
Abstract
The ongoing SARS-CoV-2 pandemic is characterized by poor outcome and a high mortality especially in the older patient cohort. Up to this point there is a lack of data characterising COVID-19 patients in Germany admitted to intensive care (ICU) vs. non-ICU patients. German Reimbursement inpatient data covering the period in Germany from January 1st, 2020 to December 31th, 2021 were analyzed. 561,379 patients were hospitalized with COVID-19. 24.54% (n = 137,750) were admitted to ICU. Overall hospital mortality was 16.69% (n = 93,668) and 33.36% (n = 45,947) in the ICU group. 28.66% (n = 160,881) of all patients suffer from Cardiac arrhythmia and 17.98% (n = 100,926) developed renal failure. Obesity showed an odds-ratio ranging from 0.83 (0.79–0.87) for WHO grade I to 1.13 (1.08–1.19) for grade III. Mortality-rates peaked in April 2020 and January 2021 being 21.23% (n = 4539) and 22.99% (n = 15,724). A third peak was observed November and December 2021 (16.82%, n = 7173 and 16.54%, n = 9416). Hospitalized COVID-19 patient mortality in Germany is lower than previously shown in other studies. 24.54% of all patients had to be treated in the ICU with a mortality rate of 33.36%. Congestive heart failure was associated with a higher risk of death whereas low grade obesity might have a protective effect on patient survival. High admission numbers are accompanied by a higher mortality rate.
Similar content being viewed by others


Introduction
The ongoing COVID-19 pandemic is affecting people worldwide since the first reported case. Up to the end of October, more than 246 million cases and up to 5 million deaths have been reported1,2. The number of unreported cases is probably much higher. This makes the COVID-19 pandemic one of the deadliest in history.
Infection with the SARS-CoV-2 virus presents with a wide variety of symptoms—From none to life threatening. This complicates the detection and containment of the virus. With the worldwide spread of the SARS-CoV-2 virus, a burden has been placed on the health care systems worldwide. Especially the intensive care units (ICU) as a limited resource were occupied with the care of COVID-19 patients. In some countries, the ICU capacities reached their limits3,4, resulting in catastrophic outcomes for the patients. Over the pandemic, admission rates to ICU and mortality rate varied strongly. In the early phase of the pandemic, first reports and characterisations based on smaller populations mainly in China suggested only mild symptoms in 80% of the cases5,6,7,8. 20% needed hospital treatment and 20% of the hospitalized patients required ICU treatment6,7,9. Those numbers vary within the European Union10. Estimates suggest that between 10 and 20% of SARS-CoV-2 patients become so severely ill, that hospital treatment is required. In addition, the proportion of infected people who require intensive care also varies between 5 and 32%10,11.
Therefore, it is important to be able to adequately calculate the resources of the health care system to avoid a collapse of the system in the event of another wave. The present study therefore provides up-to-date data based on which calculations could be made. The aim of this observational study is to describe the dynamic of the pandemic in Germany and identify the underlying characteristics of hospitalized patients from January 2020 until the end of December 2021, based on data from the German Institute for Hospital Remuneration System (InEK).
Materials and methods
Inclusion criteria
All hospitalized patients in Germany with proven SARS-CoV-2 infection between January 1st, 2020 and December 31th, 2021 were included.
Definitions and data acquisition
We divided patients into subgroups in dependence of admission to the ICU or to the general ward (non-ICU) and distinguished in both subgroups between survivors and non-survivors. The collected data included age, comorbidities (congestive heart failure, arterial hypertension, chronic pulmonary disease, diabetes and obesity), complications (acute renal failure, dialysis, cardiac arrhythmias, cardiopulmonary resuscitation (CPR), embolism, thrombosis, myocardial infarction, pulmonary embolism, intracranial hemorrhage and stroke), length of hospital stay and mortality. Due to our findings associated with obesity, we used and subdivided obesity according to the WHO-definition into grade I, II and III. Diagnoses were coded according to the tenth revision of the International Classification of Diseases (ICD) and procedures were coded according to the International Classification of Procedures in Medicine in the version of 2020 (Table 1). The InEK only allows anonymized queries; there is no possibility to track a case back to a patient and therefore no further analysis is possible at the individual case level. In this study, we included only patients with a confirmed SARS-CoV-2 infection by Real-Time-(RT)-PCR (ICD U07.1) and admitted to hospital between January 1st, 2020 and December 31th, 2021.
Existing comorbidities (e.g. arterial hypertension, ICD I10.x, I11.x–I13.x, I15.x) and complications were defined by their respective ICD codes (Table 1).
Statistical analysis
The data were descriptively analyzed. Categorical variables are expressed as absolute numbers and percentages. Due to the lack of median and quartiles in the data source, continuous variables were calculated using mean and standard deviation (SD). Due to the aggregated data, only group comparisons of categorical variables were possible. The OR were calculated by means of 2 × 2 frequency tables. For this purpose, the Pearson Chi square test with an assumed significance level of 0.05 was utilized and the OR was determined with the 95% confidence interval (CI). Excel 2019 (Microsoft Corp., Seattle, WA, USA) and Python with SciPy and the statsmodels (sm) package were used for the analyses.
Ethics approval and consent to participate
Due to the institutional anonymization, no conclusions can be drawn about individual patients. According to §21KHEntgG the reimbursement data is free for scientific use. The Ethics Committee of the University Hospital Frankfurt waived the need for an Ethical Committee approval for this study (Chair: Prof. Dr. Harder, Ref: 2022-766). All data processing was performed in accordance with the Declaration of Helsinki.
Consent for publication
As this are anonymised register data, no consensus of the patients can be collected.
Results
A total of 561,379 patients were hospitalized with a confirmed SARS-CoV-2 infection in Germany from January 1st, 2020 to December 31th, 2021 and analyzed in this study.
Patients’ characteristics
The proportion of female hospitalized patients was 47.65% (n = 267,516) overall. In total, 75.46% (n = 423,611) non-ICU and 24.54% (n = 137,750) ICU patients (Table 2). The biggest group was aged 80 years or older, being 30.07% (n = 168,779) overall. Divided in groups ICU and non-ICU and subgroups survivors and non-survivors: Patients aged 80 years or older had the highest conditional (relative) frequencies in non-ICU overall (32.17% (n = 136,270)), non-ICU-survivors (26.72% (n = 100,430)), non-ICU-non-survivors (75.10% (n = 35,840)), ICU overall (32.17% (n = 136,270)) and ICU-non- survivors (37.04% (n = 17,020)). The biggest age group in ICU-survivors was 65–74 years (22.63% (n = 20,772).
Length of in-hospital stay (LOS) comorbidities, complications and mortality rate
In all patients the LOS was 11.2 (SD = 12.2) days in 2020 and 11.7 (SD = 12.4) days in 2021. The most common comorbidity in all hospitalized patients was arterial hypertension (51.94% n = 291,577), followed by congestive heart failure (24.32% n = 136,505). In the non-ICU-group arterial hypertension was the most common comorbidity in survivors (47.82% (n = 179,738)) and non-survivors (61.79% (n = 29,489)), followed by congestive heart failure (17.25% (n = 179,738) in survivors and 61.79% (n = 29,489) in non-survivors, respectively. All other comorbidities and their frequencies in subgroups are displayed in Table 3.
The most common complication was cardiac arrhythmia overall, coded in 28.66% (n = 160,881) of the patients overall and in every subgroup, as well. Especially in non-survivor group in ICU patients 58.04% (n = 26,667) and non-ICU patients 45.99% (n = 21,946), respectively. In each non-survivor group the rates were significantly higher, compared to the survivor group (Table 3).
Overall, 17.98% (n = 100,926) patients developed renal failure. The highest conditional (relative) frequency of patients needing dialysis was seen in non-survivors non-ICU-patients being 35.46% (n = 16,920). Cardiopulmonary resuscitation (CPR) was performed in 1.73% (n = 9728) of all COVID-19 inpatients. In non-survivor ICU-patients 14.23% (n = 6536) were treated with CPR. Pulmonary embolism occurred in 2.27% (n = 12,730) of all patients.
Our data shows an overall mortality rate of 16.69% (n = 93,668), 11.27% (n = 47,721) in non-ICU patients, and 33.36% (n = 45,947) in ICU-patients, respectively.
Comparison survivors vs. non-survivors
The highest OR for comorbidity was seen in congestive heart failure (Overall: OR: 3.81 (3.78–3.89) non-ICU: OR: 4.23 (4.15–4.31) ICU: OR: 2.42 (2.37–2.48)). Obesity WHO grade I and II were the only comorbidities in which an OR < 1 was seen. In particular in obesity WHO grade I (Overall: OR: 0.83 (0.79–0.87), non-ICU: OR: 0.55 (0.50–0.60), ICU: OR: 0.77 (0.72–0.82)) (Table 3).
There is a significant difference between the groups of non-survivor/survivor within all complications (p < 0.001). The highest OR for the non-survivor groups were seen in CPR (Overall: OR: 20.83 (19.82–21.89) non-ICU: OR: 85.36 (70.31–103.64) ICU: OR: 7.86 (7.46–8.29)). Followed by renal replacement therapy in patients overall (OR: 7.26 (7.09–7.43)), renal failure in non-ICU patients (OR: 3.09 (3.03–3.15)) and embolism or thrombosis in non-ICU patients (OR: 2.75 (2.32–3.25)). (Table 3).
Analysis in the context of time course
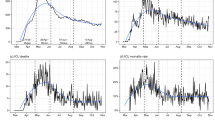
The observed in-hospital mortality-rates fluctuated during the analyzed and showed three peaks: April 2020 and January 2021 being 21.23% (n = 4539) and 22.99% (n = 15,724) and in November, December 2021 (16.82%, n = 7173 and 16.54%, n = 9416) (Fig. 1, Table 4).

Mortality, vaccination and corona cases over time in Germany. Mortality of in hospital patients compared to COVID-19 vaccination and number of COVID-19 cases in Germany over time. Corona cases in Germany [n]. Fraction of mortality for \(\ge\) 60 years [%]. Vaccinated percentage of age group \(\ge\) 60 years [%] and total mortality [%] over time.
Within the whole-time patients aged 60 years or older had the highest mortality in all hospitalized patients. Analyzed by the time trend of the data divided into months from January 2021 until the end of December 2021, in every month the highest mortality was observed in the age group 80–85 years, with particularly high mortality in months when hospitalization rates were the highest (Fig. 1, Table 4).
Discussion
This retrospective study includes a cohort of 561,379 hospitalized patients from January 1st, 2020 to December 31th, 2021 with a positive SARS-CoV-2 PCR test. Our main findings are a mortality rate of 16.69% overall. Between months of the ongoing pandemic, the mortality fluctuates. Especially in the “third wave”, a noticeable decrease in the proportion of elderly patients was seen.
The COVID-19 pandemic in Germany in the analyzed period can be described in four waves: the first one from March until May 202012, the second one from October 2020 until January 202112 and a third wave from March until April 202113. In the end of 2021 Germany went through the fourth wave. The cause of the undulating course of infection numbers is multifactorial, main reasons are higher temperatures in spring/summer14, social distancing and shutdown measures by the government13.
Mortality rate
The mortality rate of 16.69% overall is lower than previously described mortality-rates. Richardson et al. described 5700 hospitalized patients diagnosed with COVID-19 in New York from March until April 2020 and found a mortality rate of 21%, overall but a particularly lower rate of ICU-patients (12.2%)15. Karagiannidis et al. described over 10,000 patients suffering from COVID-19 in Germany from February until April 2020 in Germany and found a mortality rate of 22% overall16. This might be explained by the fact that previous studies describe a shorter time period. In December of 2020 the vaccine against COVID-19 was licensed in Germany17. Over time, more and more treatment options are being explored, and guidelines for the treatment of COVID-19 infection continue to evolve on a regular basis.
Due to prioritization rules the vaccines were only available for patients over 75 years of age, employees in high-risk facilities and patients with defined comorbidities were vaccicinated17. The prioritization was lifted in May 2021. The first “vaccination effect” may occur in January 2021, which could explain the decreasing proportion of patients aged 60 years or older from there on.
In contrast to that we found higher mortality rates in ICU patients, being 33.36%. A possible explanation might the higher capacity of ICU-beds in germany16 and therefore the possibility to admit patients with more comorbidities or at higher age to the ICU, while in some countries ICUs reached their capacity limit3.
Our data shows a distinct mortality between minors (< 18 years) and old adults (> 60 years).
Compared to the German population (17%, in 2020) and the share of SARS-CoV-2 infected persons (29%), the group of children (< 18 years) is significantly underrepresented among all hospitalised patients (2.35%, Table 2)18,19. Furthermore, 9% (< 18 years) against 26% (> 60 years) conditional on the respective group were admitted to ICU. There a various explanation for this finding. Children have less comorbidities such as obesity, diabetes, cancer and other chronic diseases. Children and adults show a different immune response to a viral infection, protecting children from severe COVID-1920. Our findings can also be explained with a difference in the expression of ACE2-receptor, the primary receptor of SARS-CoV-221. Children express lower levels of ACE221 and therefore have fewer symptoms and a better prognosis22.
Comorbidities
Arterial hypertension was the most common comorbidity in our study (51.94% (n = 291,577) overall), this result is in line with other studies describing hypertension as the most common comorbidity with rates of 42%23 up to 56%16.
Obesity is known to be a risk factor for COVID-1924 and is associated with higher mortality11. The incidence of 6.52% for obesity is lower than rates described in the UK (10.2%)11 or France (47.6%)25. Surprisingly our data showed a reduced odd for death in patients with low grade obesity, especially WHO grade I (non-ICU: 0.55 (0.50–0.60) and ICU: 0.77 (0.72–0.82), respectively). Dana et al. found a lower risk of death for critically ill COVID-19 patients among patients with moderate obesity26. This finding is not in line with other studies27. However, the Centers for Disease Control and Prevention (CDC) states that patients at the “threshold” between healthy weight and overweight are at lower risk for hospitalization, ICU admission, and death while the risk for mechanically ventilation raised continuously with rising body mass index (BMI)28. Our findings support the statement of the CDC. Patients with a low grade overweight (WHO grade I) have a higher chance of survival (With increasing obesity, the effect is lost and the overweight becomes a risk factor for the patient (WHO grade III, OR: 1.13 (1.08–1.19)). However, overweight and moderate obesity are known to have a protective effect on hospitalized non-COVID-19 ICU-Patients29. This effect is not yet fully understood and often controversially referred to as “obesity paradox”30. With a lower rate of high grade obese patients admitted to the hospital, more patients are at the “threshold” described by the CDC. Foo et al. described for every 1% increase in obesity prevalence, the COVID-19 mortality rate was increased by 8.3%31. This might explain our finding.
We could find a significant difference in the frequency of patients suffering from congestive heart failure between survivors and non-survivors, with a bigger frequency of heart failure in non-survivors. One possible explanation is that patients suffering from heart failure have a higher overall frailty and are at higher risk for acute cardiac injury. Several studies investigated cardiovascular manifestations and mechanisms in patients suffering from COVID-19 and showed a high prevalence of cardiovascular comorbidities32 and a higher risk for mortality in patients suffering from cardiovascular comorbidities or cardiac injury32,33. Jabri et al. described a significant increase in stress cardiomyopathy during the pandemic34, furthermore a frequent occurrence of cor pulmonale in COVID-19 patients has been described35. All this factors explain the high proportion of cardiac comorbidities in hospitalized patients and the increase of those diagnoses in the non-survivor groups.
Complications
We found arrhythmias to be the most common complication in our study. We showed a rate of 42.74% (n = 58,870) for ICU patients. This result is comparable to a study by Duo et al. who described a rate of 44.4% among ICU patients in a study investigating 138 patients overall32.
Electrocardiographic abnormalities are often described in patients suffering from COVID-1936,37.
One underlying reason may be the mismatch between oxygen supply and oxygen demand resulting in cardiac injury. Therefore, the high OR for death is not surprising.
Thrombotic events are often seen in COVID-19 patients. Those events are associated with a more severe disease and increased mortality38,39. The molecular explanation range from COVID-19-associated coagulopathy to genetic predisposition and is still subject to research40,41. Our findings are in line with literature, we showed a pulmonary embolism rate of 2.27% (n = 12,730) for all hospitalized COVID-19 patient. Patients suffering from pulmonary embolism have a higher chance of dying (OR: 2.14 (2.05–2.22)). OR on ICU is lower (OR: 1.35 (1.28–1.41). One explanation for this could be that more radiological examinations are performed on ICU and therefore associated with a higher number of incidental findings without clinical relevance42. A second explanation is that patients on ICU are more likely to be sufficiently anticoagulated, as recommended in guidelines43,44. Unfortunately, medication application such as anticoagulation is not provided in the reimbursement data.
Renal failure is a common complication in patients suffering from COVID-1915,45. The observed rate of patients with acute kidney failure (17.98% n = 100,926) is in line with other studies, describing rates between 20 and 40%15,45. The higher proportion of patients with renal replacement therapy (RRT) in the ICU-group might be explained by the fact that needing dialysis is a common reason to be admitted to the ICU. Patients who had been diagnosed with acute kidney failure and a following admission to the ICU are displayed in the ICU-group only. In our study 5.67% (n = 31,847) patients needed RRT, this result seems to be higher than in other studies, for example Richardson et al. described a rate of 3.2%.
COVID-19 patients are more likely to suffer from in-hospital-cadiac-arrest (IHCA)46. In our study 1.73% (n = 9728) of all patients received CPR. The OR of dying was remarkably higher on the normal ward compared to the ICU. This is in accordance to the literature. Acharya et al. described a IHCA for non-ICU patients in 2.2% (in our study: 2.48%) and for ICU patients in 15.4% (in our study 14.2%)47. A possible cause for the high difference between non-ICU and ICU patients might be the longer timespan between the circulatory arrest and the actual start of CPR due to the lack of monitoring48.
This study is the first in Germany to describe the course of the pandemic from the beginning to the end of December 2021, covering 561 379 hospitalized COVID-19 Patients.
Further studies should be conducted to identify risk factors for an adverse course of the disease. On one hand, this could help to identify patients with a special risk profile at an early stage (for example Simonnet et al. investigated obesity as a risk factor25) or, on the other hand, serve as criteria in possible triaging.
Conclusion
The overall mortality rate of 16.69% in COVID-19 patients in Germany is lower than previously shown in other studies. 24.54% of all patients had to be treated on the ICU with a mortality rate of 33.36%, which was high in comparison to the literature. Congestive heart failure was associated with a significantly higher risk of death. In non-ICU patients suffering from congestive heart failure the OR was especially high, being 4.23 (4.15–4.31). The most common comorbidity in all COVID-19 patients was arterial hypertension. The most common complication were arrhythmias, which were diagnosed significantly more often in non-survivors (p < 0.001). In COVID-19 patients CPR is associated with a high chance of death, especially on normal wards (OR: 85.36 (70.31–103.64)). With an OR: 0.83 (0.79–0.87) WHO grade I obesity might have a protective effect of the patient’s survival.
Pre-existing cardiac conditions appear to carry a particularly high risk in patients suffering from COVID-19.
Due to the limited data, no further research could be done, so it is extremely important to make this data available to the scientific community in order to gain a wider insight and better understand possible causal relationships.
Limitations
Due to the provision of data by the InEK during the year, only highly aggregated data are available and no further detailed queries are possible. Patients’ age is only available in the provided subgroups, so no further analysis like mean or median age can be made. As the data (e.g. comorbidities) were anonymized and cannot be tracked back to a single patient further analysis such as linear regression are not possible. Laboratory findings or medication are not coded for reimbursement and are therefore not available for analysis.
Data availability
The German Institute for Hospital Remuneration System (InEK) supports hospitals and health insurance funds as well as their associations in the introduction and continuous further development of the German-DRG system in accordance with the Krankenhausfinanzierungsgesetz (KHG; Hospital Financing Act). Since 2020, access to these data has been possible during the year. For this observational study, we used publicly accessible performance data provided by InEK. Since the register data were anonymized, the Ethics Committee of the University Hospital Frankfurt waived the need for an Ethical approval (Chair: Prof. Dr. Harder, Ref: 2022-766).
Abbreviations
- CDC:
-
Centers for Disease Control and Prevention
- CI:
-
Confidence interval
- COVID-19:
-
Coronavirus disease 2019
- CPR:
-
Cardiopulmonary resuscitation
- DRG:
-
Diagnosis-related group
- ICD:
-
International classification of diseases
- ICU:
-
Intensive care unit
- IHCA:
-
In-hospital-cardiac-arrest
- InEK:
-
German Institute for Hospital Remuneration System
- KHG:
-
Krankenhausfinanzierungsgesetz (Hospital Financing Act)
- LOS:
-
Length of in-hospital stay
- Non-ICU:
-
Non-intensive care unit (= general ward)
- OPS:
-
Operation and procedure code
- RT-PCR:
-
Real-time-polymerase chain reaction
References
COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University (JHU). https://gisanddata.maps.arcgis.com/apps/dashboards/bda7594740fd40299423467b48e9ecf6. Accessed 25 May 2022.
Dong, E., Du, H. & Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet. Infect. Dis 20, 533–534. https://doi.org/10.1016/S1473-3099(20)30120-1 (2020).
Immovilli, P. et al. COVID-19 mortality and ICU admission: The Italian experience. Crit. Care 24, 228. https://doi.org/10.1186/s13054-020-02957-9 (2020).
Remuzzi, A. & Remuzzi, G. COVID-19 and Italy: What next? Lancet 395, 1225–1228. https://doi.org/10.1016/s0140-6736(20)30627-9 (2020).
Wu, Z. & McGoogan, J. M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72314 cases from the Chinese Center for Disease Control and Prevention. JAMA 323, 1239–1242. https://doi.org/10.1001/jama.2020.2648 (2020).
Guan, W. J. et al. Clinical characteristics of coronavirus disease 2019 in China. N. Engl. J. Med. 382, 1708–1720. https://doi.org/10.1056/NEJMoa2002032 (2020).
Huang, C. et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395, 497–506. https://doi.org/10.1016/S0140-6736(20)30183-5 (2020).
Du, R. H. et al. Hospitalization and critical care of 109 decedents with COVID-19 pneumonia in Wuhan, China. Ann. Am. Thorac. Soc. 17, 839–846. https://doi.org/10.1513/AnnalsATS.202003-225OC (2020).
Wu, Z. & McGoogan, J. M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 323, 1239–1242. https://doi.org/10.1001/jama.2020.2648 (2020).
European Centre for Disease Prevention and Control, A. a. o. t. E. U. Data on Hospital and ICU Admission Rates and Current Occupancy for COVID-19 https://www.ecdc.europa.eu/en/publications-data/download-data-hospital-and-icu-admission-rates-and-current-occupancy-covid-19. Accessed 3 May 2022.
Docherty, A. B. et al. Features of 20 133 UK patients in hospital with covid-19 using the ISARIC WHO clinical characterisation protocol: Prospective observational cohort study. BMJ 369, m1985. https://doi.org/10.1136/bmj.m1985 (2020).
Schilling, J. et al. Die verschiedenen Phasen der COVID-19-Pandemie in Deutschland: Eine deskriptive analyse von Januar 2020 bis Februar 2021. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 64, 1093–1106. https://doi.org/10.1007/s00103-021-03394-x (2021).
Schuppert, A., Polotzek, K., Karschau, J. & Karagiannidis, C. Effectiveness of extended shutdown measures during the ‘Bundesnotbremse’ introduced in the third SARS-CoV-2 wave in Germany. Infection 49, 1331–1335. https://doi.org/10.1007/s15010-021-01713-7 (2021).
Fan, G. et al. Decreased case fatality rate of COVID-19 in the second wave: A study in 53 countries or regions. Transbound. Emerg. Dis. 68, 213–215. https://doi.org/10.1111/tbed.13819 (2021).
Richardson, S. et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York city area. JAMA 323, 2052–2059. https://doi.org/10.1001/jama.2020.6775 (2020).
Karagiannidis, C. et al. Case characteristics, resource use, and outcomes of 10 021 patients with COVID-19 admitted to 920 German hospitals: An observational study. Lancet Respir. Med. 8, 853–862. https://doi.org/10.1016/S2213-2600(20)30316-7 (2020).
Vygen-Bonnet, S. et al. Beschluss und Wissenschaftliche Begründung der Ständigen Impfkommission (STIKO) für die COVID-19-Impfempfehlung, 3–63. https://doi.org/10.25646/7755.2 (2020).
Robert-Koch-Institut. COVID-19-Fälle nach Altersgruppe und Meldewoche https://www.rki.de/DE/Content/InfAZ/N/Neuartiges_Coronavirus/Daten/Altersverteilung.html (2022). Accessed 24 May 2022.
Bundesamt, S. (2022).
Yoshida, M. et al. Local and systemic responses to SARS-CoV-2 infection in children and adults. Nature 602, 321–327. https://doi.org/10.1038/s41586-021-04345-x (2022).
Vaduganathan, M. et al. Renin-angiotensin-aldosterone system inhibitors in patients with Covid-19. N. Engl. J. Med. 382, 1653–1659. https://doi.org/10.1056/NEJMsr2005760 (2020).
Ludvigsson, J. F. Systematic review of COVID-19 in children shows milder cases and a better prognosis than adults. Acta Paediatr. 109, 1088–1095. https://doi.org/10.1111/apa.15270 (2020).
Grasselli, G. et al. Risk factors associated with mortality among patients with COVID-19 in intensive care units in Lombardy, Italy. JAMA Intern. Med. 180, 1345–1355. https://doi.org/10.1001/jamainternmed.2020.3539 (2020).
Kwok, S. et al. Obesity: A critical risk factor in the COVID-19 pandemic. Clin. Obes. 10, e12403. https://doi.org/10.1111/cob.12403 (2020).
Simonnet, A. et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity (Silver Spring) 28, 1195–1199. https://doi.org/10.1002/oby.22831 (2020).
Dana, R. et al. Obesity and mortality in critically ill COVID-19 patients with respiratory failure. Int. J. Obes. 45, 2028–2037. https://doi.org/10.1038/s41366-021-00872-9 (2021).
Poly, T. N. et al. Obesity and mortality among patients diagnosed with COVID-19: A systematic review and meta-analysis. Front. Med. https://doi.org/10.3389/fmed.2021.620044 (2021).
Kompaniyets, L. et al. Body mass index and risk for COVID-19-related hospitalization, intensive care unit admission, invasive mechanical ventilation, and death-United States, March-December 2020. Morb. Mortal Wkly. Rep. 70, 355–361. https://doi.org/10.15585/mmwr.mm7010e4 (2021).
Schetz, M. et al. Obesity in the critically ill: A narrative review. Intens. Care Med 45, 757–769. https://doi.org/10.1007/s00134-019-05594-1 (2019).
Donini, L. M., Pinto, A., Giusti, A. M., Lenzi, A. & Poggiogalle, E. Obesity or BMI paradox? Beneath the tip of the Iceberg. Front. Nutr. 7, 53. https://doi.org/10.3389/fnut.2020.00053 (2020).
Foo, O., Hiu, S., Teare, D., Syed, A. A. & Razvi, S. A global country-level analysis of the relationship between obesity and COVID-19 cases and mortality. Diabetes Obes. Metab. 23, 2697–2706. https://doi.org/10.1111/dom.14523 (2021).
Dou, Q., Wei, X., Zhou, K., Yang, S. & Jia, P. Cardiovascular manifestations and mechanisms in patients with COVID-19. Trends Endocrinol. Metab. 31, 893–904. https://doi.org/10.1016/j.tem.2020.10.001 (2020).
Shi, S. et al. Association of cardiac injury with mortality in hospitalized patients with COVID-19 in Wuhan, China. JAMA Cardiol. 5, 802–810. https://doi.org/10.1001/jamacardio.2020.0950 (2020).
Jabri, A. et al. Incidence of stress cardiomyopathy during the coronavirus disease 2019 pandemic. JAMA Netw. Open 3, e2014780. https://doi.org/10.1001/jamanetworkopen.2020.14780 (2020).
Creel-Bulos, C. et al. Acute cor pulmonale in critically ill patients with covid-19. N. Engl. J. Med. 382, e70. https://doi.org/10.1056/NEJMc2010459 (2020).
He, J. et al. Characteristic electrocardiographic manifestations in patients with COVID-19. Can. J. Cardiol. 36(966), e961–e966. https://doi.org/10.1016/j.cjca.2020.03.028 (2020).
Angeli, F. et al. Electrocardiographic features of patients with COVID-19 pneumonia. Eur. J. Intern. Med. 78, 101–106. https://doi.org/10.1016/j.ejim.2020.06.015 (2020).
Klok, F. A. et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 191, 145–147. https://doi.org/10.1016/j.thromres.2020.04.013 (2020).
Middeldorp, S. et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 18, 1995–2002. https://doi.org/10.1111/jth.14888 (2020).
Loo, J., Spittle, D. A. & Newnham, M. COVID-19, immunothrombosis and venous thromboembolism: Biological mechanisms. Thorax 76, 412–420. https://doi.org/10.1136/thoraxjnl-2020-216243 (2021).
Polak, S. B., Van Gool, I. C., Cohen, D., von der Thusen, J. H. & van Paassen, J. A systematic review of pathological findings in COVID-19: A pathophysiological timeline and possible mechanisms of disease progression. Mod. Pathol. 33, 2128–2138. https://doi.org/10.1038/s41379-020-0603-3 (2020).
Lumbreras, B., Donat, L. & Hernandez-Aguado, I. Incidental findings in imaging diagnostic tests: A systematic review. Br. J. Radiol. 83, 276–289. https://doi.org/10.1259/bjr/98067945 (2010).
Kluge, S. et al. German recommendations for treatment of critically ill patients with COVID-19-version 3: S1-guideline. Anaesthesist 69, 653–664. https://doi.org/10.1007/s00101-020-00833-3 (2020).
Kluge, S. et al. Clinical practice guideline: Recommendations on the In-hospital treatment of patients with COVID-19. Dtsch. Arztebl. Int. 118, 865–871. https://doi.org/10.3238/arztebl.m2021.0374 (2021).
Ronco, C., Reis, T. & Husain-Syed, F. Management of acute kidney injury in patients with COVID-19. Lancet Respir. Med. 8, 738–742. https://doi.org/10.1016/s2213-2600(20)30229-0 (2020).
Ippolito, M. et al. Mortality after in-hospital cardiac arrest in patients with COVID-19: A systematic review and meta-analysis. Resuscitation 164, 122–129. https://doi.org/10.1016/j.resuscitation.2021.04.025 (2021).
Acharya, P. et al. Incidence, predictors, and outcomes of in-hospital cardiac arrest in COVID-19 patients admitted to intensive and non-intensive care units: Insights from the AHA COVID-19 CVD registry. J. Am. Heart Assoc. 10, e021204. https://doi.org/10.1161/JAHA.120.021204 (2021).
Perman, S. M. et al. Location of in-hospital cardiac arrest in the United States—Variability in event rate and outcomes. J. Am. Heart Assoc. 5, e003638. https://doi.org/10.1161/JAHA.116.003638 (2016).
Funding
Open Access funding enabled and organized by Projekt DEAL. This study was supported by internal institutional research funds from the Department of Anaesthesiology, Intensive Care and Pain Therapy, University Hospital Frankfurt, Goethe University, Frankfurt Germany.
Author information
Authors and Affiliations
Contributions
L.V.B. and J.K. wrote the manuscript and were in charge of planning the study in close consultation with B.F. and K.Z. B.F. conceived the study and was in charge of overall direction and planning. Statistical analysis and proofreading was done by O.O. All authors contributed to the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kloka, J.A., Blum, L.V., Old, O. et al. Characteristics and mortality of 561,379 hospitalized COVID-19 patients in Germany until December 2021 based on real-life data. Sci Rep 12, 11116 (2022). https://doi.org/10.1038/s41598-022-15287-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-15287-3
- Springer Nature Limited
This article is cited by
-
Mechanical ventilation as a major driver of COVID-19 hospitalization costs: a costing study in a German setting
Health Economics Review (2024)
-
Lessons Learned from Model-based Economic Evaluations of COVID-19 Drug Treatments Under Pandemic Circumstances: Results from a Systematic Review
PharmacoEconomics (2024)
-
Cellular and molecular features of COVID-19 associated ARDS: therapeutic relevance
Journal of Inflammation (2023)
-
High-dose methylprednisolone pulse therapy during refractory COVID-19 acute respiratory distress syndrome: a retrospective observational study
BMC Pulmonary Medicine (2023)
-
COVID-19 associated bacterial infections in intensive care unit: a case control study
Scientific Reports (2023)