
Abstract
Metastatic triple-negative breast cancer (mTNBC) is a heterogeneous disease with a poor prognosis. Individualized survival prediction tool is useful for this population. We constructed the predicted nomograms for breast cancer-specific survival (BCSS) and overall survival (OS) using the data identified from the Surveillance, Epidemiology, and End Results database. The Concordance index (C-index), the area under the time-dependent receiver operating characteristic curve (AUC) and the calibration curves were used for the discrimination and calibration of the nomograms in the training and validation cohorts, respectively. 1962 mTNBC patients with a median follow-up was 13 months (interquartile range, 6–22 months), 1639 (83.54%) cases died of any cause, and 1469 (74.87%) died of breast cancer. Nine and ten independent prognostic factors for BCSS and OS were identified and integrated to construct the nomograms, respectively. The C-indexes of the nomogram for BCSS and OS were 0.694 (95% CI 0.676–0.712) and 0.699 (95% CI 0.679–0.715) in the training cohort, and 0.699 (95% CI 0.686–0.712) and 0.697 (95% CI 0.679–0.715) in the validation cohort, respectively. The AUC values of the nomograms to predict 1-, 2-, and 3-year BCSS and OS indicated good specificity and sensitivity in internal and external validation. The calibration curves showed a favorable consistency between the actual and the predicted survival in the training and validation cohorts. These nomograms based on clinicopathological factors and treatment could reliably predict the survival of mTNBC patient. This may be a useful tool for individualized healthcare decision-making.
Similar content being viewed by others


Introduction
Breast cancer is the most common cancer in women and the leading cause of cancer-related deaths worldwide1,2. Among all newly diagnosed breast cancers, about 5–10% are de novo metastatic diseases3. The transition from phenotypic research to the exploration of intrinsic molecular subtypes has made a substantial transformation in the management of breast cancer1. Molecular-targeted therapies and precision medicine has greatly improved the prognosis of patients with specific genetic backgrounds2,3,4. However, the overall prognosis of metastatic breast cancer is still poor and heterogeneous. Triple negative breast cancer (TNBC) is the subtype of breast cancer with the most aggressive biological behavior, and is associated with a poor prognosis. Chemotherapy is the primary established systemic treatment for TNBC patients5,6. With the improvement of treatment strategies, the mortality rate for patients with de novo metastatic TNBC (mTNBC) is decreasing. However, the survival of this patients remains unsatisfactory7,8,9,10,11. Accurately predicting the prognosis of these patients can help guide clinical decision-making. At present, the American Joint Committee on Cancer (AJCC) TNM staging system is one of the best-established tools to predict survival for breast cancer. However, once the patients are confined to those with metastatic diseases, its prognostic value becomes limited. Therefore, an effective and accurate prognostic prediction model is urgently desired for this population.
Nomogram has been widely used for prognostic estimation in oncology. With the ability to generate individual probabilities of clinical events by integrating diverse prognostic and determinant variables, nomograms meet the demands for integrated biological-clinical models, and promotes the development of personalized medicine12,13. Nomograms can provide rapid computation through user-friendly digital interfaces, and output results that are easy to understand14,15. However, the survival predicting nomogram for mTNBC patients is needed. Therefore, in this study, we identified clinicopathologic factors associated with the prognosis of mTNBC patients using population-based data, and developed a nomogram based on these prognostic factors for individualized survival prediction.
Materials and methods
This study protocol was approved by the Clinical Research Ethics Committee of the Affiliated Suining Central Hospital of Chongqing Medical University (No. LLSLH20210029). Written informed consent was waived for this study as for all patients have given prior informed consent to being registered in SEER database. This study was conducted according to the type 2a of prediction model studies and the article in accordance with the TRIPOD Statement16.
Patients selection
After acquiring the access, we extracted eligible cases from the Research Plus Database of the Surveillance, Epidemiology, and End Results (SEER) program (https://seer.cancer.gov/, released April 2021), which consists of 18 population-based cancer registries. Cases that met the following inclusion criteria were generated using SEER*Stat Version 8.3.9 software: female, diagnosed from 2010 to 2017, age at diagnosis was older and equal to 18-year-old, pathologically confirmed as breast carcinoma, breast cancer as the first primary unilateral tumor, and the AJCC stage IV. Inflammatory breast cancer was allowed to be included. Cases with data obtained from death certificates or autopsy reports, or those without follow-up information were excluded. Patients’ unknown of race, marital status, tumor stage, node stage, histology, or history of breast surgery were excluded.
Variables
We extracted the demographic features (including year of diagnosis, age at diagnosis, race, and marital status), clinicopathological characteristics (including histological type, tumor stage, node stage, TNM stage, bone metastasis, lung metastasis, liver metastasis, brain metastasis, and breast cancer subtype), treatment (including breast surgery, radiotherapy, and chemotherapy), and survival data (including survival months, vital status, etc.) of each case. Patients were grouped into five groups according to the age of diagnosis: 18–40 years old, 41–50 years old, 51–60 years old, 61–60 years old, and > 70 years old. Patients were classified as invasive ductal carcinoma (IDC, Code: 8500/3) and invasive lobular carcinoma (ILC, Code: 8522/3)/Others according to the International Classification of Diseases for Oncology third edition (ICD-O-3). The tumor TNM stage classification was based on the AJCC breast cancer system 7th edition.
The main outcomes of this study were breast cancer-specific survival (BCSS) and overall survival (OS). BCSS was defined as the interval (month) from the diagnosis to the breast cancer-related death, with lose of follow-up or death of other causes as censored data. OS was defined as the interval (month) from the diagnosis to death of any cause, with lose of follow-up was as censored data.
Statistical analysis
Patients were randomly divided into the training and the validation cohorts at the ratio of 7:3. Chi-square test was used to determine the consistency of clinicopathological characteristics between the training and the validation cohorts. Parameters with a P value less than 0.1 in univariate Cox analysis or with a clinical consideration of potential prognostic factors were included in the multivariable Cox model to identify independent prognostic factors in the training cohort. The nomograms to predict 1-, 2-, and 3-year BCSS and OS were constructed based on the independent prognostic factors. The performance of the nomograms was evaluated in the training set and the validation set, respectively. The concordance index (C-index), time-dependent receiver operating characteristic (ROC) curve, and the area under the ROC curve were used to evaluate the distinguishing ability of the nomograms. The C-index and AUC value range from 0 to 1, and a higher value indicates a stronger predictive ability, and the value between 0.7 and 0.9 is generally considered to have well identification ability. The calibration curves were used to evaluate the accuracy of point estimates of nomogram-predicted survival with the actual survival. Bootstrap resample method (B = 1000) was used for calibration curve plot. The Survival curves were plotted by Kaplan–Meier method. Statistical analyses and figure plots were conducted by R software version 4.0.3 (www.r-project.org) using the packages of ‘survminer’, ‘survival’, ‘rms’, and ‘riskRegression’. All statistical analyses were two-sided, and a P value of less than 0.05 was considered statistically significant.
Ethics statement
This study protocol was approved by the Clinical Research Ethics Committee of the Affiliated Suining Central Hospital of Chongqing Medical University (No. LLSLH20210029).
Results
Patient characteristics
A total of 1962 patients met the criterial and were included in our analyses (Fig. 1). The demographic characteristics, clinicopathological features, and treatments of all patients were summarized in Table 1. Among all patients, the median age at diagnosis was 59 years (IQR: 50–69 years). Most (67.79%) of the patients were white. The percentage of distance metastasis of bone, lung, liver, and brain were 44.14%, 39.40%, 27.12%, and 9.93%, respectively. 864 (44.04%) patients received primary breast surgery including mastectomy (628 patients, 32.01%) and breast-conserving surgery (236 patients, 12.03%). 703 (35.83%) patients received radiotherapy, and 81.14% (1592) of patients received chemotherapy. Patients were randomly allocated into the training cohort (N = 1369) and the validation cohort (N = 593), and the distributions of clinicopathological features between the two cohorts were balanced (Table 1).

Flow chart of patient selection.
Identification of predictors in training set
The median follow-up was 13 months (IQR: 6–22 months) for all patients. Among them, 1639 (83.54%) cases died of any cause, and 1469 (74.87%) cases died of breast cancer. There was no significant difference detected in the estimated 1-, 2-, and 3-year BCSS and OS between the total cohort, the training cohort, and the validation cohort (Table 2 and Fig. 2). The BCSS and OS rates between patients with different number of metastatic organs in training cohort were significantly different (Supplementary Fig. 1A,B and Table 1).

Survival curves of BCSS (A) and OS (B) in training and validation cohorts.
The results of univariate Cox analyses in the training cohort showed that age at diagnosis, marital status, tumor stage, node stage, bone metastasis, lung metastasis, liver metastasis, brain metastasis, breast surgery, radiotherapy, and chemotherapy were the potential prognostic factors for BCSS and OS (Table 3). Considering the interaction between the metastatic site and the number of metastatic organs, the metastatic organs were included in the Cox model to well investigate the impact of metastatic pattern on the survival. In multivariable Cox analysis, age at diagnosis, marital status, tumor stage, node stage, bone metastasis, liver metastasis, brain metastasis, breast surgery, and chemotherapy were the independent prognostic factors for BCSS and OS (Table 3). In addition, radiotherapy was significantly associated with the OS in patients with mTNBC (Table 3).
Construction of the nomograms for BCSS and OS
The nomograms were constructed based on the independent prognostic factors identified by the multivariable Cox model. Nine variables including tumor stage, node stage, bone metastasis, liver metastasis, brain metastasis, breast surgery, chemotherapy, marital status, and age at diagnosis were contained in the nomogram for BCSS (Fig. 3A). Ten variables including tumor stage, node stage, bone metastasis, liver metastasis, brain metastasis, breast surgery, radiotherapy, chemotherapy, marital status, and age at diagnosis were contained in the nomogram for OS (Fig. 3B).

Nomograms for BCSS (A) and OS (B) in training cohort.
Validation of the nomograms
The C-indexes of the nomogram for BCSS and OS were 0.694 (95% CI 0.676–0.712) and 0.699 (95% CI 0.679–0.715) in the training cohort, and 0.699 (95% CI 0.686–0.712) and 0.697 (95% CI 0.679–0.715) in the validation cohort, respectively.
The time-dependent ROC was used to evaluate the point predictive values of the nomograms. In internal validation, the AUC values of the nomogram to predict 1-, 2-, and 3-year BCSS were 0.748 (95% CI 0.722–0.775), 0.738 (95% CI 0.706–0.769), and 0.772 (95% CI 0.738–0.806), respectively (Fig. 4A). In external validation, the AUC values of the nomogram to predict 1-, 2-, and 3-year BCSS were 0.768 (95% CI 0.730–0.807), 0.698 (95% CI 0.646–0.750), and 0.746 (95% CI 0.684–0.807), respectively (Fig. 4B). In the training cohort, the AUC values of the nomogram to predict 1-, 2-, and 3-year OS were 0.751 (95% CI 0.726–0.777), 0.747 (95% CI 0.716–0.777), and 0.783 (95% CI 0.749–0.817), respectively (Supplementary Fig. 2A). In the validation cohort, the AUC values of the nomogram to predict 1-, 2-, and 3-year OS were 0.768 (95% CI 0.731–0.806), 0.707 (95% CI 0.655–0.759), and 0.755 (95% CI 0.695–0.816), respectively (Supplementary Fig. 2B).

ROC curves and AUC for 1-, 2-, and 3-year BCSS in training (A) and validation (B) cohorts.
The 1-, 2-, and 3-year calibration curves of the nomogram for the prediction of BCSS demonstrated a good consistency in training cohort (Fig. 5A–C) and validation cohort (Fig. 5D–F). Similarly, the calibration curves of the nomogram for OS revealed a good consistency in two cohorts (Supplementary Fig. 3).

Calibration curves of 1-, 2-, and 3-year BCSS in training and validation cohorts. (A–C) Calibration curves of 1-, 2-, and 3-year BCSS in training cohort, respectively. (D–F) Calibration curves of 1-, 2-, and 3-year BCSS in validation cohort, respectively.
Stratified survival analysis based on nomograms
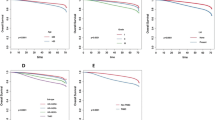
The risk score of each case in training and validation set were calculated based the nomograms for BCSS and OS. Patients were classified as low- and high-risk group with the cutoff of median risk score (BCSS: 110 points; OS: 90 points). The discrepancy of the median BCSS between low- and high-risk patients were 12 months and 9 months in training (21 months versus 9 months) and validation (17 months versus 8 months) sets, respectively (Fig. 6A,B). The discrepancy of the median OS between low- and high-risk patients were 11 months and 9 months in training (20 months versus 9 months) and validation (17 months versus 8 months) sets, respectively (Fig. 6C,D).

Survival curves of BCSS and OS stratified by nomogram estimated risk. (A, B) BCSS in training and validation cohort, respectively. (C, D) OS in training and validation cohort, respectively.
Discussion
Metastatic breast cancer remains an incurable disease, although the survival has been improved in the past few decades thanks to advances in systemic treatment options17. The median overall survival for mTNBC is about 15 months9, and accurately estimating the prognosis of individual patients in this population can help medical care decision-making. We used data of the mTNBC patients extracted from the SEER database to identify the prognostic factors, and developed the nomograms to predict the 1-,2- and 3-year BCSS and OS. The nomogram showed good discrimination in both internal and external validations and is expected to provide favorable guidance for prognosis prediction and disease management. Previous studies have shown that a later time of diagnosis and treatment was associated with a better prognosis18,19. However, year of diagnosis was not associated with improved survival in the current multivariable Cox model, which might be related to the inherently poor prognosis of the disease and the insignificant improvement in treatment within a short period of time. Health gains and cost effectiveness are negatively related to age at diagnosis. Younger patients with stage IV breast cancer have better survival than their older counterparts20,21. In our analysis, we found that age was a significant prognostic factor for mTNBC patients.
Accumulated evidence has confirmed that race plays an independent prognostic role in TNBC patients, and that black women have a poorer survival than the white22,23. Comparing to white patients, black women had more advanced disease at diagnosis, had more germline BRCA mutations, had lower socioeconomic status, and received fewer treatments24. However, as indicated in our study, race was not an independent predictor of prognosis in mTNBC. Therefore, the racial/ethnic disparities in prognosis might be the result of unequal insurance coverage and access to care. Marital status is strongly associated with improved health and longevity. A growing body of evidence has shown that the mortality of unmarried breast cancer patients is higher than that of married patients, which may be explained married patients can get more mental and financial support from their partners25,26. Again, this conclusion was confirmed in our study. Although the needs of breast cancer patients can be partially provided by their children and relatives, not all of them can be provided. In unmarried patients, the marriage after the breast cancer diagnosis also has the positive impact on the survival27.
At present, the treatment strategy and prognostic prediction for invasive breast cancer patients are mainly based on the TNM staging system. According to our report, nodal stage does not affect the prognosis of mTNBC patients. Stage T4 breast cancers, including tumors with chest wall invasion (T4a), skin invasion consisting of ulceration or nodules (T4b) or both (T4c), and inflammatory breast cancer (IBC), had unfavorable influences on the prognosis. Besides, tumor histology were not independent predictors of prognosis in the multivariable analysis. In this cohort, the cumulative incidence of bone, liver, lung, and brain metastases were 41.13%, 39.78%, 26.97%, and 9.79%, respectively. Any site of distant metastasis except for lung confers a worse prognosis, and the survival was worse with the increased number of metastatic organs. Why is there no statistical significance in the effect of lung metastasis on survival in our data? TNBC is prone to visceral metastasis, which usually has more than two sites of metastasis simultaneously5. In this cohort data, over 52% of patients with lung metastasis had metastasis at other organs. The prognostic value of lung metastasis has changed for the interaction with other factors in the multivariable model, which explains why lung metastasis harmed survival in univariate analysis but not in multivariable analysis. Besides, there is also some discrepancy in the treatment sensitivity of different metastatic sites, which could change the prediction value of a variable5,19. In addition, number of lesions in a single metastatic organ may also affect patients’ outcome. This issue needs to be further studied.
Management of mTNBC is aimed at relieving symptoms and extending quality-adjusted life expectancy, and multidisciplinary collaboration is required. Generally, local treatments (surgery and radiation therapy) are not the mainstay of advanced breast cancer treatment, but can be very useful in certain situations. The survival benefits brought by resecting primary tumor in patients with metastatic breast cancer remains controversial, as suggested by some trials28,29,30,31,32. Radiation therapy has a crucial role in alleviating symptoms from bone, brain33,34, and should be prescribed in a multidisciplinary and individualized approach with dose and fractionation schedules depending on the severity of the lesions and the remaining life expectancy. Although previous researches and this analysis have indicated possibility improvement in survival contributed by radiation therapy35, the actual effect should be further validated. Despite less direct evidences about the prognostic value of radiotherapy on mTNBC patients, it should be considered for selected patients based on the pattern and metachronicity of the disease. In line with previous studies, our results suggested that chemotherapy promoted survival independently36,37. Chemotherapy has been the main treatment for TNBC, the change of chemotherapy regimens not only improve the prognosis, but also provide more treatment options. A phase III randomized clinical trial has investigated the efficacy and safety of cisplatin combined with nab-paclitaxel (AP) or gemcitabine (GP) as the first line treatment for metastatic TNBC, and the results demonstrated patients received AP had a longer PFS than that in patient treateated with GP regimen (9.8 months versus 7.4 months)38. Quite recently, while immunotherapy and targeted therapy has been emerging as novel treatment modalities for mTNBC10,11,39, further improvements in patients’ life expectancy and quality are foreseeable. KEYNOTE-355 trail has investigated the efficacy and safety of immunotherapy (pembrolizumab) added to chemotherapy in 847 advanced TNBC. In patients whose tumors expressed programmed death ligand (PD-L1), pembrolizumab could significantly longer survival than chemotherapy alone40. Besides, our previous study, have also shown that novel targeted therapeutic modalities may be an inspiring outlook in triple negative breast cancer41.
The value of local surgery in metastatic breast cancer is controversial. Several randomized clinical trials had investigated the efficacy of surgery in this population28,29,42,43. The results of these studies were inconsistent for the discrepancy in patient features, study design, and background between each study. But, the viewpoint of some patients who may benefit from surgery can be drawn in the modern era. Patients could be classified into a high- or low-risk group according to the nomograms, which could predict a relative worse or good outcome. The prediction tool considered several factors, which would avoid overemphasizing the value of surgery for mTNBC patients. Meanwhile, the prediction model could predict which patient received surgery had a relatively good outcome. Besides, some stage IV patients would accept surgery for local control, when presented with tumor growth, local infection, and bleeding.
In mTNBC patients, the ultimate aims of care are to optimize both quality and life span. The management of mTNBC is complex and, therefore, involvement of all appropriate specialties in a multidisciplinary team (including but not restricted to medical, radiation, surgical oncologists, imaging experts, pathologists, gynecologists, psycho-oncologists, social workers, nurses, and palliative care specialists), is crucial44.
Limitations
Our study has several limitations. First, the SEER database does not provide details about chemotherapy and radiotherapy regimens, which may impact the survival or quality of life differently for mTNBC patients. Second, the information about metastatic involvement of specific organ sites is only collected at the time of initial presentation in SEER, and currently there is no longitudinal follow-up data to document subsequent organs affected. Third, SEER currently does not collect information on other sites of metastases such as distant lymph nodes, pleura, peritoneum, or skin. This information could assist in more specific prognostic assessment of the other metastatic groups. Fourth, the performance status (PS) of each patient were not provided in the SEER database, which was an important factor for clinical decision-making and survival. Finally, these nomograms were based on a retrospective set, and further validation in prospective clinical trials is needed.
Conclusion
The nomograms have been established and validated for predicting BCSS and OS in TNBC patients with metastatic disease, which hold promises in realizing individualized prognostic prediction and identifying the high-risk patients who require more specialized treatment strategies and follow-up plans.
Data availability
The datasets analyzed during the current study are available from the SEER registry https://seer.cancer.gov/. Further inquiries of this study data can be directed to the corresponding author.
Abbreviations
- AJCC:
-
American Joint Committee on Cancer
- AUC:
-
Area under the time-dependent receiver operating characteristic curve
- BCSS:
-
Breast cancer-specific survival
- IBC:
-
Inflammatory breast cancer
- IDC:
-
Invasive ductal carcinoma
- ILC:
-
Infiltrating lobular carcinoma
- IQR:
-
Interquartile range
- mTNBC:
-
Metastatic triple-negative breast cancer
- OS:
-
Overall survival
- ROC:
-
Receiver operating characteristic
- TNBC:
-
Triple-negative breast cancer
References
Ferlay, J. et al. Cancer statistics for the year 2020: An overview. Int. J. Cancer. https://doi.org/10.1002/ijc.33588 (2021).
Siegel, R. L., Miller, K. D., Fuchs, H. E. & Jemal, A. Cancer statistics, 2021. CA Cancer J. Clin. 71, 7–33. https://doi.org/10.3322/caac.21654 (2021).
Heller, D. R., Chiu, A. S., Farrell, K., Killelea, B. K. & Lannin, D. R. Why has breast cancer screening failed to decrease the incidence of de Novo Stage IV Disease?. Cancers (Basel). 11, 500. https://doi.org/10.3390/cancers11040500 (2019).
Pagani, O. et al. International guidelines for management of metastatic breast cancer: Can metastatic breast cancer be cured?. J. Natl. Cancer Inst. 102, 456–463. https://doi.org/10.1093/jnci/djq029 (2010).
Bianchini, G., Balko, J. M., Mayer, I. A., Sanders, M. E. & Gianni, L. Triple-negative breast cancer: Challenges and opportunities of a heterogeneous disease. Nat. Rev. Clin. Oncol. 13, 674–690. https://doi.org/10.1038/nrclinonc2016.66 (2016).
Li, X. et al. Triple-negative breast cancer has worse overall survival and cause-specific survival than non-triple-negative breast cancer. Breast Cancer Res. Treat. 161, 279–287. https://doi.org/10.1007/s10549-016-4059-6 (2017).
Cortes, J. et al. Pembrolizumab plus chemotherapy versus placebo plus chemotherapy for previously untreated locally recurrent inoperable or metastatic triple-negative breast cancer (KEYNOTE-355): A randomised, placebo-controlled, double-blind, phase 3 clinical trial. Lancet 396, 1817–1828. https://doi.org/10.1016/S0140-6736(20)32531-9 (2020).
Kang, C. & Syed, Y. Y. Atezolizumab (in combination with nab-paclitaxel): A review in advanced triple-negative breast cancer. Drugs 80, 601–607. https://doi.org/10.1007/s40265-020-01295-y (2020).
Kim, S. B. et al. Ipatasertib plus paclitaxel versus placebo plus paclitaxel as first-line therapy for metastatic triple-negative breast cancer (LOTUS): A multicentre, randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Oncol. 18, 1360–1372. https://doi.org/10.1016/S1470-2045(17)30450-3 (2017).
Schmid, P. et al. Atezolizumab and nab-paclitaxel in advanced triple-negative breast cancer. N. Engl. J. Med. 379, 2108–2121. https://doi.org/10.1056/NEJMoa1809615 (2018).
Schmid, P. et al. Atezolizumab plus nab-paclitaxel as first-line treatment for unresectable, locally advanced or metastatic triple-negative breast cancer (IMpassion130): Updated efficacy results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 21, 44–59. https://doi.org/10.1016/S1470-2045(19)30689-8 (2020).
Balachandran, V., Gonen, M., Smith, J. J. & DeMatteo, R. P. Nomograms in oncology: More than meets the eye. Lancet Oncol. 16, e173-180. https://doi.org/10.1016/S1470-2045(14)71116-7 (2015).
Iasonos, A., Schrag, D., Raj, G. V. & Panageas, K. S. How to build and interpret a nomogram for cancer prognosis. J. Clin. Oncol. 26, 1364–1370. https://doi.org/10.1200/JCO.2007.12.9791 (2008).
El Sharouni, M. A. et al. Development and validation of nomograms to predict local, regional, and distant recurrence in patients with thin (T1) melanomas. J. Clin. Oncol. 39, 1243–1252. https://doi.org/10.1200/JCO.20.02446 (2021).
Weiser, M. R. et al. Clinical calculator based on molecular and clinicopathologic characteristics predicts recurrence following resection of stage I–III colon cancer. J. Clin. Oncol. 39, 911–919. https://doi.org/10.1200/JCO.20.02553 (2021).
Collins, G. S., Reitsma, J. B., Altman, D. G. & Moons, K. G. M. Transparent reporting of a multivariable prediction model for individual prognosis or diagnosis (TRIPOD): The TRIPOD statement. BMJ 350, g7594. https://doi.org/10.1136/bmj.g7594 (2015).
Richard, D. R. et al. Calculating the sample size required for developing a clinical prediction model. BMJ 368, m441. https://doi.org/10.1136/bmj.m441 (2020).
Malmgren, J. A., Calip, G. S., Atwood, M. K., Mayer, M. & Kaplan, H. G. Metastatic breast cancer survival improvement restricted by regional disparity: Surveillance, epidemiology, and end results and institutional analysis: 1990 to 2011. Cancer 126, 390–399. https://doi.org/10.1002/cncr.32531 (2020).
Malmgren, J. A., Mayer, M., Atwood, M. K. & Kaplan, H. G. Differential presentation and survival of de novo and recurrent metastatic breast cancer over time: 1990–2010. Breast Cancer Res. Treat. 167, 579–590. https://doi.org/10.1007/s10549-017-4529-5 (2018).
Eng, L. G. et al. Ten-year survival in women with primary stage IV breast cancer. Breast Cancer Res. Treat. 160, 145–152. https://doi.org/10.1007/s10549-016-3974-x (2016).
Iqbal, J., Ginsburg, O., Rochon, P. A., Sun, P. & Narod, S. A. Differences in breast cancer stage at diagnosis and cancer-specific survival by race and ethnicity in the United States. JAMA 313, 165–173. https://doi.org/10.1001/jama.2014.17322 (2015).
Luo, J. et al. Mediation analysis of racial disparities in triple-negative breast cancer incidence among postmenopausal women. Breast Cancer Res. Treat. 188, 283–293. https://doi.org/10.1007/s10549-021-06158-y (2021).
Wang, F. et al. Racial/ethnic disparities in all-cause mortality among patients diagnosed with triple-negative breast cancer. Cancer Res. 81, 1163–1170. https://doi.org/10.1158/0008-5472.CAN-20-3094 (2021).
Walsh, S. M., Zabor, E. C., Stempel, M., Morrow, M. & Gemignani, M. L. Does race predict survival for women with invasive breast cancer?. Cancer 125, 3139–3146. https://doi.org/10.1002/cncr.32296 (2019).
Hinyard, L., Wirth, L. S., Clancy, J. M. & Schwartz, T. The effect of marital status on breast cancer-related outcomes in women under 65: A SEER database analysis. Breast 32, 13–17. https://doi.org/10.1016/j.breast.2016.12.008 (2017).
Iglay, K. et al. Impact of preexisting mental illness on all-cause and breast cancer-specific mortality in elderly patients with breast cancer. J. Clin. Oncol. 35, 4012–4018. https://doi.org/10.1200/JCO.2017.73.4947 (2017).
Ding, W. et al. Dynamic changes in marital status and survival in women with breast cancer: A population-based study. Sci. Rep. 11, 5421. https://doi.org/10.1038/s41598-021-84996-y (2021).
Badwe, R. et al. Locoregional treatment versus no treatment of the primary tumour in metastatic breast cancer: An open-label randomised controlled trial. Lancet Oncol. 16, 1380–1388. https://doi.org/10.1016/S1470-2045(15)00135-7 (2015).
Fitzal, F. et al. Impact of breast surgery in primary metastasized breast cancer: Outcomes of the prospective randomized phase III ABCSG-28 POSYTIVE Trial. Ann. Surg. 269, 1163–1169. https://doi.org/10.1097/SLA.0000000000002771 (2019).
Lane, W. O. et al. Surgical resection of the primary tumor in women with De Novo Stage IV Breast Cancer: Contemporary practice patterns and survival analysis. Ann. Surg. 269, 537–544. https://doi.org/10.1097/SLA.0000000000002621 (2019).
van Uden, D. J. P. et al. Better survival after surgery of the primary tumor in stage IV inflammatory breast cancer. Surg. Oncol. 33, 43–50. https://doi.org/10.1016/j.suronc.2020.01.005 (2020).
Yao, N. et al. Primary tumor removal improves the prognosis in patients with stage IV breast cancer: A population-based study (cohort study). Int. J. Surg. 83, 109–114. https://doi.org/10.1016/j.ijsu.2020.08.056 (2020).
Chow, E. et al. Single versus multiple fractions of repeat radiation for painful bone metastases: A randomised, controlled, non-inferiority trial. Lancet Oncol. 15, 164–171. https://doi.org/10.1016/S1470-2045(13)70556-4 (2014).
Phillips, C., Jeffree, R. & Khasraw, M. Management of breast cancer brain metastases: A practical review. Breast 31, 90–98. https://doi.org/10.1016/j.breast.2016.10.006 (2017).
Morgan, S. C. & Parker, C. C. Local treatment of metastatic cancer–killing the seed or disturbing the soil?. Nat. Rev. Clin. Oncol. 8, 504–506. https://doi.org/10.1038/nrclinonc.2011.88 (2011).
Loibl, S., Poortmans, P., Morrow, M., Denkert, C. & Curigliano, G. Breast cancer. Lancet 397, 1750–1769. https://doi.org/10.1016/S0140-6736(20)32381-3 (2021).
Vidula, N., Ellisen, L. W. & Bardia, A. Novel agents for metastatic triple-negative breast cancer: Finding the positive in the negative. J. Natl. Compr. Canc. Netw. 15, 1–9. https://doi.org/10.6004/jnccn.2020.7600 (2020).
Wang, B. Y. et al. A randomized phase 3 trial of Gemcitabine or Nab-paclitaxel combined with cisPlatin as first-line treatment in patients with metastatic triple-negative breast cancer. Nat. Commun. 13, 4025. https://doi.org/10.1038/s41467-022-31704-7 (2022).
Esteva, F. J., Hubbard-Lucey, V. M., Tang, J. & Pusztai, L. Immunotherapy, and targeted therapy combinations in metastatic breast cancer. Lancet Oncol. 20, e175–e186. https://doi.org/10.1016/S1470-2045(19)30026-9 (2019).
Cortes, J. et al. Pembrolizumab plus chemotherapy in advanced triple-negative breast cancer. N. Engl. J. Med. 387, 217–226. https://doi.org/10.1056/NEJMoa2202809 (2022).
Hou, L. M. et al. Targeted intervention of NF2-YAP signaling axis in CD24-overexpressing cells contributes to encouraging therapeutic effects in TNBC. ACS Nano https://doi.org/10.1021/acsnano.1c10921 (2022).
Khan, S. A. et al. Early local therapy for the primary site in De Novo Stage IV Breast Cancer: Results of a randomized clinical trial (EA2108). J. Clin. Oncol. 40, 978–987. https://doi.org/10.1200/JCO.21.02006 (2022).
Soran, A. et al. Primary surgery with systemic therapy in patients with de Novo Stage IV Breast Cancer: 10-year Follow-up; Protocol MF07–01 randomized clinical trial. J. Am. Coll. Surg. 233, 742-751.e5. https://doi.org/10.1016/j.jamcollsurg.2021.08.686 (2021).
Cardoso, F. et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann. Oncol. 31, 1623–1649. https://doi.org/10.1016/j.annonc.2020.09.010 (2020).
Funding
This study supported by the National Natural Science Foundation of China (No. 81902686), the Fundamental Research Funds for the Central Universities (No. 2021SCU12021), and the Scientific Research Project of Sichuan Health Commission (No. 17PJ599). Young Talent Lifting Project of Suining Science and Technology Association.
Author information
Authors and Affiliations
Contributions
Q.L., J.Y., M.C.: conception, design, and methodology. J.Y., L.X., T.H., and H.W.: data acquisition, curation, and analysis. L.X.: drawing images. M.C. and P.L.: writing-original draft. Q.L. and J.Y.: writing-review, administrative, and material support. P.L. and J.Y.: writing-editing. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
Cite this article
Chen, MS., Liu, PC., Yi, JZ. et al. Development and validation of nomograms for predicting survival in patients with de novo metastatic triple-negative breast cancer. Sci Rep 12, 14659 (2022). https://doi.org/10.1038/s41598-022-18727-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-18727-2
- Springer Nature Limited