
Abstract
Frailty is associated with gait variability in several quantitative parameters, including high stride time variability. However, the associations between joint kinematics during walking and increased gait variability with frailty remain unclear. In the current study, principal component analysis was used to identify the key joint kinematics characteristics of gait related to frailty. We analyzed whole kinematic waveforms during the entire gait cycle obtained from the pelvis and lower limb joint angle in 30 older women (frail/prefrail: 15 participants; non-frail: 15 participants). Principal component analysis was conducted using a 60 × 1224 input matrix constructed from participants’ time-normalized pelvic and lower-limb-joint angles along three axes (each leg of 30 participants, 51 time points, four angles, three axes, and two variables). Statistical analyses revealed that only principal component vectors 6 and 9 were related to frailty. Recombining the joint kinematics corresponding to these principal component vectors revealed that frail older women tended to exhibit greater variability of knee- and ankle-joint angles in the sagittal plane while walking compared with non-frail older women. We concluded that greater variability of knee- and ankle-joint angles in the sagittal plane are joint kinematic characteristics of gait related to frailty.
Similar content being viewed by others


Introduction
Frailty is associated with an increased risk of adverse consequences, including functional decline, deterioration, multiple hospitalizations and death, and is an important public health concern in aging societies1,2,3,4,5,6. Clinical literature over the past several decades has identified clear sex differences in frailty, typically reporting that women have a higher prevalence and risk of frailty7,8,9,10,11. Women are also reported to have a higher prevalence of muscle weakness, lower bone density and a higher risk of future fractures associated with a decrease in female hormone levels with menopause, and are at a higher risk of decline in walking ability and becoming bedridden from frailty than males13,70,71,72,73. To prevent frailty, it is important to detect symptoms of frailty before the condition becomes severe, so that appropriate interventions can be carried out12. Preclinical changes in gait have been reported as an early sign of frailty, for both males and females13,14,15,16,17,18,19,20,21,22,23,24. Therefore, comparison of gait characteristics in healthy and frail older women is necessary for gaining a detailed understanding of the frailty-related decrease in walking ability among older women.
Gait variability is associated with frailty status17. Previous studies have consistently reported that, compared with healthy older adults, frail older adults tend to exhibit greater within-participant variability on various gait related parameters, including stride length, step width and cadence, using pressure sensitive walkways or accelerometry17,18,25,26. However, the way in which the joint kinematics of the lower extremities during walking are associated with increased gait variability in frailty has not yet been thoroughly investigated. In addition, to the best of our knowledge, no previous study has evaluated joint angles or the variability of the lower extremities during the entire gait cycle in relation to frailty status. Detailed investigation of the relationships between frailty status and gait characteristics, including variability in joint kinematics while walking, could be helpful for understanding the mechanisms of increased gait variability and decreased walking ability in frail older adults. Moreover, elucidating this issue could inform the development of better indicators for early detection of frailty and early preventive measures.
In the last several decades, the effects of frailty on various gait variables, such as walking speed, stride length, step width and cadence have been investigated17,18,19,20,21,22,23,24,25,26,27,28,29,30,31. However, these previous studies of gait in frail older people have focused on variables and discrete time points selected by researchers. An advantage of traditional biomechanical analysis methods (e.g., analysis of several discrete variables, such as peak angles, together with statistical hypothesis tests, such as t-tests or analysis of variance) is that they allow for detailed comparisons of selected variables between different groups, and investigation of relevant factors. However, the disadvantage of these methods is that they may not be able to detect crucial information in large portions of unanalyzed data32. In this regard, principal component analysis has recently attracted increasing interest in biomechanical studies because of its usefulness in identifying the movement characteristics of various groups under a range of conditions using waveforms of the entire time series data set in a comprehensive manner32,33,34,35,36,37,38,39,40,41,42. Principal component analysis is a multivariate statistical technique that summarizes the information conveyed by a large number of correlated variables using a smaller number of uncorrelated variables (principal components). Principal component analysis generates principal component vectors and a set of principal component scores for each principal component vector. Each principal component vector corresponds to an axis of variance, and a principal component score is a projection of the input data onto each principal component vector. The waveforms related to each principal component vector can be reconstructed by adding and subtracting the principal component scores. Therefore, the use of this principal component analysis-based approach could enable increased understanding of walking characteristics and joint kinematics among frail older women throughout the entire gait cycle.
The purpose of the current study was to compare the key characteristic features of joint kinematics during the entire gait cycle in frail older women and non-frail older women using principal component analysis. To understand the gait characteristics of frail older women, we also compared basic spatiotemporal parameters of the gait cycle: walking speed, stride length, stride time, and stance time percentage. Previous studies of combined samples of women and males have reported that frail older adults exhibit increased variability in stride time and length compared with non-frail older adults17,18,25. Therefore, we hypothesized that walking in frail older women involves increased joint angle variability of the lower extremities during the swing phase of the gait cycle compared with that in non-frail older women.
Results
Participants’ demographic data (means and standard deviations [SDs]) are presented in Table 1. We defined frailty based on criteria developed by Fried et al.6. Thirteen participants were classified as prefrail, two were classified as frail and 15 were classified as non-frail. There were no significant differences in basic information between frail/prefrail participants and non-frail participants.
Principal component analysis revealed that 26 extracted principal component vectors explained more than 84% of the joint movement patterns. The explained variance, means, and SDs of the principal component scores by group are shown in Table 2. Univariate analysis (independent t-tests) revealed significant differences between frail/prefrail participants and non-frail participants on principal component vectors 6 (p = 0.024, d = 0.60) and 9 (p = 0.001, d = 0.72) and explained 4.12% and 3.33% of the total variance, respectively.
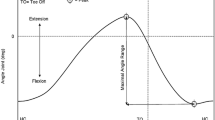
We used these vectors to reconstruct joint kinematic waveforms (average and SD) of the pelvis, hip-, knee-, and ankle-joint angles on the sagittal, frontal, and horizontal planes (Figs. 1, 2). The reconstructed waveforms illustrated the differences between frail/prefrail participants (solid line) and non-frail participants (dotted line). As shown in Fig. 1, compared with non-frail participants, frail/prefrail participants tended to exhibit greater variability of the knee joint angle during the pre-swing, initial swing and terminal swing phases, and tended to exhibit greater variability of ankle joint angle during the pre-swing and initial swing phases in the sagittal plane. We used univariate analysis to confirm the presence of a significant difference between groups in the gait phase and joints where these trends were observed. Compared with the variability in the non-frail participants’ raw data, the raw data of frail/prefrail participants showed significantly greater variability of the knee, and ankle joints during the pre-swing and initial swing phases in the sagittal plane, and significantly greater variability of the knee joint during the terminal swing phase in the sagittal plane (see Supplementary Fig. S1). Furthermore, the reconstructed waveforms (Fig. 2) showed that frail/prefrail participants tended to exhibit smaller pelvis front and horizontal plane movement, hip extension, knee flexion and ankle plantar-flexion angles during all phases. Compared with the raw range of motion data (max angle minus minimum angle) for non-frail participants during the entire gait cycle, the raw data for frail/prefrail participants revealed a significantly smaller range of motion of the pelvis in the horizontal plane and of the hip joint in the sagittal plane (see Supplementary Fig. S2).

Waveforms of variability (standard deviation: SD) recombined from the principal component scores of principal component vectors 6 and 9. The gray highlighted area indicates the instance of the toe off (the transition from the stance phase to the swing phase). This area has a certain width because we did not separate the stance phase from the swing phase in the time-normalization procedure.

Waveforms of central tendency (average) recombined from the principal component scores of principal component vectors 6 and 9. The definitions of the abbreviations in the variability graph are as follows: Post. posterior tilt, Ant. anterior tilt, Flex. flexion, Ext. extension, D.F. dorsiflexion, P.F. plantarflexion, Hike. pelvic hike, Drop. pelvic drop, Add. adduction, Abd. abduction, I.R. internal rotation, E.R. external rotation, Ever. eversion, Inv. inversion.
Table 3 shows the central tendency and the variability (coefficient of variation) of the spatiotemporal parameters. Univariate analysis revealed that frail/prefrail participants walked significantly more slowly (p = 0.045, d = 0.75) with a significantly shorter stride length (p = 0.003, d = 0.53) compared with non-frail participants. In addition, walking in frail/prefrail participants exhibited greater variability of stride time (p = 0.029, d = 0.58) and stance time percentage (p = 0.008, d = 0.72) compared with that in non-frail participants.
The Pearson’s product moment correlation coefficients between the spatiotemporal parameters and principal component vectors are shown in Table 4. The correlation coefficients between the spatiotemporal parameters and principal component vectors 6 and 9 (the principal component vectors related to frailty) revealed that the principal component score of vector 6 was significantly correlated with the central tendencies of walking speed (r = − 0.349, p = 0.006), step length (r = − 0.428, p = 0.001) and stance time percentage (r = 0.282, p = 0.029), as well as variability of stride time (r = 0.269, p = 0.038). Vector 9 was significantly correlated with the variability of stance time percentage (r = 0.259, p = 0.046) (Table 4).
Discussion
The purpose of the current study was to compare the key joint kinematics characteristics during the entire gait cycle in frail and non-frail older women using principal component analysis. Principal component analysis was conducted on the time-normalized average and SD of the pelvis and lower limb joint angles. Significant differences between frailty status groups were found for two principal component vectors: vector 6 and vector 9. Vector 6 had a moderate effect (p = 0.024, d = 0.60) and vector 9 had a large effect (p = 0.001, d = 0.72), which were then used to reconstruct kinematic waveforms of the joint angles. Because the principal component scores for the two vectors were both positive on average for the frail/prefrail group and negative on average for the non-frail group, the reconstructed waveforms with positive and negative deviations from the mean can be interpreted as the extreme gait characteristics of frail/prefrail and non-frail participants, respectively.
Importantly, the reconstructed waveforms in the current study indicated that the gait characteristics of frail/prefrail participants exhibited greater within-participant variability in the knee- and ankle-joint angles compared with non-frail participants (see Fig. 1). This greater variability in the knee- and ankle-joint angles of frail/prefrail participants compared with that of non-frail participants could potentially contribute to increased variability in spatiotemporal parameters. In accord with this possibility, a significant positive correlation was found between the principal component scores of the principal component vectors used for reconstruction of waveforms and the variability of stride time (r = 0.269) as well as the variability of stance time percentage (r = 0.259) (see Table 4). Regarding spatiotemporal parameters, the variability of stride time and stance time percentage were significantly greater in frail/prefrail participants (an increase of approximately 1.3 times compared with those in non-frail participants; Table 3). Previous studies also reported greater variability in spatiotemporal parameters in frail older adults17,18,24,25. Two studies using the same definition of frailty status as that used in the current study examined a combined sample of both males and females17,18. First, Montero-Odasso et al.17 reported that variability of stride time was approximately 1.3 times greater in prefrail older adults compared with that in non-frail older adults, and approximately 1.6 times greater in frail older adults. Second, Ritt et al.18 reported that variability of stride time was approximately 1.3 times greater in prefrail and frail older adults compared with that in non-frail older adults. These findings are similar to the increased variability of stride time in frail/prefrail participants found in the current study. These results suggest that, in frail older women, the variability in spatiotemporal parameters (stride time, stance time percentage) may increase because of greater variability in the knee- and ankle-joint angles during walking. This increased variation in joint angles was not observed in the pelvis or hip joints (see Fig. 1). Although they did not examine frail older people specifically, previous studies have reported that aging is associated with decreased muscle activity during walking and decreased proprioception in distal areas compared with that in proximal areas43,44. One previous study of frail older adults reported that gait variability of frail older adults was associated with quadriceps quality45. Therefore, we speculate that these aging and frailty-related phenomena may affect the knee and ankle joints, possibly increasing the variability of joint angle in frail participants.
The reconstructed average joint angle waveforms revealed that frail/prefrail participants tended to exhibit smaller pelvis front and horizontal plane movement, hip extension, knee flexion and ankle plantar-flexion angles (see Fig. 2). These observations are well-known characteristics among older people with slow walking speed46,47,48. In the current study, the walking speed of frail/prefrail participants was slower than that of non-frail participants (non-frail: 1.43 m/s, frail/prefrail: 1.35 m/s, Table 3). These overall walking speeds were faster than those reported in a previous study that used the same definition of frailty and included female participants only, but shows the same trend of slower speed in frail/prefrail participants compared with that in non-frail participants (non-frail: 0.95 m/s, frail/prefrail: 0.62 m/s)49. In addition, several previous studies that included both males and women reported a similar trend (non-frail: 1.03–1.4 m/s, prefrail; 0.92–1.4 m/s, frail: 0.64–1.30 m/s,17,19,28,50,51,52,53,54. Significant correlations with walking speed were found in the principal component scores of vectors 2, 3, 6, 15 and 17 (Table 4). Among these vectors, only vector 6 exhibited a significant difference between frailty status groups. Therefore, we concluded that the joint kinematics features related to vector 6 were the joint kinematics features associated with frailty. Thus, we reconstructed a waveform with principal component vector 6 and produced waveforms for frail/prefrail participants with smaller pelvis front and horizontal plane movement, hip extension, knee flexion and ankle plantar-flexion angles (see Supplementary Fig. S4). On the basis of these results, we hypothesize that these decreases in joint angle during walking could lead to a decrease in the stride length regardless of frailty status, leading to slower walking speed. Slow walking speed has also been adopted as one of the criteria for the definition of frailty by Fried et al.6, and has been reported to provide a good reflection of frailty status6,19,20,21,22. It is therefore not surprising that frail older women exhibited a slower walking speed than non-frail older women in the current study. Moreover, because walking speed is related to joint angle, the finding that frail older women exhibited a significantly lower joint angle than non-frail older women may be expected. Among the principal component vectors associated with frailty, walking speed was significantly correlated with principal component vector 6, but not with vector 9 (see Table 4). This result indicates that only the joint kinematics related to principal component vector 6, and not those related to vector 9, affected gait speed. Reconstructing a waveform with only vector 9 reduced the differences in joint angles between frail/prefrail participants and non-frail participants that were observed in Fig. 2, which was reconstructed with vectors 6 and 9, and Supplementary Fig. 4, which was constructed with vector 6 only (see Supplementary Fig. S6). In addition, the waveform reconstructed with only vector 9 exhibited greater within-participant variability in the knee- and ankle-joint angles of frail/prefrail participants compared with the other waveforms (see Supplementary Fig. S5). Therefore, knee and ankle joint variability (the joint kinematics features related to vector 9) may capture the gait characteristics of frail older women that are not affected by the change in walking speed associated with the frailty status of participants.
These types of variability can be measured using several easy-to-use ambulatory devices, in addition to 3D motion analysis systems. One previous study proposed a new ambulatory measurement method for measuring 3D knee joint angle during walking using two wearable inertial measurement units, each of which consists of a tri-axial gyroscope and an accelerometer55. Other studies reported that measurement using wearable inertial motion sensors and in-shoe pressure sensors provided a reliable method for measuring lower extremity joint kinetics during walking56. The variability of gait reflects complex physiological changes, such as neural control, muscle function, postural control and cardiovascular function57. Thus, the large joint angle variability observed in the current study may reflect physiological changes in frail older women. The change from a healthy state to a frail state in older people could potentially be detected early by observing joint variability. The measurement of frailty-related joint angle variability could be performed easily at health checkups, community clinics, or at home. Simple measurement methods introduced in previous studies could be applied to older adults, which would be useful for elucidating the physiological changes associated with frailty and establishing systems for early detection. Further research will be needed to develop such methods in the future.
Limitations
The present study involved several limitations that should be noted. First, soft tissue artifacts may have caused a bias in the observed plane angles, particularly in the hip and knee joints. Although we placed markers on the body’s bony landmarks, the existence of such artifacts should be considered. Second, the participants in the current study were 30 asymptomatic older women with relatively fast gait speeds (1.39 m/s on average). Thus, the findings may not be generalizable to some patient populations or target groups. Nevertheless, the current findings provide an important basis for further validation of methods for identifying the characteristic features of joint kinematics during walking that are associated with frailty in different target groups. Further data accumulation and analyses from various perspectives, such as the dominant and non-dominant legs and asymmetry, may provide new insights to inform the development of an accurate model for distinguishing frailty and the trajectory of frailty-related gait deterioration among older adults, particularly those with diseases or disorders.
Conclusions
In the current study, principal component analysis was used to identify the key characteristic features of joint kinematics of gait related to frailty status. Statistical analyses revealed that only principal component vectors 6 and 9 were related to frailty. We recombined the joint kinematics corresponding to these vectors and found greater variability of knee- and ankle-joint angles in the sagittal plane while walking in frail older women, compared with that in non-frail older women. Therefore, these results suggest that greater variability of the knee- and ankle-joint angles in the sagittal plane are characteristic features of joint kinematics during walking in frail older women. Depending on the findings of future validation studies, the measurement of variability may constitute part of a useful tool for evaluating frailty in both clinical and research settings.
Methods
Participants
Thirty healthy community-dwelling older females aged 60 and older who were able to walk independently were recruited for the study. Participants were excluded if they: (1) needed assistive devices (e.g., canes, crutches, or orthotic devices); (2) underwent surgery for trauma or orthopedic diseases; (3) had neurological disorders; and/or (4) regularly engaged in competitive sports on a professional level. All of the participants were capable of walking independently without assistive devices, had normal or corrected-to-normal vision, and had no diseases that they were aware of. Participants were asked to maintain their normal dietary habits and refrain from vigorous physical activity the day before and immediately before the experiment. The experimental protocol was approved by the ethical review board at the National Institute of Advanced Industrial Science and Technology (AIST), and all participants gave written informed consent before participating. The research complied with the principles of the Declaration of Helsinki.
Definition of frailty
Many definitions of frailty have been proposed. Fried et al. used five criteria (weight loss, slowness, weakness, exhaustion, and low activity) to identify frailty6. Fried’s phenotype criteria are the most widely cited criteria and focus on physical frailty25,58,59,60. Rockwood et al. developed a frailty index based on impairments in cognitive status, mood, motivation, communication, mobility, balance, bowel and bladder function, activities of daily living, nutrition, social resources and number of comorbidities61. Mitnitski et al. constructed a frailty index based on 20 deficits as observed in a structural clinical examination based on the comprehensive geriatric assessment (CGA)62. Jones et al. also based their frailty index based on the CGA, which included 10 standard domains to construct a three-level frailty index permitting risk stratification of future adverse outcomes63. In addition, Chin et al. compared three different working definitions of frailty: inactivity plus low energy intake, inactivity plus weight-loss and inactivity plus low body mass index64. Although many definitions of frailty have been proposed, because the current study was focused was on kinematic characteristics during walking and frailty status, we used Fried’s frailty criteria (the revised Japanese version)6,65, which is the most widely used frailty phenotype assessment tool. We assessed weight loss by asking a single “yes or no” question, “Have you lost 2–3 kg or more of your body weight in the past 6 months?” Slowness was established using a cutoff of < 1.0 m/s. We assessed weakness using maximum grip strength using a Smedley-type dynamometer (TKK 5401; Takei Scientific Instruments Co., Tokyo, Japan) and a sex-specific cutoff (< 26 kg for males and < 18 kg for females). We assessed exhaustion with a “yes or no” question: “In the last 2 weeks, have you felt tired without a reason?” We assessed low activity using the following two questions: “Do you engage in moderate levels of physical exercise or sports aimed at health?” and “Do you engage in low levels of physical exercise aimed at health?” If participants responded “No” to these two questions, they were classified as having low physical activity. Participants whose responses did not correspond to any of these target criteria were considered to be robust, those who met one or two criteria were considered prefrail, and those who met three or more criteria were considered frail. In this model, we combined frail and prefrail participants into a frail/prefrail group because of the limited number of frail participants.
Definition of sarcopenia
Although several criteria have been proposed to define sarcopenia, the recently reported criteria of the Asian Working Group for Sarcopenia (AWGS 2019) were applied in this study66. The skeletal muscle mass index was measured using dual energy X-ray absorptiometry with a bioelectrical impedance data acquisition system (Inbody 770; Biospace Co, Ltd, Seoul, Korea). Low muscle mass was defined as a skeletal muscle index value of less than 7.0 kg/m2 in males and less than 5.7 kg/m2 in females. Low muscle strength was defined as handgrip strength < 28 kg for males and < 18 kg for females. Criteria for low physical performance was 6-m walk < 1.0 m/s. Sarcopenia was defined as “low muscle mass + low muscle strength or low physical performance”, and severe sarcopenia was defined as “low muscle mass + low muscle strength and low physical performance”.
Gait measurement
Gait measurement was performed in a room with a straight 10-m path on which the participants could walk. All participants wore the same type of clothing during the experiment (sleeveless shirt and spats), which was provided by the experimenter. The clothing size was selected by participants. During gait measurement, participants were asked to walk barefoot at a comfortable, self-selected speed. Three-dimensional (3D) positional data were obtained during walking, using reflective markers and 10-camera and a 3D motion capture system (MAC3D, Motion Analysis Corporation, California, USA) with a 200 Hz sampling frequency. A total of 57 infrared reflective markers were attached in accordance with the guidelines of the Visual 3D software (C-Motion Inc., Rockville, MD, US). Simultaneously, ground reaction forces (GRFs) were obtained using four force plates (BP400600-2000, AMTI, Watertown, MA, US) sampled at 2000 Hz. Before the walking trials, the positions of the markers were recorded while participants stood stationary. The participants were then given sufficient practice walking to ensure a natural gait. After the practice, five successful trials per each leg were recorded, in which each participant correctly stepped on a force plate.
Data analysis
The raw motion and GRF data were digitally filtered using a zero-lag, fourth-order, low-pass Butterworth filter; the filter cut-off frequencies were 10 Hz for the positional data and 56 Hz for the GRF data based on a previous study67. The angles of the hip, knee, and ankle joints, and the pelvis-link angle during one gait cycle were calculated for the x-axis (i.e., flexion–extension), y-axis (i.e., abduction–adduction), and z-axis (i.e., internal–external rotation) using a Cardan sequence of rotations (X–Y-Z) from the trajectories measured in each trial. Based on a previous study40, the angles were time-normalized using the gait cycle duration determined from the force plate data and divided into 51 variables ranging from 0 to 100%. Therefore, each trial corresponded to a dataset of 612 variables (51 time points, four angles in three axes). Means and within-participants coefficients of variation of walking speed, stride length, step width, stride time, stance time, swing time, and stance time percentage were also determined, to help understand the gait characteristics. Low-pass filtering, variable calculation (i.e., joint and link angles, and spatiotemporal parameters), and time normalization processes were performed using Visual 3D software.
Statistical analysis
Statistical analyses were performed using the Statistical Package for the Social Sciences version 15.0 (SPSS Inc., USA). Principal component analysis is a multivariate statistical technique for analyzing data waveforms based on their variance, and has been used in various biomechanical studies to identify the movement characteristics of various groups under various conditions33,34,35,36,37. We therefore expected that principal component analysis analyses could be used to determine the relationship between the gait patterns observed during normal walking, as represented by the principal component vectors, and the states of frailty. The specific principal component analysis procedure and kinematic waveform reconstruction were conducted using the method reported by Kobayashi et al.38,39,40,41,42. Briefly, in our study, the following six steps were used to conduct the principal component analysis. First, the the intra-participant average and SDs were calculated for each time point within the five trials of data obtained from each leg of each participant. Second, mean centering was conducted on each of 1224 variables (i.e., averages and SDs for 51 time points, four angles in three axes) using the z-score:
where zt is the z-score for the parameter t, Xt is the raw data of the parameter t, μt is the mean of the parameter t for the participant, and σt is SD of the parameter t. Third, input matrices of 60 data points (each leg of 30 participants) by 1224 variables were constructed. Fourth, principal component vectors were extracted until their cumulative ratio attained 84% of the total variance. Fifth, the statistical analyses described in the next subsection were conducted to identify the main effects of frailty status on the joint kinematic characteristics represented by the principal component vectors. Finally, for each principal component vector, simulated kinematic waveforms were reconstructed from the principal component scores with very large or very small values (deviating from the mean by three SDs), to interpret data on the average joint angle and joint angle variability corresponding to the principal component vectors. If there were significant differences between the principal component scores obtained from frail/prefrail participants and those obtained from non-frail participants for a certain principal component vector, the joint kinematics corresponding to this vector were interpreted as key characteristic features of joint kinematics of walking that are related to the states of frailty. Univariate analysis was conducted on the principal component scores between two groups using independent t-tests, in the same way that the differences between the principal component vectors of different groups were tested in previous studies34,35. Furthermore, we also calculated Cohen’s d effect size to validate the results of the t-test according to the recommendation by Lakens68 and interpreted the results using 0.2 for a small effect, 0.5 for a moderate effect, and 0.8 for a large effect, according to previously reported guidelines69. In addition, we conducted independent t-tests to analyze differences (central tendencies and variability) between the following parameters: walking speed, stride length, step width, stride time, stance time, swing time, and stance time percentage. Furthermore, we determined the Pearson’s product-moment correlation coefficients between the principal component vector related to the states of frailty and the above-mentioned parameters. Differences were considered statistically significant when p-values were < 0.05.
Data availability
All data needed to evaluate the conclusions in the paper are present in the paper, Supplementary Material, and/or references cited within.
References
Dent, E. et al. Physical frailty: ICFSR international clinical practice guidelines for identification and management. J. Nutr. Health Aging 23, 771–787 (2019).
Hoogendijk, E. O. et al. Self-perceived met and unmet care needs of frail older adults in primary care. Arch. Gerontol. Geriatr. 58, 37–42 (2014).
Chode, S., Malmstrom, T. K., Miller, D. K. & Morley, J. E. Frailty, diabetes, and mortality in middle-aged African Americans. J. Nutr. Health Aging 20, 854–859 (2016).
Vermeiren, S. et al. Gerontopole Brussels Study group. Frailty and the prediction of negative health outcomes: A meta-analysis. J. Am. Med. Dir. Assoc. 1163, e1–e1163 (2016).
Topinková, E. Aging, disability and frailty. Ann. Nutr. Metab. 52, 6–11 (2008).
Fried, L. P. et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 563, M146–M156 (2001).
Kane, A. E. & Howlett, S. E. Sex differences in frailty: Comparisons between humans and preclinical models. Mech. Ageing Dev. 198, 111546 (2021).
Collard, R. M., Boter, H., Schoevers, R. A. & Oude, V. R. C. Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 60, 1487–1492 (2012).
Gordon, E. H. et al. Sex differences in frailty: A systematic review and meta-analysis. Exp. Gerontol. 89, 30–40 (2017).
Ofori-Asenso, R. et al. Global incidence of frailty and prefrailty among community-dwelling older adults: A systematic review and meta-analysis. JAMA Netw. Open 2, e198398 (2019).
Ryan, J. et al. Validation of a deficit-accumulation Frailty Index in the ASPREE study and its predictive capacity for disability-free survival. J. Gerontol. A Biol. Sci. Med. Sci. 2, 225 (2021).
World Health Organization. World Report on Ageing and Health (WHO, 2015).
Kim, M. J. et al. Mobility performance tests for discriminating high risk of frailty in community-dwelling older women. Arch. Gerontol. Geriatr. 51, 192–198 (2010).
Newman, A. B. et al. Associations of subclinical cardiovascular disease with frailty. J. Gerontol. A Biol. Sci. Med. Sci 56, M158–M166 (2001).
Lang, P. O. et al. Frailty syndrome: A transitional state in a dynamic process. Gerontology 55, 539–549 (2009).
Noguerón García, A. et al. Gait plasticity impairment as an early frailty biomarker. Exp. Gerontol. 142, 111137. https://doi.org/10.1016/j.exger.2020.111137 (2020).
Montero-Odasso, M. et al. Gait variability is associated with frailty in community-dwelling older adults. J. Gerontol. A Biol. Sci. Med. Sci. 66, 568–576 (2011).
Ritt, M. et al. High-technology based gait assessment in frail people: Associations between spatio-temporal and three-dimensional gait characteristics with frailty status across four different frailty measures. J. Nutr. Health Aging 21, 346–353 (2017).
Navarrete-Villanueva, D. et al. Frailty and physical fitness in elderly people: A systematic review and meta-analysis. Sports Med. 51, 143–160 (2021).
Binotto, M. A., Lenardt, M. H. & Rodríguez-Martínez, M. D. C. Physical frailty and gait speed in community elderly: A systematic review. Rev. Esc. Enferm. USP 52, e03392 (2018).
Pamoukdjian, F. et al. Measurement of gait speed in older adults to identify complications associated with frailty: A systematic review. J. Geriatr. Oncol. 6, 484–496 (2015).
Jung, H. W. et al. Usual gait speed is associated with frailty status, institutionalization, and mortality in community-dwelling rural older adults: A longitudinal analysis of the aging study of pyeongchang rural area. Clin. Interv. Aging 13, 1079–1089 (2018).
Theou, O., Jones, G. R., Jakobi, J. M., Mitnitski, A. & Vandervoort, A. A. A comparison of the relationship of 14 performance-based measures with frailty in older women. Appl. Physiol. Nutr. Metab. 36, 928–938 (2011).
Theou, O., Jakobi, J. M., Vandervoort, A. A. & Jones, G. R. A comparison of physical activity (PA) assessment tools across levels of frailty. Arch. Gerontol. Geriatr. 54, e307–e314 (2012).
Martínez-Ramírez, A. et al. Frailty assessment based on trunk kinematic parameters during walking. J. Neuroeng. Rehabil. 12, 48 (2015).
Moe-Nilssen, R. & Helbostad, J. L. Interstride trunk acceleration variability but not step width variability can differentiate between fit and frail older adults. Gait Posture 21, 164–170 (2005).
Kressig, R. W. et al. Temporal and spatial features of gait in older adults transitioning to frailty. Gait Posture 20, 30–35 (2004).
Schwenk, M. et al. Frailty and technology: A systematic review of gait analysis in those with frailty. Gerontology 60, 79–89 (2014).
Brown, M., Sinacore, D. R., Binder, E. F. & Kohrt, W. M. Physical and performance measures for the identification of mild to moderate frailty. J. Gerontol. A Biol. Sci. Med. Sci. 55, M350–M355 (2000).
Caballero-Mora, M. A. et al. Factors associated with impairment in gait speed in older people with clinically normal gait. A cross-sectional study. Aging Clin. Exp. Res. 32, 1043–1048 (2020).
Pradeep Kumar, D. et al. Sensor-based characterization of daily walking: A new paradigm in pre-frailty/frailty assessment. BMC Geriatr. 20, 164 (2020).
Nigg, B. M., Baltich, J., Maurer, C. & Federolf, P. Shoe midsole hardness, sex and age effects on lower extremity kinematics during running. J. Biomech. 45, 1692–1697 (2012).
Wrigley, A. T., Albert, W. J., Deluzio, K. J. & Stevenson, J. M. Differentiating lifting technique between those who develop low back pain and those who do not. Clin. Biomech. 20, 254–263 (2005).
Raptopoulos, L. S., Dutra, M., Castro Pinto, F. A. & de Pina Filho, A. C. Alternative approach to modal gait analysis through the Karhunen-Loève decomposition: An application in the sagittal plane. J. Biomech. 39, 2898–2906 (2006).
Deluzio, K. J. & Astephen, J. L. Biomechanical features of gait waveform data associated with knee osteoarthritis: An application of principal component analysis. Gait Posture 25, 86–93 (2007).
Maurer, C., Federolf, P., von Tscharner, V., Stirling, L. & Nigg, B. M. Discrimination of gender-, speed-, and shoe-dependent movement patterns in runners using full-body kinematics. Gait Posture 36, 40–45 (2012).
Federolf, P. A., Boyer, K. A. & Andriacchi, T. P. Application of principal component analysis in clinical gait research: Identification of systematic differences between healthy and medial knee-osteoarthritic gait. J. Biomech. 46, 2173–2178 (2013).
Kobayashi, Y., Hobara, H., Matsushita, S. & Mochimaru, M. Key joint kinematic characteristics of the gait of fallers identified by principal component analysis. J. Biomech. 47, 2424–2429 (2014).
Kobayashi, Y., Hobara, H., Heldoorn, T. A., Kouchi, M. & Mochimaru, M. Age-independent and age-dependent sex differences in gait pattern determined by principal component analysis. Gait Posture 46, 11–17 (2016).
Nakajima, K., Kobayashi, Y., Tada, M. & Mochimaru, M. Evaluation of plantar pressures in people with hallux valgus using principal component analysis. Technol. Health Care 26, 667–674 (2018).
Kobayashi, Y. & Ogata, T. Association between the gait pattern characteristics of older people and their two-step test scores. BMC Geriatr. 18, 101 (2018).
Hida, N., Fujimoto, M., Ooie, T. & Kobayashi, Y. Effects of footwear fixation on joint angle variability during straight gait in the elderly. Gait Posture 86, 162–168 (2021).
Shaffer, S. W. & Harrison, A. L. Aging of the somatosensory system: A translational perspective. Phys. Ther. 7, 193–207 (2007).
Ihira, H. et al. Differences between proximal and distal muscle activity of the lower limbs of community-dwelling women during the 6-minute walk test. J. Phys. Ther. Sci. 24, 205–209 (2012).
Martinikorena, I. et al. Gait variability related to muscle quality and muscle power output in frail nonagenarian older adults. J. Am. Med. Dir. Assoc. 17, 162–167 (2016).
Murray, M. P., Kory, R. C. & Clarkson, B. H. Walking patterns in healthy old men. J. Gerontol. 24, 169–178 (1969).
Kerrigan, D. C., Lee, L. W., Collins, J. J., Riley, P. O. & Lipsitz, L. A. Reduced hip extension during walking: Healthy elderly and fallers versus young adults. Arch. Phys. Med. Rehabil. 82, 26–30 (2001).
Judge, J. O., Davis, R. B. & Ounpuu, S. Step length reductions in advanced age: The role of ankle and hip kinetics. J. Gerontol. A Biol. Sci. Med. Sci. 51, M303–M312 (1996).
Parentoni, A. N. et al. Gait speed as a predictor of respiratory muscle function, strength, and frailty syndrome in community-dwelling elderly people. J. Frailty Aging 4, 64–68 (2015).
Verghese, J. & Xue, X. Identifying frailty in high functioning older adults with normal mobility. Age Ageing 39, 382–385 (2010).
Curcio, C. L., Henao, G. M. & Gomez, F. Frailty among rural elderly adults. BMC Geriatr. 14, 2 (2014).
Tay, L. B. et al. Multidomain geriatric screen and physical fitness assessment identify prefrailty/frailty and potentially modifiable risk factors in community-dwelling older adults. Ann. Acad. Med. Singap. 48, 171–180 (2019).
Arakawa, M. B. et al. Frailty prevalence using Frailty Index, associated factors and level of agreement among frailty tools in a cohort of Japanese older adults. Arch. Gerontol. Geriatr. 84, 103908 (2019).
Jansen, C. P. et al. The association between motor capacity and mobility performance: Frailty as a moderator. Eur. Rev. Aging Phys. Act. 16, 16 (2019).
Favre, J., Jolles, B. M., Aissaoui, R. & Aminian, K. Ambulatory measurement of 3D knee joint angle. J. Biomech. 41, 1029–1035 (2008).
Khurelbaatar, T., Kim, K., Lee, S. & Kim, Y. H. Consistent accuracy in whole-body joint kinetics during gait using wearable inertial motion sensors and in-shoe pressure sensors. Gait Posture 42, 65–69 (2015).
Hausdorff, J. M. Gait variability: methods, modeling and meaning. J. Neuroeng. Rehabil. https://doi.org/10.1186/1743-0003-2-19 (2005).
Bouillon, K. et al. Measures of frailty in population-based studies: An overview. BMC Geriatr. 13, 64 (2013).
Buta, B. J. et al. Frailty assessment instruments: Systematic characterization of the uses and contexts of highly-cited instruments. Ageing Res. Rev. 26, 53–61 (2016).
Pritchard, J. M. et al. Measuring frailty in clinical practice: A comparison of physical frailty assessment methods in a geriatric out-patient clinic. BMC Geriatr. 17, 264 (2017).
Rockwood, K. et al. A brief clinical instrument to classify frailty in elderly people. Lancet 353, 205–206 (1999).
Mitnitski, A. B., Graham, J. E., Mogilner, A. J. & Rockwood, K. Frailty, fitness and late-life mortality in relation to chronological and biological age. BMC Geriatr. 2, 1–8 (2002).
Jones, D. M., Song, X. & Rockwood, K. Operationalizing a frailty index from a standardized comprehensive geriatric assessment. J. Am. Geriatr. Soc. 52, 1929–1933 (2004).
Chin, A. et al. Inactivity and weight loss: Effective criteria to identify frailty. J. Nutr. Health Aging 7, 55–60 (2003).
Satake, S. & Arai, H. The revised Japanese version of the Cardiovascular Health Study criteria (revised J-CHS criteria). Geriatr. Gerontol. Int. 20, 992–993 (2020).
Chen, L. K. et al. Asian Working Group for Sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 21, 300–307 (2020).
van den Bogert, A. J., & de Koning, J. J. On optimal filtering for inverse dynamics analysis. In Proc. IXth Biennial Conference of the Canadian Society for Biomechanics, 214–215 (1996).
Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 4, 863 (2013).
Cohen, J. Statistical Power Analysis for the Behavioral Sciences (Academic Press, 2013).
Kato, T. et al. Differences in lower limb muscle strength and balance ability between sarcopenia stages depend on sex in community-dwelling older adults. Aging Clin. Exp. Res. https://doi.org/10.1007/s40520-021-01952-6 (2021).
Pasco, J. A. et al. Dynapenia and low cognition: A cross-sectional association in postmenopausal women. J. Clin. Med. 10, 173 (2021).
Juppi, H. K. et al. Role of menopausal transition and physical activity in loss of lean and muscle mass: A follow-up study in middle-aged finnish women. J. Clin. Med. 9, 1588 (2020).
Roche, N. et al. Effects of age, gender, frailty and falls on spatiotemporal gait parameters: A retrospective cohort study. Eur. J. Phys. Rehabil. Med. 57, 923 (2021).
Acknowledgements
The authors are grateful to all participants as well as Ms. Sayuri Matsubara, Ms. Nami Yasumatsu and Ms. Saori Ohtani for their technical assistance in data acquisition and analysis. We thank Benjamin Knight, MSc., from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Author information
Authors and Affiliations
Contributions
W.T., T.O. and Y.K. conceived the project, designed the experimental approach, conducted experiments, analyzed the data, and prepared the manuscript. K.I., M.H. and K.Y. analyzed the results and wrote the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tsuchida, W., Kobayashi, Y., Inoue, K. et al. Kinematic characteristics during gait in frail older women identified by principal component analysis. Sci Rep 12, 1676 (2022). https://doi.org/10.1038/s41598-022-04801-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-04801-2
- Springer Nature Limited
This article is cited by
-
Stroke walking and balance characteristics via principal component analysis
Scientific Reports (2024)