
Abstract
Currently, antibiotic-resistant bacterial infections are a challenge for the health care system. Although physicians demand timely drug resistance data to guide empirical treatment, local data is rather scarce. Hence, this study performed a retrospective analysis of microbiological findings at the Hawassa public hospital. Secondary data were retrieved to assess the prevalence and level of drug resistance for the most common bacterial isolates from clinical samples processed at Hawassa University Comprehensive Specialized Hospital. Out of 1085 clinical samples processed in the microbiology laboratory, the prevalence of bacterial infection was 32.6%. Bacterial bloodstream infection was higher in children than in adults (OR, 4; 95% CI 1.8–14.6; p = 0.005). E. coli and K. pneumoniae were the commonest bacterial isolate both in children (36.8%, 26.3%) and in adults (33.3%, 26.7%) from the urine sample while, the leading bacteria identified from the CSF sample was P. aeruginosa, 37% in children and 43% in adult. In this study, all identified bacterial isolates were multi-drug resistant (MDR) ranging from 50 to 91%. The highest proportion of MDR was S. aureus 91.1 followed by K. pneumoniae 87.6%. Since the nationwide investigation of bacterial isolate, and drug resistance is rare in Ethiopia, a report from such type of local surveillance is highly useful to guide empirical therapy by providing awareness on the level resistance of isolates.
Similar content being viewed by others


Introduction
Bacterial infections and antibiotic resistant are threatening modern health care and have triggered the development of coordinated and comprehensive national and global actions plans. However, estimating the incidence, complications, and attributable mortality is challenging especially in Africa1. In developing countries like Ethiopia, the burden is so serious due to the unaffordability of the expensive alternative antibiotics for most of the patients2. The unregulated and often misusage of antibiotics provoked the development of antimicrobial resistance in the country3. Moreover, the rapid spread of antimicrobial-resistant organisms threatens the health care system due to a rising number of infectious diseases4.
Management of bacterial infection in Ethiopia has been largely empirical without the use of a bacterial culture and susceptibility testing to guide therapy. However, few teaching hospitals like Hawassa University comprehensive and specialized hospital (HU-CSH) have laboratory facilities to perform culture and antibacterial resistance tests. Indeed, this practice is a risk for development of antimicrobial resistance in most developing countries. In Ethiopia, where there are regulatory hindrances the challenge of antimicrobial resistance continued beside the scarcely available data5. The previous study has already reported the existence of elevated antimicrobial resistance (AMR) to different isolates, erythromycin (89.4%), amoxicillin (86.0%) and tetracycline (72.6%). The problem is more challenging due to about 75% of the burden found in developing countries6.
As to the WHOs declaration, AMR is one of the top 10 global public health threats facing humankind. Currently antibiotics are becoming increasingly ineffective as drug-resistance spreads globally leading to more difficult to treat infections. For common bacterial infections, including urinary tract infections, sepsis, sexually transmitted infections, and some forms of diarrhoea, high rates of resistance indicating that health facilities are running out of effective antibiotics7,8. There was considerable concern in several clinical situations where treatment options have become very limited and continues to threaten the ability to treat common infections9. In low-income countries, like Ethiopia, the problem is higher due to misuse and overuse of antimicrobials in addition to lack of laboratory facilities for antimicrobial susceptibility testing10.
According to the World Health Organization (WHO), bacterial resistance to first-line drugs ranges from zero to almost 100%. In some instances, resistance to second-and third-line drugs seriously compromising treatment outcome11. Indeed, due to the complex effect of drug resistance, it became global attention that needs urgent action to improve and coordinated global effort to encompass AMR12.
Infections by ESKAPE (Enterococcus, S. aureus, K. pneumoniae, A. baumannii, P. aeruginosa, and E. coli) organisms are the leading cause of healthcare-acquired infections worldwide. Most of them are multidrug resistant isolates, which is one of the greatest challenges in clinical practice13,14. It has been said also that, ESKAPE pathogens have developed resistance mechanisms either through inactivation or alteration of the antimicrobial molecule, bacterial target site modifications, reduced antibiotic penetration/accumulation, or by formation of bacterial biofilms14,15. The acquisition of antimicrobial resistance genes by ESKAPE pathogens has reduced the treatment options for serious infections15,16.
Enterococcus faecium is a prominent cause of health care-associated infections, several countries have now reported increases in resistance in hospitalized patients14,17,18. Methicillin-resistant staphylococci (MRSA) are also a major causes of bacterial infections with a serious challenge of antibiotics resistance19. The mecA gene, encoding MERSA, is located on a mobile genetic element called Staphylococcal Cassette Chromosome mec (SCCmec). Horizontal, interspecies transfer of this element could be an important factor in the dissemination of MRSA20,21. Many antibiotics, including β-lactams, can induce the expression of SCCmec excision from the bacterial chromosome22.
On the other hand, cephalosporin resistance due the enzymes β-lactamase, extended-spectrum lactamases (ESBLs) and carbapenemases destroys the β-lactam antibiotics such as penicillin, cephalosporins, and carbapenem drugs15,23,24. A. baumannii and E. coli also resist a number of carbapenem and lactam class antibiotics25,26. Whereas P. aeruginosa, the common infections in patients with impaired immunity27,28 more and more resisting antibiotics through intrinsic and acquired resistance mechanisms29.
The governmental organization known as Ethiopian Food, Medicine and Health Care Administration and Control Authority (EFMHACA) bears the responsibility to regulate drugs, food, health care personnel and setting at the central level. The authority controls and regulates drugs used in the country30. However, data’s on rates of bacterial isolate and AMR are scarce therefore, the local survey of laboratory data to note major isolates and their antibiotic resistance were as important to guide optimal empiric treatment of patients31.
Thus, the aim of this study is to indicate major pathogenic isolates and their antimicrobial resistance in the study area so that the finding supports health professionals empirical therapy.
Methods
A retrospective cross-sectional study was conducted at the microbiology laboratory of HUCSH, Hawassa, Ethiopia. HU-CSH is a teaching hospital providing services to more than 5 million people in the region as well from nearby region. Likewise, the HU-CSH microbiology laboratory also responsible for bacterial culture and resistance tests for patients in the area. The laboratory was supervised and supported by Federal government through the Ethiopian public health institute (EPHI). The EPHI makes mentor and monthly technical support including external quality assessment.
Samples were collected by the physician or the nurses from all inpatient and outpatient departments and immediately sent to the microbiology laboratory. The decision to take samples for microbiological culture and the selection of samples was made by the physicians. While, patient-related data (age and sex) with a full record of bacteriological culture and antimicrobial resistance profile were retrieved from the laboratory registration book. The study retrieved all microbiological reports on bacterial pathogens from January 2019 to December 2020.
Study participants and data collection
The study participants were individuals who visit HU-CSH and had complain of any infection suspected for bacterial infections during the study period. This study retrieved all documented data’s including age and sex of patients, the bacteria isolated and the drug susceptibility profiles from HU-CSH microbiology unit registration books using a standard data collection form.
All laboratory procedures were performed in accordance with the relevant guidelines and regulations of the Clinical and Laboratory Standards Institute’s (CLSI)32 and accustomed to the local standard operation procedures (SOPs) of our microbiology unit. Data obtained in the course of the study were kept confidential and used only for this study. We included all documented data within the study period except we rejected illegible or incompletely documented culture results.
Bacteriological investigation
Our bacteriological analysis follows SOPs adopted from CLSI guideline. The collected clinical samples were submitted to the laboratory and processed following standard procedures. Several types of clinical samples were cultured, including stool, urine, blood, urethral smear, and swabs from various body sites (vagina, ear, eye and wound). Each clinical samples employed similar standard microbiological culturing techniques. Specimens collected were inoculated onto appropriate isolation culture media and incubated at 35–37 °C conferring to standard protocols for each sample33. Bacterial identification was done primarily based on colony characteristics and Gram-stain reaction followed by proper biochemical tests as per suitability according to CLSI guidelines and developed SOP.
Antimicrobial susceptibility
The antimicrobial susceptibility profile of isolates was determined by Kirby-Bauer disc diffusion method and the results were interpreted according to CLSI guidelines34. The antimicrobial discs were obtained from Oxoid (Oxoid, Hampshire, UK) in the following concentrations: Amoxicillin-Calvulanic acid (AMC, 20/10 μg), cotrimoxazole (SXT, 25 μg), Ceftazidime (CAZ, 30 μg), cefotaxime (CTX, 30 μg), Chloramphenicol (CAF, 30 μg), nitrofurantoin (NIT 300 μg), ceftriaxone (CRT, 30 μg), ampicillin (AMP,10 μg) Erythromycin(E, 30 μg), gentamicin (GN, 10 μg), meropenem (MER 10 μg), Amikacin(AMK, 30 μg), ceftriaxone (CRO, 30 μg). The definition of MDR in this study refers to resistant to at least one agent in three or more antimicrobial classes.
Quality control
The quality of our laboratory culture system was performed using E. coli (ATCC-25922), P. aeruginosa (ATCC-27853), and S. aureus (ATCC-25923) as reference strains for culture and susceptibility testing. Thus, qualities of prepared media were monitored all the time according to the set criteria by CLSI in fact EPHI closely supervised our laboratory monthly.
Data analysis
The data was entered and analysed using SPSS version 20 (IBM Corporation, Armonk, NY, USA). Descriptive statistics like frequency and percentages of categorical variables were calculated. Bivariate comparisons using Chi-square logistic regression were employed to assess the association between variables. A p-value of less than 0.05 was considered statistical significant.
Ethical clearance
Ethical clearance was obtained from the institutional review board (IRB) of Hawassa University College of medicine and health science. As the study was retrospective, following IRB clearance, we have asked the hospital administration for a waiver to retrieve the data. Accordingly, the official waiver letter was obtained from the HU-CSH hospital administration. We have also obtained official permission from the hospital laboratory manager of HU-CSH. All data obtained in the course of the study were reserved confidential and used only for this study.
Result
Study population
In this study, a total of 1085 clinical samples were processed. Of these, females were one-third 385 (35.5%) of the study population. Likewise, the rate of positivity in female is lower 114 (32.2%) compared to males 240 (67.8%) but not significantly associated (p = 0.11). Regarding the age group, the proportion of under-5 children was about two-thirds (61.3%) of participants. There was a significant association between age group of participants and positivity of bacterial infection (p = 0.154). The age range of participants was from zero-day neonates to 82 years old elders with a mean age of 8.7 years (Table 1).
Of 1085 clinical sample diagnosed in microbiology laboratory 32.6% (354/1085) of them were positive for any of bacterial infection. The proportion of positivity was decrease with age (Table 1).
Bacterial spectrum
The overall prevalence of the bacterial infection was (354/ 1085, 32.6%). The predominant type of infection was bloodstream infection (78, 22%). Of the total 354 identified isolates, 91 were from urine, 34 from CSF, 105 from blood and the remaining 91 were documented from different clinical samples (including pus, discharge and stool sputum) (Table 3). Nearly 46% (n = 162) of the isolate were attained from patients those who have one or two types of the previous history of antibiotic exposure before specimen collection.
The children were more positive in bloodstream infection than adults (OR, 4; 95% CI 1.8–14.6; p = 0.005) (Table 2). The isolates from different groups of infections were not similar however, common bacterial pathogens were documented in both adults and children (Tables 2, 3). For instance, nearly equal proportions of E. coli and K. pneumoniae isolates were observed in children (36.8%, 26.3%) and adults (33.3%, 26.7%) from urine samples. Again, a comparable result was recorded for P. aeruginosa in the CSF sample, 37% in children and 43% in adults. On the other hand, the most frequent isolate from blood cultures in children was CoNS (29.5%) followed by K. pneumoniae (25.7%) and S. aureus (20%). But in adult CoNS (60%) followed by S. aureus (20%) were found (Table 3).
Antibiotic resistance
As indicated in Table 4, most of the gram positive isolates showed the highest resistance to erythromycin and gentamicin for instance; S. pyogens (75%), S. aureus (55%). CoNS showed about 30–55% resistances to Trimethoprim-Sulphametoxazole, ceftazidime, erythromycin and gentamicin. The Enterococci spp. also showed 85.7% resistance to gentamicin and 57.2% to Trimethoprim-Sulphametoxazole, respectively.
Among gram-negative bacteria, K. pneumoniae has shown the highest resistance rates to ampicillin (75%), ceftazidime (82%) and ciprofloxacin (80.9) while the least resistance (3.3%) to meropenem was documented. Likewise, E. coli also showed the highest resistance to cotrimoxazole (70.4%) and ciprofloxacin (63.6%) while less resistant to meropenem (4.5%). In general, in this study gram-negative isolates were susceptible to meropenem (Table 5).
Multidrug‑resistance profiles of the isolates
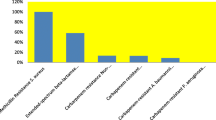
As indicated in Table 6, S. aureus and K. pneumoniae documented a highest multidrug-resistance for more than two antibiotics, 91.1% (51/56) and 87.6% (78/89) respectively. About 15% of S. aureus isolates were resisted to more than 5 antibiotics while only 5.4% of them were susceptible to tested drugs. Likewise, 15% K. pneumoniae isolates resisted for more than 5 antibiotics and only 4.5% susceptibility was documented. According to our finding, 9 (16%) of S. aureus were resistant to AMC, SXT, CAF, CRT, GN and CAZ. Around 6 (10%) isolates were also resistance to CAZ, CTX, and CAF. Similarly, 15 (28.8%) of E. coli were resistant to AMP, AMC, AMK, SXT, CAF and CIP, while 3 (5.8%) for CAZ, CIP and AMK.
Discussion
The burden of drug-resistant bacterial infections remains a global challenge that triggers the development of global actions. According to this study, the leading bacterial isolates were K. pneumoniae 89 (25.2%) and S. aureus 56 (15.8%). Out of 1085 clinical samples processed, 32.6% of them were culture positive of which the gram-negative pathogens were dominant. It is similar to others report that K. pneumoniae and S. aureus were dominant isolates from different clinical samples35,36,37.
According to this study, the major bacterial isolate in bloodstream infection among children is CoNS and K. pneumoniae which is similar to our previous report38 and with others finding at northern39 and central Ethiopia40,41,42. Nearly similar to a study in Egypt, Gabon and Zimbabwe where CoNS, E. coli and K. pneumoniae were the major isolates in bloodstream infection43,44,45. In our finding, P. aeruginosa and K. pneumoniae are the major bacteria isolated from CSF unlike others report5,38,41,46. On the other hand, study from Tanzania has reported that S. aureus was the main pathogen in bloodstream infection unlike our finding47. Based on this finding, CoNS was the major pathogen in bloodstream infection. The possible attribute might be the poor hygienic care as well as the higher nosocomial infection in our setup48 that significantly contributes to the high proportion of CoNS. A recent report also showed the highest prevalence of hospital-acquired bacterial infections in a developing country49.
In regard to the isolates from UTI, E. coli and K. pneumoniae were documented as major bacterial agent which is consistent with a study conducted with others41,50. Our finding was slightly higher than previously published results in Ethiopia35,36. Of course, the variation in bacterial isolate of UTI infection has been seen across region50. This could be due to differences among study participants, catheterization and hospitalization history.
Unlike our previous report, where N. meningitis and E. coli were the predominant isolate in CSF38, in this study P. aeruginosa and K. pneumoniae were the leading isolate. In this study the highest number of bacterial infection were documented in neonates which shows that newborns might be at higher risk of bacterial infection. Hence adequate attention should be given particularly in maintaining the proper hygiene at the ICU51.
From other specimens like stool, pus, sputum and discharges, S. aureus and K. pneumoniae were found a major infectious agent. Compiling such type of laboratory database is useful to provide valuable insight about the types of sample and identified drug resistant isolates in areas where microbiological investigations are scarce41. Hence our data can be used in support of the existing empirical therapy.
Now a day, MDR bacterial infections due to ESKAPE groups become a major health problem and account for a great burden in the effective therapeutic strategies52. Our study showed high-level ESKAPE groups MDR (greater than 70%) which is comparable with others report in Ethiopia41,42. However, certain variation in bacterial isolate and resistance level reported within-country5,39 besides related reports in Africa43,45. This might be due to a lack of consistency in the measurement and reporting of drug susceptibility data. In fact, most studies were conducted using a disk diffusion technique similar to this study53.
The rate of overall MDR S. aureus documented in this study is similar to most other studies54,55,56,57,58,59. This might be due to the fact that S. aurous can present and cause infection to diverse sites of a human body beyond being normal commensal. The major antibiotics prescribed for S. aurous in local area were mostly resisted emphasizing the need for continuous investigation as well as etiologic based therapy. However, in Ethiopia majorities of hospitals were not performing bacteriological culture routinely. Hence, clinician need to look for such type of compiled reports for further consideration of their antibiotics selection.
On the other hand, nearly 88% of K. pneumoniae, 75% E. coli and 70% of P. aeruginosa isolates were resistant to the tested antibiotics. These isolates were mainly identified as hospital-acquired pathogen also they were reported to be community-acquired. The ESKAPE pathogens are the leading cause of nosocomial infections and most of them are MDR, which is one of the greatest challenges in clinical practice amongst critically ill and immunocompromised individuals15. Our finding is somehow comparable to previous studies where MDR-ESKAPE reported as predominant isolates55,60,61,62. The resistances acquired to available drugs either by mutation or receipt of foreign genetic materials through the transfer of plasmids and transposons of other microorganisms of the surrounding flora.
In general, the Gram-negative ESKAPE pathogens drug resistance in this study was somehow comparable with others finding for instance, with a study in Latin American countries63, Sudan64 Northern Ethiopia9 and the systematic reviews conducted in Ethiopia65,66. According to the systematic review, the Gram-negative ESKAPE pathogens were highly drug-resistant with estimates between 76 and 87%66. Similarly, high MDR Acinetobacter isolates usually reported around 45% of hospitalized patients globally14. In Asia–Pacific countries, around 57% of A. baumannii were resistant to all tested drugs67. While our finding showed a bit higher, 70% that is similar with Latin American countries report63.
Such type of study has an important effect to help the approval of guidelines to the empirical choice of antibiotic therapy. Moreover, from the patient perspective, an appropriate antibiotic resistance profile is essential to reduce mortality and length of hospitalization, the loss of work and family time associated with increased hospitalization time and subsequent recovery, and even the emotional impact of having a resistant infection. In fact, the economic burden of antimicrobial resistance in the prospect of hospital costs, hospital charges including operation costs, the cost of drugs and tests, and other patient care activities and resources used is also a major concern. Hence, such types of studies have a great role for clinicians as well as for policy makers68.
Limitations
There were certain limitations in this study: First, this retrospective study does not includes all patients visiting our hospital due to some the fact that in our setup culture is not ordered for non-critical patients. For instant most asymptomatic STI and enteric infections by default managed by empirical therapy. Second, we can’t compare our findings by dwelling and wards as these variables were not registered in laboratory log book Third, we did not investigate risk factors for infection as well as for drug resistance as it is retrospective data.
Conclusions
According to our investigation, a high rate of bacterial infection (32.6%) was reported and most of the isolates resist the commonly used antibiotics. K. pneumoniae, S. aureus, E. coli were the common isolates in most clinical samples meanwhile CoNS was major bloodstream infection in neonates. The least resistance antibiotics for gram-positive isolate were cefotaxime, meropenem nitrofurantoin and amoxicillin-calvulanic acid. On the other hand, highest levels of resistance were seen for ciprofloxacin, ampicillin and cotrimoxazole. We advise clinicians to see options from such type of compiled data for their routine empirical therapy of bacterial infections.
Data availability
The data that support the findings of this study are available from the corresponding author on upon reasonable request.
Abbreviations
- AMR:
-
Antimicrobial resistance
- ATCC:
-
American type culture collection
- CLSI:
-
Clinical and laboratory standard Institute
- CoNS:
-
Coagulase-negative staphylococcus
- CSF:
-
Cerebrospinal fluid
- HUCSH:
-
Hawassa University Comprehensive Specialized Hospital
- IRB:
-
Institutional Review Board
- SNNPR:
-
Southern Nation Nationalities’ and peoples’ region
- SOP:
-
Standard operating procedure
- SPSS:
-
Statistical package for social sciences
- WHO:
-
World Health Organisation
References
WHO. Global Action Plan on Antimicrobial Resistance (WHO, 2015).
Laxminarayan, R. & Heymann, D. L. Challenges of drug resistance in the developing world. BMJ 344, e1567 (2012).
Hart, C. A. & Kariuki, S. Antimicrobial resistance in developing countries. BMJ 317(7159), 647–650 (1998).
Muhie, O. A. Antibiotic use and resistance pattern in Ethiopia: Systematic review and meta-analysis. Int. J. Microbiol. 2019, 2489063 (2019).
Abebe, M., Tadesse, S., Meseret, G. & Derbie, A. Type of bacterial isolates and antimicrobial resistance profile from different clinical samples at a Referral Hospital, Northwest Ethiopia: Five years data analysis. BMC. Res. Notes 12(1), 568 (2019).
Alessandro Cassini, M., Liselotte Diaz Högberg, P., Diamantis Plachouras, P., Annalisa Quattrocchi, P., Ana Hoxha, M. & Gunnar Skov Simonsen, P. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: A population-level modelling analysis. 2018.
World Health Organization. Antimicrobial resistance and primary health care (World Health Organization, 2018).
Essack, S. Y., Desta, A. T., Abotsi, R. E. & Agoba, E. E. Antimicrobial resistance in the WHO African region: Current status and roadmap for action. J. Public Health 39(1), 8–13 (2016).
Mulu, W. et al. Bacterial agents and antibiotic resistance profiles of infections from different sites that occurred among patients at Debre Markos Referral Hospital, Ethiopia: A cross-sectional study. BMC. Res. Notes 10(1), 254 (2017).
FMHCA. E. Food, Medicine and Health Care Administration and Control Authority of Ethiopia. www.fmhaca.gov.et.
World Health Organization. WHO Global Strategy for Containment of Antimicrobial Resistance (World Health Organization, 2001).
Prestinaci, F., Pezzotti, P. & Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 109(7), 309–318 (2015).
Zhen, X., Lundborg, C. S., Sun, X., Hu, X. & Dong, H. Economic burden of antibiotic resistance in ESKAPE organisms: A systematic review. Antimicrob. Resist. Infect. Control 8(1), 137 (2019).
De Oliveira, D. M. P. et al. Antimicrobial resistance in ESKAPE pathogens. Clin. Microbiol. Rev. 33(3), e00181-e219 (2020).
Santajit, S. & Indrawattana, N. Mechanisms of antimicrobial resistance in ESKAPE pathogens. Biomed. Res. Int. 2016, 2475067 (2016).
Pendleton, J. N., Gorman, S. P. & Gilmore, B. F. Clinical relevance of the ESKAPE pathogens. Expert Rev. Anti Infect. Ther. 11(3), 297–308 (2013).
Gastmeier, P., Schröder, C., Behnke, M., Meyer, E. & Geffers, C. Dramatic increase in vancomycin-resistant enterococci in Germany. J. Antimicrob. Chemother. 69(6), 1660–1664 (2014).
Pinholt, M. et al. Multiple hospital outbreaks of vanA Enterococcus faecium in Denmark, 2012–13, investigated by WGS, MLST and PFGE. J. Antimicrob. Chemother. 70(9), 2474–2482 (2015).
Tong, S. Y., Davis, J. S., Eichenberger, E., Holland, T. L. & Fowler, V. G. Jr. Staphylococcus aureus infections: Epidemiology, pathophysiology, clinical manifestations, and management. Clin. Microbiol. Rev. 28(3), 603–661 (2015).
Hanssen, A. M. & Ericson Sollid, J. U. SCCmec in staphylococci: Genes on the move. FEMS Immunol. Med. Microbiol. 46(1), 8–20 (2006).
Otto, M. Coagulase-negative staphylococci as reservoirs of genes facilitating MRSA infection: Staphylococcal commensal species such as Staphylococcus epidermidis are being recognized as important sources of genes promoting MRSA colonization and virulence. BioEssays 35(1), 4–11 (2013).
Liu, P., Wu, Z., Xue, H. & Zhao, X. Antibiotics trigger initiation of SCCmec transfer by inducing SOS responses. Nucleic Acids Res. 45(7), 3944–3952 (2017).
Paterson, D. L. & Bonomo, R. A. Extended-spectrum β-lactamases: A clinical update. Clin. Microbiol. Rev. 18(4), 657–686 (2005).
Cheng, N.-C. et al. Recent trend of necrotizing fasciitis in Taiwan: Focus on monomicrobial klebsiella pneumoniae necrotizing fasciitis. Clin. Infect. Dis. 55(7), 930–939 (2012).
Xie, R., Zhang, X. D., Zhao, Q., Peng, B. & Zheng, J. Analysis of global prevalence of antibiotic resistance in Acinetobacter baumannii infections disclosed a faster increase in OECD countries. Emerg. Microb. Infect. 7(1), 1–10 (2018).
Collignon, P. Resistant Escherichia coli—We are what we eat. Clin. Infect. Dis. 49(2), 202–204 (2009).
Gellatly, S. L. & Hancock, R. E. W. Pseudomonas aeruginosa: New insights into pathogenesis and host defenses. Pathog. Dis. 67(3), 159–173 (2013).
Yayan, J., Ghebremedhin, B. & Rasche, K. Antibiotic resistance of Pseudomonas aeruginosa in pneumonia at a single university hospital center in Germany over a 10-year period. PLoS ONE 10(10), e0139836 (2015).
Pang, Z., Raudonis, R., Glick, B. R., Lin, T.-J. & Cheng, Z. Antibiotic resistance in Pseudomonas aeruginosa: Mechanisms and alternative therapeutic strategies. Biotechnol. Adv. 37(1), 177–192 (2019).
Gazeta FN. Proclamation no. 661/2009. A proclamation to provide for food, medicine and health care administration and control. 2010:5157-91.
Han, Y.-Y. et al. Rapid antibiotic susceptibility testing of bacteria from patients’ blood via assaying bacterial metabolic response with surface-enhanced Raman spectroscopy. Sci. Rep. 10(1), 12538 (2020).
Clinical Institute LS,. Performance Standards for Antimicrobial Susceptibility Testing (Clinical and Laboratory Standards Institute, 2017).
Cheesbrough, M. District Laboratory Practice in Tropical Countries 2nd edn. (Cambridge University Press, 2006).
Patel, J. et al. M100 Performance Standards for Antimicrobial Susceptibility Testing 240 (Clinical and Laboratory Standards Institute, 2017).
Gorems, K., Beyene, G., Berhane, M. & Mekonnen, Z. Antimicrobial susceptibility patterns of bacteria isolated from patients with ear discharge in Jimma Town, Southwest, Ethiopia. BMC Ear Nose Throat Disord. 18(1), 1–9 (2018).
Beyene, D., Bitew, A., Fantew, S., Mihret, A. & Evans, M. Multidrug-resistant profile and prevalence of extended spectrum β-lactamase and carbapenemase production in fermentative Gram-negative bacilli recovered from patients and specimens referred to National Reference Laboratory, Addis Ababa, Ethiopia. PLoS ONE 14(9), e0222911 (2019).
Amsalu, A., Geto, Z., Asegu, D. & Eshetie, S. Antimicrobial resistance pattern of bacterial isolates from different clinical specimens in Southern Ethiopia: A three year retrospective study. Afr. J. Bacteriol. Res. 9(1), 1–8 (2017).
Tsegay, E. et al. Bacterial isolates and drug susceptibility pattern of sterile body fluids from tertiary hospital, Northern Ethiopia: A four-year retrospective study. J. Pathog. 2019, 5456067 (2019).
Abebaw, A., Tesera, H., Belachew, T. & Mihiretie, G. D. The Bacterial Profile and antibiotic Susceptibility Pattern Among Patients with Suspected Bloodstream Infections, Gondar, North-West Ethiopia Vol. 10, 1–7 (Pathology and Laboratory Medicine International Dove Press, 2018).
Legese, M. H., Weldearegay, G. M. & Asrat, D. Extended-spectrum beta-lactamase- and carbapenemase-producing Enterobacteriaceae among Ethiopian children. Infect. Drug Resist. 10, 27–34. https://doi.org/10.2147/IDR.S127177 (2017).
Ten Hove, R. J., Tesfaye, M., Ten Hove, W. F. & Nigussie, M. Profiling of antibiotic resistance of bacterial species recovered from routine clinical isolates in Ethiopia. Ann. Clin. Microbiol. Antimicrob. 16(1), 46 (2017).
Beyene, D., Bitew, A., Fantew, S., Mihret, A. & Evans, M. Multidrug-resistant profile and prevalence of extended spectrum β-lactamase and carbapenemase production in fermentative Gram-negative bacilli recovered from patients and specimens referred to National Reference Laboratory, Addis Ababa, Ethiopia. PLoS ONE 14(9), e0222911. https://doi.org/10.1371/journal.pone.0222911 (2019).
Alabi, A. S. et al. Retrospective analysis of antimicrobial resistance and bacterial spectrum of infection in Gabon, Central Africa. BMC Infect. Dis. 13, 455 (2013).
Chinowaita, F. et al. Sepsis in cancer patients residing in Zimbabwe: Spectrum of bacterial and fungal aetiologies and their antimicrobial susceptibility patterns. BMC Infect. Dis. 20(1), 161. https://doi.org/10.1186/s12879-020-4886-2 (2020).
Tohamy, S. T., Aboshanab, K. M., El-Mahallawy, H. A., El-Ansary, M. R. & Afifi, S. S. Prevalence of multidrug-resistant Gram-negative pathogens isolated from febrile neutropenic cancer patients with bloodstream infections in Egypt and new synergistic antibiotic combinations. Infect. Drug Resist. 11, 791–803. https://doi.org/10.2147/IDR.S163293 (2018).
AntenehAmsalu, A., Geto, Z., Asegu, D. & Eshetie, S. Antimicrobial resistance pattern of bacterial isolates from different clinical specimens in Southern Ethiopia: A three year retrospective study. Afr. J. Bacteriol. Res. 9(1), 1–8 (2017).
Mhada, T. V., Fredrick, F., Matee, M. I. & Massawe, A. Neonatal sepsis at Muhimbili National Hospital, Dar es Salaam, Tanzania; Aetiology, antimicrobial sensitivity pattern and clinical outcome. BMC Public Health 12, 904. https://doi.org/10.1186/1471-2458-12-904 (2012).
Alemayehu, T., Tadesse, E., Ayalew, S., Nigusse, B., Yeshitila, B., Amsalu, A, et al. High burden of Nosocomial infections caused by multi-drug Re-sistant pathogens in pediatric patients at Hawassa university comprehensive specialized hospital. Ethiop. Med. J. 58 (2019).
Rosenthal, V. D. et al. International Nosocomial Infection Control Consortium (INICC) report, data summary of 43 countries for 2007–2012. Device-associated module. Am. J. Infect. Control 42(9), 942–956 (2014).
Seifu, W. D. & Gebissa, A. D. Prevalence and antibiotic susceptibility of Uropathogens from cases of urinary tract infections (UTI) in Shashemene referral hospital, Ethiopia. BMC Infect. Dis. 18(1), 30 (2018).
Hailemariam, M., Worku, M. & Azerefegne, E. Intensive care units and operating rooms bacterial load and antibiotic susceptibility pattern. J. Surg. 4(2), 60–64 (2016).
Ma, Y.-X. et al. Considerations and caveats in combating ESKAPE pathogens against nosocomial infections. Adv. Sci. 7(1), 1901872 (2020).
Tadesse, B. T. et al. Antimicrobial resistance in Africa: A systematic review. BMC Infect. Dis. 17(1), 616 (2017).
Deyno, S., Fekadu, S. & Astatkie, A. Resistance of Staphylococcus aureus to antimicrobial agents in Ethiopia: A meta-analysis. Antimicrob. Resist. Infect. Control 6(1), 85 (2017).
Godebo, G., Kibru, G. & Tassew, H. Multidrug-resistant bacterial isolates in infected wounds at Jimma University Specialized Hospital, Ethiopia. Ann. Clin. Microbiol. Antimicrob. 12, 17 (2013).
Abera, B., Kibret, M. & Mulu, W. Knowledge and beliefs on antimicrobial resistance among physicians and nurses in hospitals in Amhara Region, Ethiopia. BMC Pharmacol. Toxicol. 15, 26 (2014).
Moges, F. et al. The growing challenges of antibacterial drug resistance in Ethiopia. J. Glob. Antimicrob. Resist. 2(3), 148–154 (2014).
Mama, M., Abdissa, A. & Sewunet, T. Antimicrobial susceptibility pattern of bacterial isolates from wound infection and their sensitivity to alternative topical agents at Jimma University Specialized Hospital, South-West Ethiopia. Ann. Clin. Microbiol. Antimicrob. 13, 14 (2014).
Mulu, W., Kibru, G., Beyene, G. & Damtie, M. Postoperative nosocomial infections and antimicrobial resistance pattern of bacteria isolates among patients admitted at Felege Hiwot Referral Hospital, Bahirdar, Ethiopia. Ethiop. J. Health Sci. 22(1), 7–18 (2012).
Tuem, K. B. et al. Drug resistance patterns of Escherichia coli> in Ethiopia: A meta-analysis. Biomed. Res. Int. 2018, 4536905 (2018).
Demilie, T., Beyene, G., Melaku, S. & Tsegaye, W. Urinary bacterial profile and antibiotic susceptibility pattern among pregnant women in North West Ethiopia. Ethiop. J. Health Sci. 22(2), 121–128 (2012).
Ramsamy, Y., Essack, S. Y., Sartorius, B., Patel, M. & Mlisana, K. P. Antibiotic resistance trends of ESKAPE pathogens in Kwazulu-Natal, South Africa: A five-year retrospective analysis. Afr. J. Lab. Med. 7(2), 1–8 (2018).
Karlowsky, J. A., Hoban, D. J., Hackel, M. A., Lob, S. H. & Sahm, D. F. Resistance among Gram-negative ESKAPE pathogens isolated from hospitalized patients with intra-abdominal and urinary tract infections in Latin American countries: SMART 2013–2015. Braz. J. Infect. Dis. 21(3), 343–348 (2017).
Ibrahim, M., Bilal, N. & Hamid, M. Increased multi-drug resistant Escherichia coli from hospitals in Khartoum state, Sudan. Afr. Health Sci. 12(3), 368–375 (2012).
Tuem, K. B. et al. Drug resistance patterns of Escherichia coli in Ethiopia: A meta-analysis. BioMed Res. Int. 2018, 4536905 (2018).
Chelkeba, L., Melaku, T. & Mega, T. A. Gram-negative bacteria isolates and their antibiotic-resistance patterns in patients with wound infection in Ethiopia: A systematic review and meta-analysis. Infect. Drug Resist. 14, 277 (2021).
Karlowsky, J. A., Hoban, D. J., Hackel, M. A., Lob, S. H. & Sahm, D. F. Antimicrobial susceptibility of Gram-negative ESKAPE pathogens isolated from hospitalized patients with intra-abdominal and urinary tract infections in Asia–Pacific countries: SMART 2013–2015. J. Med. Microbiol. 66(1), 61–69 (2017).
Giacomini, E. et al. Evidence of antibiotic resistance from population-based studies: A narrative review. Infect. Drug Resist. 14, 849 (2021).
Acknowledgements
We would wish to express our genuine thankfulness to the staff of microbiology lab for reliable help during compiling of data from log books. We also thank Hawassa university comprehensive specialized hospital for official permission of this study.
Author information
Authors and Affiliations
Contributions
All authors; M.H., T.A., E.A., A.A., T.H., M.A., N.N., B.T. and E.M.: participated in conception of the study, collected the data, interpretation of data and drafting the manuscript. M.H. and T.A.: design of study and critically reviewing the manuscript for important intellectual content. All authors read and approved the final manuscript for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hailemariam, M., Alemayehu, T., Tadesse, B. et al. Major bacterial isolate and antibiotic resistance from routine clinical samples in Southern Ethiopia. Sci Rep 11, 19710 (2021). https://doi.org/10.1038/s41598-021-99272-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-99272-2
- Springer Nature Limited