
Abstract
This retrospective cross-sectional study investigated the association between bone marrow lesions (BMLs) and bone mineral density (BMD) in the proximal tibia of end-stage osteoarthritic knees from a large patient sample. Overall, 1308 end-stage osteoarthritic knees were enrolled before total knee arthroplasty. The preoperative range of motion was recorded. Bone mineral density in the medial tibial plateau (MTP), lateral tibial plateau (LTP), and metaphysis were measured using dual-energy X-ray absorptiometry. The MTP/LTP, MTP/metaphysis, and LTP/metaphysis ratios were calculated. BMLs were scored using a whole-organ magnetic resonance imaging scoring system. The relationship between BMD and BML scores was investigated using linear regression analysis. The highest BMD was 0.787 ± 0.176 g/cm2 at the MTP, followed by 0.676 ± 0.180 g/cm2 and 0.572 ± 0.145 g/cm2 at the metaphysis and LTP, respectively. The prevalence of BMLs was 90.4% and 24.2% in the MTP and LTP, respectively. In women, higher BML scores at the MTP were positively correlated with the BMD of the MTP (p < 0.001, r = 0.278), MTP/LTP (p < 0.001, r = 0.267), and MTP/metaphysis ratios (p < 0.001, r = 0.243). Regression analysis showed that higher BML scores in the MTP were correlated with higher BMD in the MTP (p < 0.001) and lower BMD in the LTP (p < 0.001). High BML scores in the MTP were positively associated with high BMD in the MTP, which also induced the medial to lateral imbalance of BMD in the proximal tibia.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Sufficient bone strength is essential for successful total knee arthroplasty (TKA). Despite its promising long-term clinical outcomes1,2, complications such as aseptic loosening and periprosthetic fractures have been reported in patients3,4. Because lower preoperative bone mineral density (BMD) of the tibial plateau is associated with an increased risk of tibial component migration after TKA5, bone fragility and lower BMD must be addressed preoperatively. However, unlike the lumbar spine and proximal femur, BMD measurement of the proximal tibia is not common in clinical practice, and these measurements are not widely used. Thus, little is known about age-related changes of BMD in the proximal tibia and its effect on the incidence of complications after TKA.
Here, we focused on bone marrow lesions (BMLs) on magnetic resonance imaging (MRI) as a possible indicator for focal bone strength in the proximal tibia. BML, a common finding detected on MRI during the early- to end-stage of knee osteoarthritis (OA)6,7,8, which is associated with knee pain9,10, predicts radiographic structural changes11,12 and indicates the need for joint replacement13. BML histology reveals microcracks, bone remodeling, edema, fibrosis, and bleeding in the subchondral bone14,15; hence, BMLs may indicate possible weakness of the subchondral bone. An epidemiological study showed that BMD in patients with early knee OA was lower, with a high turnover of bone metabolism16. However, the relationship between BMD and BML in the proximal tibia of patients with end-stage knee OA remains unclear. These relationships with BMLs may be important to consider, without the need for an additional perioperative intervention or surgical planning, given that MRI scanning has become a routine preoperative examination.
This cross-sectional study aimed to examine BMD of the proximal tibia in patients with end-stage knee OA for age-related changes. Additionally, the association between BMLs and BMD in the proximal tibia was investigated in a large patient population. We hypothesized that BML size would correlate with increased BMD due to sclerosis of the subchondral bone. Examining these relationships may aid in understanding the etiology of end-stage knee OA and clinicians’ planning for perioperative therapeutic strategies.
Methods
Patients
Overall, 1621 TKA procedures were performed between November 2007 and September 2018. Among consecutive patients who underwent TKA, the following were excluded from the study: (1) 12 patients with rheumatoid arthritis, (2) one patient treated for knee joint infection, (3) 12 patients who underwent postoperative high tibial osteotomy, and (4) 281 patients with incomplete datasets. Finally, data from 837 patients (1307 knees; 106 men, 731 women) were analyzed. Demographic data of all patients at the time of surgery, including age, sex, height, weight, body mass index (BMI), loss of knee extension angle, and knee flexion angle, were retrospectively collected from medical records. All patients’ data were de-identified. All participants provided written informed consent, and the study was done in agreement with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards and conducted with approval by the ethics committee of the Hirosaki Memorial Hospital (No. 2021-05, approved date: Jul. 29th, 2021). The reporting of this study conforms to the STROBE statement17.
BMD measurement
BMD of the proximal tibia was determined by dual-energy X-ray absorptiometry using Horizon W (S/N200827, Hologic, Inc. Tokyo, Japan). Patients were positioned supine with their knee flexed at 10° using a customized knee and ankle joint supportive device that positioned the knee with the patella facing upward. BMD was measured in the metaphysis, medial, and lateral parts of the proximal tibia. The region of interest (ROI) of the medial tibia was defined as the center of the tibial plateau, 10 mm distal to the subchondral bone on the AP scout image, shown as R1 (Fig. 1). The ROI of the lateral tibia was defined in the same manner, shown as R2 in Fig. 1. The ROI of the metaphysis was defined as the center of the tibia, 50 mm distal to the joint line of the proximal tibia, shown as R3 (Fig. 1). The size of ROI was uniformly set as 0.6 cm2. The medial tibial plateau/lateral tibial plateau (MTP/LTP), MTP/metaphysis, and LTP/metaphysis ratios were calculated to estimate the medial to lateral balance of BMD in the proximal tibia.

Regions of interest (ROIs) in the proximal tibia for evaluating bone mineral density. ROI of the medial tibial plateau (R1): center of the medial tibial plateau 10 mm distal to the subchondral bone on the anterior–posterior scout image. ROI of the lateral tibial plateau (R2): the center of the lateral tibial plateau, 10 mm distal to the subchondral bone on the anterior–posterior scout image. ROI of the metaphysis (R3): the center of the tibia, 50 mm distal to the joint line of the proximal tibia.
BML scores in MRI
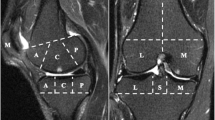
MRI scans of the involved knee were taken using a rapid extremity coil and mobile magnetic resonance unit (1.5 T; 8-channel knee phased array coil, GE Healthcare, Tokyo, Japan) preoperatively. Patients were positioned supine with their knees in full extension. Sequences included sagittal and coronal T2-weighted fat saturation-fast spin-echo (repetition time, 2400 ms; echo time, 90 ms; field of view, 10–20 cm; 320 × 224 matrix; 4-mm thick slices with a 1-mm interslice gap). BML was defined as an area of irregular hyperintense signals in the subchondral bone. The area was measured semi-quantitatively using the whole-organ MRI scoring method in 15 subregions18. Specifically, MTP, LTP, medial femoral condyle (MFC), and lateral femoral condyle (LFC) were divided into three subregions (anterior, central, and posterior), and the tibia had one additional subregion that represented the area below the tibial spine. The patella was divided into medial and lateral subregions. BMLs were each scored as integers from 0 to 3, where 0 = normal; 1 = mild, < 25% of the region; 2 = moderate, 25–50% of the region; and 3 = severe, > 50% of the region (Fig. 2).

Bone marrow lesion scores using magnetic resonance imaging. Sagittal and coronal views of short TI inversion recovery (STIR) images of the knee are taken. Bone marrow lesions (BMLs) are scored using the whole magnetic resonance imaging score, where A is scored as grade 0, B as grade 1, C as grade 2, and D as grade 3 in the medial femoral condyle.
The scores of the medial and lateral femorotibial (FT) joints were calculated as the total scores of BMLs in the center and posterior femur and the total scores of BMLs in three regions of the tibia, respectively. The BML score of the whole joint was calculated as the sum of the abovementioned 15 subregional scores. A BML was considered present if the total BML score was greater than zero. One blinded observer, an orthopedic surgeon, scored MR images with no access to the patients’ clinical information, and these scores were used for statistical analyses. Furthermore, to validate the scoring reliability, the BMLs of 100 randomly selected MR images were scored by an independent blinded orthopedic surgeon. The inter-rater reliability of the two observers, expressed as intraclass correlation coefficients (2.1), were 0.920 (95% confidence interval [CI] 0.884–0.945, p < 0.001) for medial FT scores, 0.942 (95% CI 0.915–0.960, p < 0.001) for lateral FT images, and 0.941 (95% CI 0.914–0.959, p < 0.001) for whole joint scores.
Radiographic evaluation
Anteroposterior (AP) weight-bearing radiographs of the knee were obtained from all patients. FT angle (FTA) was measured before surgery as a parameter of the lower extremity alignment using the anatomical axis drawn at the center of the femoral and tibial shafts in AP weight-bearing knee radiographs to assess the medial or lateral type OA.
Statistical analysis
To achieve 80% statistical power with an alpha of 0.05, power analysis revealed the requirement of a minimum of 144 patients for detecting any correlation between BML scores in MTP and BMD at MTP with Spearman’s correlation analysis. In the analysis, statistical power using 1307 patients was calculated as 1.000.
Quantitative data are expressed as mean ± SD. The chi-square test was used to compare differences in categorical variables. Mann–Whitney U test was used to compare differences in continuous variables between men and women, as most of these parameters were not normally distributed by Shapiro–Wilk tests. Spearman’s correlation coefficients (r) were estimated between BMD and BML scores and among BMD, BML scores and FTA. Linear regression analysis was performed with BML scores in the whole, MTP, and LTP as dependent variables. Age, sex, BMI, loss of knee extension and flexion, radiographic femorotibial angles, and BMD of the MTP, LTP, and metaphysis were the independent variables. Data input and analyses were performed using SPSS version 27.0 J (SPSS Inc., Chicago, IL, USA). Statistical significance was set at p < 0.05.
Ethics approval and consent to participate
The study was conducted with the approval of the ethics committee of the Hirosaki Memorial Hospital (No. 2021-05, approved date: Jul. 29th 2021). All participants provided written informed consent.
Results
A total of 1307 knees (from 106 men and 731 women) were enrolled for the statistical analysis. Preoperative FTAs (p < 0.001) were higher, weight and height were lower, and disease duration was longer in women than in men; however, no significance between-group differences in age, BMI, and preoperative range of motion were found (Table 1). In all patients, BMD of the MTP showed the highest value of 0.787 ± 0.176 g/cm2, followed by 0.676 ± 0.180 g/cm2 at the metaphysis and 0.572 ± 0.145 g/cm2 at the LTP. BMDs of the MTP, LTP, and metaphysis in women were significantly lower than those in men (Table 2). Also, the medial/lateral and medial/metaphysis ratios of women were higher than those of men, while there was no difference in the lateral/metaphysis ratio between men and women. Regarding the BMD of age groups, while fewer age-related changes were observed in men, the BMDs of the medial tibial plateau, lateral tibial plateau, and metaphysis in women decreased with age, especially in those aged > 65 years (Fig. 3).

Bone mineral densities among different age groups in both sexes. Mean and standard deviations of the bone mineral density of the medial tibial plateau (A), lateral tibial plateau (B), and metaphysis (C) in men and those of the medial tibial plateau (D), lateral tibial plateau (E), and metaphysis (F) in women are shown. A p-value below 0.05 was considered significant in the comparison of the following age groups: < 59 group (*), 60–65 group (†), 65–69 group (‡), and 70–74 group (#).
Overall BML scores in the medial femoral condyle, medial tibial plateau, medial femorotibial joint, lateral femoral condyle, lateral tibial plateau, lateral femorotibial joint, patellofemoral joint, and whole joint were 2.0 ± 1.5, 3.5 ± 2.5, 5.5 ± 3.8, 0.5 ± 1.0, 0.5 ± 1.2, 1.0 ± 1.9, 1.1 ± 1.3, and 8.5 ± 5.8, respectively. No significant difference in the BML score of each compartment was found between the sexes (Table 2). The prevalence of BMLs was 90.4% in MTP, 24.2% in LTP, 83.2% in MFC, 28.7% in LFC, 94.0% in medial FT joints, 38.3% in lateral FT joints, and 97.6% in whole joints. While the prevalence of BMLs was higher in the medial compartment than in the lateral compartment, no significant differences were found between men and women in both compartments (Fig. 4). Correlation analysis showed that women had higher BML scores in the MTPs, which were positively and weakly correlated with medial BMD (p < 0.001, r = 0.278) and the MTP/LTP (p < 0.001, r = 0.267) and MTP/metaphysis ratios (p < 0.001, r = 0.243). The MTP/LTP ratio weakly correlated with the FTA (r = 0.373, p < 0.001) (Fig. 5).

Prevalence of bone marrow lesions among different age groups in both sexes. Prevalence of bone marrow lesions (BMLs) at the medial femoral condyle (MFC) (A), medial tibial plateau (MTP) (B), and medial femorotibial (FT) joint (C), lateral femoral condyle (LFC) (D), lateral tibial plateau (LTP) (E), and lateral FT joint (F) in men and women are shown.

Correlation among medial to lateral balance of bone mineral density (BMD), bone marrow lesion (BML) score, and femorotibial angle (FTA). Scatter plot among BMD or BML score in medial tibia plateau (MTP), lateral tibia plateau (LTP), and MTP/LTP ratio and FTA are shown. Spearman’s correlation coefficients were calculated.
Regression analysis showed that high BML scores of the whole joint were positively correlated with loss of knee extension angle (p < 0.001) and BMD in MTP (p < 0.001) and negatively correlated with BMI (p < 0.001), knee flexion angle (< 0.001), BMD in LTP (p = 0.011), and BMD in metaphysis (p = 0.021) (Table 3). Similarly, higher BML scores of the MTP were correlated with lower BMI (p = 0.003), higher loss of knee extension angle (p < 0.001), higher FTA (p < 0.001), higher BMD in MTP (p < 0.001), and lower BMD in LTP (p < 0.001) (Table 3). Contrastingly, the BML scores of the LTP were positively correlated with BMDs of the MTP (p = 0.037) and LTP (p = 0.001) and negatively correlated with BMDs of the metaphysis (p = 0.017) (Table 3).
Discussion
The present study revealed that higher BML scores in MTP were associated with higher BMD in the MTP in end-stage osteoarthritic knees. This indicated that BMD of the proximal tibia was not low, even in severe osteoarthritic knees with large BMLs. However, a higher BML score in MTP showed a weak correlation with a higher MTP/LTP ratio, indicating medial to lateral imbalance of BMD in the proximal tibia. This information can help determine the surgical strategy or perioperative interventions for bone fragilities.
This study demonstrated detailed age-related changes in BMD of the proximal tibia, which was reduced in women aged > 65 years and not in men. Previous reports have shown that BMD of the proximal tibia was moderately correlated with distal femoral19,20, proximal femoral, and lumbar BMDs20. Bone strength around the knee joint can be estimated using systemic BMD. However, medial to lateral balance of the bone strength in the proximal tibia was not estimated using systemic BMD; measurement of local BMD in the proximal tibia is more valuable in detecting the medial to lateral balance of the BMD in the proximal tibia.
The MTP/LTP BMD ratio was above 1.0, as previously reported19,21,22. A higher MTP/LTP ratio was weakly correlated with higher BML scores, especially in the MTP. This medial to lateral imbalance of the bone strength within the proximal tibia could have been induced by increased sclerotic changes in the medial proximal tibia due to excessive medial loading, leading to severe varus deformity and lateral bone atrophy. Similarly, previous reports have shown that increased medial/lateral BMD ratios of the proximal tibia were positively associated with increased mechanical axis angle and OA worsening21,23. Further, Lo et al. reported that the prevalence of medial sclerosis in OA patients is associated with a higher MTP/LTP BMD ratio22. In the Framingham study, medial BMLs were correlated with a higher MTP/LTP ratio of BMD24. The coronal balance of bone strength within the tibia is an important factor for accurate osteotomy and implantation techniques. Since TKA with mechanical alignment needs balanced load-bearing on the tibial axis, low bone strength at the lateral tibia poses a risk for aseptic loosening25.
Higher BML scores in MTP were weakly correlated with higher BMD in MTP. This direct association of BML scores with BMD in MTP will be useful when considering indications for unicompartmental knee arthroplasty (UKA). Bone strength of MTP is one of the major factors that surgeons consider when planning a UKA; periprosthetic fractures of the MTP are frequent and cause severe complications in UKA at a rate of 3.3–7.2%, followed by aseptic loosening of the tibial component26,27. Our results suggest that a greater BML score in MTP did not reflect a lower BMD. This information may help determine structural surgical strategy and planning for UKA.
There was a discrepancy in interpreting BML causation between the early- and end-stage knee OA. Mechanical alignments of normal adults originally showed a varus of ≥ 3°, and the mechanical axis was slightly shifted to the medial side28. In early-knee OA, excessive contact pressure on the medial FT joint forms BMLs due to meniscus dysfunction or tibial varus29,30. We speculated that microcracks caused by excessive loading resulted in bleeding, bone remodeling, and high turnover of bone metabolism in the medial FT joint. In support of this, a previous epidemiological study showed that patients with early-knee OA had low systemic BMD and a high turnover of bone metabolism16; with disease progression, repeated bone remodeling caused sclerotic changes in the medial FT joint and accelerated varus deformity. Consequently, BMD in the medial FT joint in end-stage OA knees was not reduced and potentially reflected secondary changes of edema or micro-bleeds within sclerosis. Menopause causes BMD reduction31 and modulates subchondral bone remodeling32, which possibly caused the positive correlation between BMD and BML scores in women and not in men in our study.
Our results demonstrated that increased BML scores in end-stage osteoarthritic knees did not reflect bone fragility. BML score as an indication of perioperative intervention with a bisphosphonate or parathyroid hormone is controversial. Some reports demonstrated that bisphosphonates improved knee pain in patients with OA33 and reduced the need for TKA34. Contrastingly, a systematic review concluded that bisphosphonates had no remarkable effect on pain relief and the prevention of OA progression35. Ballal et al. also reported no significant benefit of oral bisphosphonates in patients with OA with BMLs in a 12-month clinical trial36. Furthermore, among patients with symptomatic knee OA and BMLs, yearly zoledronic acid infusions, compared with a placebo, did not significantly reduce 24-month cartilage volume loss37. These reports suggest that bisphosphonate use is not recommended for the treatment of knee OA. Therefore, interventions may not be required to improve bone strength in end-stage osteoarthritic knees with severe BML scores, although they may be necessary for patients with low systemic BMD. Furthermore, longitudinal studies should be conducted to investigate the relationship among the incidence of aseptic loosening or periprosthetic fractures, BMD of the proximal tibia, and BMLs.
This study has several limitations, including its retrospective design. First, the rate of bone metabolism was not evaluated. BMLs reflect bone remodeling; hence, measuring bone metabolic markers would aid in understanding bone quality. Moreover, complications such as renal failure, diabetes, and malignancy should be included in the analysis as they affect bone quality38. Second, the clinical outcomes of tibia component migration, aseptic loosening, and periprosthetic fractures were not examined. A longitudinal observational study could reveal the influence of BMLs or BMD on these complications. Third, the associations among knee OA severity, its symptoms, and the presence of BMLs could have been evaluated further. Fourth, the populations of men and women were not balanced, which had a risk for bias in comparisons between men and women. Fifth, the location of ROIs might be affected by the size of the proximal tibia because their size varies based on an individual’s body size. In this study, measurement location was defined clearly and uniformly, although the location might differ among individuals. Lastly, selection bias and reverse causation may have occurred in this retrospective study. Fewer patients with rheumatoid arthritis might lead to selection bias. Also, this study could not conclude whether a lower BML score led to lower BMD by partial weight bearing via pain or lower BMD easily led to microcracks and a higher BML. Further longitudinal analysis is needed to determine the absolute causality. Despite these limitations, this study revealed a positive association between higher BML scores and high BMD in the medial FT joint in women. Further longitudinal studies should investigate its association with clinical outcomes of aseptic loosening and periprosthetic fractures.
Conclusions
High BML scores in the MTP were positively and weakly associated with high BMD in MTP, which also induced the medial to lateral imbalance of BMD in the proximal tibia. Higher BML scores did not directly reflect focal lower BMD.
Data availability
All of data and material are available from the database of Department of Orthopaedic Surgery and Social Medicine, Hirosaki University Graduate School of Medicine.
Abbreviations
- BML:
-
Bone marrow lesions
- BMD:
-
Bone marrow density
- MTP:
-
Medial tibial plateau
- LTP:
-
Lateral tibial plateau
- TKA:
-
Total knee arthroplasty
- OA:
-
Osteoarthritis
- MRI:
-
Magnetic resonance imaging
- BMI:
-
Body mass index
- ROI:
-
Region of interest
- MFC:
-
Medial femoral condyle
- LFC:
-
Lateral femoral condyle
- FT:
-
Femorotibial
- CI:
-
Confidence interval
- UKA:
-
Unicompartmental knee arthroplasty
- FTA:
-
Femorotibial angle
References
Seo, S. S., Nha, K. W., Kim, T. Y. & Shin, Y. S. Survival of total knee arthroplasty after high tibial osteotomy versus primary total knee arthroplasty: A meta-analysis. Medicine Baltimore. 98, e16609 (2019).
Serna-Berna, R. et al. Cruciate-retaining vs posterior-stabilized primary total arthroplasty. Clinical outcome comparison with a minimum follow-up of 10 years. J. Arthroplasty. 33, 2491–2495 (2018).
Bauer, C. et al. Management and results in periprosthetic tibial fracture after total knee arthroplasty: Two-center 15-case retrospective series at 2 years’ follow-up. Orthop. Traumatol. Surg. Res. 106, 449–458 (2020).
Thiele, K. et al. Current failure mechanisms after knee arthroplasty have changed: polyethylene wear is less common in revision surgery. J. Bone. Joint. Surg. Am. 97, 715–720 (2015).
Andersen, M. R. et al. Low preoperative BMD is related to high migration of tibia components in uncemented TKA-92 patients in a combined DEXA and RSA study with 2-year follow-up. J. Arthroplasty. 32, 2141–2146 (2017).
Felson, D. T. et al. The association of bone marrow lesions with pain in knee osteoarthritis. Ann. Intern. Med. 134, 541–549 (2001).
Guermazi, A. et al. Severe radiographic knee osteoarthritis—Does Kellgren and Lawrence grade 4 represent end stage disease?—The MOST study. Osteoarthritis Cartilage 23, 1499–1505 (2015).
Ota, S. et al. Relationship between abnormalities detected by magnetic resonance imaging and knee symptoms in early knee osteoarthritis. Sci. Rep. 11, 15179 (2021).
Aso, K., Shahtaheri, S. M., McWilliams, D. F. & Walsh, D. A. Association of subchondral bone marrow lesion localization with weight-bearing pain in people with knee osteoarthritis: Data from the osteoarthritis initiative. Arthritis Res. Ther. 23, 35 (2021).
Foong, Y. C. et al. The clinical significance, natural history and predictors of bone marrow lesion change over eight years. Arthritis Res. Ther. 16, R149 (2014).
Driban, J. B. et al. Evaluation of bone marrow lesion volume as a knee osteoarthritis biomarker–longitudinal relationships with pain and structural changes: Data from the osteoarthritis initiative. Arthritis Res. Ther. 15, R112 (2013).
Felson, D. T. et al. Bone marrow edema and its relation to progression of knee osteoarthritis. Ann. Intern. Med. 139, 330–336 (2003).
Tanamas, S. K. et al. Bone marrow lesions in people with knee osteoarthritis predict progression of disease and joint replacement: A longitudinal study. Rheumatology (Oxford) 49, 2413–2419 (2010).
Kon, E. et al. Bone marrow lesions and subchondral bone pathology of the knee. Knee Surg. Sports Traumatol. Arthrosc. 24, 1797–1814 (2016).
Madry, H., van Dijk, C. N. & Mueller-Gerbl, M. The basic science of the subchondral bone. Knee Surg. Sports Traumatol. Arthrosc. 18, 419–433 (2010).
Ota, S. et al. Symptomatic bone marrow lesions induced by reduced bone mineral density in middle-aged women: A cross-sectional Japanese population study. Arthritis Res. Ther. 21, 113 (2019).
Vandenbroucke, J. P. et al. Strengthening the reporting of observational studies in epidemiology (STROBE): Explanation and elaboration. Int. J. Surg. 12, 1500–1524 (2014).
Peterfy, C. G. et al. Whole-organ magnetic resonance imaging score (WORMS) of the knee in osteoarthritis. Osteoarthritis Cartilage 12, 177–190 (2004).
Akamatsu, Y., Mitsugi, N., Taki, N., Kobayashi, H. & Saito, T. Medial versus lateral condyle bone mineral density ratios in a cross-sectional study: A potential marker for medial knee osteoarthritis severity. Arthritis Care Res (Hoboken). 64, 1036–1045 (2012).
Yoon, C. et al. Bone mineral density around the knee joint: Correlation with central bone mineral density and associated factors. J. Clin. Densitom. 23, 82–91 (2020).
Ishii, Y. et al. Association between bone mineral density distribution and various radiographic parameters in patients with advanced medial osteoarthritis of the knee. J. Orthop. Sci. 24, 686–692 (2019).
Lo, G. H. et al. The ratio of medial to lateral tibial plateau bone mineral density and compartment-specific tibiofemoral osteoarthritis. Osteoarthritis Cartilage 14, 984–990 (2006).
Johnston, J. D., Masri, B. A. & Wilson, D. R. Computed tomography topographic mapping of subchondral density (CT-TOMASD) in osteoarthritic and normal knees: Methodological development and preliminary findings. Osteoarthritis Cartilage 17, 1319–1326 (2009).
Lo, G. H. et al. Bone marrow lesions in the knee are associated with increased local bone density. Arthritis Rheum. 52, 2814–2821 (2005).
Jaroma, A., Soininvaara, T. & Kröger, H. Periprosthetic tibial bone mineral density changes after total knee arthroplasty. Acta Orthop. 87, 268–273 (2016).
Leenders, A. M., Schotanus, M. G. M., Wind, R. J. P., Borghans, R. A. P. & Kort, N. P. A high rate of tibial plateau fractures after early experience with patient-specific instrumentation for unicompartmental knee arthroplasties. Knee Surg. Sports Traumatol. Arthrosc. 26, 3491–3498 (2018).
Yokoyama, M. et al. Factors related to stress fracture after unicompartmental knee arthroplasty. Asia Pac. J. Sports Med. Arthrosc. Rehabil. Technol. 15, 1–5 (2019).
Bellemans, J., Colyn, W., Vandenneucker, H. & Victor, J. The Chitranjan Ranawat award: is neutral mechanical alignment normal for all patients? The concept of constitutional varus. Clin. Orthop. Relat. Res. 470, 45–53 (2012).
Ishibashi, K. et al. Bone marrow lesion severity was associated with proximal tibial inclination in early knee osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. 30, 668–679 (2022).
Willinger, L. et al. Varus alignment increases medial meniscus extrusion and peak contact pressure: A biomechanical study. Knee Surg. Sports Traumatol. Arthrosc. 28, 1092–1098 (2020).
Black, D. M. & Rosen, C. J. Postmenopausal osteoporosis. N. Engl. J. Med. 374, 2096–2097 (2016).
Xu, X. et al. Estrogen modulates cartilage and subchondral bone remodeling in an ovariectomized rat model of postmenopausal osteoarthritis. Med. Sci. Monit. 25, 3146–3153 (2019).
Laslett, L. L. et al. Zoledronic acid reduces knee pain and bone marrow lesions over 1 year: A randomised controlled trial. Ann. Rheum. Dis. 71, 1322–1328 (2012).
Fu, S. H., Wang, C. Y., Yang, R. S., Wu, F. L. & Hsiao, F. Y. Bisphosphonate use and the risk of undergoing total knee arthroplasty in osteoporotic patients with osteoarthritis: A nationwide cohort study in Taiwan. J. Bone Joint Surg. Am. 99, 938–946 (2017).
Vaysbrot, E. E., Osani, M. C., Musetti, M. C., McAlindon, T. E. & Bannuru, R. R. Are bisphosphonates efficacious in knee osteoarthritis? A meta-analysis of randomized controlled trials. Osteoarthritis Cartilage 26, 154–164 (2018).
Ballal, P. et al. The relation of oral bisphosphonates to bone marrow lesion volume among women with osteoarthritis. Osteoarthritis Cartilage 28, 1325–1329 (2020).
Cai, G. et al. Effect of intravenous zoledronic acid on tibiofemoral cartilage volume among patients with knee osteoarthritis with bone marrow lesions: A randomized clinical trial. JAMA 323, 1456–1466 (2020).
Saito, M., Fujii, K., Mori, Y. & Marumo, K. Role of collagen enzymatic and glycation induced cross-links as a determinant of bone quality in spontaneously diabetic WBN/Kob rats. Osteoporos. Int. 17, 1514–1523 (2006).
Acknowledgements
We would like to thank Editage (www.editage.jp) for English language editing.
Author information
Authors and Affiliations
Contributions
E.S., R.A., T.S., Y.W., Y.Y., and Y.I. contributed to the conception and design of the study. E.S., R.A., T.S., and Y.W. contributed to the acquisition of the data. E.S., R.A., Y.Y., and Y.I. contributed to the analysis and/or interpretation of the data. E.S., R.A., and Y.I. drafted the manuscript. E.S., R.A., and Y.I. revised the manuscript critically for important intellectual content. E.S., R.A., T.S., Y.W., Y.Y., and Y.I. approved the final version of the manuscript to be published. Y.I. is the guarantor. The corresponding author attests that all listed authors meet the authorship criteria and that no other authors meeting the criteria have been omitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sasaki, E., Araki, R., Sasaki, T. et al. Association between bone marrow lesions and bone mineral density of the proximal tibia in end-stage osteoarthritic knees. Sci Rep 13, 6516 (2023). https://doi.org/10.1038/s41598-023-33251-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-33251-7
- Springer Nature Limited