
Abstract
Chronic obstructive pulmonary disease (COPD) is among the leading causes of death worldwide and HIV is an independent risk factor for the development of COPD. However, the etiology of this increased risk and means to identify persons with HIV (PWH) at highest risk for COPD have remained elusive. Biomarkers may reveal etiologic pathways and allow better COPD risk stratification. We performed a matched case:control study of PWH in the Strategic Timing of Antiretoviral Treatment (START) pulmonary substudy. Cases had rapid lung function decline (> 40 mL/year FEV1 decline) and controls had stable lung function (+ 20 to − 20 mL/year). The analysis was performed in two distinct groups: (1) those who were virally suppressed for at least 6 months and (2) those with untreated HIV (from the START deferred treatment arm). We used linear mixed effects models to test the relationship between case:control status and blood concentrations of pneumoproteins (surfactant protein-D and club cell secretory protein), and biomarkers of inflammation (IL-6 and hsCRP) and coagulation (d-dimer and fibrinogen); concentrations were measured within ± 6 months of first included spirometry. We included an interaction with treatment group (untreated HIV vs viral suppression) to test if associations varied by treatment group. This analysis included 77 matched case:control pairs in the virally suppressed batch, and 42 matched case:control pairs in the untreated HIV batch (n = 238 total) who were followed for a median of 3 years. Median (IQR) CD4 + count was lowest in the controls with untreated HIV at 674 (580, 838). We found no significant associations between case:control status and pneumoprotein or biomarker concentrations in either virally suppressed or untreated PWH. In this cohort of relatively young, recently diagnosed PWH, concentrations of pneumoproteins and biomarkers of inflammation and coagulation were not associated with subsequent rapid lung function decline.
Trial registration: NCT00867048 and NCT01797367.
Similar content being viewed by others


Introduction
Chronic obstructive pulmonary disease (COPD) and human immunodeficiency virus (HIV) are among the leading causes of death worldwide1. COPD is common in HIV, and HIV is an independent risk factor for the development of COPD, airflow obstruction, and worse lung function2,3. Decreased lung function, airway obstruction, and lower diffusing capacity are associated with increased mortality in people with HIV (PWH)4,5. Smoking, high viral load, and low nadir CD4 + T-cell counts increase susceptibility to COPD among PWH, but underlying mechanisms of how HIV affects COPD pathogenesis remain unknown and biomarkers of COPD risk in PWH have not been established6,7,8,9.
Biomarkers of systemic inflammation and coagulation in PWH are predictive of a variety of clinically important outcomes including death, cardiovascular disease, and malignancies10,11. Biomarkers of inflammation, coagulation, immune activation, and endothelial activation have been associated with cross-sectional lung function, but cross-sectional analyses are limited by the possibility of reverse causality, where a pulmonary process leads to an increase in biomarkers, whereas longitudinal analyses have the potential to predict lung function decline, and identify etiologic pathways12,13,14,15,16,17,18,19,20,21,22. Reliable predictors of lung function decline have been elusive, but higher blood concentrations of the pneumoprotein club cell secretory protein (CCSP) may be associated with slower decline in FEV1 in people with COPD and in the general non-HIV population23,24. The pneumoprotein surfactant protein D (SPD) has not been associated with longitudinal lung function in non-HIV COPD, but blocks HIV entry into target cells, is involved in innate immunity, and is reduced with initiation of antiretroviral therapy (ART); thus it may have a unique role in HIV-related lung disease24,25,26. The association of CCSP or SPD with longitudinal lung function decline in PWH has not been evaluated.
We sought to test the ability of the pneumoproteins SPD and CCSP, biomarkers of inflammation [C-reactive protein (CRP) and interleukin-6 (IL6)], and biomarkers of coagulation (d-dimer and fibrinogen) to predict lung function decline, both among PWH with effective viral suppression and those with untreated HIV.
Methods
We conducted this study using data and stored plasma samples collected in the Strategic Timing of Antiretroviral Treatment (START) Pulmonary Substudy27.
Parent cohort description
The design, methods, participant characteristics, and primary results of the parent START trial and its Pulmonary Substudy have been previously published27,28,29,30. Briefly, START enrolled HIV-positive, ART-naïve adults > 18 years of age with CD4 + T-cell counts > 500 cells/mm3 and then randomized participants to either immediate initiation of ART or deferred initiation until the CD4 + count declined to 350 cells/mm3 or AIDS developed. Participants were seen at study centers every 4 months, at which time fasting plasma was also collected for future analyses in those who provided informed consent for sample storage. Of 4685 participants enrolled in the parent START trial (from 215 sites in 35 countries), we co-enrolled 1026 participants (from 80 sites in 20 countries) into the START Pulmonary Substudy prior to randomization. In addition to the entry criteria for the parent START trial, additional Pulmonary Substudy criteria included the requirement that participants be ≥ 25 years old and free of factors affecting validity or safety of post-bronchodilator spirometry testing (e.g. respiratory illness within six weeks; surgery of the chest, abdomen, or eyes within three months; allergy to albuterol/salbutamol; unstable cardiac condition).
All START Pulmonary Substudy participants and START parent study participants provided informed consent specific to their study participation, all site institutional review boards/ethics committees approved the substudy, and we registered the substudy at ClinicalTrials.gov [NCT01797367 (2/22/2013) and NCT00867048 (2/23/2009)]. This study was performed in accordance with the relevant guidelines and regulations/ethical principles of the Declaration of Helsinki.
Spirometry methods and outcomes
Study participants performed post-bronchodilator spirometry at baseline prior to randomization and annually during follow-up. Spirometry was performed using the EasyOne ultrasonic flow device (ndd Medical, Zurich, Switzerland) following inhalation of 180 mcg of albuterol/salbutamol via a metered dose inhaler. Author KMK centrally reviewed all spirometry tests for quality control. Repeat testing was requested when tests failed to meet published quality standards31. We used Global Lung Function Initiative (GLI) 2012 normative equations to determine predicted FEV1 and the lower limit of normal (fifth percentile) of the FEV1/FVC ratio32. FEV1 slope was determined using repeated measures mixed models in the original analysis and in this analysis27.
Study design
We designed this analysis as a matched case:control study based upon rate of FEV1 decline. FEV1 decreases with age, but faster decline in FEV1 is a marker of COPD susceptibility and increased mortality33,34,35. Cases were defined as participants with rapid lung function decline, defined as an FEV1 slope of faster than − 40 mL/year. Though there is no consensus definition of rapid lung function decline, a rate of decline in FEV1 greater than 40 mL/year is commonly used24,33,35. Controls were defined as participants with stable lung function decline, defined as an FEV1 slope between − 20 and + 20 mL/year. We sought to test biomarkers of rapid lung function decline in two distinct groups of PWH: (1) those on ART with effective viral suppression and (2) those with untreated HIV. Therefore case:control identification was carried out in two distinct groups.
In the first group of case:control identification, we searched for matched case:control pairs among a virally suppressed group. In START, all participants were naïve to ART at study entry, so viral suppression could only be achieved at follow-up visits. Elite controllers, defined as having entered the study with HIV-RNA < 200 copies/mL despite lack of any previous ART exposure were excluded from this analysis. Participants could enter the viral suppression group if the met the following four criteria: (1) a minimum of 6 months with HIV-RNA < 200 copies/mL while on ART, (2) no subsequent HIV-RNA levels ≥ 200 copies/mL, (3) at least three high-quality annual FEV1 measurements beginning after at least 6 months of HIV-RNA < 200 copies/mL and (4) a corresponding plasma sample was available in the repository within ± 6 months of the first high-quality spirometry measure (and after the required 6 months with HIV-RNA level < 200 copies/mL). We allowed those in either arm of START (immediate or deferred ART initiation) to enter this analysis if they met these criteria, to better reflect clinical practice and allow a mix of CD4 + T-cell counts at the time of the plasma sample. This overall selection criteria allowed us to evaluate the relationship between biomarker concentrations and subsequent lung function decline in PWH who have successfully achieved viral suppression. We matched cases and controls (1:1 ratio) on sex and assigned randomization arm (immediate vs. deferred ART initiation), along with age (± 10 years), smoking status, and lung function (± 15% of predicted FEV1) at the first lung function test used in the analysis.
For the second case:control group, we searched for matched case:control pairs among an untreated HIV group. In START, since approximately half of participants were randomized to begin ART immediately after randomization, the untreated HIV group was restricted to those randomized to the deferred ART strategy. Participants could enter the untreated HIV group if they had three or more high-quality annual FEV1 measurements, no current or previous ART exposure at the time of those measurements, and a plasma sample available in the repository within ± 6 months of the first high-quality spirometry measurement. We also excluded elite controllers from this untreated HIV group. Due to the smaller pool of eligible participants in this untreated HIV analysis, we matched (1:1 ratio) on only age (± 10 years), smoking status, and lung function (± 15% of predicted FEV1) at the first lung function test used in the analysis.
Biomarker measurements
Samples were collected at baseline and all follow up visits (1 month, 4 months, and every 4 months thereafter) and stored in a central laboratory at – 70 °C. Assays were performed using commercially available ELISA kits (Abcam, Cambridge, UK), with antibody kit numbers listed as [abxxxxxx] below. Participant samples were randomly assigned to individual masterplates and all ELISA assays were performed in duplicate with values below the limit of detection assigned the lower limit of detection value.
Our primary focus was to test the ability of the plasma pneumoproteins CCSP [ab238266] and SPD [ab239431] to identify risk of rapid lung function decline among PWH. We also investigated biomarkers with previously published data from PWH suggesting their potential to predict pulmonary outcomes in HIV-positive persons. These included the marker of Th1 inflammation interleukin-6 (IL-6 [ab178013]), the general systemic inflammatory response marker high-sensitivity C-reactive protein (hsCRP [ab181416]) and markers of activated coagulation (fibrinogen [ab208036] and d-dimer [ab196269]).
Statistical analysis
We created histograms for each protein to assess skewness, and data were log transformed to improve normality if indicated. Pairwise concordance of replicate samples was assessed via Pearson’s correlation coefficient, and the log replicates were then averaged as the primary outcome variable in our models.
In our primary analyses we used standard linear models and linear mixed effects models to test whether case:control status and treatment status (virally suppressed vs untreated HIV) had a significant effect on the measured protein concentrations. We used these methods, rather than logistic regression, because one of our primary goals was to separately test associations in well controlled HIV and untreated HIV. Since matching was performed separately in each treatment group, there would be no association between treatment group and case:control status in logistic regression models. Logistic regression would also not have allowed us to test for an interaction between case:control status and treatment group on the levels of each biomarker. We hypothesized that the association between case:control status and biomarker concentrations may differ in the virally suppressed and untreated HIV groups, so we included an interaction term between case:control and treatment status (case:control × treatment status). We were unable to match for sex in the untreated HIV group, so sex was a covariate in those analyses. We also considered including a random effect for each matched pair, and a random intercept for the masterplate. We used the Akaike information criteria (AIC) to compare models of different complexity36. If the AICs for two models were within 2 units of each other, we selected the simpler model. We reported the significance of case:control status, treatment group, and their interaction on biomarker levels using Type I sums of squares based on the model selected using the AIC.
In secondary analyses we used paired t-tests to test whether log transformed biomarker concentrations varied by case:control status and treatment group. This was chosen as a secondary analysis as this method is straightforward but does not allow us to control for masterplate or sex, and additionally does not account for treatment group. We further used two-sample t-tests to test whether log-transformed biomarker concentrations varied by case:control status.
All statistical analyses were conducted using R version 3.6.1.
Ethics declarations
The INSIGHT Network used the University of Minnesota Institutional Review Board (ID number: 0603M83587) for the START parent study and START Pulmonary Substudy. The START Pulmonary substudy was also approved by the institutional review board/ethics committee at each site.
Study drugs
Antiretroviral drugs were donated to the central drug repository by AbbVie, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline/ViiV Healthcare, Janssen Scientific Affairs, and Merck.
Results
Participants and matching
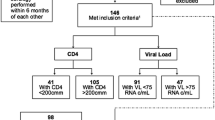
Of 1026 participants in the START Pulmonary Subsudy, we identified 77 eligible matched case:control pairs (n = 144 total) amongst the viral suppression group. We identified 43 matched pairs in the untreated HIV group, but at the time of biomarker measurement one serum sample was missing, and that case:control pair was excluded, leaving 42 matched pairs (n = 84 total) in the untreated HIV group (see Fig. 1 for STROBE figure). The most common reasons for exclusion were intermediate lung function decline (neither rapid nor stable, so neither meeting case or control criteria) and lacking three or more annual high-quality spirometry tests under the same treatment conditions (virally suppressed or untreated).

STROBE participant selection figure.
Characteristics of the cases and matched controls are shown in Table 1 for both the virally suppressed and untreated HIV groups. Median age was similar in cases and controls, across both groups. In the untreated HIV group, there were more female, and fewer Black participants among controls than among cases. Very few participants (n = 4 total) likely acquired HIV through injection drug use. As expected, CD4 + T cell counts at the first FEV1 measurement used were lower in the untreated HIV group than the virally suppressed group, but were similar in cases and matched controls in both groups. Median lung function, as measured by FEV1 percent predicted at the time of first included FEV1 measurement, was normal. There were minimal differences in lung function, HIV lab values, or timing of biomarker measurement between cases and matched controls in the viral suppression group, or the untreated HIV group (Supplementary Table S1). Longitudinal lung function decline in cases and matched controls for both groups is shown in Table 2. FEV1 decline was much faster in cases (− 86 and − 105 mL/year in virally suppressed and untreated, respectively) than controls (− 3 and − 5 mL/year in virally suppressed and untreated, respectively).
Biomarkers
The correlation between experimental replicates was greater than 0.8 for all biomarkers considered. Histograms of the averaged biomarker replicates before and after log transformation are included in the online supplement (Supplementary Fig. S2).
Associations between case:control status, treatment group, and biomarker concentrations
Results for our primary analysis, testing whether case:control status, treatment group (viral suppression vs untreated HIV), and their interaction affected biomarker concentrations, are shown in Table 3. Case:control status did not have a significant relationship with any of the six biomarkers. Treatment group had a significant relationship with d-dimer concentrations (F-value 6.49; p-value 0.01), but not other biomarkers. We also found a significant interaction between case:control status and treatment group on d-dimer concentrations (interaction p = 0.03), indicating that the association between case:control status and d-dimer concentrations varies by treatment group. However, the individual strata p-values were not statistically significant in either the virally suppressed (p = 0.49) or the untreated strata (p = 0.09).
In secondary analyses comparing biomarker concentrations by t-testing rather than linear models, we found no significant difference in biomarker concentrations between cases and controls (Fig. 2). When comparing the untreated HIV and virally suppressed groups, both d-dimer concentrations [mean (95% CI) for difference in log (pg/mL) − 0.47 (− 0.76 to − 0.18)] and IL-6 concentrations [− 0.41 (− 0.75 to − 0.08)] were lower in the virally suppressed group (Supplementary Fig. S3).

Comparison of log transformed biomarker concentrations by case:control status, where cases represent those with rapid lung function decline (FEV1 decline faster than 40 mL/year) and controls represent those with stable lung function (FEV1 change between − 20 and 20 mL/year). Values across the top represent the mean (95% confidence interval) of the differences in biomarker levels within each case control pair and p-values are from paired t-tests.
Discussion
We found no difference in plasma concentrations of pneumoproteins or biomarkers of inflammation and coagulation among PWH with rapid lung function decline compared to PWH with stable lung over a median of 3 years of follow up. Findings were consistent for both untreated HIV and virally suppressed groups.
The use of samples and data from the START Pulmonary Substudy uniquely allowed us to investigate associations between biomarkers and longitudinal lung function in two well characterized groups of PWH, with either untreated HIV or viral suppression. Based in large part on findings from the parent START trial, current recommendations are to immediately begin treatment for HIV at the time of diagnosis, but studying the untreated HIV group may still have relevance to persons who present late in the course of HIV infection or face barriers to accessing ART. The virally suppressed group represents current optimal care, with early ART initiation at high CD4 + T-cell counts. Findings among virally suppressed PWH have the potential to identify those most at risk for future lung disease and to reveal pathways important in HIV lung disease pathogenesis in the modern era of more widely available HIV testing and immediate treatment.
One of our primary goals was to evaluate the association between blood pneumoprotein concentrations and longitudinal lung function in PWH. Blood biomarkers of lung function decline have been elusive37. We measured two of the most well characterized blood pneumoproteins: (1) SPD, which is produced by type II alveolar cells, involved in innate immunity, and may have a unique role in HIV; and (2) CCSP, which is formed in the bronchioles, and is the only pneumoprotein that has shown a relationship with longitudinal lung function decline in multiple large studies24,26,38,39,40. Though lower CCSP concentrations may be predictive of faster lung function decline, these associations have been quite weak, even in large studies (r2 = 0.0043 for the relationship between log transformed CCSP concentrations and FEV1 decline in 4724 participants in the Lung Health Study, and a 1 SD decrease associated with a 4 ± 2.1 mL/year faster FEV1 decline in 2163 participants in ECLIPSE)24,39. We were likely underpowered to find a significant relationship between CCSP and rapid lung function decline. We also studied a cohort of PWH without established lung disease as opposed to these previous studies in non-HIV COPD, which included participants with at least moderate expiratory airflow obstruction. Though blood pneumoproteins are appealing because they can be collected rather simply, they cannot directly measure what is happening at the level of the lung tissue. Direct measurements of pneumoproteins from lung tissue or bronchoalveolar lavage may be more revealing, but these samples would require more invasive methods.
There are few previous analyses of blood pneumoproteins and lung function in PWH, and we are aware of no previous analyses of pneumoproteins and longitudinal lung function in PWH. In a cross-sectional analysis of PWH (n = 65) Jeon and colleagues found significant associations between higher CCSP and lower FVC, and higher CCSP and lower diffusing capacity for carbon monoxide (DLCO)41. Those findings were in contrast to general COPD as discussed above, where higher CCSP has been associated with better cross-sectional lung function and slower longitudinal lung function decline24. Analysis of CCSP in larger cohorts of PWH would help to clarify these associations and how they compare to non-HIV COPD, though the general population data suggest that CCSP may be a relatively weak marker of obstructive lung disease risk. Similar to our findings, Jeon et al. found no significant associations between SPD and lung function in PWH41.
We also found that treatment status (viral suppression or untreated HIV) had no effect on SPD or CCSP. These findings are consistent with Shiels and colleagues who found no significant differences in SPD concentrations between those on ART and not on ART42. We previously reported that SPD decreased after initiation of ART, but that was a small study (n = 15) in persons with more advanced HIV (median CD4 + cell count 320 cells/mm3), and the pathways leading to changes in SPD and lung function may be different in more advanced HIV43. Jambo and colleagues analyzed SPD concentrations in bronchoalveolar lavage (BAL) fluid from PWH and HIV negative participants. They found that BAL SPD concentrations were similar in HIV negative participants and PWH with CD4 + counts > 200, but SPD concentrations were greater in those with CD4 + counts < 20044. These data suggest that SPD may be more important in PWH with lower CD4 + counts, and though we analyzed a group of PWH with untreated HIV, very few participants reached CD4 + counts as low as these previous studies because ART was initiated at a CD4 + count of 350 cells/mm3, and the study was terminated early at which time all participants were offered ART28.
We did not find a significant association between longitudinal lung function decline and biomarkers of inflammation and coagulation. There are few previous studies of these associations. Our findings are consistent with Gupte and colleagues who found that CRP had no association with longitudinal lung function in 619 South African PWH15. Our findings are also consistent with Fitzpatrick and colleagues who found that IL-6 was not associated with longitudinal lung function (n = 124 PWH in the Lung HIV study)14. Verboeket and colleagues recently found that higher hsCRP and lower IL-6 were associated with faster decline in FEV1, but as they discussed, these relationships may have been confounded by smoking (which is known to increase inflammatory markers and decrease lung function), and when they analyzed these relationships among non-smokers, they were no longer significant22. Lastly, in a previous analysis of the START Pulmonary Substudy utilizing biomarkers measured at the time of study entry (i.e. when all participants were ART naïve, but some were subsequently immediately initiated on ART), we found cross-sectional associations between biomarkers of inflammation and coagulation, but no associations with subsequent longitudinal lung function decline18. We are aware of no other data on the association between biomarkers of inflammation and coagulation and longitudinal lung function in PWH.
Biomarkers of inflammation and coagulation have been associated with cross-sectional lung function measures in previous studies of PWH. For example, in the study of 124 PWH in the Lung HIV study mentioned previously, higher IL-6 was associated with lower baseline FEV1% predicted and DLCO % predicted, but not with longitudinal changes in either measure14. In a cross-sectional analysis of 147 HIV-positive individuals by the same authors, CRP and IL6 were associated with lower FEV1% predicted13. Cross-sectional analyses have not shown a relationship between fibrinogen and FEV1 in PWH, but higher fibrinogen may be associated with small airway dysfunction in PWH16,18,20 In our previous analysis of the START Pulmonary Substudy we found that IL-6, hsCRP, serum amyloid A (another inflammatory marker), and the IL-6/d-dimer score were associated with cross-sectional FEV1, but none associated with subsequent longitudinal lung function decline18. In sum, these data suggest reverse causality, where a pulmonary process leads to worse lung function, inflammation, and coagulation, as opposed to inflammation or dysregulated coagulation driving worsening lung function.
Though not the primary focus of this analysis, we also tested the effect of treatment group (virally suppressed vs untreated HIV) on biomarkers of inflammation and coagulation. In our primary analysis we found that d-dimer was lower among virally suppressed participants than among participants with untreated HIV; in secondary analysis, we found that both IL-6 and d-dimer concentrations were lower in virally suppressed participants than those with untreated HIV. This is consistent with a previous analysis in the Strategies for Management of Antiretroviral Therapy (SMART) trial where a randomized comparison of patients who received immediate ART showed a decrease in d-dimer and trend toward a decrease in IL-6, compared to participants who received deferred ART45. This is also consistent with a previous analysis of the parent START trial, in which participants assigned to immediate ART had significant reductions in d-dimer and IL-6 over 8 months compared to those assigned to deferred ART. There was no significant difference in change in hsCRP46.
Our study has several limitations. First, we did not measure other pneumoproteins, such as prosurfactant protein B, which have shown variation by HIV status and CD4 + counts42. We also did not measure markers of endothelial function, such as endothelin-1 which has been associated with longitudinal decline in FEV1 and DLCO, and macrophage activation, such as soluble CD163 which have been associated with longitudinal DLCO decline (n = 70 PWH) 14]. Second, we did not have measures of diffusing capacity, which are the most frequently abnormal measure of lung function in PWH43. Third, we had a modest sample size which limited power to detect small effect sizes, particularly in the context of analyzing pneumoproteins which have shown very small effect sizes in non-HIV cohorts24,39. Fourth, we do not have bronchoalveolar lavage or other respiratory samples in the START Pulmonary Substudy, and findings in respiratory samples are not always reflected in plasma47. Lastly, we studied a cohort of generally young, recently diagnosed PWH with high CD4 + counts at relatively low risk of lung disease. Though this is a limitation, we feel it is also a strength, as this represents optimal care and should represent an increasing proportion of PWH in coming years. Though these participants were at a low risk of lung disease, the use of a matched case:control design allowed us to compare participants with rapid lung function decline (median FEV1 decline of 86 to 105 mL/year depending on group) to participants with stable lung function (median FEV1 decline 3 to 5 mL/year), and all participants had at least 3 high quality spirometry measures. This case:control design and large difference in lung function decline also maximized power given our modest sample size. Future work in our cohort will use untargeted metabolomic profiling methods to identify other potential biomarkers and pathways that might explain why these persons with early HIV experience such rapid lung function decline, independent of cigarette smoking.
Our study has several additional strengths. Our international, multi-center, clinical trial cohort is uniquely representative of the global HIV epidemic. FEV1 decline was the carefully standardized and quality controlled primary outcome of the substudy, thus providing high quality measures of lung function. We also utilized the randomization to immediate versus deferred ART to analyze associations in those with virally suppressed HIV and untreated HIV. Finally, this is the first study to analyze the association of pneumoproteins with longitudinal lung function decline among PWH.
In conclusion, we did not find an association between longitudinal FEV1 decline and blood concentrations of pneumoproteins or biomarkers of inflammation and coagulation in PWH. Future studies should explore other pathways and consider non-spirometry outcomes such as DLCO.
Data availability
Requests for data can be submitted to the START Scientific Steering Committee upon completion of START. The Research Proposal form can be found here: http://insight.ccbr.umn.edu/research_proposal/.
References
GBD 2017 Causes of Death Collaborators. Global, regional, and national age-sex specific mortality for 282 cuases of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 392, 1736–1788 (2018).
Bigna, J. J., Kenne, A. M., Asangbeh, S. L. & Sibetcheu, A. T. Prevalence of chronic obstructive pulmonary disease in the global population with HIV: A systematic review and meta-analysis. Lancet GlobHealth 6, e193-202 (2018).
Makinson, A. et al. HIV is associated with airway obstruction: A matched controlled study. AIDS 32(2), 227–232 (2018).
Gingo, M. R. et al. Decreased lung function and all-cause mortality in HIV-infected individuals. Ann. ATS 15(2), 192–199 (2018).
Tripplette, M. et al. Markers of chronic obstructive pulmonary disease are associated with mortality in people living with HIV. AIDS 32(4), 487–493 (2018).
Drummond, M. B. et al. The effect of HIV infection on longitudinal lung function decline among injection drug users: A prospective cohort. AIDS 27(8), 1303–1311 (2013).
Drummond, M. B. et al. Association between obstructive lung disease and markers of HIV infection in a high-risk cohort. Thorax 67, 309–314 (2012).
MacDonald, D. M. et al. Smoking and accelerated lung function decline in HIV-positive individuals: A secondary analysis of the START Pulmonary Substudy. JAIDS 79(3), e85–e92 (2018).
Risso, K. et al. COPD in HIV-infected patients: CD4 cell count highly correlated. PLoS One 12(1), e0169359 (2017).
Grund, B. et al. Relevance of interleukin-6 and d-dimer for serious non-AIDS morbidity and death among HIV-positive adults on suppressive antiretroviral therapy. PLoS One 11(5), e0155100 (2016).
Kuller, L. H. et al. Inflammatory and coagulation biomarkers and mortality in patients with HIV infection. PLoS Med. 5(10), e203 (2008).
Attia, E. F. et al. Increased risk of radiographic emphysema in HIV is associated with elevated soluble CD14 and nadir CD4. Chest 146(6), 1543–1553 (2014).
Fitzpatrick, M. E. et al. Relationships of pulmonary function, inflammation, and T-cell activation and senescence in an HIV-infected cohort. AIDS 28(2), 2505–2515 (2014).
Fitzpatrick, M. E. et al. Novel relationships of markers of monocyte activation and endothelial dysfunction with pulmonary dysfunction in HIV-infected persons. AIDS 30(9), 1327–1339 (2016).
Gupte, A. N. et al. Factors associated with pulmonary impairment in HIV-infected South African Adults. PLoS ONE 12(9), e0184530 (2017).
Kan, A. K., Moore, J. V., Wang, R. J., McGing, M., Farr, C. K., et al. Markers of inflammation and immune activation are associated with lung function in a multicenter cohort of persons with HIV. AIDS. (2021) https://doi.org/10.1097/QAD.0000000000002846 (in press).
Kuniholm, M. H. et al. Association of monocyte migration marker CD11b with pulmonary function in people living with HIV. JAIDS 86(3), 344–352 (2021).
MacDonald, D. M. et al. Associations between baseline biomarkers and lung function in HIV-positive individuals. AIDS 33(4), 655–665 (2019).
North, C. M. et al. Systemic inflammation, immune activation and impaired lung function among people living with HIV in rural Uganda. JAIDS 78(5), 543–548 (2018).
Ronit, A. et al. Small airway dysfunction in well-treated never-smoking HIV-infected individuals. Eur. Resp. J. 49, 1602186 (2017).
Thudium, R. F. et al. Independent association of interleukin 6 iwith low dynamic lung function and airflow limitation in well treated people with human immunodeficiency virus. JID https://doi.org/10.1093/infdis/jiaa600 (2021) (in press).
Verboeket, S. O. et al. Changes in lung function among treated HIV-positive and HIV-negative individuals: Analysis of the prospective AGEhIV cohort study. Lancet Healthy Longev. 2, e202-211 (2021).
Guerra, S. et al. The relation of circulating CC16 to lung function growth, decline, and development of COPD across the lifespan. Lancet Respir. Med. 3(8), 613–620 (2015).
Vestbo, J. et al. Changes in forced expiratory volume in 1 second over time in COPD. NEJM 365(13), 1184–1192 (2011).
Kunisaki, K. M., Quick, H. & Baker, J. V. HIV antiretroviral therapy reduces circulating surfactant protein-D levels. HIV Med. 12(9), 580–581 (2011).
Pandit, H. et al. Surfactant protein D inhibits HIV-1 infection of target cells via interference with gp-120-CD4 interaction and modulates pro-inflammatory cytokine production. PLoS One 9(7), e102395 (2014).
Kunisaki, K. M. et al. Pulmonary effects of immediate versus deferred antiretroviral therapy in HIV-positive individuals: A nested substudy within the multicenter, international, randomized, controlled Strategic Timing of Antiretroviral Treatment (START) trial. Lancet Respir. Med. 4, 980–989 (2016).
The INSIGHT START Study Group. Initiation of antiviral therapy in early asymptomatic HIV infection. NEJM 373(9), 795–807 (2015).
Kunisaki, K. M. et al. Lung function decline in early HIV infection: Impact of antiretroviral drug timing and drug regimen. Am. J. Respir. Crit. Care Med. 201(6), 739–741 (2020).
Kunisaki, K. M. et al. Pulmonary function in an international sample of HIV-positive, treatment-naïve adults with CD4 counts > 500 cells/uL: A substudy of the INSIGHT Strategic Timing of AntiRetroviral Treatment trial. HIV Med. 16(S1), 119–128 (2015).
Standardization of Spirometry, 1994 Update. American Thoracic Society. Am. J. Respir. Crit. Care Med. 152, 1107–1136 (1995).
Quanjer, P. H. et al. Mult-ethnic reference values for spirometry for the 3–95-year age range: The global lung function 2012 equations. Eur. Respir. J. 40(6), 1324–1343 (2012).
Lange, P. et al. Lung-function trajectories leading to chronic obstructive pulmonary disease. NEJM 373(2), 111–122 (2015).
Mannino, D. M., Reichert, M. M. & Davis, K. J. Lung function decline and outcomes in an adult population. AJRCCM 173, 985–990 (2006).
Petersen, H. et al. Rapid lung function decline in smokers is a risk factor for COPD and is attenuated by angiotensin-converting enzyme inhibitor use. Chest 145(4), 695–703 (2014).
Akaike, H. A new look at the statistical model identification. IEEE Trans. Autom. Control 19(6), 716–723 (1974).
Stockley, R. A., Halpin, D. M. G., Celli, B. R. & Singh, D. Chronic obstructive pulmonary disease biomarkers and their interpretation. Am. J. Respir. Crit. Care Med. 199, 1195–1204 (2019).
Lomas, D. A. et al. Evaluation of serum CC-16 as a biomarker for COPD in the ECLIPSE cohort. Thorax 63, 1058–1063 (2008).
Park, H. Y. et al. Club cell protein 16 and disease progression in chronic obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 188, 1413–1419 (2013).
Pastva, A. M., Wright, J. R. & Williams, K. L. Immunomodulatory roles of surfactant proteins A and D: Implications in lung disease. Proc. Am. Thorac. Soc. 4, 252–257 (2007).
Jeon, D. et al. Pneumoproteins are associated with pulmonary function in HIV-infected persons. PLoS ONE 14(10), e0223263 (2019).
Shiels, M. S. et al. HIV infection and circulating levels of prosurfactant protein B and surfactant protein D. JID 217, 413–417 (2018).
Kunisaki, K. M. et al. Lung function in men with and without HIV. AIDS 34(8), 1227–1235 (2020).
Jambo, K. C., French, N., Zijlstra, E. & Gordon, S. B. AIDS patients have increased surfactant protein D but normal mannose binding lectin levels in lung fluid. Respir. Res. 8, 42 (2007).
Baker, J. V. et al. Changes in inflammatory and coagulation biomarkers: A randomized comparison of immediate versus deferred antiretroviral therapy in patients with HIV infection. JAIDS 56(1), 36–43 (2011).
Baker, J. V. et al. Systemic inflammation, coagulation, and clinical risk in the START trial. Open Forum Infect. Dis. 4(4), 262 (2017).
Wendt, C. H. et al. Lung and plasma metabolome in HIV-associated obstructive lung disease. JAIDS 91(3), 312–318 (2022).
Acknowledgements
The study thanks all START Pulmonary Substudy participants for their contributions to our scientific understanding of lung disease in HIV infection. A full listing of START Pulmonary Substudy team members is included in the online supplement (S4) and a full listing of the parent START study team members can be found in the primary START results publication28. We would also like to thank Alan Mickelson for his technical assistance. Disclaimer: The views expressed in this article are those of the authors and do not reflect the views of the United States Government, the National Institutes of Health, the Department of Veterans Affairs, the funders, the sponsors, or any of the authors’ affiliated academic institutions.
Funding
The START Pulmonary Substudy reported here was supported by the National Heart Lung and Blood Institute (R01 HL096453); the parent START trial was primarily supported by the National Institute of Allergy and Infectious Diseases Division of AIDS (UM1 AI068641 and UM AI120197) with additional support from the German Ministry of Education and Research, the European AIDS Treatment Network (NEAT), the Australian National Health and Medical Research Council, and the UK Medical Research Council and National Institute for Health Research. DMM was supported by NHLBI T32 HL007741 during the conduct of this work. The Veterans Health Administration Office of Research and Development also provided protected research time in support of this study. CHW, EFL, and SS were supported by NHLBI R01 HL140971-01A1. The University of Minnesota served as sponsor of the study. None of the funders nor sponsor had any input regarding the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication. This material is also the result of work supported with resources and the use of facilities at the Minneapolis Veterans Affairs Medical Center, Minneapolis/USA.
Author information
Authors and Affiliations
Consortia
Contributions
Conceived the study: K.M.K. Designed the study: K.M.K., J.V.B., C.H.W. Obtained funding: K.M.K. Acquired the data: S.P., A.W., R.W., C.H.W. Performed the primary statistical analyses: G.C., S.S., E.L. Drafted the manuscript: K.M.K. and D.M.M. Critically revised the manuscript for important intellectual content and approved the final manuscript: all authors. Take responsibility for the integrity of the data and the accuracy of the data analysis: all authors.
Corresponding author
Ethics declarations
Competing interests
KMK reports personal fees from Nuvaira (Independent Data and Safety Monitoring Board; current) and Allergan (consulting; past). RPD reports research grants (awarded to his institution) from ViiV, Gilead and MSD, and participating in advisory commitees from Gilead, ViiV, MSD, Lilly and Theratechnologies. The remaining authors have nothing to declare.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
MacDonald, D.M., Samorodnitsky, S., Wendt, C.H. et al. Pneumoproteins and biomarkers of inflammation and coagulation do not predict rapid lung function decline in people living with HIV. Sci Rep 13, 4749 (2023). https://doi.org/10.1038/s41598-023-29739-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-29739-x
- Springer Nature Limited