not differ between PD and healthy groups (ES: − 1.023; 95% CI − 2.291 to 0.245; p = 0.114; I2: 83%) (Supplementary material 2.3).
Meta-analysis of knee angle at initial contact
Data concerning knee angle at initial contact were available from 3 studies, which compared the knee angle at initial contact of PD versus healthy group, in a total of 70 participants. Meta-analysis showed that knee angle at initial contact did not differ between PD and healthy groups (ES: 0.210; 95% CI − 0.395 to 0.814; p = 0.496; I2: 35%) (Supplementary material 2.4).
Meta-analysis of ankle angle at initial contact
Data concerning ankle angle at initial contact were available from 3 studies, which compared the ankle angle at initial contact of PD versus control groups in a total of 70 participants. Meta-analysis showed that the ankle angle at initial contact did not differ between PD and healthy groups (ES: 0.188; 95% CI − 0.290 to 0.666; p = 0.440; I2: 0%) (Supplementary material 2.5).
Discussion
To the best of our knowledge, this is the first meta-analysis of published studies regarding the spatiotemporal and lower limb angles during SSWS on people with PD compared with healthy control subjects. The main results agree with our hypotheses showing that SSWS, stride length, cadence, double support, swing time and sagittal hip angle were different in people with PD compared with healthy control participants. In some cases, the method of evaluation of walk can influence these variables. Furthermore, the present study strongly contributes to the literature regarding PD gait characteristics, addressing measures that were not yet elucidated, such as (1) speed is 0.17 m s−1 reduced, (2) stride length is 0.16 m reduced, (3) cadence is 1.75 step min−1 higher; (4) double support time is 1.79% longer, (5) swing time is 1.76% reduced, and (vi) hip sagittal ROM is 5 degrees reduced in people with PD compared with the healthy control group.
Spatiotemporal variables
Walking speed is an essential parameter of functional activities in daily life. Also, the walking speed test is a practical method useful for monitoring people's mobility with PD24. In this review, using 69 studies, we observed that PD SSWS is 0.17 m s−1 slower than healthy control group. Possibly, the bradykinesia and rigidity associated with physical inactivity may be a contributing factor, but the studies did not measure these outcomes25. The slower walking speeds are associated with mortality, hospitalization, frailty, and risk of falling24. Creaby and Cole14 revealed that reduced walking speeds denote a compensation strategy to avoid fallings, causing alterations, especially in spatiotemporal variables in individuals with PD13.
Gait speed is strictly related to stride length and cadence. Our systematic review with metanalysis showed that individuals with PD walk slower than healthy controls through a largely reduced stride length (0.16 m) despite showing higher cadence. Therefore, the relation stride length versus cadence is altered in PD which disagrees with previous findings that found this relationship unaltered26. Importantly, the cadence is similar between PD and healthy control during walking on the treadmill. The similarity is probably due to imposed treadmill speed (less-ecological task). These different results due to walking conditions need to be considered during rehabilitation interventions. One consequence of these changes is the reduced external mechanical work, mainly due to shorter stride length and reduced hip excursion10.
The findings of double support and swing time may be associated with gait instability in people with PD. In Peppe and collaborators’ study25, the long double support time was attributed to an inability to transfer weight in preparation for stepping adequately. In addition, swing time was reduced in people with PD compared with healthy control group, probably due to reduced walking speed, reduced stride length and higher cadence and double support time, resulting in reduced dynamical stability of gait in PD. Further, we found that level of disease progression affected the swing time. While the general scale of disease progression (H&Y) shows an increase in differences for swing time between PD individuals and healthy controls according to the severity of motor symptoms, the motor scale of disease progression (UPDRS) surprisingly showed a reduction of these differences according to the disease severity. This intriguing finding needs further consideration in future studies to understand the causes of this discrepancy. It has been suggested to include more sensitive measurements to associate the PD stage and their consequences on gait pattern27. Although double support time and swing time have been impaired, the step width remains unchanged, showing that lateral margins of stability are maintained in PD. These temporal alterations of gait are considered strategies of the neural system to reduce the risk of falls, allowing an enhanced postural control28.
The walking speed was reduced between individuals with PD and without PD in both free and treadmill walking conditions. Despite the reduction was 0.17 m s−1 in overground and 0.13 m s−1 in treadmill, both conditions can detect differences in that important marker of functionality. In general, the SSWS is reduced in treadmill compared with overground because most protocols using treadmill does not allow people to select their speed initially but instead choose one for them and then let them go up down from there29.
Mostly, gait alterations in people with PD occur at the early disease stage, evolving from uni to bilateral alteration13. The participants evaluated from the studies were somewhat homogeneous and, therefore, resulting in poor relation between disease stage and gait performance. Future studies in this field should include advanced staging and young PD as well as analysis with ON and OFF state of medication13.
Angular variables
In addition to the spatiotemporal variables, angular measurements are relevant to characterize the walking pattern. The pelvic rotation, tilt and lateral oscillation, knee flexion in stance phase, foot on heel-strike and toe-off are determinants to recovery energy and avoid compensations during walking30. The present study showed that only the range of hip motion was reduced (5°) during SSWS for individuals with PD compared to controls, while the knee and ankle ROM remained unaltered. The reduced hip excursion is probably accompanied by a reduced knee extension in the terminal stance phase10. Additionally, there is a reduced activity of gastrocnemius medial and higher activity of tibialis anterior, accompanied by a higher co-contraction of these ankle muscles during gait12. These changes influence adequately transfer weight in preparation for stepping and it can reflect in a higher metabolic cost of walking10,12,30.
No differences in knee and ankle sagittal ROM and hip, knee and ankle angles at initial contact were found between people with PD compared with healthy control group. However, DiPaola et al.10 found that knee ROM is critical, influencing the pendular mechanism of walking. Few studies analyzed these variables, therefore precluding the meta-regression analysis. The walking parameters in individuals with PD may be improved, and the variables that showed alterations in the present study should be the focus of rehabilitation and exercise interventions31,32. For example, some interventions like dance and Nordic walking have the potential to improve gait biomechanics and energetics in people with PD. These exercise modalities combine auditory stimulus, rhythmicity with direction changes, and large joint excursions33,34.
A significant contribution of the present analysis to the literature is comparing gait between people with relatively low disease severity in ON state of medication and healthy control group, which showed quantitatively how the variables differ from people with PD and healthy group. It was possible to affirm that SSWS, stride length, swing time, hip sagittal ROM are reduced and cadence and double support are higher during gait in people with PD. These findings can support health professionals to monitor the interventions to improve the gait parameters.
Finally, we highlight the first systematic review with sensitivity analysis and meta-regression that measured the differences in the gait of people with PD compared with healthy control groups. The high heterogeneity of some comparisons is a limitation of the present study. However, in general, the studies showed high methodological quality. Besides, more original studies are needed to explore the possible alterations in angular parameters. Our findings using treadmill protocols to evaluate gait biomechanics in PD individuals are preliminary, and further research is required to address this issue. This review selected studies with the ON phase of medication because these populations usually do the daily life in this phase of medication. Thus, more investigations are needed to explore the role of medication on gait.
Conclusion
The present meta-analysis showed that people with PD have differences in gait characteristics compared with healthy control group. Different evaluation methods can influence some biomechanical parameters, though the PD’s main alterations are sensible in overground and treadmill setups. Based on our results, the subjects were homogeneous and meta-regression analysis showed that age, disease duration, H&Y and UPDRS, in general, did not exert influence over walking biomechanics.
References
Schneider, S. A. & Alcalay, R. N. Neuropathology of genetic synucleinopathies with parkinsonism: review of the literature. Mov. Disord. 32, 1504–1523. https://doi.org/10.1002/mds.27193 (2017).
Peterson, D. S. & Horak, F. B. Neural control of walking in people with parkinsonism. Physiology 31, 95–107. https://doi.org/10.1152/physiol.00034.2015 (2016).
Dorsey, E. R. et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 68, 84–86. https://doi.org/10.1212/01.wnl.0000247740.47667.03 (2007).
Pringsheim, T., Jette, N., Frolkis, A. & Steeves, T. D. The prevalence of Parkinson’s disease: a systematic review and meta-analysis. Mov. Disord. 29, 1583–1590. https://doi.org/10.1002/mds.25945 (2014).
Ascherio, A. & Schwarzschild, A. M. D. The epidemiology of Parkinson’s disease: risk factors and prevention. Lancet Neurol. 15, 1257–1272. https://doi.org/10.1016/S1474-4422(16)30230-7 (2016).
Elbaz, A., Carcaillon, L., Kab, S. & Moisan, F. Epidemiology of Parkinson’s disease. Rev. Neurol. 172, 14–26. https://doi.org/10.1016/j.neurol.2015.09.012 (2016).
Sveinbjornsdottir, S. The clinical symptoms of Parkinson’s disease. J. Neurochem. 139, 318–324. https://doi.org/10.1111/jnc.13691 (2016).
Morris, M. E., Iansek, R., Matyas, T. A. & Summers, J. J. Ability to modulate walking cadence remains intact in Parkinson’s disease. J. Neurol. Neurosurg. 57, 1532–1534. https://doi.org/10.1136/jnnp.57.12.1532 (1994).
Van Emmerik, R. E. A., Wagenaar, R. C., Winogrodzka, A. & Wolters, E. C. Identification of axial rigidity during locomotion in Parkinson disease. Arch. Phys. Med. Rehabil. 2, 186–191. https://doi.org/10.1016/S0003-9993(99)90119-3 (1999).
Dipaola, M. et al. Mechanical energy recovery during walking in patients with Parkinson disease. PLoS ONE 11, e0156420. https://doi.org/10.1371/journal.pone.0156420 (2016).
Carpinella, I. et al. Locomotor function in the early stage of Parkinson’s disease. IEEE Trans. Rehabil. Eng. 15, 543–551. https://doi.org/10.1109/TNSRE.2007.908933 (2007).
Monteiro, E. P., Wind, L. B., Martinez, F. G., Pagnussat, A. S. & Peyré-Tartaruga, L. A. Aspectos biomecânicos da locomoção de pessoas com doença de Parkinson: revisão narrativa. RBCE 39, 450–457. https://doi.org/10.1016/j.rbce.2016.07.003 (2017).
Mirelman, A. et al. Gait impairments in Parkinson’s disease. Lancet Neurol. 18, 697–708. https://doi.org/10.1016/S1474-4422(19)30044-4 (2019).
Creaby, M. W. & Cole, M. H. Gait characteristics and falls in Parkinson’s disease: a systematic review and meta-analysis. Parkinsonism Relat. Disord. 57, 1–8. https://doi.org/10.1016/j.parkreldis.2018.07.008 (2018).
Stroup, D. F. et al. Meta-analysis of observational studies in epidemiology a proposal for reporting. JAMA Netw. Open 283, 2008–2012. https://doi.org/10.1001/jama.283.15.2008 (2000).
Higgins, J., Deeks, J., & Altman, D. Cochrane handbook for systematic reviews of interventions, version 5.1. The Cochrane Collaboration (2011).
Downs, S. H. & Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 52, 377–384. https://doi.org/10.1136/jech.52.6.377 (1998).
Bates, A. V. & Alexander, C. M. Kinematics and kinetics of people who are hypermobile. A systematic review. Gait Posture 41, 361–369. https://doi.org/10.1016/j.gaitpost.2015.01.009 (2015).
Dixon, C. J., Knight, T., Binns, E., Ihaka, B. & O’brien, D. Clinical measures of balance in people with type two diabetes: a systematic literature review. Gait Posture 58, 325–332. https://doi.org/10.1016/j.gaitpost.2017.08.022 (2017).
Mousavi, S. H. et al. Kinematic risk factors for lower limb tendinopathy in distance runners: a systematic review and meta-analysis. Gait Posture 69, 13–24. https://doi.org/10.1016/j.gaitpost.2019.01.011 (2019).
Ratcliffe, E., Pickering, S., McLean, S. & Lewis, J. Is there a relationship between subacromial impingement syndrome and scapular orientation? A systematic review. Br. J. Sports Med. 48, 1251–1256. https://doi.org/10.1136/bjsports-2013-092389 (2014).
Egger, M., Davey Smith, G., Schneider, M. & Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 315, 629–634 (1997).
Duval, S. & Tweedie, R. Trim and fill: a simple Funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 56, 455–463. https://doi.org/10.1111/j.0006-341x.2000.00455.x (2000).
Lindemann, U. Spatiotemporal gait analysis of older persons in clinical practice and research: Which parameters are relevant?. Z. Gerontol. Geriatr. 53, 1–7. https://doi.org/10.1007/s00391-019-01520-8 (2019).
Peppe, A., Chiavalon, C., Pasqualetti, P., Crovato, D. & Caltagirone, C. Does gait analysis quantify motor rehabilitation efficacy in Parkinson’s disease patients?. Gait Posture 26, 452–462. https://doi.org/10.1016/j.gaitpost.2006.11.207 (2007).
Morris, M., Iansek, R., Matyas, T. & Summers, J. Abnormalities in the stride length-cadence relation in parkinsonian gait. Mov. Disord. 13, 61–69. https://doi.org/10.1002/mds.870130115 (1998).
Bloem, B. R. et al. Measurement instruments to assess posture, gait, and balance in Parkinson’s disease: critique and recommendations. Mov. Disord. 31, 1342–1355. https://doi.org/10.1002/mds.26572 (2016).
Owings, M. & Grabiner, D. Variability of step kinematics in young and older adults. Gait Posture 20, 26–29. https://doi.org/10.1016/S0966-6362(03)00088-2 (2004).
Malatesta, D., Canepa, M. & Fernandez, A. The effect of treadmill and overground walking on preferred walking speed and gait kinematics in healthy, physically active older adults. Eur. J. Appl. Physiol. 117, 1833–1843. https://doi.org/10.1007/s00421-017-3672-3 (2017).
Saunders, J. B. D. M., Inman, V. T. & Eberhart, H. D. The major determinants in normal and pathological gait. J. Bone Joint Surg. Am. 35, 543–558 (1953).
Shu, H. F. et al. Aerobic exercise for Parkinson’s disease: a systematic review and meta-analysis of randomized controlled trials. PLoS ONE 9, e100503. https://doi.org/10.1371/journal.pone.0100503 (2014).
LaHue, S. C., Comella, C. L. & Tanner, C. M. The best medicine? The influence of physical activity and inactivity on Parkinson’s disease. Mov. Disord. 31, 444–454. https://doi.org/10.1002/mds.26728 (2016).
Sharp, K. & Hewitt, J. Dance as an intervention for people with Parkinson’s disease: a systematic review and meta-analysis. Neurosci. Biobehav. Rev. 47, 445–456. https://doi.org/10.1016/j.neubiorev.2014.09.009 (2014).
Gougeon, M. A., Zhou, L. & Nantel, J. Nordic walking improves trunk stability and gait spatial-temporal characteristics in people with Parkinson disease. NeuroRehabilitation 41, 205–210. https://doi.org/10.3233/NRE-171472 (2017).
Arias, P. & Cudeiro, J. Effects of rhythmic sensory stimulation (auditory, visual) on gait in Parkinson’s disease patients. Exp. Brain. Res. 186, 589–601. https://doi.org/10.1007/s00221-007-1263-y (2008).
Azulay, J. P. et al. Visual control of locomotion in Parkinson’s disease. Brain 122, 111–120. https://doi.org/10.1093/brain/122.1.111 (1999).
Azulay, J. P., Mesure, S., Amblard, B. & Pouget, J. Increased visual dependence in Parkinson’s disease. Percept. Mot. Skills 95, 1106–1114. https://doi.org/10.2466/pms.2002.95.3f.1106 (2002).
Bhatt, H., Pieruccini-Faria, F. & Almeida, Q. J. Dynamics of turning sharpness influences freezing of gait in Parkinson’s disease. Parkinsonism Relat. Disord. https://doi.org/10.1016/j.parkreldis.2012.09.006 (2013).
Blin, O., Ferrandez, A. M. & Serratrice, G. Quantitative analysis of gait in Parkinson patients: increased variability of stride length. J. Neurol. Sci. 98, 91–97. https://doi.org/10.1016/0022-510X(90)90184-O (1990).
Bond, J. M. & Morn’s, M. Goal-directed secondary motor tasks: their effects on gait in subjects with Parkinson disease. Arch. Phys. Med. Rehabil. 81, 110–116. https://doi.org/10.1016/S0003-9993(00)90230-2 (2000).
Brown, L. A., Bruin, N., Doan, J. B., Suchowersky, O. & Hu, B. Novel challenges to gait in Parkinson’s disease: the effect of concurrent music in single- and dual-task contexts. Arch. Phys. Med. Rehabil. 90, 1578–1583. https://doi.org/10.1016/j.apmr.2009.03.009 (2009).
Bugalho, P., Alves, L. & Miguel, R. Gait dysfunction in Parkinson’s disease and normal pressure hydrocephalus: a comparative study. J. Neural. Transm. 120, 1201–1207. https://doi.org/10.1007/s00702-013-0975-3 (2013).
Caetano, M. J., Gobbi, L. T., Sanchez-Arias, M. D. E. R., Stella, F. & Gobbi, S. Effects of postural threat on walking features of Parkinson’s disease patients. Neurosci. Lett. 52, 136–140. https://doi.org/10.1007/978-3-319-48980-3_12 (2009).
Castagna, A. et al. Quantitative gait analysis in Parkinson’s disease: Possible role of dystonia. Mov. Disord. 31, 1720–1728. https://doi.org/10.1002/mds.26672 (2016).
Chen, S. W. et al. Quantification and recognition of parkinsonian gait from monocular video imaging using kernel-based principal component analysis. Biomed. Eng. Online https://doi.org/10.1186/1475-925X-10-99 (2011).
Cole, M. H., Silburn, P. A., Wood, J. M., Worringham, C. J. & Kerr, G. K. Falls in Parkinson’s disease: kinematic evidence for impaired head and trunk control. Mov. Disord. 25, 2369–2378. https://doi.org/10.1002/mds.23292 (2010).
Cole, M. H., Naughton, G. A. & Silburn, P. A. Neuromuscular impairments are associated with impaired head and trunk stability during gait in Parkinson fallers. Neurorehabil. Neural Repair. 31, 34–47. https://doi.org/10.1177/1545968316656057 (2017).
Danoudis, M. & Iansek, R. Gait in Huntington’s disease and the stride length-cadence relationship. BMC Neurol. https://doi.org/10.1186/s12883-014-0161-8 (2014).
De Nunzio, A. M., Grasso, M., Nardone, A., Godi, M. & Schieppati, M. Alternate rhythmic vibratory stimulation of trunk muscles affects walking cadence and velocity in Parkinson’s disease. Clin. Neurophysiol. 121, 240–247. https://doi.org/10.1016/j.clinph.2009.10.018 (2010).
Del Din, S., Godfrey, A., Galna, B., Lord, S. & Rochester, L. Free-living gait characteristics in ageing and Parkinson’s disease: impact of environment and ambulatory bout length. J. Neuroeng. Rehabil. https://doi.org/10.1186/s12984-016-0154-5 (2016).
Demonceau, M. et al. Contribution of a trunk accelerometer system to the characterization of gait in patients with mild-to-moderate Parkinson’s disease. IEEE J. Biomed. Health. 19, 1803–1808. https://doi.org/10.1109/jbhi.2015.2469540 (2015).
Dillmann, U. et al. Principal component analysis of gait in Parkinson’s disease: relevance of gait velocity. Gait Posture 39, 882–887. https://doi.org/10.1016/j.gaitpost.2013.11.021 (2014).
Ebersbach, G. et al. Comparative analysis of gait in Parkinson’s disease, cerebellar ataxia and subcortical arteriosclerotic encephalopathy. Brain 122, 1349–1355. https://doi.org/10.1093/brain/122.7.1349 (1999).
Egerton, T., Williams, D. R. & Iansek, R. Comparison of gait in progressive supranuclear palsy, Parkinson’s disease and healthy older adults. BMC Neurol. https://doi.org/10.1186/1471-2377-12-116 (2012).
Eltoukhy, M. et al. Microsoft Kinect can distinguish differences in over-ground gait between older persons with and without Parkinson’s disease. Med. Eng. Phys. 44, 1–7. https://doi.org/10.1016/j.medengphy.2017.03.007 (2017).
Esser, P., Dawes, H., Collett, J. & Howells, K. Insights into gait disorders: walking variability using phase plot analysis, Parkinson’s disease. Gait Posture 38, 648–652. https://doi.org/10.1016/j.gaitpost.2013.02.016 (2012).
Esser, P., Dawes, H., Collett, J., Feltham, M. G. & Howells, K. Assessment of spatio-temporal gait parameters using inertial measurement units in neurological populations. Gait Posture 34, 558–560. https://doi.org/10.3791/51878 (2011).
Frenkel-Toledo, S. et al. Effect of gait speed on gait rhythmicity in Parkinson’s disease: variability of stride time and swing time respond differently. J. Neuroeng. Rehabil. https://doi.org/10.1186/1743-0003-2-23 (2005).
Frenkel-Toledo, S. et al. Treadmill walking as an external pacemaker to improve gait rhythm and stability in Parkinson’s disease. Mov. Disord. 20, 1109–1114. https://doi.org/10.1002/mds.20507 (2005).
Galletly, R. & Brauer, S. G. Does the type of concurrent task affect preferred and cued gait in people with Parkinson’s disease?. Aust. J. Physiother. 51, 175–180. https://doi.org/10.1016/S0004-9514(05)70024-6 (2005).
Hackney, M. E. & Earhart, G. M. The effects of a secondary task on forward and backward walking in Parkinson’s disease. Neurorehabil. Neural Repair. 24, 97–106. https://doi.org/10.1177/1545968309341061 (2010).
Hackney, M. E. & Earhart, G. M. Backward walking in Parkinson’s disease. Mov. Disord. 24, 218–223. https://doi.org/10.1002/mds.22330 (2009).
Hausdorff, J. M. et al. Rhythmic auditory stimulation modulates gait variability in Parkinson’s disease. Eur. J. Neurosci. 26, 2369–2375. https://doi.org/10.1111/j.1460-9568.2007.05810.x (2007).
Jaywant, A., Shiffrar, M., Roy, S. & Cronin-Golomb, A. Impaired perception of biological motion in Parkinson’s disease. Neuropsychology 30, 720–730. https://doi.org/10.1037/neu0000276 (2016).
Kimmeskamp, S. & Hennig, E. M. Heel to toe motion characteristics in Parkinson patients during free walking. Clin. Biomech. 16, 806–812. https://doi.org/10.1016/s0268-0033(01)00069-9 (2001).
Kincses, P. et al. Association of gait characteristics and depression in patients with Parkinson’s disease assessed in goal-directed locomotion task. Parkinsons Dis. https://doi.org/10.1155/2017/6434689 (2017).
Latt, M. D., Menz, H. B., Fung, V. S. & Lord, S. R. Acceleration patterns of the head and pelvis during gait in older people with Parkinson’s disease: a comparison of fallers and nonfallers. J. Gerontol. A Biol. Sci. Med. Sci. 64, 700–706. https://doi.org/10.1093/gerona/glp009 (2009).
Lewis, G. N., Byblow, W. D. & Walt, S. E. Stride length regulation in Parkinson’s disease: the use of extrinsic, visual cues. Brain 123, 2077–2090. https://doi.org/10.1093/brain/123.10.2077 (2000).
Lin, H. et al. Quantitative measurement of Parkinsonian gait from walking in monocular image sequences using a centroid tracking algorithm. Med. Biol. Eng. Comput. 54, 485–496. https://doi.org/10.1007/s11517-015-1335-2 (2016).
Lohnes, C. A. & Earhart, G. M. The impact of attentional, auditory, and combined cues on walking during single and cognitive dual tasks in Parkinson disease. Gait Posture 33, 478–483. https://doi.org/10.1016/j.gaitpost.2010.12.029 (2011).
Lowry, K. A., Smiley-Oyen, A. L., Carrel, A. J. & Kerr, J. P. Walking stability using harmonic ratios in Parkinson’s disease. Mov. Disord. 24, 261–267. https://doi.org/10.1002/mds.22352 (2009).
Maggioni, M. A. et al. Energy cost of spontaneous walking in Parkinson’s disease patients. Neurol. Sci. 33, 779–784. https://doi.org/10.1007/s10072-011-0827-6 (2012).
Mak, M. K. Reduced step length, not step length variability is central to gait hypokinesia in people with Parkinson’s disease. Clin. Neurol. Neurosurg. 115, 587–590. https://doi.org/10.1016/j.clineuro.2012.07.014 (2013).
Mak, M. K., Yu, L. & Hui-Chan, C. W. The immediate effect of a novel audio-visual cueing strategy (simulated traffic lights) on dual-task walking in people with Parkinson’s disease. Eur. J. Phys. Rehabil. Med. 49, 153–159 (2013).
McNeely, M. E., Duncan, R. P. & Earhart, G. M. Medication improves balance and complex gait performance in Parkinson disease. Gait Posture 36, 144–148. https://doi.org/10.1016/j.gaitpost.2012.02.009 (2012).
Morris, M. E., Iansek, R., Matyas, T. A. & Summers, J. J. The pathogenesis of gait hypokinesia in Parkinson’s disease. Brain 117, 1169–1181. https://doi.org/10.1093/brain/117.5.1169 (1994).
Morris, M., Iansek, R., McGinley, J., Matyas, T. & Huxham, F. Three-dimensional gait biomechanics in Parkinson’s disease: evidence for a centrally mediated amplitude regulation disorder. Mov. Disord. 20, 40–50. https://doi.org/10.1002/mds.20278 (2005).
O’Shea, S., Morris, M. E. & Iansek, R. Dual task interference during gait in people with Parkinson disease: effects of motor versus cognitive secondary tasks. Phys. Ther. 82, 888–897. https://doi.org/10.1093/ptj/82.9.888 (2002).
Pieruccini-Faria, F. et al. Evaluating the acute contributions of dopaminergic replacement to gait with obstacles in Parkinson’s disease. J. Mot. Behav. 45, 369–380. https://doi.org/10.1080/00222895.2013.810139 (2013).
Rabin, E. et al. Parkinsonian gait ameliorated with a moving handrail, not with a banister. Arch. Phys. Med. Rehabil. 96, 735–741. https://doi.org/10.1016/j.apmr.2014.07.427 (2015).
Rafferty, M. R. et al. Effects of 2 years of exercise on gait impairment in people with parkinson disease: the PRET-PD randomized trial. J. Neurol. Phys. Ther. 41, 21–30. https://doi.org/10.1097/NPT.0000000000000163 (2017).
Rochester, L. et al. Cholinergic dysfunction contributes to gait disturbance in early Parkinson’s disease. Brain 135, 2779–2788. https://doi.org/10.1093/brain/aws2079 (2012).
Roiz, R. M. et al. Gait analysis comparing Parkinson’s disease with healthy elderly subjects. Arq. Neuropsiquiatr. 68, 81–86. https://doi.org/10.1590/S0004-282X2010000100018 (2010).
Salazar, R. D. et al. Dual tasking in Parkinson’s disease: cognitive consequences while walking. Neuropsychology 31, 613–623. https://doi.org/10.1037/neu0000331 (2017).
Santos, P. C. et al. Effects of leg muscle fatigue on gait in patients with Parkinson’s disease and controls with high and low levels of daily physical activity. Gait Posture 47, 86–91. https://doi.org/10.1016/j.gaitpost.2016.04.002 (2016).
Sofuwa, O. et al. Quantitative gait analysis in Parkinson’s disease: comparison with a healthy control group. Arch. Phys. Med. Rehabil. 86, 1007–1013. https://doi.org/10.1016/j.apmr.2004.08.012 (2005).
Stolze, H. et al. Comparative analysis of the gait disorder of normal pressure hydrocephalus and Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 70, 289–297. https://doi.org/10.1136/jnnp.70.3.289 (2001).
Tramonti, C. et al. Gait dynamics in Pisa syndrome and camptocormia: the role of stride length and hip kinematics. Gait Posture 57, 130–135. https://doi.org/10.1016/j.gaitpost.2017.05.029 (2017).
Trojaniello, D. et al. Estimation of step-by-step spatio-temporal parameters of normal and impaired gait using shank-mounted magneto-inertial sensors: application to elderly, hemiparetic, parkinsonian and choreic gait. J. Neuroeng. Rehabil. https://doi.org/10.1186/1743-0003-11-152 (2014).
Turcato, A. M. et al. Abnormal gait pattern emerges during curved trajectories in high-functioning Parkinsonian patients walking in line at normal speed. PLoS ONE 13, e0197264. https://doi.org/10.1371/journal.pone.0197264 (2018).
Van Wegen, E. et al. The effects of visual rhythms and optic flow on stride patterns of patients with Parkinson’s disease. Parkinsonism Relat. Disord. 12, 21–27. https://doi.org/10.1016/j.parkreldis.2005.06.009 (2006).
Vaugoyeau, M., Viallet, F., Mesure, S. & Massion, J. Coordination of axial rotation and step execution: deficits in Parkinson’s disease. Gait Posture 18, 150–157. https://doi.org/10.1016/S0966-6362(03)00034-1 (2003).
Vieregge, P., Stolze, H., Klein, C. & Heberlein, L. Gait quantitation in Parkinson’s disease-locomotor disability and correlation to clinical rating scales. J. Neural. Transm. (Vienna) 104, 237–248. https://doi.org/10.1007/BF01273184 (1997).
Vitorio, R. et al. Visual cues and gait improvement in Parkinson’s disease: Which piece of information is really important?. Neuroscience 277, 273–280. https://doi.org/10.1016/j.neuroscience.2014.07.024 (2014).
Vitório, R. et al. The role of vision in Parkinson’s disease locomotion control: free walking task. Gait Posture 35, 175–179. https://doi.org/10.1016/j.gaitpost.2011.09.002 (2012).
Wahid, F. A. Multiple regression approach to normalization of spatiotemporal gait Features. J. Appl. Biomech. 32, 128–139. https://doi.org/10.1123/jab.2015-0035 (2016).
Willems, A. M. et al. The use of rhythmic auditory cues to influence gait in patients with Parkinson’s disease, the differential effect for freezers and non-freezers, an explorative study. Disabil. Rehabil. 28, 721–728. https://doi.org/10.1080/09638280500386569 (2006).
Xu, H., Merryweather, A., Foreman, K. B., Zhao, J. & Hunt, M. Dual-task interference during gait on irregular terrain in people with Parkinson’s disease. Gait Posture https://doi.org/10.1016/j.gaitpost.2018.04.027 (2018).
Yang, Y. R., Lee, Y. Y., Cheng, S. J., Lin, P. Y. & Wang, R. Y. Relationships between gait and dynamic balance in early Parkinson’s disease. Gait Posture 27, 611–615. https://doi.org/10.1016/j.gaitpost.2007.08.003 (2008).
Zhou, L., Gougeon, M. A. & Nantel, J. Nordic walking improves gait power profiles at the knee joint in Parkinson’s disease. J. Aging Phys. Act 26, 84–88. https://doi.org/10.1123/japa.2017-0031 (2018).
Zijlstra, W., Rutgers, A. W. & Van Weerden, T. W. Voluntary and involuntary adaptation of gait in Parkinson’s disease. Gait Posture 7, 53–63. https://doi.org/10.1016/s0966-6362(97)00037-4 (1998).
Vitorio, R., Pieruccini-Faria, F., Stella, F., Gobbi, S. & Gobbi, L. T. Effects of obstacle height on obstacle crossing in mild Parkinson’s disease. Gait Posture 31, 143–146. https://doi.org/10.1016/j.gaitpost.2009.09.011 (2010).
Zhang, S. et al. Age- and Parkinson’s disease-related evaluation of gait by General Tau theory. Exp. Brain Res. 234, 2829–2840. https://doi.org/10.1007/s00221-016-4685-6 (2016).
Acknowledgements
We are grateful to the Locomotion Group of the Universidade Federal do Rio Grande do Sul for discussions and comments. We extend our acknowledgments to all Brazilian citizens who, through the payment of their taxes, allow so many researchers to improve their scientific knowledge in public graduate programs.
Funding
This work was supported by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Brazil, Call Capes/Print 47/2017 – UFRGS); Ministério da Ciência, Tecnologia e Inovação—Conselho Nacional de Desenvolvimento Científico e Tecnológico—CNPq (Productivity grant to Prof. L.A. Peyré-Tartaruga); and Fundação de Amparo à Pesquisa do Estado do Rio Grande do Sul (Fapergs, Call FAPERGS/MS/CNPq/SESRS 03/2017 – PPSUS; 17/2551-0001464-2).
Author information
Authors and Affiliations
Contributions
A.P.J.Z.: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Software; Visualization; Roles/writing—original draft; Writing—review and editing, final approval of the version to be submitted. E.S.d.S.: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Software; Visualization; Roles/writing—original draft; Writing—review and editing, final approval of the version to be submitted. R.R.C.: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Software; Visualization; Roles/writing—original draft; Writing—review and editing, final approval of the version to be submitted. E.P.-M.: Formal analysis; Roles/writing—original draft; Writing—review and editing, final approval of the version to be submitted. I.O.d.S.: Data curation; Investigation; Methodology; Software; L.F.M.K.: Formal analysis; Roles/writing—original draft; Writing—review and editing, final approval of the version to be submitted. L.A.P.-T.: Conceptualization; Formal analysis; Funding acquisition; Project administration; Resources; Supervision; Visualization; Roles/writing—original draft; Writing—review and editing, final approval of the version to be submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Zanardi, A.P.J., da Silva, E.S., Costa, R.R. et al. Gait parameters of Parkinson’s disease compared with healthy controls: a systematic review and meta-analysis. Sci Rep 11, 752 (2021). https://doi.org/10.1038/s41598-020-80768-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-80768-2
- Springer Nature Limited
This article is cited by
-
Stride width and postural stability in frontal gait disorders and Parkinson’s disease
Journal of Neurology (2024)
-
Impaired dual-task gait in Parkinson’s disease is associated with brain morphology changes
Journal of Neural Transmission (2024)
-
Early-onset and late-onset Parkinson’s disease exhibit a different profile of gait and posture features based on the Kinect
Neurological Sciences (2024)
-
The impact of the COVID-19 pandemic on neuropsychiatric and sleep disorders, and quality of life in individuals with neurodegenerative and demyelinating diseases: a systematic review and meta-analysis of observational studies
BMC Neurology (2023)
-
Subthalamic 85 Hz deep brain stimulation improves walking pace and stride length in Parkinson’s disease patients
Neurological Research and Practice (2023)