
Abstract
Osteoporosis is the most common metabolic bone disease. The complications of osteoporosis have influence on people's lives and lead to anxiety and depression. The aim of this study was to determine the relationship between osteoporosis and depression among Iranian patients. This cross-sectional analytical survey study conducted among 500 patients referred to a Bone Densitometry Center in Iran. They were assigned into with osteoporosis group (n = 250) and non-affected group (n = 250). The Persian version of the 13-item Beck Depression Inventory (BDI) was used to assess depression. ANOVA, independent t-test, chi-square were used to compare the data. All analyses were done using SPSS version 22 software. A P value ≤ 0.05 represented statistical significance. The majority of people with osteoporosis (86.9%), suffered from mild to moderate depression and the majority of normal people (84.6%) were non-depressed. The mean scores (SD) of depressions in the patients with osteoporosis and normal status was 6.94 (2.39) and 2.50 (1.01), respectively. Statistical analyses showed that the mean scores of depressions significantly different between the two groups (P < 0.05). The results indicate that depression is associated with osteoporosis. As a result, physicians are expected to pay attention to depression in people with osteoporosis and to treat it.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Osteoporosis is now recognized as a public health problem and is known as the silent disease of the century. It is the most common metabolic bone disease, which appears as bone mass reduction and the resulting complications (fracture), impose high and irreparable financial and physical harm to society and patients1,2,3,4,5. The most common and serious complications of osteoporosis are fractures, which is about 1.5 million fractures every year6,7. In the United Kingdom and the United States about 7.1 billion pounds and 18 billion dollars a year are spent on these fractures8. Also, a pelvic fracture alone in the first year in European countries, costs about 20,000 dollars to treat9. Therefore, the importance of this disease is associated with increased fractures in the femur, pelvic and spinal areas10.
Factors that increase the chances of osteoporosis in a person include uncontrollable factors, such as familial history of osteoporosis, aging, female gender, menopause, small body and controllable factors such as cigarette smoking, alcohol, low body mass index, sedentary lifestyle, lack of calcium and vitamin D intake, high levels of sodium, protein and caffeine intake, lack of adequate intake of fruits and vegetables, as well as medical and pharmaceutical factors such as long-term corticosteroid use, and diseases such as Rheumatoid Arthritis, thyroid and parathyroid disorders11,12,13,14.
Chronic illnesses may have several negative consequences that may lead to psychological worries such as depression15. The complications of osteoporosis influence on people's lives and lead to anxiety and depression, limitation of activity, acute and chronic pain, difficulty in doing daily routine, dependency to others, and change in social interactions, and ultimately affect the quality of life of suffering people16. Depression with some changes in the hormonal system, such as increase in cortisol and decrease in sex hormones, can lead to reduction in bone mineral density17.
Depression is one of the most common psychiatric disorders and also the most common mood disorder, which has multi-factorial etiology. It affects 25% of men and 12% of women in their life spans18,19. Researches show that every year in the United States about 19 million people experience depression. According to the research conducted in Iran, about 7 million people suffer from a kind of mental disorder, and about 15–25% of the population experience mild to severe depression. This disorder is a common disorder that affects 15% of people at least once in a lifetime. It is also anticipated that the number of depressed people is rising due to pressures from social change, the environment, and some physical illnesses20.
Some studies have shown a relationship between depression and osteoporosis. It is reported that people with depression, are at a high risk for osteoporosis21,22. Various studies have reported multiple biological mechanisms are associated with both depression and osteoporosis. Depression is associated with a decrease in estrogen and testosterone levels. Additionally, depression is an inflammatory state associated with multiple cytokines such as alpha tumor necrosis factor and IL-6, which results in apoptosis of osteoclasts. In depression, with the disruption of the HPA axis, cortisol plasma levels increase, all of which ultimately leads to reduction in bone density23. In another study, it has been shown that in depressed people, levels of 25-hydroxy vitamin D decrease and levels of parathyroid hormone increase24, which both can lead to bone loss.
Barbour et al. reported that there is a relationship between increasing inflammatory markers and pelvic fracture25. The mechanism of TCA anti-depressant drugs is not clear in bone density reduction, but the complications of these drugs, such as orthostatic hypotension, vertigo and balance disturbance, can lead to falling down and bone fractures26. Studies have shown that bone marrow cells have serotonin 5-HT2 receptors. Serotonin plays a key role in bone metabolism. So, the use of SSRI drugs in depressed patients leads to bone density reduction27.
Considering the contradictory results of studies on the association between depression and osteoporosis, the present study was conducted to determine the relationship between depression and osteoporosis to improve the health of the community.
Methods
Study design and participants
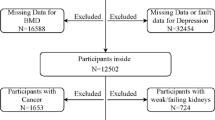
This cross-sectional analytical survey study conducted among patients referred to a Bone Densitometry Center in Iran. To calculate sample size, we used \(n = \frac{{\left( {Z_{1 - \alpha /2} \cdot \sqrt {2\overline{P}(1 - \overline{P})} + Z_{1 - \beta } \cdot \sqrt {P_{1} (1 - P_{1} ) + P_{2} (1 - P_{2} )} } \right)^{2} }}{{d^{2} }}\), where \(\overline{P}\) = 41.5, \(Z_{1 - \alpha /2}\) = 95%, \(Z_{1 - \beta }\) = 80%, P1 = 40%, P2 = 43%, d = 0.05. Based onminimum sample size of the obtained 290. In order to improve the power of study, we selected 500 patients (250 patients in each group). In this study, randomized sampling was used; so that among all individuals referring to the bone densitometry center, 250 patients with diagnosis of osteoporosis, were selected as osteoporosis group. Also, to determine the non-osteoporotic group, among the list of referrals to the center, 250 patients who confirmed not having osteoporosis, had been randomly selected as the normal group. Inclusion criteria included persons aged 35 years and older, no history of corticosteroid use for more than 6 months, no history of anticonvulsant use, no history of liver, renal, pulmonary, thyroid, parathyroid and skeletal diseases, insulin-dependent diabetes, autoimmune diseases such as rheumatoid arthritis, no history of osteoporosis treatment, no history of hysterectomy and ovariectomy before menopause, no history of precocious menopause, no history of infertility and no eating disorders. The aims of the study and procedure of the research was explained to the patients, participation was entirely voluntary, written consent was obtained, and the questionnaires were submitted anonymously. The patients filled out the questionnaire in a private and quiet room on the center. The Scientific and Ethics Committee of Shiraz University of Medical Sciences approved the research project (IR.SUMS.MED.REC.1398.308).
Measures
The survey was made up of the following questionnaires:
Demographic information
The following demographic information were measured by a research-made questionnaire: sex, age, BMI, education level, job type, smoking, alcohol consumption, taking calcium, income status, and history of fracture.
Depression
The Persian version of the 13-item Beck Depression Inventory (BDI) was used to assess depression. This form is one of the best Standard questionnaires used to evaluation of depression. The BDI is an international standard which was invented by an American psychologist Dr. Beck in 196028. The satisfactory psychometric properties of the Persian version 13-item BDI used have been reported by Rajabi et al.29. The Cronbach's alpha and split-half coefficient for the questionnaire were 0.82 and 0.8930. In this questionnaire, the score for each question is 0–3 and the score of 21 is the highest score. The score of 0–4 consider as non-depressed, the score of 5–7 as mild depression, score of 8–16 moderate depression, and over 16 consider as severe depression31.
Data analysis
All analyses were done using SPSS version 22 software (SPSS Inc., Chicago, IL, USA). A P value ≤ 0.05 represented statistical significance. The Kolmogorov–Smirnov (K–S) test was used for assessment of data distribution and ssumption of normality. The dependent variables were all normally distributed. Thus, To describe quantitative variables, we used mean and standard deviation, and qualitative variables were characterized by frequency and frequency percentage, as well as independent t-test, Chi-square, ANOVA were used to compare the data.
Ethical approval and consent to participate
The study procedures were carried out following the Declaration of Helsinki. This study was approved by the Ethics Committee of Shiraz University of Medical Sciences. There was an emphasis on maintaining privacy in keeping and delivering the information accurately without mentioning the names of the participants. The participants were given the right to leave the interview at any time if they wished to leave the interview process, and they were promised to have the study results if they want. Informed consent was taken from all the participants. For illiterate people involved, informed consent from a parent and/or legal guardian obtained in the study.
Results
In this study, 500 people referred to the Bone Densitometry Center were studied. 368 (73.6%) were female and 132 (26.4%) were male. More than half of them had a high school diploma and consisted of domestic women. Tables 1 and 2 shows demographic information of the participants. The distributions of sex, age, BMI, education level, job type, smoking, alcohol consumption, taking calcium, income status, and history of fracture did not significantly differ between the two groups.
Statistical analyses showed that there was no significant relationship between depression and BMI, sex, education level, job type,smoking, alcohol consumption, taking calcium, income status, and history of fracture variablesin osteoporosis patients (P > 0.05). But, pearson correlation coefficient test showed that there was a significant relationship between depression and age in osteoporosis patients (P < 0.05) (Table 3).
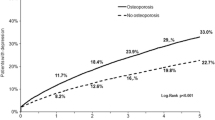
The mean scores (SD) of depressions in the patients with osteoporosis and normal status was 6.94 (2.39) and 2.50 (1.01), respectively. It should be noted that according to the standardized scores in BDI, a higher score indicates more severe depression in a person. Statistical analyses showed that the mean scores of depressions significantly different between the two groups (P < 0.001). The majority of people with osteoporosis (86.9%), suffered from mild to moderate depression and the majority of normal people (84.6%) were non-depressed.
Discussion
Regarding the comparison of the frequency distribution of demographic variables in two groups of people with osteoporosis and normal people, the findings showed that the two groups had the same demographic and underlying characteristics (age, level of education, sex, etc.), Which suggests the homogeneity of the studied groups. Study of Saei Gharenaz et al.18 is consistent with the results of this study.
The findings of this study indicate that there is a significant difference between bone density status and depression. In other words, people with osteoporosis have higher depression scores than normal people. In recent years, a number of studies have examined the relationship between depression and bone loss, which has controversial results.In the study of Cizza32, patients with major depressive disorder had lower bone density compared with the control group and the frequency of osteoporosis was higher. Eskandari et al.33 also reported in a study of pre-menopause women that depression is associated with a decrease in bone density. Michelson et al.16 also found significant correlation between depression and bone density in a case–control study in 24 women with major depression and 24 without depression. In another study, depressive disorder was associated with reduced bone mineral density in the spine, femoral neck and femur34. All of the above studies are consistent with the present study. But some researchers also reported contradictory results. The study of Saei Gharenaz et al.18 on Iranin women showed that depression was not significantly associated with osteoporosis. Ljubicic Bistrovic et al.21 and Ozsoy et al.31 also reported there is not a relationship between osteoporosis and depression which is not consistent with the results of this study. It seems the design method of the study and the study group and important behavioral factors such as lifestyle, culture, history of hormone therapy and the important factor of genetics can be the cause of this contradiction.
The results of this study showed that there is no relationship between depression and sex in people with osteoporosis. In this regard, Ozsoy et al.31 reported that there is no relationship between depression and bone loss in men and women in terms of gender. In studies by Patti et al.35 and Fallah et al.36, there was no statistically significant relationship between depression and sex, which confirms the findings of this study. The results of other studies also confirm this finding37,38,39. Oh et al.40 concluded in their study of Korean women aged 80–80 years that depression was associated with a decrease in bone density in men, but in women, depression did not correlate with decreased bone density, which is not consistent with the present study. The causes of this contradiction can be explained by the difference in age group and differences in the culture of the population under study.
The results of studies by Musarezaie et al.39, Fallah et al.36 and Chevalier et al.37 showed that there is no significant relationship between depression and age, which is not consistent with the present study. The heterogeneity of the research samples, the data collection tool, the difference in sample size, and the different entry and exit criteria in studies can be considered for possible reasons for this discrepancy.
The results of this study indicated that there was no correlation between depression and education level in osteoporosis patients. Studies by Musarezaie et al.39, Fallah et al.36 and Chevalier et al.37 suggest that there is a significant relationship between depression and staff educational status, which was not consistent with the present study. The heterogeneity of the research samples, the differences in the data collection tool, the differences in sample size, and the different entry and exit criteria in studies can be considered as the possible reasons for these inconsistencies.
The results of this study showed that there is no significant relationship between depression and job type and income status in osteoporosis patients. In the study of Khajavi et al.41, there was a significant negative relationship between employment and economic status with depression, meaning that with increasing employment and improving the economic status of participants in the study, the rate of depression decreased. In addition, there was no significant relationship between depression and history of fracture. Studies have suggested that many drugs prescribed for the treatment of depression, in addition to increasing the likelihood of falling down and thereby increasing the risk of fracture, also affect calcium metabolism. One study reported that depression was 3 times higher in patients with pelvic fracture than in the control group42, which is not consistent with the present study.
The results of this study showed that there was no correlation between depression and smoking in sin osteoporosis patients. Smoking is one of the factors affecting bone density43. Many studies indicate that there is a high rate of depression and anxiety in smokers44,45, which contrasts with the present study.
The limitations of the present study, included not being possible to generalize the study to the whole society as samples were selected from those referring to bone densitometry center; so that it may not present the general population as well. Answering and completing the questionnaire in this project considered as the satisfaction of participating in the study and the participants were assured that their information would stay confidential. Case–control” design used in this study is appropriate to confirm the well-known associations between osteoporosis and depression. However, such design it is not enough for proving that depression increases risk of osteoporosis. In addition, "clinical” sample as a control group can lead to bias. The participants of "main" group with the diseases forced them to seek medical help at the osteoporosis center, more likely could have symptoms such as fatigue, pain, weakness that may artificially inflate BDI-13 scores due to symptoms of the illness, rather than of depression. Despite, the study could be consider as a pilot for future wide population-based research in original population of Iran as well as the clinical research in osteoporosis.
Conclusion
According to the results of this study, which depression is associated with osteoporosis, depression should be considered as a risk factor for osteoporosis, such as smoking or low calcium intake. Also, the results of this study can be used as a guide for implementation of educational program in people with osteoporosis, in order to help their patients and their families to promote mental health, especially control and reduce depression.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
Abbreviations
- BMI:
-
Body mass index
References
Kasper, D. L. et al. Harrison’s Manual of Medicine (Mcgraw-Hill, 2005).
Munch, S. & Shapiro, S. The silent thief: Osteoporosis and women’s health care across the life span. Health Soc. Work 31(1), 44–53 (2006).
Risk WSGoAoF, Osteoporosis iAtSfP. Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Report of a WHO Study Group (World Health Organization, 1994).
Sturtridge, W., Lentle, B. & Hanley, D. The use of bone density measurement in the diagnosis and management of osteoporosis. Can. Med. Assoc. J. 155(7), 924–929 (1996).
Stamp, T. C. B. Osteoporosis. 111 Scott JT eCsTotRdL, Churchil- 1 Livingstone, l004–1008 (1986).
Forouzi, M. A. Z., Haghdoost, A., Saidzadeh, Z. & Mohamadalizadeh, S. Study of knowledge and attitude of Rafsanjanian female teachers toward prevention of osteoporosis. J. Birjand Univ. Med. Sci. 16(1), 71–78 (2009).
Malgo, F. et al. High prevalence of secondary factors for bone fragility in patients with a recent fracture independently of BMD. Arch. Osteoporos. 11(1), 12 (2016).
Bagheri, P. et al. Ultra analysis of prevalence of osteoporosis in Iranian women (2011).
NOFNAYaRAihno (2013).
Shobeiri, F. & Nazari, M. Age at menopause and its main predictors among Iranian women. Int. J. Fertil. Steril. 8(3), 267 (2014).
Shobeiri, F. & Nazari, M. Patterns of weight gain and birth weight amongst Indian women. Iran. J. Med. Sci. 31(2), 94–97 (2006).
Shobeiri, F. & Nazari, M. Assessment of cervical erosion in Hamedan city, Iran. Pak. J. Biol. Sci. PJBS 10(19), 3470–3472 (2007).
Salehi, I., Khazaeli, S., Najafizadeh, S. R., Ashraf, H. & Malekpour, M. High prevalence of low bone density in young Iranian healthy individuals. Clin. Rheumatol. 28(2), 173–177 (2009).
http://emri.tums.ac.ir/pages/mainpage.asp?I=S10M5P2C1. ORCOPICOAf.
Park, R., Goodyer, I. & Teasdale, J. Self-devaluative dysphoric experience and the prediction of persistent first-episode major depressive disorder in adolescents. Psychol. Med. 35(4), 539–548 (2005).
Michelson, D. et al. Bone mineral density in women with depression. N. Engl. J. Med. 335(16), 1176–1181 (1996).
Tolea, M., Black, S., Carter-Pokras, O. & Kling, M. Depressive symptoms as a risk factor for osteoporosis and fractures in older Mexican American women. Osteoporos. Int. 18(3), 315–322 (2007).
Saei Gharenaz, M., Ozgoli, G., Aghdashi, M. A. & Salmany, F. Relationship between depression and osteoporosis in women. Urmia Med. J. 26(1), 10–16 (2015).
ShahMiri, H. & Ghorayshi Zade, S. Relationship between coping strategies and demographic characteristics and severity of depression in patients with major depression. Med. J. Tabriz Univ. 28(1), 81–86 (2006).
Marofi, M. Prevalence of depressive symptoms among medical students and graduate physicians. Med. J. Jahrom Univ. 1(1), 1–4 (2003).
Ljubicic Bistrovic, I. et al. Connection of depression and bone loss in perimenopausal and postmenopausal women. Coll. Antropol. 36(4), 1219–1223 (2012).
Whooley, M. A., Cauley, J. A., Zmuda, J. M., Haney, E. M. & Glynn, N. W. Depressive symptoms and bone mineral density in older men. J. Geriatr. Psychiatry Neurol. 17(2), 88–92 (2004).
Barbour, K. E. et al. Inflammatory markers and the risk of hip fracture: The Women’s Health Initiative. J. Bone Miner. Res. 27(5), 1167–1176 (2012).
Vestergaard, P., Rejnmark, L. & Mosekilde, L. Anxiolytics, sedatives, antidepressants, neuroleptics and the risk of fracture. Osteoporos. Int. 17(6), 807–816 (2006).
Westbroek, I., van der Plas, A., de Rooij, K. E., Klein-Nulend, J. & Nijweide, P. J. Expression of serotonin receptors in bone. J. Biol. Chem. 276(31), 28961–28968 (2001).
Blazer, D. & Friedman, S. Depression in late life. Am. Fam. Phys. 20, 91–96 (1979).
Baghiani, M. M., Ehrampoush, M., Rahimi, B., Aminian, A. & Aram, M. Prevalence of depression among successful and unsuccessful students of Public Health and Nursing-Midwifery schools of Shahid Sadoughi University of Medical Sciences in 2008 (2012).
Rajabi, G. R. Psychometric properties of Beck depression inventory short form items (BDI-13). J. Iran. Psychol. 1(4), 291–298 (2005).
McDowell, I. Measuring Health: A Guide to Rating Scales and Questionnaires (Oxford University Press, 2006).
Shirazi Khah, M., Mousavi, M. & Sahaf, R. Study of health and social indicators of elderly women in Iran. Iran. J. Ageing 6, 66–78 (2012).
Ozsoy, S. et al. Is there any alteration in bone mineral density in patients with depression?. Turk. Psikiyatri Derg. 16(2), 77–82 (2005).
Cizza, G. Major depressive disorder is a risk factor for low bone mass, central obesity, and other medical conditions. Dialogues Clin. Neurosci. 13(1), 73–87. https://doi.org/10.31887/DCNS.2011.13.1/gcizza (2011).
Eskandari, F. et al. Low bone mass in premenopausal women with depression. Arch. Intern. Med. 167(21), 2329–2336 (2007).
Ağrısının, P. O. H. S. The effect of back pain on quality of life, sleep quality and depression in patients with postmenopausal osteoporosis. Turk. J. Osteoporosis 20, 6–9 (2014).
Patti, E. et al. Prevalence of anxiety and depression among emergency department staff. Nursing 48(2), 105–111 (2007).
Fallah, R., Farhadi, S., Amini, K. & Mohajeri, M. Prevalence of depression in personnel of Zanjan University of Medical Sciences. ZUMS J. 19(75), 107–113 (2011).
Chevalier, A. & Feinstein, L. The causal effect of education on depression 2004 [citado 2008 Jun 1].
Mahmodi, S. & Zehni, K. The comparison of depression prevalence between shift work nurses in education hospitals of Kurdistan Medical Sciences University. Iran. J. Nurs. Res. 8, 29–38 (2013).
Musarezaie, A., Momeni-Ghalehghasemi, T., Musarezaie, N., Moeini, M. & Khodaee, M. Investigate the prevalence of depression and its association with demographic variables in employees. Iran. J. Psychiatr. Nurs. 2(3), 37–45 (2014).
Oh, S. M., Kim, H. C., Ahn, S. V., Rhee, Y. & Suh, I. Association between depression and bone mineral density in community-dwelling older men and women in Korea. Maturitas 71(2), 142–146. https://doi.org/10.1016/j.maturitas.2011.11.007 (2012).
Khajavi, D. & Khanmohammadi, R. Prediction of depression syndrome in elderly people based on physical activity and demographic characteristics: The role of age and gender. Growth Learn. Motor Exerc. 7(1), 87–103 (2015).
Coelho, R., Silva, C., Maia, A., Prata, J. & Barros, H. Bone mineral density and depression: A community study in women. J. Psychosom. Res. 46(1), 29–35 (1999).
Qadir, F., Jamshidi Oruk, R., Najaf Yarandi, A., Mukharshahi, Sh. B. & Aflaki, E. Inspired investigating the relationship between water drainage and bone density in menopausal women. Iran. J. Nurs. 18, 41–45 (2005).
Byeon, H. Association among smoking, depression, and anxiety: Findings from a representative sample of Korean adolescents. PeerJ 3, e1.288 (2015).
Wagena, E. J. et al. Risk of depression and anxiety in employees with chronic bronchitis: The modifying effect of cigarette smoking. Psychosom. Med. 66(5), 729–734 (2004).
Acknowledgements
The researchers would like to appreciate the staff of Bone Densitometry Center and all the patients who participated in this study.
Author information
Authors and Affiliations
Contributions
S.S.K., Gh.A., J.H., H.M. and A.K.H.J. assisted in conceptualization and design of the study, oversaw data collection, conducted data analysis and drafted the manuscript. S.S.K. and Gh.A. conceptualized and designed the study, assisted in data analysis and reviewed the manuscript. S.S.K., Gh.A., J.H., H.M. and A.K.H.J. assisted in study conceptualization and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kashfi, S.S., Abdollahi, G., Hassanzadeh, J. et al. The relationship between osteoporosis and depression. Sci Rep 12, 11177 (2022). https://doi.org/10.1038/s41598-022-15248-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-15248-w
- Springer Nature Limited