
Abstract
The effects of forced vital capacity (FVC) on clinical outcomes of asthma-chronic obstructive pulmonary diseases overlap (ACO) are still unknown. We conducted this study to examine the association of FVC on clinical outcomes in ACO. Data from the Korean COPD Subgroup Study cohort were analyzed. Patients who fulfilled the ACO criteria were included and grouped according to FVC changes, such as FVC-incline and FVC-decline. No significant differences were observed between the FVC-incline and FVC-decline groups in baseline clinical characteristics. In a year after, FVC-decline group experienced more moderate (47.1% vs. 36.8%, p = 0.02) and moderate-to-severe (49.8% vs. 39.6%, p = 0.03) acute exacerbations (AEs), compared to FVC-incline group. The frequency of moderate AEs (1.3 ± 2.1 vs. 0.9 ± 1.7, p = 0.03) and moderate-to-severe AEs (1.5 ± 2.5 vs. 1.1 ± 1.9, p = 0.04) were higher in the FVC-decline group than in the FVC-incline groups. After adjusting for confounding factors, FVC-decline group was associated with moderate AEs (odds ratio [OR] = 1.58; 95% confidence interval [CI] 1.02–2.44; p = 0.04), and moderate-to-severe AEs (OR = 1.56; 95% CI 1.01–2.41; p < 0.05) in ACO patients, which was not seen in FEV1 changes. FVC changes are associated with clinical outcomes in ACO.
Similar content being viewed by others


Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are chronic inflammatory airway diseases that are common and burdensome worldwide1,2,3. Features of asthma and COPD can co-exist in the same patient, which is called asthma-COPD overlap (ACO)4,5,6. Asthmatic features in ACO patients include high blood eosinophil and immunoglobulin E levels, a large post-bronchodilator (BD) response, and a history of asthma, atopy, or allergic rhinitis. COPD features in ACO are associated with exposure to smoking or air pollution, typically has a late onset, and is characterized by a post-BD forced expiratory flow rate in 1 s/forced vital capacity (FEV1/FVC) ratio < 0.707. ACO is present in approximately 2.0% of the population worldwide and is associated with a very large healthcare burden8,9.
Lung function tests are physiologic markers of chronic airway disease, and traditional marker of COPD is FEV110. As in COPD, annual FEV1 decline of ACO is more rapid than that of healthy adults11,12,13. When it compares to that of COPD or asthma, controversial results were found in lung function of ACO14,15. Moreover, their impact on clinical outcomes of ACO is controversial16.
There are not enough studies on which lung function indicators, such as FEV1 or FVC, are better for explanation of clinical outcomes in ACO. Interestingly, ACO patients showed significant difference in change of FVC, not that of FEV117. In that study, they showed larger variation of FVC than that of FEV117. They also showed different tendency of FVC changes compared to those of COPD13. FVC is an undervalued marker of lung function until these days. We hypothesized that FVC, not FEV1, is associated with clinical outcomes of ACO. We conducted this study to compare FVC and FEV1 to predict the clinical outcomes of ACO, such as symptom scores, exercise capacity, and annual frequency and severity of exacerbations.
Results
Demographics according to FVC change
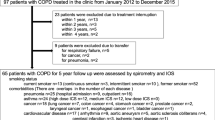
The ACO criteria were fulfilled with 532 patients in the KOCOSS, of whom 298 were included in the FVC-decline group (Fig. 1). Age, sex, body mass index (BMI), or smoking status showed no statistical differences between the FVC-decline and FVC-incline groups. The proportion of patients with gastroesophageal reflux disease (GERD) was higher in the FVC-incline compared to FVC-decline group (21.4% vs. 14.1%, p = 0.03). However, the other comorbidities were not different between the groups. Baseline mean post-BD FVC values were higher in the FVC-decline group compared to the FVC-incline group (3.29 ± 0.76 vs. 2.99 ± 0.75 L, p < 0.01). The mean post-BD FEV1 values were not significantly different between the two groups. The annual change in FVC of the FVC-decline group was − 0.33 ± 0.29 L/year and that of the FVC-incline group was 0.26 ± 0.27 L/year. The annual change in FEV1 of the FVC-decline group was − 0.12 ± 0.21 L/year and that of the FVC-incline group was 0.16 ± 0.27 L/year. There was no statistical difference in medication use. Baseline St. George’s Respiratory Questionnaire-C (SGRQ-C) total scores were not significantly different between the groups. 6-min walk distance (6MWD) was lower in FVC-decline group than in FVC-incline group (378.5 m [320.0 {1st quartile}; 442.0 {3rd quartile}] vs. 401.5 m [328.0; 474.5], p < 0.05]. The history of past exacerbation within 1 year of study enrollment was not different between the groups (Table 1).

Flowchart of this study. Patients were extracted from KOCOSS study (n = 2147) who meet the COPD definition. If they satisfy the exclusion criteria or do not perform the pulmonary function tests 1 year after, they were excluded. Overall, 532 patients were finally enrolled in this study. They were divided into FVC-decline and FVC-incline group. Characteristics were compared between FVC-decline and FVC-incline. ACO asthma-COPD overlap, ATS American Thoracic Society, COPD chronic obstructive pulmonary disease, FEV1 forced expiratory volume in one second, FVC forced vital capacity.
Clinical outcomes of ACO in 1 year are varied by FVC change
The SGRQ-C scores and the occurrence and frequency of acute exacerbations (AEs) during the 1-year follow-up were compared between the groups. One year after, SGRQ-C total scores were higher in FVC-decline group than in FVC-incline group (35.5 [19.2; 50.7] vs. 26.1 [14.5; 47.4], p = 0.01). In subgroup analyses, SGRQ-C symptom scores did not show the statistical difference between the FVC-decline and FVC-incline group. On the other hand, the SGRQ-C activity score (45.4 [29.8; 67.8] vs. 37.6 [22.5; 59.7], p = 0.01) and the SGRQ-C impact score (21.9 [5.1; 40.1] vs. 14.2 [4.6; 35.0], p = 0.03) were higher in the FVC-decline group than in the FVC-incline group. Patients in the FVC-decline group, compared to those in the FVC-incline group, experienced more moderate COPD exacerbation (47.1% vs. 36.8%, p = 0.02) and moderate-to-severe COPD exacerbation (49.8% vs. 39.6%, p = 0.03). An analysis of the number of exacerbations showed similar results. Moderate COPD exacerbations in the FVC-decline group were more frequent compared to the FVC-incline group (1.3 ± 2.1 times/year vs. 0.9 ± 1.7 times/year, p = 0.03). The number of moderate-to-severe COPD exacerbations was higher in the FVC-decline group compared to the FVC-incline group (1.5 ± 2.5 times/year vs. 1.1 ± 1.9 times/year, p = 0.04). There was no statistical difference in 6MWD and 1-year mortality between the two groups (Table 2).
Comparison of SGRQ-C and acute exacerbations in 1 year after by ΔFVC quartile and ΔFEV1 quartile
FEV1-decline group also showed higher SGRQ-C total score, activity score, and impact scores than FEV1-incline group (Supplementary Table 1). Therefore, the association of ΔFVC (delta FVC: annual changes of the postbronchodilator values of FVC) quartile with SGRQ-C and that of ΔFEV1 quartile with SGRQ-C were evaluated for distinguishing better marker for SGRQ-C. Post-hoc analyses by Bonferroni method were performed between the groups. There was no statistical difference of baseline SGRQ-C by ΔFVC quartile (Fig. 2A) and ΔFEV1 quartile (Fig. 2C). It is also found in comparing the SGRQ-C in 1-year after by ΔFEV1 quartile (Fig. 2D). However, SGRQ-C (1 year) was improved as increasing order of ΔFVC quartile, especially in SGRQ-C total score, SGRQ-C activity score, and SGRQ-C impact scores (p < 0.05, each) (Fig. 2B). Therefore, FVC grouping explains respiratory related symptoms better than FEV1 grouping.

SGRQ-C in year after by ΔFVC quartile and ΔFEV1 quartile. For comparison, post-hoc analyses by Bonferroni method were performed between the groups, such as ΔFVC quartile and ΔFEV1 quartile. Baseline SGRQ-C by ΔFVC quartile (A) and ΔFEV1 quartile (C) did not show statistical difference between four groups in post-hoc analyses. Comparison of SGRQ-C (1 year) by ΔFVC quartile (B) showed a significant difference between the groups in post-hoc analyses. Especially, SGRQ-C activity and impact scores were different between the four groups and showed negative relationship according to the increase of ΔFVC quartile. On the other hand, SGRQ-C (1 year) by Δ FEV1 quartile (D) did not show the statistical difference between the groups. *p value < 0.05. Δ annual changes of the postbronchodilator values, FEV1 forced expiratory volume in one second, FVC forced vital capacity, SGRQ-C St. George’s Respiratory Questionnaire-Chronic obstructive pulmonary disease specific version.
Compared to those of FVC, the number and percentage of who experienced exacerbations were not different between the FEV1-decline and the FEV1-incline group (Supplementary Table 1). The scatter plots of ΔFVC and ΔFEV1 by annual frequency of COPD exacerbation (Supplementary Fig. 1) showed that trend lines and linear regression of ΔFVC correlated with annual AE frequency (p < 0.01), but ΔFEV1 did not (p = 0.77). In the comparing the association of both ΔFVC quartile and ΔFEV1 quartile with the percentage of AEs, they did not show statistically significant difference between the groups. However, ΔFVC quartile showed decreasing tendency in moderate COPD exacerbation and moderate-to-severe COPD exacerbation (Fig. 3).

The percentage of patients who experienced COPD exacerbation in a year by ΔFVC quartile and ΔFEV1 quartile. FVC quartile showed the decreasing tendency of moderate-to-severe exacerbation without clinical significance. In the comparison by FEV1 quartiles, they did not show any significant differences. COPD chronic obstructive pulmonary disease, Δ annual changes of the postbronchodilator values, FEV1 forced expiratory volume in one second, FVC forced vital capacity, Q quartile.
Differences between the exacerbation and non-exacerbation groups
We compared the clinical characteristics of patients who experienced and those who did not experience exacerbations. BMI was lower in the moderate AE group compared to non-AE group (22.7 ± 3.3 vs. 23.5 ± 3.6, p < 0.01). Other demographic data, such as age, sex, and smoking status, were not different between the two groups. Osteoporosis was more common in the moderate AE group compared to the non-AE group (10.9% vs. 4.1%, p < 0.01), while other comorbidities had a similar frequency between the groups. Osteoporosis was also more frequent in the moderate-to-severe AE group compared to the non-AE group (11.2% vs. 3.5%, p < 0.01). The history of past AEs was higher in AE group than in non-AE group (moderate AEs [32.5% vs. 16.2%, p < 0.01] and moderate-to-severe AEs [32.9% vs. 15.1%], both p < 0.01). The proportion of baseline 6MWD was different between the AE group and the non-AE group, but no significant differences were observed for other demographic data.
A higher percentage of FVC-decline patients were included in the moderate and moderate-to-severe AE groups. FVC-decline patients constituted 61.4% of the moderate AE group compared to 50.9% of the non-AE group (p = 0.02). Similarly, FVC-decline patients constituted 60.9% of the moderate-to-severe AE group compared to 50.8% of the non-AE group (p = 0.03). Conversely, the proportion of FEV1-decline patients was not different between the moderate and moderate-to-severe AE groups (p = 0.87 and p = 0.70, respectively) (Table 3).
FVC-decline group, not FEV1-decline group, was associated with exacerbation in ACO patients
Univariable and multivariable logistic regression analyses were used to evaluate the factors associated with exacerbations in ACO patients (Table 4). Analyses were performed by two models, such as model 1 for ΔFVC and model 2 for ΔFEV1. Age, sex, BMI, 6MWD, and history of past AEs were selected as common variables because these were associated with next AEs in many previous articles10,18. Osteoporosis, and GERD were selected as variables because these were different factors in demographic analyses (FVC-decline vs. FVC-incline group and AEs “Yes” vs. AEs “No” group). In the unadjusted analyses, FVC-decline group (odds ratio [OR] = 1.53; 95% confidence interval [CI] 1.06–2.22; p = 0.02) was associated with moderate COPD exacerbation. After adjusted, FVC-decline group (OR = 1.58; 95% CI 1.02–2.44; p = 0.04) was still associated with moderate COPD exacerbation. For moderate-to-severe AEs, FVC-decline group showed significant association both in unadjusted analysis (OR 1.51; 95% CI 1.05–2.18, p = 0.03) and in adjusted analysis (OR 1.56; 95% CI 1.01–2.41, p < 0.05). On the other hand, FEV1-decline group did not showed association with moderate and moderate-to-severe COPD exacerbation both in unadjusted and in adjusted analyses. Details for other variables were summarized in Supplementary Table 3.
Discussion
Traditional lung function test variables, such as FEV1, are associated with long-term mortality in COPD patients19. However, they are not strongly associated with the respiratory symptoms, quality of life, or exacerbation of these patients20,21. Therefore, Global Initiative for Chronic Obstructive Lung Disease guidelines recommend the management by the symptom and risk of exacerbation10. It is important but frequently overlooked that COPD is diagnosed based on the FEV1/FVC ratio, not FEV1 alone. However, the role of FVC in COPD evaluation is not clear. Previous studies have reported that the variation in FVC among COPD patients, particularly before and after an exacerbation, was greater compared to that of FEV117,22. A similar situation was observed for ACO patients. Large longitudinal study showed that FVC changes in ACO was different from that of healthy adults, like in COPD. However, no previous studies have focused on FVC changes as prognostic value for clinical outcomes in ACO13.
In this ACO study, we identified some interesting points of FVC changes. First, grouping by FVC changes well explained symptoms and exacerbation of ACO after 1 year. The FVC-decline group existed in 56% of ACO patients. The SGRQ-C scores in 1 year after were higher in the FVC-decline group than in the FVC-incline group, especially in total, activity, and impact scores. They also showed negative relationship in comparison by quartile range. The annual frequency of COPD exacerbation was higher in FVC-decline group than in FVC-incline group. After adjusting confounding variables, the risk of moderate (OR 1.58) and moderate-to-severe exacerbation (OR 1.56) was higher in the FVC-decline group than in the FVC-incline group. These results supported the value of FVC changes in ACO explanation, which was not seen in previous studies. Theoretical mechanism of these results can be explained by increased residual volume (RV) or air-trapping. There were many reports that RV/total lung capacity (TLC) was the markers of lung hyperinflation and were associated with AEs23,24,25. FVC-decline is coincided with increased RV, which finally leads to increased RV/TLC13,17. In a recent study, Alter et al. showed that FVC was an alternative value of RV/TLC, which represented air-trapping or pulmonary hyperinflation26. Especially in absence of body plethysmography, FVC can be a good lung function marker on behalf of the role of RV/TLC as a predictor of COPD exacerbations. Further studies should be followed including subjects such as the cut-off values of FVC changes for predicting next AEs or possibility of FVC changes as COPD lung function phenotypes in near future.
Second, FVC changes were valuable than FEV1 changes in explaining exacerbation of ACO. In the logistic regression analyses, FVC changes had prognostic value which was not shown in FEV1 changes. We also showed the decreasing trends of moderate and moderate-to-severe exacerbations as the quartile of FVC changes increases. These highlighted the importance of FVC (but not FEV1) which was associated with exacerbation in ACO. ACO showed higher BDR of FEV1 which means that FEV1 can be affected by other conditions such as individual efforts, medication, and exacerbation17. It is the possible reason why FVC changes showed significant results compared to FEV1 changes.
There were several limitations in this study. First, we did not compare the outcomes between different ACO diagnostic criteria. However, the diagnosis criteria of ACO have not been fully established. We did not want to miss any cases of ACO to avoid the selection bias. Future studies should compare outcomes between different ACO diagnostic criteria. Second, we only used the 1-year follow-up data. However, we set this study to understand the intuitive relationship between FVC changes and outcomes of ACO management. We showed the clinical difference of SGRQ-C changes by FVC grouping compared to those of by FEV1 grouping. Also, we showed the association of exacerbation with FVC changes as originally hypothesized. Further study should be analyzed in details for evaluating consistent results by the long-term follow-up data. Third, there was no contained radiographic data for analyzing the relationship between FVC changes and air trapping in this study. However, we previously described that FVC itself was a good marker of air trapping. Future study about the association of the diameter of bronchi or low attenuation area that are measured by chest tomography scan with FVC changes should be good subjects to evaluate.
This study is the first to report the importance of FVC changes that it is associated with exacerbations in ACO. FVC changes should be considered in managing ACO patients.
Methods
Data sources and protocols
The Korea COPD Subgroup Study (KOCOSS) cohort is a prospective, multicenter, and observational cohort study that recruited participants from 58 referral university hospitals in South Korea. The KOCOSS protocol was registered at www.clinicaltrial.gov (NCT02800499). For the current study, we used 1-year follow-up data from the KOCOSS database. All participants were recruited between 2012 and 2019. Details of the KOCOSS cohort have been described previously27,28,29.
Study population and design
KOCOSS cohort included COPD patients aged ≥ 40 years with a post-BD FEV1/FVC ratio < 0.70, and respiratory symptoms such as cough, sputum production, or dyspnea29. Patients were excluded if they are (1) not suitable for pulmonary function test or communication, (2) recent myocardial infarction or cerebrovascular event (≤ 3 months), (3) pregnant, (4) underlying rheumatoid disease, (5) cancer or hematologic malignancy patients, or (6) used systemic corticosteroid (≥ 10 mg/day) within 1 month. Among KOCOSS cohort participants, we extracted ACO patients who was diagnosed based on various diagnostic criteria, such as the modified Spanish, updated Spanish, and American Thoracic Society (ATS) roundtable criteria, as well as a specialist’s diagnosis30,31. Patients were included if they fulfill at least one of the ACO criteria.
-
(1)
Modified Spanish COPD guideline criteria (at least 1 major or 2 minor)
-
(A)
Major: (i) previous history of asthma, (ii) Bronchodilator response (BDR) > 15% and 400 mL
-
(B)
Minor: (i) Ig E > 100 IU, or history of atopy, (ii) BDR > 12% and 200 mL, (iii) blood eosinophil > 5%
-
(A)
-
(2)
Updated Spanish COPD guideline criteria (A and B or A and C)
-
(A)
Age ≥ 35, ≥ 10 pack-year smoking history, and post-BD FEV1/FVC < 0.7
-
(B)
Current diagnosis of asthma
-
(C)
BDR > 15% and 400 mL, and/or blood eosinophilia ≥ 300 cell/μL
-
(A)
-
(3)
ATS roundtable criteria
-
(A)
Major: (i) post-BD FEV1/FVC < 0.7 and Age ≥ 40, (ii) ≥ 10 pack-year smoking or exposure to air pollution ≥ 10 years, (iii) history of asthma before 40-year-old or BDR > 400 mL in FEV1
-
(B)
Minor: (i) history of atopy or allergic rhinitis, (ii) separate BDR ≥ 12% and 200 mL, (iii) blood eosinophil ≥ 300 cell/μL
-
(A)
-
(4)
Specialist’s diagnosis: answer yes to this question “Is this patient likely to be classified as ACO?”
We excluded patients who did not undergo the follow-up lung function tests. We divided the patients into FVC-decline and FVC-incline groups on the basis of post-BD FVC changes. We compared the demographics between the groups. To analyze the predictive value of FVC and FEV1, clinical outcomes such as respiratory symptoms and AEs were compared. We also compared the ability of FVC and FEV1 changes to predict exacerbations during the 1-year follow up.
Study variables
The demographic data of patients were collected at KOCOSS enrollment. Age, sex, BMI, smoking status, and comorbidities such as myocardial infarction, heart failure, peripheral vessel disease, diabetes, hypertension, osteoporosis, and GERD were recorded. Pulmonary function tests (PFT, including pre- and post-BD tests) were conducted at baseline. Symptoms and exercise capacity were evaluated using the modified Medical Research Council scale, SGRQ-C, and 6MWD. History of AEs within one year was recorded also at the enrollment. At 1 year, all variables including PFT with post-BD tests, SGRQ-C, and 6MWD were gathered at the same time. All tests were voluntarily performed. If patients do not want, they did not perform the previously mentioned tests under free will. Moderate and severe AE were recorded also.
Definition of exacerbation
Currently, there is no established consensus of AEs in ACO. Moreover, the definition of AEs in COPD differs from that in asthma. The definition of exacerbations in this study was adopted from the guideline of Global Initiative for Chronic Obstructive Lung Disease (GOLD), because all cohort data was originally targeted COPD patients10. As previously mentioned in GOLD guideline, AE was defined by acute change of respiratory symptoms, which need medication changes such as systemic corticosteroid or antibiotics10. Among them, severe AE was defined who requires hospitalization or care of emergency room for management of changed symptoms32.
Statistical analyses
We used the Student’s t-test for compare continuous variables. Pearson’s chi-square test and Fisher’s exact test were used to compare categorical variables. Kruskal–Wallis test was used for comparing the means of multiple groups and Bonferroni method was used for post-hoc analyses. Univariable and multivariable logistic regression analyses were used to identify predictors of AE. P values < 0.05 were considered statistically significance. The statistical analyses were performed using RStudio (version: 2020; RStudio, Inc., Boston, MA, USA).
Ethical approval and consent to participate
Current study was conducted according to the Helsinki declaration, and it was approved by the Ethics Committee of each participating medical center. Relevant data was provided by anonymous form. All participants provided written informed consent prior to enrollment. The lists of participated medical centers and their Ethics Committee were as follows: Gachon University Gil Medical Center, Gangnam Severance Hospital, Gangdong Kyung Hee University Hospital, Kangbuk Samsung Hospital, Gangwon National University Hospital, Konkuk University Medical Center, Kyungpook National University Hospital, Kyung Hee University Medical Center, Keimyung University Dongsan Medical Center, Korea University Guro Hospital, Korea University Anam Hospital, Dong-A University Hospital, Pusan National University Hospital, The Catholic University of Korea Bucheon St. Mary’s Hospital, Soonchunhyang University Hospital, Bundang Cha Medical Center, Nowon Eulji Medical Center, Seoul National University Hospital, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Samsung Medical Center, The Catholic University of Korea Seoul St. Mary’s Hospital, The Catholic University of Korea St. Vincent’s Hospital, Severance Hospital, Ajou University Hospital, The Catholic University of Korea Yeouido St. Mary’s Hospital, Yeungnam University Medical Center, Yongin Severance Hospital, Ulsan University Hospital, Dongkang Hopital, wonkwang university Hospital, Wonju Severance Christian Hospital, The Catholic University of Korea, Eunpyeong St. Mary's Hospital, The Catholic University of Korea Uijeongbu St. Mary’s Hospital, Ewha Womans University Medical Center, The Catholic University of Korea Incheon St. Mary’s Hospital, Inje University Ilsan Paik Hospital, Chosun University Hospital, Chonnam National University Hospital, Jeonbuk National University Hospital, Jeju National University Hospital, Gyeongsang National University Changwon Hospital, Chungnam National University Hospital, Hallym University Medical Center, Kangdong Sacred Heart Hospital, Hallym University Sacred Heart Hospital, Hanyang University Medical Center, Inje University Haeundae Paik Hospital.
Data availability
Researchers may send reasonable requests for access to the datasets used in this study to the corresponding author.
References
An, T. J. et al. Effects of macrolide and corticosteroid in neutrophilic asthma mouse model. Tuberc. Respir. Dis. (Seoul) 81(1), 80–87 (2018).
Viegi, G. et al. Definition, epidemiology and natural history of COPD. Eur. Respir. J. 30(5), 993–1013 (2007).
An, T. J. et al. Inhaled corticosteroid is not associated with a poor prognosis in COVID-19. Respirology 26(8), 812–815 (2021).
Barrecheguren, M. et al. Identification and definition of asthma-COPD overlap: The CanCOLD study. Respirology 25(8), 836–849 (2020).
Pérez-de-Llano, L. et al. Asthma-COPD overlap is not a homogeneous disorder: Further supporting data. Respir. Res. 18(1), 183 (2017).
Sin, D. D. et al. What is asthma−COPD overlap syndrome? Towards a consensus definition from a round table discussion. Eur. Respir. J. 48(3), 664–673 (2016).
Yanagisawa, S. & Ichinose, M. Definition and diagnosis of asthma–COPD overlap (ACO). Allergol. Int. 67(2), 172–178 (2018).
Hiles, S. A., Gibson, P. G. & McDonald, V. M. Disease burden of eosinophilic airway disease: Comparing severe asthma, COPD and asthma–COPD overlap. Respirology 26(1), 52–61 (2021).
Hosseini, M., Almasi-Hashiani, A., Sepidarkish, M. & Maroufizadeh, S. Global prevalence of asthma-COPD overlap (ACO) in the general population: A systematic review and meta-analysis. Respir. Res.h. 20(1), 229 (2019).
2020 Global Initiative for Chronic Obstructive Lung Disease I. Global Strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Available from: https://goldcopd.org/2021-gold-reports/ (2021)
Kim, T. B. et al. Factors associated with severity and exacerbation of asthma: A baseline analysis of the cohort for reality and evolution of adult asthma in Korea (COREA). Ann. Allergy Asthma Immunol. 103(4), 311–317 (2009).
Leem, A. Y. et al. Longitudinal decline in lung function: A community-based cohort study in Korea. Sci Rep. 9(1), 13614 (2019).
de Marco, R. et al. Asthma, COPD and overlap syndrome: A longitudinal study in young European adults. Eur. Respir. J. 46(3), 671–679 (2015).
Park, S. Y. et al. Longitudinal analysis to better characterize Asthma-COPD overlap syndrome: Findings from an adult asthma cohort in Korea (COREA). Clin. Exp. Allergy 49(5), 603–614 (2019).
Park, H. Y. et al. Favorable longitudinal change of lung function in patients with asthma-COPD overlap from a COPD cohort. Respir. Res. 19(1), 36 (2018).
Jo, Y. S. Current status of studies investigating asthma-chronic obstructive pulmonary disease overlap in Korea: A review. Tuberc. Respir. Dis. 85, 101–110 (2021).
Lim, J. U. et al. Clinical characteristics and changes of clinical features in patients with asthma-COPD overlap in Korea according to different diagnostic criteria. Tuberc. Respir. Dis. (Seoul) 83(Supple 1), S34–S45 (2020).
Celli, B. R. et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N. Engl. J. Med. 350(10), 1005–1012 (2004).
Menezes, A. M. B. et al. FEV1 is a better predictor of mortality than FVC: The PLATINO cohort study. PLoS ONE 9(10), e109732-e (2014).
Han, M. K. et al. GOLD 2011 disease severity classification in COPDGene: A prospective cohort study. Lancet Respir. Med. 1(1), 43–50 (2013).
Jones, P. W. Health status and the spiral of decline. COPD 6(1), 59–63 (2009).
Halpin, D. M. G. et al. Effect of a single exacerbation on decline in lung function in COPD. Respir. Med. 128, 85–91 (2017).
Shin, T. R. et al. The prognostic value of residual volume/total lung capacity in patients with chronic obstructive pulmonary disease. J. Korean Med. Sci. 30(10), 1459–1465 (2015).
Kakavas, S. et al. Pulmonary function testing in COPD: Looking beyond the curtain of FEV1. NPJ Primary Care Respir. Med. 31(1), 23 (2021).
Kim, Y. et al. Air trapping and the risk of COPD exacerbation: Analysis from prospective KOCOSS cohort. Front. Med. (Lausanne). 9, 835069 (2022).
Alter, P. et al. Prediction of air trapping or pulmonary hyperinflation by forced spirometry in COPD patients: Results from COSYCONET. ERJ Open Res. 6(3), 00092–02020 (2020).
Choi, J. Y. et al. Clinical characteristics of chronic obstructive pulmonary disease in female patients: Findings from a KOCOSS cohort. Int. J. Chronic Obstruct. Pulm. Dis. 15, 2217–2224 (2020).
Jo, Y. S. et al. Exhaled nitric oxide in patients with stable chronic obstructive pulmonary disease: Clinical implications of the use of inhaled corticosteroids. Tuberc. Respir. Dis. (Seoul) 83(1), 42–50 (2020).
Lee, J. Y. et al. Characteristics of patients with chronic obstructive pulmonary disease at the first visit to a pulmonary medical center in Korea: The Korea COPD subgroup study team cohort. JKMS 31(4), 553–560 (2016).
Jo, Y. S. et al. Comparing the different diagnostic criteria of asthma-COPD overlap. Allergy 74(1), 186–189 (2019).
Jo, Y. S. et al. Different prevalence and clinical characteristics of asthma-chronic obstructive pulmonary disease overlap syndrome according to accepted criteria. Ann. Allergy Asthma Immunol. 118(6), 696–703 (2017).
An, T. J. Y. et al. Diaphragm ultrasound is an imaging biomarker that distinguishes exacerbation status from stable chronic obstructive pulmonary disease. Int. J. Chronic Obstruct. Pulm. Dis. 17, 3–12 (2022).
Funding
This work was supported by the Research Program funded Korea National Institute of Health. (Fund CODE 2016ER670100, 2016ER670101, 2016ER670102, 2018ER67100, 2018ER67101, 2018ER67102, 2021ER120500 and 2021ER120501).
Author information
Authors and Affiliations
Contributions
T.J.A. and H.K.Y. conceptualized the study. T.J.A. curated and analyzed the data. The investigations were performed by C.K.R., Y.B.P., and K.H.Y. The methodology was devised and reviewed by C.K.R., Y.B.P., K.H.Y., and H.K.Y. Project administration and resource management were done by K.H.Y. The software was managed by T.J.A. The study was supervised by C.K.R., Y.B.P., and K.H.Y. Validation was performed by C.K.R. and H.K.Y. Visualization, original draft writing, and manuscript review and editing were done by T.J.A. All authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
An, T.J., Rhee, C.K., Park, Y.B. et al. FVC, but not FEV1, is associated with clinical outcomes of asthma-COPD overlap. Sci Rep 12, 13820 (2022). https://doi.org/10.1038/s41598-022-15612-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-15612-w
- Springer Nature Limited