
Abstract
Limited data are available on the association of legumes and nuts consumption with health status in pediatrics. So, we assessed the relation of legumes and nuts intake with metabolic health status in Iranian adolescents. A random sample of overweight/obese adolescents aged 12 to 18 years was included in this cross-sectional study. Dietary intakes were gathered using a validated 147-item food frequency questionnaire (FFQ). We measured metabolic indices including blood pressure, lipid profile, glycemic and anthropometrics indices. Two strategies were used for classification of adolescents to metabolically healthy obese (MHO) or unhealthy obese (MUO): International Diabetes Federation (IDF) and combination of IDF with Homeostasis Model Assessment Insulin Resistance (HOMA-IR). Information on 203 overweight/obese adolescents (50.2% girls and 49.8% boys) with an average age of 13.98 (± 1.61) years and a mean weight of 73.48 (± 11.60) kg/m2 was evaluated. Based on the IDF and IDF/HOMA-IR definition, higher consumption of legumes and nuts consumption was related to a 66% and 61% decreased odds of MUO in crude model (OR = 0.34, 95%CI 0.17–0.69), (OR = 0.39, 95%CI 0.19–0.80); but in fully-adjusted model, these relations disappeared. After adjustment for potential cofounders, an inverse association was found between legumes and nuts consumption and odds of hyperglycemia (OR = 0.35, 95%CI 0.16–0.78). Moreover, although inverse significant associations were found between legumes and nuts consumption and odds of MUO in girls and overweight subjects in crude models, these associations disappeared after adjustment for all confounders. After taking potential confounders into account, no significant association was found between consumption of legumes and nuts and MUO in Iranian adolescents. The findings should be affirmed by further prospective studies.
Similar content being viewed by others

Introduction
Overweight and obesity prevalence have increased significantly over the past four decades1. Based on the Global Burden of Disease (GBD) data, the overweight prevalence in children and obesity in adolescents will be increased to 268 and 124 million by 2025, in the world1. It was estimated that 4 million adolescents with excess weight will live in Iran by 20252. Obesity in childhood has an increased burden on healthcare systems3, because it is related to complications like insulin resistance, dyslipidemia, impaired glucose metabolism, high blood pressure (BP), and some cancers4,5,6. Previous evidences documented that children with obesity may still be obese in adulthood4 and had an increased risk of cardiac events7 and all-cause mortality in adulthood8. Individuals with obesity have one of two phenotypes of metabolically healthy overweight/obese (MHO) or metabolically unhealthy overweight/obese (MUO)6,9. MHO is a dynamic state before MUO and MUO is a progressive state6,10. Overweight/obese subjects with at least 2 metabolic disorders (including, hyperglycemia, hypertension, dyslipidemia (low serum HDL-c and/or hypertriglyceridemia), and insulin resistance) are classified as MUO. On the other hand, overweight/obese subjects with less than 2 above-mentioned disorders are defined as MHO11,12.
Several risk factors are involved in the etiology of MUO such as age, genetic predispositions, lifestyle factors and their interactions10,13. A healthy diet has a beneficial effect on metabolic profile10; such that, a higher Dietary Approaches to Stop Hypertension (DASH) score was adversely related to MUO odds in obese children9. Additionally, adherence to a Mediterranean-style diet improved glucose, body mass index (BMI), total cholesterol (TC), triglycerides (TG), high density lipoprotein cholesterol (HDL-c), and low density lipoprotein cholesterol (LDL-c), in Mexican obese children and adolescents14. Furthermore, a cohort study indicated that nuts consumption decreased the values of TG, waist circumference, systolic blood pressure (SBP), BMI and weight15. Several legumes, such as soy, have functional properties that have favorable effects on cholesterol, TG, glucose metabolism, blood pressure and inflammation16. A systematic review and meta-analysis of prospective studies demonstrated that legumes consumption reduce the risk of overweight/obesity and weight gain17. To our knowledge, the association between food groups and MUO or MHO has less been studied, and most former studies were conducted in European and USA populations18. So, the current study was conducted to assess the relation of legumes and nuts consumption with metabolic health status in Iranian overweight/obese adolescents.
Methods and materials
Participants and study design
Overall 203 overweight/obese adolescents (101 boys and 102 girls) aged between 12 to 18 years were included in this cross-sectional study. Using a stratified, multi-stage cluster sampling method, subjects were selected from 16 schools of 5 different districts of Isfahan, Iran in 2020. By this method, students with different socio-economic statuses were considered for the study. Taking a prevalence of MUO in overweight and obese Iranian adolescents (60%)19,20, precision (d) of 7%, 0.95 confidence interval (CI), 0.05 type I error and 80% power into account, at least 188 subjects were required to be included in the current analysis. Only overweight and obese adolescents (based on growth curve age-sex specific BMI percentiles21) were selected for the study. We did not include subjects that followed a weight-loss diet or had an endocrine disorder or were taking supplements or medications that might influence their metabolic status. All subjects and their parents signed a written informed consent. The local Ethics Committee of Isfahan University of Medical Sciences confirmed the study protocol.
Assessment of dietary intake
Dietary intakes were gathered using a validated 147-item food frequency questionnaire (FFQ)22. Previous studies demonstrated that this FFQ could be a valid and reliable tool for assessing food and nutrient intake among Iranian adolescents23,24. To complete the FFQs, a trained dietitian asked the adolescents to report the frequency (based on daily, weekly, monthly) and quantity (based on common portion sizes) of their food intakes in the preceding year. By using household measures25, the portion size of food intake was converted to g/day. Finally, Nutritionist IV software was used to estimate the overall intake of energy and nutrients per day. Consumption of nuts was defined as intake of tree nuts (including almond, walnut, hazelnuts, peanuts, seeds, and pistachio) and consumption of legumes was defined as intake of beans, peas, lentil, split peas, mung beans and soy.
Assessments of anthropometric indices and cardiometabolic risk factors
A trained dietitian evaluated all anthropometric indices. Height of participants was assessed with a stadiometer (to the nearest 0.1 cm) without shoes and with relaxed shoulders. Weight was measured with a calibrated electronic scale (Seca Instruments, Germany) (to the nearest 100 g) with minimum clothes and without shoes. After that, BMI was computed based on the Quetelet formula (weight(kg))/height2) and individuals were categorized as obese (> 95th percentile), overweight (85–95th percentile) and normal (< 85th percentile) based on the sex, and age-specific World Health Organization (WHO) cut-off points for adolescents21. Only overweight and obese adolescents were selected for the study. The measurement of SBP and diastolic blood pressure (DBP) was done through the use of a mercury sphygmomanometer with an appropriate cuff for blood pressure assessment in this age group; such that, the width of the cuff was approximately 40% of the arm circumference and the bladder cuff length covered approximately 80% of the arm circumference in adolescents26,27. The values of BP were recorded two times for each subject and the average of two measurements was considered as the final value.
Based on the standard protocol for biochemical values, blood collection was conducted in a sitting position and after a 12-h overnight fasting. Based on the enzymatic colorimetric method, fasting blood glucose (FBG) was measured using the glucose oxidase enzyme. After precipitation of the apolipoprotein B-containing lipoproteins, HDL-c values were assessed using phosphotungstic acid. Using the enzymatic colorimetric tests, TG values were measured by glycerol phosphate oxidase. Moreover, the values of serum insulin were assessed through the use of the ELISA kits. In order to estimate insulin resistance (IR), Homeostasis Model Assessment Insulin Resistance (HOMA-IR) was computed using the following formula28:
Assessment of metabolic status
Two strategies were applied to classify adolescents into MUO and MHO. According to the international diabetes federation (IDF) criteria11, overweight and obese individuals with two or more of these criteria were considered as MUO: increased TG (≥ 150 mg/dL), decreased HDL-c (< 40 mg/dL for the age of < 16 years, and < 50 mg/dL in female adolescents/ < 40 mg/dL in male adolescents for the age of ≥ 16 years), increased fasting blood glucose (≥ 100 mg/dL) and increased blood pressure (≥ 130/85 mmHg); individuals with less than two above-mentioned criteria were considered as MHO. The second strategy (IDF/HOMA-IR) was the combination of the first criteria (IDF) and HOMA-IR score as an indicator of insulin resistance12; such that, overweight/obese individuals with two or more above-mentioned metabolic disorders and insulin resistance (HOMA-IR score ≥ 3.16) were defined as MUO and individuals with HOMA-IR < 3.16 were defined as MHO. The cut-off point of 3.16 was determined based on previous studies on adolescents29,30.
Assessment of other variables
Using the valid Physical Activity Questionnaire for Adolescents (PAQ-A), physical activity was assessed. This questionnaire includes 9 items, the first 8 items are about usual physical activities and the last one is about unusual activities in the last week31. Each of the first 8 items has a 1–5 score; score 1 shows the lowest level of activity, and score 5 shows the highest level of activity. Scores were calculated and students were categorized as high active (score ≥ 3) and low active (score < 3). Information of age, sex, drug and supplement use history and other confounders were assessed using a valid demographic questionnaire. Using a validated questionnaire32, the socioeconomic status (SES) of adolescents was evaluated based on parental education, parental job, number of family members, having car in the family, having computer/laptop, having personal room and number of trips per year.
Statistical analysis
The normality distribution of quantitative variables was examined using the Kolmogorov–Smirnov test. The mean ± SD/SE and frequency (percentage) were reported for continuous variables and qualitative variables, respectively. Energy-adjusted values of legumes and nuts intake were provided by the use of the residual method. First, a linear regression between legumes and nuts consumption and total energy intake was calculated. Then, energy-adjusted values of legumes and nuts were computed by summing the mean consumption of legumes and nuts with the residual values obtained from the linear regression. Participants were categorized according to energy-adjusted tertiles of legumes and nuts consumption. Using the chi-square test and one-way analysis of variance (ANOVA), the categorical and continuous variables were reported across energy-adjusted tertiles of legumes and nuts consumption. If ANOVAs were significant, post hoc comparisons by Bonferroni correction were performed. Additionally, analysis of covariance (ANCOVA) was used to determine the energy, age, and sex-adjusted dietary intakes of subjects across energy-adjusted tertiles of legumes and nuts consumption. Using binary logistic regression test, we reported crude and multivariable-adjusted odds ratios (ORs) for MUO (based on IDF and IDF/HOMA-IR definitions) across energy-adjusted tertiles of legumes and nuts consumption. In the first model, adjustments were made for energy, sex and age. In the second model, we additionally made adjustments for physical activity and socioeconomic status. Finally, we added BMI to the adjustments, in the third model. The first category of legumes and nuts consumption was considered as the reference category in all models. In order to determine the trends, energy-adjusted tertiles of legumes and nuts consumption were treated as ordinal variables in logistic regression models. Additionally, we performed a stratified analysis based on BMI categories of participants and their sex. We conducted all analyses through the use of SPSS software version 20. We considered P-values < 0.05 as statistically significant.
Ethical approval and consent to participate
The study procedure was performed according to declaration of Helsinki and STROBE checklist. All subjects and their parents signed a written informed consent. The study protocol was approved by the local Ethics Committee of Isfahan University of Medical Sciences.
Results
In this study, information on 203 overweight/obese adolescents (50.2% girls and 49.8% boys) with an average age of 13.98 (± 1.61) years and a mean weight of 73.48 (± 11.60) kg was evaluated. General characteristics and cardiometabolic risk factors of study participants in energy-adjusted tertiles of legumes and nuts consumption are provided in Table 1. Adolescents in the third tertile in comparison to persons in the first tertile were younger. Moreover, participants in the second tertile had higher levels of HDL-c, compared to those in the lowest tertile.
Age, sex and energy intake-adjusted dietary intakes of the study population across tertiles of legumes and nuts consumption are presented in Table 2. Persons in the top category of legumes and nuts compared to the bottom category had a significantly higher intake of protein, monounsaturated fatty acids (MUFA), vitamin A, vitamin C, riboflavin, folate, vitamin B12, magnesium, zinc, and dietary fiber. However, these participants had a significantly lower intake of carbohydrate, thiamin, niacin and vitamin B6 intake, compared to individuals in the first tertile.
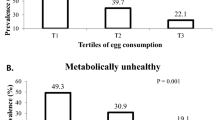
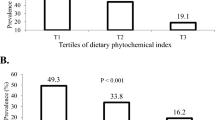
MUO prevalence based on IDF and IDF/HOMA-IR definitions in different energy-adjusted tertiles of legumes and nuts consumption is presented in Fig. 1. Participants in the highest tertile of legumes and nuts had lower prevalence of MUO based on both criteria.

Prevalence of MUO ((A) based on both IDF and (B) IDF/HOMA-IR definition) in energy-adjusted tertiles of legumes and nuts consumption.
Multivariate adjusted ORs and 95% CIs for MUO across energy-adjusted tertiles of legumes and nuts consumption are provided in Table 3. Based on IDF definition, in crude model, higher consumption of legumes and nuts was related to 66% decreased odds of MUO (OR = 0.34, 95% CI 0.17–0.69). After adjustment for potential confounders, the relation was not significant anymore (in fully-adjusted model: OR = 0.63, 95% CI 0.27–1.49). According to IDF/HOMA-IR definition, the same results were found; a 61% significant decrease in MUO odds was seen in crude model (OR = 0.39, 95% CI 0.19–0.80), but this relation was not significant in fully-adjusted model (OR = 0.69, 95% CI 0.28–1.70). Furthermore, in crude model, one tertile increment in legumes and nuts consumption was linearly related to 43% (OR = 0.57, 95% CI 0.40–0.82) and 39% (OR = 0.61, 95% CI 0.42–0.88) decreased odds of MUO, based on IDF and IDF/HOMA-IR definition, respectively. Again, these associations disappeared in fully adjusted model.
Multivariate adjusted odds ratio (OR) and 95% confidence interval (CI) for MUO components across energy-adjusted tertiles of legumes and nuts consumption are reported in Table 4. In crude model, higher legume and nut consumption was significantly related to lower odds of hyperglycemia (OR = 0.29, 95% CI 0.14–0.60), low HDL-c (OR = 0.46, 95% CI 0.23–0.93) and insulin resistance (OR = 0.20, 95% CI 0.09–0.47). After adjustment for potential cofounders, only an inverse significant association was found between legumes and nuts consumption and odds of hyperglycemia (OR = 0.35, 95% CI 0.16–0.78).
The relation between energy-adjusted legumes and nuts consumption with odds of MUO, stratified by BMI status of participants, are presented in Table 5. In overweight participants, although there was an inverse significant association between intakes of legumes and nuts and odds of MUO in the crude model, this association disappeared after adjustment for all confounders. In obese subjects, there was no significant association in crude or adjusted models, based on both definition criteria.
The associations between energy-adjusted legumes and nuts consumption with odds of MUO, stratified by sex of participants, are provided in Table 6. In girls, there was an inverse significant association between consumption of legumes and nuts and odds of MUO based on both criteria in the crude model. But after adjustment for physical activity, socioeconomic status and BMI, this relation was not significant. In boys, there was no significant association between legumes and nuts consumption and MUO, based on both definitions, in the crude or adjusted models.
Discussion
In this study, overweight/obese adolescents with higher legumes and nuts consumption compared to those with lower intake had lower odds of MUO based on IDF, IDF/HOMA-IR in the crude model and after considering main confounders in model 1. But after further adjustments for physical activity, socioeconomic status, and BMI, there was no significant association. Moreover, in girls and overweight participants, we found an inverse significant association, based on both definition criteria in crude model; however, these associations disappeared after considering all potential confounders. There was no significant association in boys or obese subjects, before or after taking potential confounders into account.
Regarding the increasing rate of childhood overweight and obesity, it must be considered that MHO is not a constant condition and children may be transferred from MHO to MUO, as they get older1,13. Considering the high morbidity and mortality due to childhood obesity33, it is worthy to prevent the incidence of these disorders and their consequences. In the current study, we illustrated that higher intakes of legumes and nuts might be related to decreased odds of MUO. Therefore, it could be clinically advised to adolescents to pay more attention to consumption of legumes and nuts for preventing MUO and its adverse effects.
Similar to the current study, some previous cross-sectional studies have examined the relationship between legumes and nuts consumption and metabolic risk factors in adolescents. Following a Mediterranean diet was related to a lower risk of MUO in European overweight or obese adolescents34. Mirmiran et al. have reported a non-significant decrease in metabolic syndrome (MetS) prevalence and its components across the quartiles of nuts and dried fruit consumption in adolescents. But they found a significant decreasing trend in TG concentration across quartiles of nuts and dried fruit consumption35. Moreover, Aghayan et al. illustrated an inverse association between nut consumption and risk of carotid intima-media thickness (cIMT) in overweight and obese pediatrics36. In addition, higher soy intake was inversely associated with the prevalence of hypertension and obesity in Chinese children and adolescents37. It is worth noting that genetic, dietary habits and life style are critical factors that influence incidence of metabolic disorders; these factors vary in different societies. Therefore, it is necessary to find the main risk factors for prevention of metabolic disorders in each nation. In the current analysis, we investigated Iranian overweight and obese adolescent and illustrated that higher habitual intake of legumes and nuts was linked to lower likelihood of MUO in crude model. Nevertheless, this association disappeared after considering socio-economic status, physical activity and weight status of subjects. In other words, adolescents with higher consumption of nuts and legumes might have better socio-economic status, healthier life style and normal weight. Therefore, a combination of these variables with consumption of nuts and legumes resulted in healthier metabolic health status in Iranian adolescents.
Epidemiologic studies on adults have also demonstrated an inverse association between regular legume intake and MetS and its components38,39. Additionally, a randomized controlled trial in adults with MetS illustrated that consumption of 30 gr/day soy protein could decrease BMI, weight, total cholesterol, LDL-c, and Apo B and increased HDL-c40. Another clinical trial revealed that adherence to the Mediterranean diet for 12 weeks had a favorable effect on oxidative stress, inflammation, liver hepatic steatosis, insulin resistance, BMI and body fat in adolescents with non-alcoholic fatty liver disease41. The contradictories in findings of previous investigations might be due to variations in study designs, study subjects, confounders, and multiple methods applied to assess dietary intakes.
Prior studies suggested some pathways to explain the positive effect of legumes and nuts on cardiometabolic risk factors. Legumes, soy and nuts are rich sources of protein, fiber, polyphenols, potassium, and magnesium42. Plant proteins have a high value of glutamic acid, a precursor for arginine. Therefore, legumes and nuts could decrease blood pressure through the production of nitric oxide43. Also, considering the role of potassium in insulin secretion, potassium intake from legumes and nuts have a favorable effect on glucose intolerance44. In addition, soluble fibers can decrease the absorption rate of nutrients and increase the excretion of bile acid and cholesterol; these fibers have also a positive effect on gut microbiota, hepatic gluconeogenesis, lipogenesis, and lipid storage through the synthesis of short-chain fatty acids (SCFAs). Moreover, the high fiber content of legumes and nuts can lead to low energy density of foods and consequently a decrease in risk of obesity and its complication45.
The current analysis investigated the relation of legumes and nuts consumption with MUO in Iranian overweight and obese adolescents who had different dietary intakes and cultural features from other societies. More than 55% of total energy intake among Iranian population is derived from carbohydrates, especially refined grains46. Moreover, two different definitions were used to categorize participants as MHO and MUO. Furthermore, several potential confounders were controlled in the analyses. However, several restrictions should be considered. Considering the cross-sectional design of the current study, it was impossible to define the causality of the relation of legumes and nuts consumption with MUO. Therefore, further prospective studies are required to confirm the causality of this relation. Although dietary intake assessment was done through a valid FFQ, some unavoidable biases such as misclassification and recall bias might have influenced our findings. We made adjustments for several confounders; however, the probable effects of residual confounders (birth weight, sleeping deprivation, maturity of persons, food habits, and BMI of parents) were not controlled. Overweight or obesity was defined through BMI; nevertheless, body composition and fat distribution, two critical factors that could affect metabolic health status, were not measured.
In conclusion, after taking potential confounders into account, no significant association was found between consumption of legumes and nuts and MUO in Iranian adolescents. The findings should be affirmed by further prospective studies.
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Abbreviations
- GBD:
-
Global burden of disease
- BP:
-
Blood pressure
- MHO:
-
Metabolically healthy overweight or obese
- MUO:
-
Metabolically unhealthy overweight or obese
- DASH:
-
Dietary approaches to stop hypertension
- BMI:
-
Body mass index
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- HDL-c:
-
High density lipoprotein cholesterol
- LDL-c:
-
Low density lipoprotein cholesterol
- SBP:
-
Systolic blood pressure
- CI:
-
Confidence interval
- FFQ:
-
Food frequency questionnaire
- WHO:
-
World Health Organization
- DBP:
-
Diastolic blood pressure
- FBG:
-
Fasting blood glucose
- IR:
-
Insulin resistance
- HOMA-IR:
-
Homeostasis model assessment insulin resistance
- IDF:
-
International Diabetes Federation
- SES:
-
Socioeconomic status
- ANOVA:
-
One-way analysis of variance
- ANCOVA:
-
Analysis of covariance
- SPSS:
-
Statistical package for the social sciences
- SD:
-
Standard deviation
- SE:
-
Standard error
- cIMT:
-
Carotid intima-media thickness
- SCFAs:
-
Short-chain fatty acids
- PAQ-A:
-
Physical Activity Questionnaire for Adolescents
- MetS:
-
Metabolic syndrome
References
Dagpo, T. D., Nolan, C. J. & Delghingaro-Augusto, V. Exploring therapeutic targets to reverse or prevent the transition from metabolically healthy to unhealthy obesity. Cells 9(7), 1596 (2020).
Lobstein, T. & Jackson-Leach, R. Planning for the worst: Estimates of obesity and comorbidities in school-age children in 2025. Pediatr. Obes. 11(5), 321–325 (2016).
Quek, Y.-H., Tam, W. W. S., Zhang, M. W. B. & Ho, R. C. M. Exploring the association between childhood and adolescent obesity and depression: A meta-analysis. Obes. Rev. 18(7), 742–754 (2017).
Geserick, M. et al. Acceleration of BMI in early childhood and risk of sustained obesity. N. Engl. J. Med. 379(14), 1303–1312 (2018).
Zhao, M. et al. Metabolically healthy obesity and high carotid intima-media thickness in children and adolescents: International Childhood Vascular Structure Evaluation Consortium. Diabetes Care 42(1), 119–125 (2018).
Robson, E. M., Costa, S., Hamer, M. & Johnson, W. Life course factors associated with metabolically healthy obesity: A protocol for the systematic review of longitudinal studies. Syst. Rev. 7(1), 50 (2018).
Balakrishnan, P. L. Identification of obesity and cardiovascular risk factors in childhood and adolescence. Pediatr. Clin. N. Am. 61(1), 153–171 (2014).
Twig, G. et al. Body-mass index in 2.3 million adolescents and cardiovascular death in adulthood. N. Engl. J. Med. 374(25), 2430–2440 (2016).
Rahimi, H. et al. Dietary approaches to stop hypertension (DASH) score and obesity phenotypes in children and adolescents. Nutr. J. 19(1), 112 (2020).
Phillips, C. M. Metabolically healthy obesity across the life course: Epidemiology, determinants, and implications. Ann. N. Y. Acad. Sci. 1391(1), 85–100 (2017).
Zimmet, P. et al. The metabolic syndrome in children and adolescents—An IDF consensus report. Pediatr. Diabetes 8(5), 299–306 (2007).
Matthews, D. R. et al. Homeostasis model assessment: insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28(7), 412–419 (1985).
Magkos, F. Metabolically healthy obesity: What’s in a name?. Am. J. Clin. Nutr. 110(3), 533–539 (2019).
Velázquez-López, L. et al. Mediterranean-style diet reduces metabolic syndrome components in obese children and adolescents with obesity. BMC Pediatr. 14, 175 (2014).
Julibert, A. et al. Metabolic syndrome features and excess weight were inversely associated with nut consumption after 1-year follow-up in the PREDIMED-Plus Study. J. Nutr. 150(12), 3161–3170 (2020).
Chatterjee, C., Gleddie, S. & Xiao, C.-W. Soybean bioactive peptides and their functional properties. Nutrients 10(9), 1211 (2018).
Schlesinger, S. et al. Food groups and risk of overweight, obesity, and weight gain: A systematic review and dose-response meta-analysis of prospective studies. Adv. Nutr. 10(2), 205–218 (2019).
Slagter, S. N. et al. Dietary patterns and physical activity in the metabolically (un)healthy obese: The Dutch Lifelines cohort study. Nutr. J. 17(1), 18 (2018).
Qorbani, M. et al. Association of dietary behaviors, biochemical, and lifestyle factors with metabolic phenotypes of obesity in children and adolescents. Diabetol. Metab. Syndr. 12(1), 108 (2020).
Yaghoubpour, K. et al. Association of obesity phenotypes in adolescents and incidence of early adulthood type 2 diabetes mellitus: Tehran lipid and glucose study. Pediatr. Diabetes 22(7), 937–945 (2021).
de Onis, M. et al. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 85(9), 660–667 (2007).
Kelishadi, R. et al. Development and evaluation of a questionnaire for assessment of determinants of weight disorders among children and adolescents: The Caspian-IV Study. Int. J. Prev. Med. 3(10), 699–705 (2012).
Daneshzad, E. et al. Food Insecurity is positively related to Dietary Inflammatory Index in Iranian high school girls. Int. J. Vitamin Nutr. Res. 90, 318 (2019).
Mohseni, H. et al. The relationship between history of dietary nutrients intakes and incidence of aggressive behavior in adolescent girls: A case–control study. Clin. Nutr. ESPEN 43, 200–205 (2021).
Ghaffarpour, M., Houshiar-Rad, A. & Kianfar, H. The manual for household measures, cooking yields factors and edible portion of foods. Tehran Nashre Olume Keshavarzy. 7(213), 42–58 (1999).
Corrado, C. Blood pressure measurement in children. Ital. J. Pediatr. 41(Suppl 2), A19. https://doi.org/10.1186/1824-7288-41-S2-A19 (2015) (eCollection 2015).
Pickering, T. G. et al. Recommendations for blood pressure measurement in humans and experimental animals: Part 1: Blood pressure measurement in humans: A statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Council on High Blood Pressure Research. Hypertension 45(1), 142–161 (2005).
Matthews, D. R. et al. Homeostasis model assessment: Insulin resistance and β-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 28, 412–419 (1985).
Kurtoglu, S. et al. The absence of insulin resistance in metabolic syndrome definition leads to underdiagnosing of metabolic risk in obese patients. Eur. J. Pediatr. 171(9), 1331–1337 (2012).
Shalitin, S., Abrahami, M., Lilos, P. & Phillip, M. Insulin resistance and impaired glucose tolerance in obese children and adolescents referred to a tertiary-care center in Israel. Int. J. Obes. (Lond). 29(6), 571–578 (2005).
Kowalski, K. C., Crocker, P. R. & Donen, R. M. The physical activity questionnaire for older children (PAQ-C) and adolescents (PAQ-A) manual. Coll. Kinesiol. Univ. Saskatchewan. 87(1), 1–38 (2004).
Garmaroudi, G. R. & Moradi, A. Socio-economic status in Iran: A study of measurement index. Health Monit. J. Iran. Inst. Health Sci. Res. 9(2), 137–144 (2010).
Park, M. H., Falconer, C., Viner, R. M. & Kinra, S. The impact of childhood obesity on morbidity and mortality in adulthood: A systematic review. Obes. Rev. 13(11), 985–1000 (2012).
Arenaza, L. et al. Adherence to the Mediterranean diet in metabolically healthy and unhealthy overweight and obese European adolescents: The HELENA study. Eur. J. Nutr. 58(7), 2615–2623 (2019).
Mirmiran, P., Ghotboddin Mohammadi, S., Bahadoran, Z. & Azizi, F. Study of nuts and dried fruits consumption in adolescents in relation to risk of metabolic syndrome and its components: Tehran lipid and glucose study. Int. J. Nutr. Food Sci. 5(1–2), 8–13 (2016).
Aghayan, M. et al. Association of nuts and unhealthy snacks with subclinical atherosclerosis among children and adolescents with overweight and obesity. Nutr. Metab. (Lond). 16, 23 (2019).
Wang, X. et al. Soy food intake associated with obesity and hypertension in children and adolescents in Guangzhou, Southern China. Nutrients 14(3), 425 (2022).
Sajjadi, F. et al. Relationship between legumes consumption and metabolic syndrome: Findings of the Isfahan Healthy Heart Program. ARYA Atheroscler. 10(1), 18–24 (2014).
Hosseinpour-Niazi, S. et al. Legume intake is inversely associated with metabolic syndrome in adults. Arch. Iran Med. 15(9), 538–544 (2012).
Ruscica, M. et al. Effect of soy on metabolic syndrome and cardiovascular risk factors: A randomized controlled trial. Eur. J. Nutr. 57(2), 499–511 (2018).
Yurtdaş, G., Akbulut, G., Baran, M. & Yılmaz, C. The effects of Mediterranean diet on hepatic steatosis, oxidative stress, and inflammation in adolescents with non-alcoholic fatty liver disease: A randomized controlled trial. Pediatr. Obes. 17(4), e12872 (2022).
Kim, Y., Keogh, J. B. & Clifton, P. M. Benefits of nut consumption on insulin resistance and cardiovascular risk factors: Multiple potential mechanisms of actions. Nutrients 9(11), 1271 (2017).
Ahnen, R. T., Jonnalagadda, S. S. & Slavin, J. L. Role of plant protein in nutrition, wellness, and health. Nutr. Rev. 77(11), 735–747 (2019).
Ashcroft, F. M. ATP-sensitive potassium channelopathies: Focus on insulin secretion. J. Clin. Investig. 115(8), 2047–2058 (2005).
Perrigue, M. M., Monsivais, P. & Drewnowski, A. Added soluble fiber enhances the satiating power of low-energy-density liquid yogurts. J. Am. Diet. Assoc. 109(11), 1862–1868 (2009).
Bahreynian, M. & Esmaillzadeh, A. Quantity and quality of carbohydrate intake in Iran: A target for nutritional intervention. Arch. Iran Med. 15, 648–649 (2012).
Acknowledgements
We wish to thank all participants of the study.
Funding
The financial support for conception, design, data analysis and manuscript drafting comes from Nutrition and Food Security Research Center, Isfahan University of Medical Sciences, Isfahan, Iran (no.2401320).
Author information
Authors and Affiliations
Contributions
H.H., Z.H., S.M., A.A., M.A., and P.S. contributed in conception, design, data collection, data interpretation, manuscript drafting, approval of the final version of the manuscript, and agreed for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Heshmatipour, H., Hajhashemy, Z., Mirzaei, S. et al. Association of legumes and nuts consumption with metabolic health status in Iranian overweight and obese adolescents. Sci Rep 13, 5784 (2023). https://doi.org/10.1038/s41598-023-32961-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-32961-2
- Springer Nature Limited