
Abstract
Bone-patellar tendon-bone (BPTB), two- and four-strand hamstring tendon (4SHT and 2SHT, respectively) are the most common autografts used for anterior cruciate ligament (ACL) reconstruction. The present study compared BPTB, 2SHT, and 4SHT for ACL reconstruction in terms of joint laxity, patient reported outcome measures (PROMs), rate of failure and anterior knee pain (AKP). The time to return to sport and the peak torque between the autografts were also compared. Finally, prognostic factors leading to worse outcomes were also investigated. It was hypothesized that all grafts yield similar proprieties in terms of joint laxity, patient reported outcome measures (PROMs) and rate of failure, but that the BPTB autograft causes a greater rate of anterior knee pain (AKP). The literature search was conducted. All clinical trials comparing BTPB and/or 2SHT, and/or 4SHT were accessed. Grafts other than BTPB and/or 4SHT and/or 2SHT were not considered. Articles reporting outcomes of allografts or synthetic grafts were not eligible, nor were those concerning revision settings. Articles reporting ACL reconstruction in patients with multi-ligament damage were also not eligible. Data from 95,575 procedures were retrieved. The median length of follow-up was 36 months. The median age of the patients was 27.5 years. With regard to joint laxity, similarity was found in terms of Lachman and Pivot shift tests between all three autografts. The BPTB demonstrated the greatest stability in terms of instrumental laxity. BPTB demonstrated the greatest PROMs. BPTB demonstrated the greatest rate of AKP, while AKP in 2SHT and 4SHT was similar. Concerning failure, statistically significant inconsistency was found (P = 0.008). The 4SHT demonstrated the quickest return to sport, followed by BPTB, and 2SHT. There was evidence of a negative association between the time span between injury to surgery, Lysholm score (P = 0.04), and Tegner scale (P = 0.04). Furthermore, there was evidence of a weak positive association between the time span between injury to surgery and return to sport (P = 0.01). BPTB may result in lower joint laxity, greater PROMs, and greater peak flexion torque compared to 2SHT and 4SHT autografts. On the other hand, BPTB reported the lowest peak extension torque and the greatest rate of AKP. Finally, a longer time span between injury and surgery negatively influences outcome.
Similar content being viewed by others
Introduction
The anterior cruciate ligament (ACL) is the primary passive constraint for internal tibial rotation and anterior tibial translation over the femur1,2,3,4. ACL injury is one of the most common knee injuries in the young athletic population5,6, most commonly in those performing jumping, twisting and cutting movements7. Its estimated incidence worldwide is about 70 per 100,000 people per year8,9,10,11,12. Anterior cruciate ligament rupture affects the knee kinematics13,14,15 resulting in joint instability, articular cartilage injury, and meniscal damage14,15,16,17,18,19,20,21,22,23,24,25,26,27. The optimal management of ACL is still debated28,29. Likewise, despite thousands of clinical articles on ACL surgical treatment, controversies still remain regarding the optimal choice of graft30,31,32,33,34. Bone-patellar tendon-bone (BPTB) and hamstring tendon (HT) autografts are the most common options for primary anterior cruciate ligament reconstruction35,36. The use of the BPTB autograft was introduced in the 1980s37 and it is still one of the most commonly used38. BPTB autografts achieve high patient satisfaction, quick return to sport and bone-to-bone healing39,40. However, concerns have been raised about donor site complications after BPTB autograft, such as anterior knee pain, discomfort, crepitus, loss of sensation, patellar fractures, contracture of the lower patella, and loss of extension strength41,42,43. To reduce damage to the extensor apparatus, the rates of anterior knee pain and patellar fractures, hamstring tendon (HT) autograft has been advocated44,45,46,47. However, ACL reconstruction using HT autograft may lead to a greater tunnel widening, flexor weakness, and knee laxity compared to BPTB42,48,49. In addition, the lack of bone block on the extremities of the HT graft may promote greater laxity leading to higher frequency of rupture50. Several clinical studies compare the autografts mentioned above, but the results are inconclusive35,51. In this Bayesian network meta-analysis, BPTB, two- and four-strand HT (4SHT and 2SHT, respectively) autografts for ACL reconstruction in young adults were compared. Joint laxity, patient reported outcome measures (PROMs), rate of failure, and anterior knee pain (AKP) between the autografts were compared, as were the time to return to sport and the peak torque. A multivariate analysis was conducted to investigate possible prognostic factors leading to worse outcomes. It was hypothesized that all grafts yield similar proprieties in terms of joint laxity, PROMs, and rate of failure, but that the BPTB autograft causes a greater rate of anterior knee pain (AKP).
Material and methods
Search strategy
The present Bayesian network meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) extension statement for reporting of systematic review incorporating network meta-analyses of health care interventions52. A PICO guide protocol was preliminary drafted:
-
P (population): ACL tears in young adults;
-
I (intervention): primary ACL reconstruction;
-
C (comparison): BPTB, 4SHT, 2SHT;
-
(outcomes): laxity, PROMs, failure, AKP.
Data source and extraction
Two reviewers (**;**) separately performed the literature search in February 2023. PubMed, Google scholar, Embase, and Scopus databases were accessed. The following keywords were used using the Boolean operator AND/OR: anterior cruciate ligament, ACL, pain, knee, tear, rupture, injury, damage, reconstruction, management, treatment, arthroscopy, surgery, autografts, bone patellar tendon bone, hamstring, strands, patient reported outcome measures, PROMs, laxity, stability, instability, complication, anterior knee pain, failure. The resulting titles were screened by the same authors independently. If the title and the abstract matched the topic, the article’s full-text was accessed. If the full-text was not accessible, the article was excluded from the present study. A cross reference of the bibliographies was also performed. Disagreements were debated and the final decision was made by a third author (**).
Eligibility criteria
All clinical investigations comparing BTPB, and/or 4SHT, and/or 2SHT were accessed. Articles in English, German, Italian, French, and Spanish were eligible. Levels I to III of evidence, according to Oxford Centre of Evidence-Based Medicine (OCEBM)53, were considered. Grafts other than BTPB and/or 4SHT and/or 2SHT were not eligible. Studies which reported data on skeletally immature patients were not considered. Articles reporting outcomes from allograft or synthetic graft reconstructions were not eligible, nor where those concerning revision settings. Articles reporting ACL reconstruction in patients with multi-ligament damage were not eligible. Letters, comments, reviews, opinions, and editorials were not included. Animals and biomechanics studies were also not considered. Only articles reporting quantitative data under the outcomes of interest were considered for inclusion. Missing data under the outcomes of interest warranted the exclusion from this study.
Data extraction
Two authors (**;**) independently examined the resulting articles for inclusion. Generalities and patient demographic were retrieved: author, year, journal, study design, length of the follow-up, type of graft, number of included patients, mean age, BMI, sex, time span from injury to surgery, and size of the graft. To investigate knee stability, data from the manual (Pivot shift and Lachman tests) and instrumental laxity were extracted. The instrumental laxity was evaluated using the arthrometers KT-1000 and KT-2000 (MEDmetric Corp, San Diego, California). Both of these devices applied a force of 134N on the tibial plateau over the femoral condyles, directed anteriorly. Concerning PROMs, data from the Tegner activity scale and Lysholm score at the last follow-up were extracted. The Lysholm score and Tegner activity scale have been validated for knee ligament surgery54,55,56. Data concerning the peak torque and the return to sport were also retrieved. The rates of failure and AKP were also investigated.
Methodology quality assessment
The methodological quality assessment was made using the risk of bias graph of the Review Manager Software (The Nordic Cochrane Collaboration, Copenhagen). The following risks of bias were evaluated: selection, detection, reporting, attrition, and other sources of bias.
Statistical analysis
The statistical analyses were performed by the main author (FM) using STATA Software/MP, Version 14.1 (StataCorporation, College Station, Texas, USA). For descriptive statistics, mean and standard deviation were calculated. The analysis of variance (ANOVA) was performed to evaluate the baseline comparability, with P values > 0.1 considered satisfactory.
To assess the return to sport, the ANOVA test with Tukey post-hoc test and honestly significant difference (HSD) were performed, with values of P < 0.05 were considered statistically significant. The confidence interval (CI) was set at 95%.
The NMA was performed through the STATA routine for Bayesian hierarchical random-effects model analysis. The inverse variance method was used for analysis of continuous variable, with standardized mean difference (STD) effect measure. The Log odd ratio (LOR) effect measure was used for binary data. The overall inconsistency was evaluated through the equation for global linearity via the Wald test. If the P value was > 0.5, the null hypothesis could not be rejected, and the consistency assumption could be accepted at the overall level of each treatment. Both confidence (CI) and percentile (PrI) intervals were set at 95%. Edge plot, interval plots, and funnel plots were obtained and evaluated.
For the multivariate analysis, a multiple linear model regression with Pearson Product-Moment Correlation Coefficient (r) was used to establish whether patient characteristics (age, BMI, women, time from injury to surgery, and graft size) are associated with the outcome (Pivot shift and Lachman tests, instrumental laxity, Lysholm score, Tegner scale, return to sport, failure, and anterior knee pain). The Cauchy–Schwarz formula was used for inequality: + 1 was considered as positive linear correlation, while − 1 was a negative one. Values of 0.1 < |\(r\)| < 0.3, 0.3 < |\(r\) | < 0.5, and |\(r\) | > 0.5 were considered to have respectively small, medium, and strong association. The overall significance was assessed through the χ2 test, with values of P < 0.05 considered statistically significant.
Ethical approval
This study complies with ethical standards.
Results
Search result
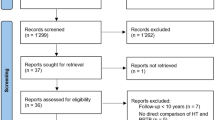
The literature search resulted in 1035 articles. Of them, 306 were excluded as they were duplicates. Furthermore, 636 articles were not eligible: not matching the topic (N = 403), reporting data on allografts or synthetic grafts (N = 41), study type (N = 154), revision or multi-ligament settings (N = 37), language limitation (N = 1). Additionally, 32 articles were excluded as they did not report quantitative data under the outcomes of interest. This left 61 clinical trials for the present study. The literature search results are shown in Fig. 1.

Flow chart of the literature search.
Methodological quality assessment
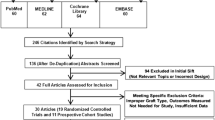
The prospective design of 85% (52 of 61) of the included investigations was an important strength of the present study. Of them, 62% (32 of 52) performed randomisation. Since most of the studies performed assessor blinding, the risk of detection bias was moderate to low. The proper analyses of most of the included studies, along with the intention to treat, clear definition of the timing of assessing outcomes, as well the use of validated tools for assessing outcomes, lead to a low risk of reporting and attrition bias. The risk of other biases was moderate to low. In conclusion, the methodological quality assessment demonstrated a moderate to low risk of bias (Fig. 2).

Methodological quality assessment.
Patient demographics
Data from 102,573 procedures were retrieved. The median length of follow-up was 51.5 ± 49.4 months. The median age of the patients was 27.9 ± 4.2 years. The median time span from injury to surgery was 14.4 ± 11.2 months. The mean BMI was 24.6 ± 1.6. The median size of the graft was 9.7 ± 0.7 mm. The ANOVA test found moderate baseline comparability among age, length of the follow-up, time span from injury to surgery, BMI, and graft size (P > 0.05). Patient demographics is shown in Table 1.
Network comparisons
With regard to joint laxity, similarities were found in terms of Lachman and Pivot shift tests between all three autografts. The BPTB demonstrated the greatest stability in terms of instrumental laxity. The equation for global linearity found no statically significant inconsistency (P = 0.06, P = 0.08, and P = 0.1, respectively). These results are shown in greater detail in Fig. 3.

Edge, funnel, and interval plots of the network comparisons: joint laxity.
Concerning PROMs, BPTB demonstrated the greatest Lysholm score and Tegner activity scale, followed by 2SHT and 4SHT, which scored similarly (Fig. 4). The equation for global linearity found no statically significant inconsistency (P = 0.3 and P = 0.5, respectively).

Edge, funnel, and interval plots of the network comparisons: PROMs.
Patients who underwent reconstruction of the ACL using a BPTB graft demonstrated the greatest rate of anterior knee pain, while both 2SHT and 4SHT ranked similarly. No statistically significant inconsistency was found (P = 0.2). The equation for global linearity found statistically significant inconsistency for the comparison of graft failure (P = 0.008), thus no further conclusion could be inferred. The network comparisons of complications are shown in greater detail in Fig. 5.

Edge, funnel, and interval plots of the network comparisons: complication.
Peak torque
Given the lack of quantitative data concerning the 2SHT group, only BPTB and 4SHT were considered for analysis of peak torque. BPTB demonstrated greater peak flexion torque at 60° (P < 0.0001) and 180° (P < 0.0001). No difference was found at 120° (P = 0.06). BPTB demonstrated lower peak extension torque at 60° (P = 0.01), 120° (P = 0.008), and 180° (P = 0.006). These results are shown in greater detail in Table 2.
Return to sport
The 4SHT demonstrated the quickest return to sport, followed by BPTB, and 2SHT (Table 3).
Multivariate analysis
There was evidence of a negative association between the time span between injury to surgery and Lysholm score (r = − 0.50; P = 0.04) and Tegner scale (r = − 0.26; P = 0.04). Furthermore, there was evidence of a weakly positive association between the time span between injury to surgery and return to sport (r = − 0.06; P = 0.01). The results of the multivariate analysis are shown in Table 4.
Discussion
According to the main findings of the present study, BPTB may promote lower joint laxity, greater PROMs, and greater peak flexion torque compared to 2SHT and 4SHT autografts in young adults. The ACL is one of the most important constraints against anteroposterior translation of the knee113,114. In the present study, BPTB was associated with the lowest peak extension torque and the greatest rate of AKP. Peak flexion torque is used to assess knee flexor muscle strength after reconstruction, as a quantitative outcome measure, particularly when comparing hamstring autografts to alternative graft options. Knee flexor weakness in knee flexion is relevant in certain sports such as gymnastics, judo, or wrestling, and it is useful to assess the return to sport115. Knee torque is significantly affected after ACL injury. Both extension and flexion isokinetic strength are important outcomes to evaluate after surgical reconstruction116. AKP remains a major complication after ACL reconstruction, and potentially recognizes several aetiologies, including bone-harvesting pain, neuroma of the infrapatellar branch of the medial saphenous following its lesion, and rarely, patellar tendinopathy33. Finally, a longer time span between ACL rupture and reconstruction may represent a negative factor influencing the outcome.
Concerning joint laxity, similarity was found in terms of Lachman and Pivot shift tests between all three autografts. The Lachman test evaluates the anterior translation of the tibia in relation to the femur with the knee in static flexion117. The Pivot shift test instead assesses the rotatory instability of the joint during its dynamic flexion118. Similarly, a previous meta-analysis found no difference in IKDC score, Lachman and Pivot shift tests between BPTB and hamstring autografts119. However, BPTB autograft resulted in a higher incidence of AKP, kneeling pain, and rate of osteoarthritis119. The literature on osteoarthritis of patients undergoing reconstruction with BPTB or HT autografts is controversial120,121. In the present study, patients receiving a BPTB graft demonstrated the lowest instrumental laxity and the greatest Lysholm score and Tegner activity scale, followed by 2SHT and 4SHT, which scored similarly. The Lysholm score and Tegner activity scale are outcomes measurements of a subjective nature that evaluate performance and activity restrictions both before and after surgery122. These PROMs have been validated for knee ligament surgery54,55,56.
On the other hand, BPTB demonstrated the greatest rate of AKP compared to both the 2SHT and 4SHT autografts, which showed a similar rate. Concerning failure, no statistically significant inconsistency was found. The equation for global linearity found statistically significant inconsistency for the comparison failure; thus, no further conclusion could be inferred. In a study on 5462 patients with primary ACL reconstruction, HT autografts resulted in greater anterior knee laxity and failures compared with BPTB autografts65. In a previous meta-analysis including 25 studies (47,613 ACL reconstructions), HT autografts failed at a higher rate than BPTB autografts123. Similar results have been evidenced in another meta-analysis involving 15 RCTs (1298 patients)121. A further meta-analysis including 20 RCTs compared BPTB versus 4SHT. The BPTP cohort evidenced lower laxity and failure rupture, but a greater risk of kneeling pain and AKP124.
Given the lack of quantitative data concerning the 2SHT group, only BPTB and 4SHT were considered in our study for analysis of peak torque. BPTB demonstrated greater peak flexion torque at 60° and 180°. No difference was found at 120°. BPTB demonstrated lower peak extension torque at 60°, 120°, and 180°. While BPTB exhibits some better outcome measures, it should be noted that BPTB also demonstrated the greatest rate of AKP. These findings agreed with previous studies comparing HT and BPTB, which stated that the latter restores greater knee stability, but also results in greater postoperative complications121,125,126. AKP is common following ACL reconstruction and can persist for a long time in athletes. The removal of the central third of the patellar tendon and its subsequent repair might cause a lowering of the patella and lead to increased sensitivity and pain during kneeling or squatting127. In this regard, in our study, the 4SHT graft demonstrated the quickest return to sport, followed by BPTB, and 2SHT. This should be considered when making a decision with athletes whose goal is to return to play as soon as possible. Lastly, results from the multivariate analysis demonstrated that a longer time span between initial injury and surgery was associated with lower Lysholm scores, Tegner scale, and longer return to sport. This worse outcome associated with a longer time from injury to surgery should be considered when planning the reconstruction. It should also be noted that some insurance companies currently require a dedicated physiotherapy trial for ACL injuries before surgery is authorized128. This delay in treatment can lead to suboptimal results129,130.
This study has certainly limitations. The retrospective nature of most studies is an important limitation which increases the risk of selection bias. Demographic data of the patients were collected, but further information regarding their general health were seldom reported in the included studies. Most of the authors did not specify whether the surgeon who performed the procedure was the investigator himself, and whether the assessor was blinded to the procedure performed. Many studies did not clearly specify the surgical technique (arthroscopic, open, or both) or postoperative management. Rehabilitation protocols following ACL reconstruction are associated with significant differences in outcome131. Several new modalities of rehabilitation after ACL reconstruction such as strengthening, and functional exercises, resistance training, neuromuscular exercise, high-level dynamic functional tasks and sport-specific training have been proposed132,133,134,135,136. However, given the lack of quantitative data, the various rehabilitation protocols could not be analysed separately. Most authors did not specify whether patients had undergone MRI preoperatively, thus providing poor information on preoperative diagnostic methods. Most authors did not report information on the sporting activity and level of the patients; therefore, further subgroup analyses were not possible. Given the lack of quantitative data, it was not possible to investigate additional autografts137,138. Allografts have been advocated as they avoid donor site morbidity139,140,141. However, the greater risk of graft-versus-host reaction, disease transmission, and delayed graft incorporation limits the use of allografts142,143,144. There is also a growing trend of using quadriceps tendon grafts, which may provide another viable and safe alternative for autografts options145,146,147,148. This autograft may result in a lower rate of failure compared to both BPTB and HT grafts, as well as a reduced rate of AKP compared to the BPTB autograft149. Further high-quality investigations should validate the present results also in skeletally immature patients. Furthermore, the aetiology of the AKP following ACL surgery still remains debated, and international recommendations on the management and classification of this condition are required.
Conclusion
BPTB may promote lower joint laxity, greater PROMs, and greater peak flexion torque compared to 2SHT and 4SHT autografts. On the other hand, BPTB resulted in the lowest peak knee extension torque and the greatest rate of AKP. Concerning PROMs and AKP, similar scores were obtained in the comparison between SHT2 and 4SHT. However, the 4SHT demonstrated the quickest return to sport, followed by BPTB, and 2SHT. Finally, longer time span between injury and ACL reconstruction negatively influences the outcomes.
Data availability
The datasets generated during and/or analysed during the current study are available throughout the manuscript.
References
Noyes, F. R. The function of the human anterior cruciate ligament and analysis of single- and double-bundle graft reconstructions. Sports Health 1(1), 66–75. https://doi.org/10.1177/1941738108326980 (2009).
Seitz, H., Schlenz, I., Muller, E. & Vecsei, V. Anterior instability of the knee despite an intensive rehabilitation program. Clin. Orthop. Relat. Res. 328, 159–164. https://doi.org/10.1097/00003086-199607000-00025 (1996).
O’Neill, D. B. Arthroscopically assisted reconstruction of the anterior cruciate ligament A prospective randomized analysis of three techniques. J. Bone Jt. Surg. Am. 78(6), 803–813 (1996).
Freeman, M. A. & Pinskerova, V. The movement of the normal tibio-femoral joint. J. Biomech. 38(2), 197–208. https://doi.org/10.1016/j.jbiomech.2004.02.006 (2005).
Gianotti, S. M., Marshall, S. W., Hume, P. A. & Bunt, L. Incidence of anterior cruciate ligament injury and other knee ligament injuries: A national population-based study. J. Sci. Med. Sport 12(6), 622–627. https://doi.org/10.1016/j.jsams.2008.07.005 (2009).
Maffulli, N., Loppini, M. & King, J. B. Anterior cruciate ligament tears: What we already know. Knee Surg. Sports Traumatol. Arthrosc. 21(7), 1704–1705. https://doi.org/10.1007/s00167-012-2123-2 (2013).
Prodromos, C. C., Han, Y., Rogowski, J., Joyce, B. & Shi, K. A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury-reduction regimen. Arthroscopy 23(12), 1320-1325 e1326. https://doi.org/10.1016/j.arthro.2007.07.003 (2007).
Clayton, R. A. & Court-Brown, C. M. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury 39(12), 1338–1344. https://doi.org/10.1016/j.injury.2008.06.021 (2008).
Meighan, A. A., Keating, J. F. & Will, E. Outcome after reconstruction of the anterior cruciate ligament in athletic patients. A comparison of early versus delayed surgery. J. Bone Jt. Surg. Br. 85(4), 521–524. https://doi.org/10.1302/0301-620x.85b4.13743 (2003).
Frank, C. B. & Jackson, D. W. The science of reconstruction of the anterior cruciate ligament. J. Bone Jt. Surg. Am. 79(10), 1556–1576. https://doi.org/10.2106/00004623-199710000-00014 (1997).
Arendt, E. A., Agel, J. & Dick, R. Anterior cruciate ligament injury patterns among collegiate men and women. J. Athl. Train. 34(2), 86–92 (1999).
Agel, J., Arendt, E. A. & Bershadsky, B. Anterior cruciate ligament injury in national collegiate athletic association basketball and soccer: A 13-year review. Am. J. Sports Med. 33(4), 524–530. https://doi.org/10.1177/0363546504269937 (2005).
Van de Velde, S. K., Gill, T. J. & Li, G. Evaluation of kinematics of anterior cruciate ligament-deficient knees with use of advanced imaging techniques, three-dimensional modeling techniques, and robotics. J. Bone Jt. Surg. Am. 91(Suppl 1), 108–114. https://doi.org/10.2106/JBJS.H.01382 (2009).
Chaudhari, A. M., Briant, P. L., Bevill, S. L., Koo, S. & Andriacchi, T. P. Knee kinematics, cartilage morphology, and osteoarthritis after ACL injury. Med. Sci. Sports Exerc. 40(2), 215–222. https://doi.org/10.1249/mss.0b013e31815cbb0e (2008).
Ferber, R., Osternig, L. R., Woollacott, M. H., Wasielewski, N. J. & Lee, J. H. Gait mechanics in chronic ACL deficiency and subsequent repair. Clin. Biomech. (Bristol, Avon) 17(4), 274–285. https://doi.org/10.1016/s0268-0033(02)00016-5 (2002).
Andersson, C., Odensten, M. & Gillquist, J. Knee function after surgical or nonsurgical treatment of acute rupture of the anterior cruciate ligament: A randomized study with a long-term follow-up period. Clin. Orthop. Relat. Res. 264, 255–263 (1991).
Fink, C., Hoser, C. & Benedetto, K. P. Sports capacity after rupture of the anterior cruciate ligament–surgical versus non-surgical therapy. Aktuelle Traumatol. 23(8), 371–375 (1993).
Fink, C., Hoser, C. & Benedetto, K. P. Development of arthrosis after rupture of the anterior cruciate ligament. A comparison of surgical and conservative therapy. Unfallchirurg 97(7), 357–361 (1994).
Frobell, R. B., Lohmander, L. S. & Roos, E. M. The challenge of recruiting patients with anterior cruciate ligament injury of the knee into a randomized clinical trial comparing surgical and non-surgical treatment. Contemp. Clin. Trials 28(3), 295–302. https://doi.org/10.1016/j.cct.2006.10.002 (2007).
Hinterwimmer, S., Engelschalk, M., Sauerland, S., Eitel, F. & Mutschler, W. Operative or conservative treatment of anterior cruciate ligament rupture: A systematic review of the literature. Unfallchirurg 106(5), 374–379. https://doi.org/10.1007/s00113-003-0596-7 (2003).
Jerosch, J., Schaffer, C. & Prymka, M. Proprioceptive abilities of surgically and conservatively treated knee joints with injuries of the cruciate ligament. Unfallchirurg 101(1), 26–31. https://doi.org/10.1007/s001130050228 (1998).
Meunier, A., Odensten, M. & Good, L. Long-term results after primary repair or non-surgical treatment of anterior cruciate ligament rupture: A randomized study with a 15-year follow-up. Scand. J. Med. Sci. Sports 17(3), 230–237. https://doi.org/10.1111/j.1600-0838.2006.00547.x (2007).
Odensten, M., Hamberg, P., Nordin, M., Lysholm, J. & Gillquist, J. Surgical or conservative treatment of the acutely torn anterior cruciate ligament. A randomized study with short-term follow-up observations. Clin. Orthop. Relat. Res. 198, 87–93 (1985).
Scavenius, M. et al. Isolated total ruptures of the anterior cruciate ligament—a clinical study with long-term follow-up of 7 years. Scand. J. Med. Sci. Sports 9(2), 114–119. https://doi.org/10.1111/j.1600-0838.1999.tb00219.x (1999).
Seitz, H., Chrysopoulos, A., Egkher, E. & Mousavi, M. Long-term results of replacement of the anterior cruciate ligament in comparison with conservative therapy. Chirurg 65(11), 992–998 (1994).
Zysk, S. P. & Refior, H. J. Operative or conservative treatment of the acutely torn anterior cruciate ligament in middle-aged patients. A follow-up study of 133 patients between the ages of 40 and 59 years. Arch. Orthop Trauma Surg. 120(1–2), 59–64. https://doi.org/10.1007/pl00021217 (2000).
van Meer, B. L. et al. Degenerative changes in the knee 2 years after anterior cruciate ligament rupture and related risk factors: A prospective observational follow-up study. Am. J. Sports Med. 44(6), 1524–1533. https://doi.org/10.1177/0363546516631936 (2016).
Bottoni, C. R., Liddell, T. R., Trainor, T. J., Freccero, D. M. & Lindell, K. K. Postoperative range of motion following anterior cruciate ligament reconstruction using autograft hamstrings: A prospective, randomized clinical trial of early versus delayed reconstructions. Am. J. Sports Med. 36(4), 656–662. https://doi.org/10.1177/0363546507312164 (2008).
Kostogiannis, I. et al. Activity level and subjective knee function 15 years after anterior cruciate ligament injury: A prospective, longitudinal study of nonreconstructed patients. Am. J. Sports Med. 35(7), 1135–1143. https://doi.org/10.1177/0363546507299238 (2007).
Migliorini, F. J. E., Tingart, M., Niewiera, M. & Rath, B. Bone-patellar tendon-bone versus four strands hamstring grafts for anterior cruciate ligament reconstruction. Muscles Ligaments Tendons J. https://doi.org/10.32098/mltj.01.2020.09 (2020).
Duchman, K. R., Lynch, T. S. & Spindler, K. P. Graft selection in anterior cruciate ligament surgery: Who gets what and why?. Clin. Sports Med. 36(1), 25–33. https://doi.org/10.1016/j.csm.2016.08.013 (2017).
Widner, M., Dunleavy, M. & Lynch, S. Outcomes following ACL reconstruction based on graft type: Are all grafts equivalent?. Curr. Rev. Musculoskelet. Med. 12(4), 460–465. https://doi.org/10.1007/s12178-019-09588-w (2019).
Thaunat, M., Fayard, J. M. & Sonnery-Cottet, B. Hamstring tendons or bone-patellar tendon-bone graft for anterior cruciate ligament reconstruction?. Orthop. Traumatol. Surg. Res. 105(1S), S89–S94. https://doi.org/10.1016/j.otsr.2018.05.014 (2019).
Johnson, D. H., Maffulli, N., King, J. B. & Shelbourne, K. D. Anterior cruciate ligament reconstruction: A cynical view from the British Isles on the indications for surgery. Arthroscopy 19(2), 203–209. https://doi.org/10.1053/jars.2003.50031 (2003).
Gifstad, T. et al. Long-term follow-up of patellar tendon grafts or hamstring tendon grafts in endoscopic ACL reconstructions. Knee Surg. Sports Traumatol. Arthrosc. 21(3), 576–583. https://doi.org/10.1007/s00167-012-1947-0 (2013).
Chee, M. Y. et al. Outcome of patellar tendon versus 4-strand hamstring tendon autografts for anterior cruciate ligament reconstruction: A systematic review and meta-analysis of prospective randomized trials. Arthroscopy 33(2), 450–463. https://doi.org/10.1016/j.arthro.2016.09.020 (2017).
Clancy, W. G. Jr., Ray, J. M. & Zoltan, D. J. Acute tears of the anterior cruciate ligament. Surgical versus conservative treatment. J. Bone Jt. Surg. Am. 70(10), 1483–1488 (1988).
Kartus, J., Movin, T. & Karlsson, J. Donor-site morbidity and anterior knee problems after anterior cruciate ligament reconstruction using autografts. Arthroscopy 17(9), 971–980. https://doi.org/10.1053/jars.2001.28979 (2001).
Gobbi, A., Mahajan, S., Zanazzo, M. & Tuy, B. Patellar tendon versus quadrupled bone-semitendinosus anterior cruciate ligament reconstruction: A prospective clinical investigation in athletes. Arthroscopy 19(6), 592–601. https://doi.org/10.1016/s0749-8063(03)00393-1 (2003).
Laxdal, G. et al. A prospective randomized comparison of bone-patellar tendon-bone and hamstring grafts for anterior cruciate ligament reconstruction. Arthroscopy 21(1), 34–42. https://doi.org/10.1016/j.arthro.2004.09.014 (2005).
Ejerhed, L., Kartus, J., Sernert, N., Kohler, K. & Karlsson, J. Patellar tendon or semitendinosus tendon autografts for anterior cruciate ligament reconstruction? A prospective randomized study with a two-year follow-up. Am. J. Sports Med. 31(1), 19–25. https://doi.org/10.1177/03635465030310011401 (2003).
Hardy, A. et al. Complications following harvesting of patellar tendon or hamstring tendon grafts for anterior cruciate ligament reconstruction: Systematic review of literature. Orthop. Traumatol. Surg. Res. 103(8S), S245–S248. https://doi.org/10.1016/j.otsr.2017.09.002 (2017).
Schandl, K. et al. Bone-Albumin filling decreases donor site morbidity and enhances bone formation after anterior cruciate ligament reconstruction with bone-patellar tendon-bone autografts. Int. Orthop. 40(10), 2097–2104. https://doi.org/10.1007/s00264-016-3246-8 (2016).
Rosenberg, T. D., Franklin, J. L., Baldwin, G. N. & Nelson, K. A. Extensor mechanism function after patellar tendon graft harvest for anterior cruciate ligament reconstruction. Am. J. Sports Med. 20(5), 519–525. https://doi.org/10.1177/036354659202000506 (1992) (discussion 525–516).
Aune, A. K., Holm, I., Risberg, M. A., Jensen, H. K. & Steen, H. Four-strand hamstring tendon autograft compared with patellar tendon-bone autograft for anterior cruciate ligament reconstruction A randomized study with two-year follow-up. Am. J. Sports Med. 29(6), 722–728. https://doi.org/10.1177/03635465010290060901 (2001).
Eriksson, K. et al. A comparison of quadruple semitendinosus and patellar tendon grafts in reconstruction of the anterior cruciate ligament. J. Bone Jt. Surg. Br. 83(3), 348–354. https://doi.org/10.1302/0301-620x.83b3.11685 (2001).
Shaieb, M. D., Kan, D. M., Chang, S. K., Marumoto, J. M. & Richardson, A. B. A prospective randomized comparison of patellar tendon versus semitendinosus and gracilis tendon autografts for anterior cruciate ligament reconstruction. Am. J. Sports Med. 30(2), 214–220. https://doi.org/10.1177/03635465020300021201 (2002).
DeFroda, S. F. et al. Tibial tunnel widening following anterior cruciate ligament reconstruction: A retrospective seven-year study evaluating the effects of initial graft tensioning and graft selection. Knee 25(6), 1107–1114. https://doi.org/10.1016/j.knee.2018.08.003 (2018).
Matthewson, G. & Macdonald, P. Techniques for femoral socket creation in ACL reconstruction. Sports Med. Arthrosc. Rev. 28(2), 56–65. https://doi.org/10.1097/JSA.0000000000000281 (2020).
Steiner, M. E., Hecker, A. T., Brown, C. H. Jr. & Hayes, W. C. Anterior cruciate ligament graft fixation. Comparison of hamstring and patellar tendon grafts. Am. J. Sports Med. 22(2), 240–246. https://doi.org/10.1177/036354659402200215 (1994) (discussion 246–247).
Matsumoto, A. et al. A comparison of bone-patellar tendon-bone and bone-hamstring tendon-bone autografts for anterior cruciate ligament reconstruction. Am. J. Sports Med. 34(2), 213–219. https://doi.org/10.1177/0363546505279919 (2006).
Page, M. J. et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 372, n160. https://doi.org/10.1136/bmj.n160 (2021).
Howick, J. C. I., et al. (2011) The 2011 Oxford CEBM Levels of Evidence. Oxford Centre for Evidence-Based Medicine. https://www.cebmnet/indexaspx?o=5653
Johnson, D. S. & Smith, R. B. Outcome measurement in the ACL deficient knee–what’s the score?. Knee 8(1), 51–57. https://doi.org/10.1016/s0968-0160(01)00068-0 (2001).
Lysholm, J. & Gillquist, J. Evaluation of knee ligament surgery results with special emphasis on use of a scoring scale. Am. J. Sports Med. 10(3), 150–154. https://doi.org/10.1177/036354658201000306 (1982).
Tegner, Y. & Lysholm, J. Rating systems in the evaluation of knee ligament injuries. Clin. Orthop. Relat. Res. 198, 43–49 (1985).
Aglietti, P., Giron, F., Buzzi, R., Biddau, F. & Sasso, F. Anterior cruciate ligament reconstruction: Bone-patellar tendon-bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J. Bone Jt. Surg. Am. 86(10), 2143–2155 (2004).
Aglietti, P., Buzzi, R., Zaccherotti, G. & De Biase, P. Patellar tendon versus doubled semitendinosus and gracilis tendons for anterior cruciate ligament reconstruction. Am. J. Sports Med. 22(2), 211–217. https://doi.org/10.1177/036354659402200210 (1994) (discussion 217–218).
Barenius, B., Nordlander, M., Ponzer, S., Tidermark, J. & Eriksson, K. Quality of life and clinical outcome after anterior cruciate ligament reconstruction using patellar tendon graft or quadrupled semitendinosus graft: An 8-year follow-up of a randomized controlled trial. Am. J. Sports Med. 38(8), 1533–1541. https://doi.org/10.1177/0363546510369549 (2010).
Beynnon, B. D. et al. Anterior cruciate ligament replacement: Comparison of bone-patellar tendon-bone grafts with two-strand hamstring grafts. A prospective, randomized study. J. Bone Jt. Surg. Am. 84(9), 1503–1513. https://doi.org/10.2106/00004623-200209000-00001 (2002).
Biz, C., Cigolotti, A., Zonta, F., Belluzzi, E. & Ruggieri, P. ACL reconstruction using a bone patellar tendon bone (BPTB) allograft or a hamstring tendon autograft (GST): A single-center comparative study. Acta Biomed. 90(12-S), 109–117. https://doi.org/10.23750/abm.v90i12-S.8973 (2019).
Bizzini, M., Gorelick, M., Munzinger, U. & Drobny, T. Joint laxity and isokinetic thigh muscle strength characteristics after anterior cruciate ligament reconstruction: Bone patellar tendon bone versus quadrupled hamstring autografts. Clin. J. Sport Med. 16(1), 4–9. https://doi.org/10.1097/01.jsm.0000188040.97135.43 (2006).
Carter, T. R. & Edinger, S. Isokinetic evaluation of anterior cruciate ligament reconstruction: Hamstring versus patellar tendon. Arthroscopy 15(2), 169–172. https://doi.org/10.1053/ar.1999.v15.0150161 (1999).
Corry, I. S., Webb, J. M., Clingeleffer, A. J. & Pinczewski, L. A. Arthroscopic reconstruction of the anterior cruciate ligament. A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am. J. Sports Med. 27(4), 444–454. https://doi.org/10.1177/03635465990270040701 (1999).
Cristiani, R. et al. Increased knee laxity with hamstring tendon autograft compared to patellar tendon autograft: A cohort study of 5462 patients with primary anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 27(2), 381–388. https://doi.org/10.1007/s00167-018-5029-9 (2019).
Denti, M., Vetere, D. L., Bandi, M. & Volpi, P. Comparative evaluation of knee stability following reconstruction of the anterior cruciate ligament with the bone-patellar tendon-bone and the double semitendinosus-gracilis methods: 1- and 2-year prospective study. Knee Surg. Sports Traumatol. Arthrosc. 14(7), 637–640. https://doi.org/10.1007/s00167-005-0007-4 (2006).
Drogset, J. O. et al. Autologous patellar tendon and quadrupled hamstring grafts in anterior cruciate ligament reconstruction: A prospective randomized multicenter review of different fixation methods. Knee Surg. Sports Traumatol. Arthrosc. 18(8), 1085–1093. https://doi.org/10.1007/s00167-009-0996-5 (2010).
Feller, J. A., Webster, K. E. & Gavin, B. Early post-operative morbidity following anterior cruciate ligament reconstruction: Patellar tendon versus hamstring graft. Knee Surg. Sports Traumatol. Arthrosc. 9(5), 260–266. https://doi.org/10.1007/s001670100216 (2001).
Gifstad, T. et al. Lower risk of revision with patellar tendon autografts compared with hamstring autografts: A registry study based on 45,998 primary ACL reconstructions in Scandinavia. Am. J. Sports Med. 42(10), 2319–2328. https://doi.org/10.1177/0363546514548164 (2014).
Gobbi, A. & Francisco, R. Factors affecting return to sports after anterior cruciate ligament reconstruction with patellar tendon and hamstring graft: A prospective clinical investigation. Knee Surg. Sports Traumatol. Arthrosc. 14(10), 1021–1028. https://doi.org/10.1007/s00167-006-0050-9 (2006).
Gudas, R., Jurkonis, R. & Smailys, A. Comparison of return to pre-injury sport after 10 mm size bone-patellar tendon-bone (BPTB) versus 8 mm hamstring anterior cruciate ligament reconstruction: A retrospective study with a two-year follow-up. Med. Sci. Monit. 24, 987–996 (2018).
Guglielmetti, L. G. B. et al. Prospective and randomized clinical evaluation of hamstring versus patellar tendon autograft for anterior cruciate ligament reconstruction in soccer players. Orthop. J. Sports Med. 9(9), 23259671211028170. https://doi.org/10.1177/23259671211028168 (2021).
Harilainen, A., Linko, E. & Sandelin, J. Randomized prospective study of ACL reconstruction with interference screw fixation in patellar tendon autografts versus femoral metal plate suspension and tibial post fixation in hamstring tendon autografts: 5-year clinical and radiological follow-up results. Knee Surg. Sports Traumatol. Arthrosc. 14(6), 517–528. https://doi.org/10.1007/s00167-006-0059-0 (2006).
Heijne, A. & Werner, S. A 2-year follow-up of rehabilitation after ACL reconstruction using patellar tendon or hamstring tendon grafts: A prospective randomised outcome study. Knee Surg. Sports Traumatol. Arthrosc. 18(6), 805–813. https://doi.org/10.1007/s00167-009-0961-3 (2010).
Heijne, A., Hagstromer, M. & Werner, S. A two- and five-year follow-up of clinical outcome after ACL reconstruction using BPTB or hamstring tendon grafts: A prospective intervention outcome study. Knee Surg. Sports Traumatol. Arthrosc. 23(3), 799–807. https://doi.org/10.1007/s00167-013-2727-1 (2015).
Holm, I., Oiestad, B. E., Risberg, M. A. & Aune, A. K. No difference in knee function or prevalence of osteoarthritis after reconstruction of the anterior cruciate ligament with 4-strand hamstring autograft versus patellar tendon-bone autograft: A randomized study with 10-year follow-up. Am. J. Sports Med. 38(3), 448–454. https://doi.org/10.1177/0363546509350301 (2010).
Ibrahim, S. A. et al. Clinical evaluation of arthroscopically assisted anterior cruciate ligament reconstruction: Patellar tendon versus gracilis and semitendinosus autograft. Arthroscopy 21(4), 412–417. https://doi.org/10.1016/j.arthro.2004.12.002 (2005).
Jansson, K. A., Linko, E., Sandelin, J. & Harilainen, A. A prospective randomized study of patellar versus hamstring tendon autografts for anterior cruciate ligament reconstruction. Am. J. Sports Med. 31(1), 12–18. https://doi.org/10.1177/03635465030310010501 (2003).
Kautzner, J., Kos, P., Hanus, M., Trc, T. & Havlas, V. A comparison of ACL reconstruction using patellar tendon versus hamstring autograft in female patients: A prospective randomised study. Int. Orthop. 39(1), 125–130. https://doi.org/10.1007/s00264-014-2495-7 (2015).
Keays, S. L., Bullock-Saxton, J. E., Keays, A. C., Newcombe, P. A. & Bullock, M. I. A 6-year follow-up of the effect of graft site on strength, stability, range of motion, function, and joint degeneration after anterior cruciate ligament reconstruction: Patellar tendon versus semitendinosus and Gracilis tendon graft. Am. J. Sports Med. 35(5), 729–739. https://doi.org/10.1177/0363546506298277 (2007).
Laxdal, G., Sernert, N., Ejerhed, L., Karlsson, J. & Kartus, J. T. A prospective comparison of bone-patellar tendon-bone and hamstring tendon grafts for anterior cruciate ligament reconstruction in male patients. Knee Surg. Sports Traumatol. Arthrosc. 15(2), 115–125. https://doi.org/10.1007/s00167-006-0165-z (2007).
Leitgeb, J. et al. Primary anterior cruciate ligament reconstruction in athletes: A 5-year follow up comparing patellar tendon versus hamstring tendon autograft. Wien Klin. Wochenschr 126(13–14), 397–402. https://doi.org/10.1007/s00508-014-0550-4 (2014).
Leys, T., Salmon, L., Waller, A., Linklater, J. & Pinczewski, L. Clinical results and risk factors for reinjury 15 years after anterior cruciate ligament reconstruction: A prospective study of hamstring and patellar tendon grafts. Am. J. Sports Med. 40(3), 595–605. https://doi.org/10.1177/0363546511430375 (2012).
Liden, M., Ejerhed, L., Sernert, N., Laxdal, G. & Kartus, J. Patellar tendon or semitendinosus tendon autografts for anterior cruciate ligament reconstruction: A prospective, randomized study with a 7-year follow-up. Am. J. Sports Med. 35(5), 740–748. https://doi.org/10.1177/0363546506298275 (2007).
Machado, F. et al. Knee isokinetic performance following anterior cruciate ligament reconstruction: Patellar tendon versus hamstrings graft. Phys. Sports Med. 46(1), 30–35. https://doi.org/10.1080/00913847.2018.1418592 (2018).
Maletis, G. B., Cameron, S. L., Tengan, J. J. & Burchette, R. J. A prospective randomized study of anterior cruciate ligament reconstruction: A comparison of patellar tendon and quadruple-strand semitendinosus/gracilis tendons fixed with bioabsorbable interference screws. Am. J. Sports Med. 35(3), 384–394. https://doi.org/10.1177/0363546506294361 (2007).
Maletis, G. B., Inacio, M. C., Desmond, J. L. & Funahashi, T. T. Reconstruction of the anterior cruciate ligament: Association of graft choice with increased risk of early revision. Bone Jt. J. 95-B(5), 623–628. https://doi.org/10.1302/0301-620X.95B5.30872 (2013).
Marder, R. A., Raskind, J. R. & Carroll, M. Prospective evaluation of arthroscopically assisted anterior cruciate ligament reconstruction. Patellar tendon versus semitendinosus and gracilis tendons. Am. J. Sports Med. 19(5), 478–484. https://doi.org/10.1177/036354659101900510 (1991).
Mohtadi, N., Chan, D., Barber, R. & Oddone Paolucci, E. A randomized clinical trial comparing patellar tendon, hamstring tendon, and double-bundle ACL reconstructions: Patient-reported and clinical outcomes at a minimal 2-year follow-up. Clin. J. Sport Med. 25(4), 321–331. https://doi.org/10.1097/JSM.0000000000000165 (2015).
Pasquini, A., Jacopetti, M., Pogliacomi, F., Ramazzina, I. & Costantino, C. Neuromuscular recovery in ACL reconstruction with bone-tendon-patellar-bone and semitendinosus-gracilis autograft. Acta Biomed. 88(4S), 62–68. https://doi.org/10.23750/abm.v88i4-S.6795 (2017).
Persson, A. et al. Increased risk of revision with hamstring tendon grafts compared with patellar tendon grafts after anterior cruciate ligament reconstruction: A study of 12,643 patients from the Norwegian Cruciate Ligament Registry, 2004–2012. Am. J. Sports Med. 42(2), 285–291. https://doi.org/10.1177/0363546513511419 (2014).
Persson, A. et al. Registry data highlight increased revision rates for endobutton/biosure HA in ACL reconstruction with hamstring tendon autograft: A nationwide cohort study from the Norwegian Knee Ligament Registry, 2004–2013. Am. J. Sports Med. 43(9), 2182–2188. https://doi.org/10.1177/0363546515584757 (2015).
Pinczewski, L. A. et al. A 10-year comparison of anterior cruciate ligament reconstructions with hamstring tendon and patellar tendon autograft: A controlled, prospective trial. Am. J. Sports Med. 35(4), 564–574. https://doi.org/10.1177/0363546506296042 (2007).
Pinczewski, L. A., Deehan, D. J., Salmon, L. J., Russell, V. J. & Clingeleffer, A. A five-year comparison of patellar tendon versus four-strand hamstring tendon autograft for arthroscopic reconstruction of the anterior cruciate ligament. Am. J. Sports Med. 30(4), 523–536. https://doi.org/10.1177/03635465020300041201 (2002).
Cristea VPVGCPVSS (2010) Anterior cruciate ligament reconstruction: Soft tissue vs. bone-tendon-bone advanced technologies for enhancing quality of life. https://doi.org/10.1109/ATEQUAL.2010.22.
Rahr-Wagner, L., Thillemann, T. M., Pedersen, A. B. & Lind, M. Comparison of hamstring tendon and patellar tendon grafts in anterior cruciate ligament reconstruction in a nationwide population-based cohort study: Results from the Danish Registry of knee ligament reconstruction. Am. J. Sports Med. 42(2), 278–284. https://doi.org/10.1177/0363546513509220 (2014).
Razi, M., Sarzaeem, M. M., Kazemian, G. H., Najafi, F. & Najafi, M. A. Reconstruction of the anterior cruciate ligament: A comparison between bone-patellar tendon-bone grafts and fourstrand hamstring grafts. Med. J. Islam Repub. Iran 28, 134 (2014).
Sadoghi, P. et al. Reconstruction of the anterior cruciate ligament: A clinical comparison of bone-patellar tendon-bone single bundle versus semitendinosus and gracilis double bundle technique. Int. Orthop. 35(1), 127–133. https://doi.org/10.1007/s00264-010-1037-1 (2011).
Sajovic, M., Vengust, V., Komadina, R., Tavcar, R. & Skaza, K. A prospective, randomized comparison of semitendinosus and gracilis tendon versus patellar tendon autografts for anterior cruciate ligament reconstruction: Five-year follow-up. Am. J. Sports Med. 34(12), 1933–1940. https://doi.org/10.1177/0363546506290726 (2006).
Sajovic, M., Strahovnik, A., Dernovsek, M. Z. & Skaza, K. Quality of life and clinical outcome comparison of semitendinosus and gracilis tendon versus patellar tendon autografts for anterior cruciate ligament reconstruction: An 11-year follow-up of a randomized controlled trial. Am. J. Sports Med. 39(10), 2161–2169. https://doi.org/10.1177/0363546511411702 (2011).
Sajovic, M., Stropnik, D. & Skaza, K. Long-term comparison of semitendinosus and gracilis tendon versus patellar tendon autografts for anterior cruciate ligament reconstruction: A 17-year follow-up of a randomized controlled trial. Am. J. Sports Med. 46(8), 1800–1808. https://doi.org/10.1177/0363546518768768 (2018).
Stanczak, K. et al. Comparison of hamstring and patellar tendon grafts in anterior cruciate ligament reconstruction: A prospective randomized study. J. Int. Med. Res. 46(2), 785–791. https://doi.org/10.1177/0300060517722696 (2018).
Svensson, M., Sernert, N., Ejerhed, L., Karlsson, J. & Kartus, J. T. A prospective comparison of bone-patellar tendon-bone and hamstring grafts for anterior cruciate ligament reconstruction in female patients. Knee Surg. Sports Traumatol. Arthrosc. 14(3), 278–286. https://doi.org/10.1007/s00167-005-0708-8 (2006).
Tajima, T. et al. Clinical and radiographic outcomes of double-bundle anterior cruciate ligament reconstruction for Asian patients with bone-patellar tendon-bone and gracilis tendon grafts: A matched-control comparison. J. Knee Surg. 34(14), 1545–1554. https://doi.org/10.1055/s-0040-1710376 (2021).
Taylor, D. C. et al. Patellar tendon versus hamstring tendon autografts for anterior cruciate ligament reconstruction: A randomized controlled trial using similar femoral and tibial fixation methods. Am. J. Sports Med. 37(10), 1946–1957. https://doi.org/10.1177/0363546509339577 (2009).
Thompson, S. M. et al. Twenty-year outcome of a longitudinal prospective evaluation of isolated endoscopic anterior cruciate ligament reconstruction with patellar tendon or hamstring autograft. Am. J. Sports Med. 44(12), 3083–3094. https://doi.org/10.1177/0363546516658041 (2016).
Wagner, M., Kaab, M. J., Schallock, J., Haas, N. P. & Weiler, A. Hamstring tendon versus patellar tendon anterior cruciate ligament reconstruction using biodegradable interference fit fixation: A prospective matched-group analysis. Am. J. Sports Med. 33(9), 1327–1336. https://doi.org/10.1177/0363546504273488 (2005).
Webster, K. E., Feller, J. A., Hartnett, N., Leigh, W. B. & Richmond, A. K. Comparison of patellar tendon and hamstring tendon anterior cruciate ligament reconstruction: A 15-year follow-up of a randomized controlled trial. Am. J. Sports Med. 44(1), 83–90. https://doi.org/10.1177/0363546515611886 (2016).
Wipfler, B. et al. Anterior cruciate ligament reconstruction using patellar tendon versus hamstring tendon: A prospective comparative study with 9-year follow-up. Arthroscopy 27(5), 653–665. https://doi.org/10.1016/j.arthro.2011.01.015 (2011).
Witvrouw, E. et al. Patellar tendon vs doubled semitendinosus and gracilis tendon for anterior cruciate ligament reconstruction. Int. Orthop. 25(5), 308–311. https://doi.org/10.1007/s002640100268 (2001).
Zaffagnini, S. et al. Prospective and randomized evaluation of ACL reconstruction with three techniques: A clinical and radiographic evaluation at 5 years follow-up. Knee Surg. Sports Traumatol. Arthrosc. 14(11), 1060–1069. https://doi.org/10.1007/s00167-006-0130-x (2006).
Zoran, Z. et al. Knee stability after arthroscopic anterior cruciate ligament reconstruction using the middle third of the patellar ligament and quadrupled hamstring tendons grafts—a two-year follow-up. Injury 46(Suppl 6), S91-95. https://doi.org/10.1016/j.injury.2015.10.056 (2015).
Blankevoort, L., Huiskes, R. & de Lange, A. The envelope of passive knee joint motion. J. Biomech. 21(9), 705–720. https://doi.org/10.1016/0021-9290(88)90280-1 (1988).
Butler, D. L., Noyes, F. R. & Grood, E. S. Ligamentous restraints to anterior–posterior drawer in the human knee. A biomechanical study. J. Bone Jt. Surg. Am. 62(2), 259–270 (1980).
Krolikowska, A., Reichert, P., Czamara, A. & Krzeminska, K. Peak torque angle of anterior cruciate ligament-reconstructed knee flexor muscles in patients with semitendinosus and gracilis autograft is shifted towards extension regardless of the postoperative duration of supervised physiotherapy. PloS One 14(2), e0211825. https://doi.org/10.1371/journal.pone.0211825 (2019).
Tsepis, E., Giakas, G., Vagenas, G. & Georgoulis, A. Frequency content asymmetry of the isokinetic curve between ACL deficient and healthy knee. J. Biomech. 37(6), 857–864. https://doi.org/10.1016/j.jbiomech.2003.11.009 (2004).
Coffey, R. & Bordoni, B. Lachman Test (StatPearls, 2022).
Horvath, A., Meredith, S. J., Nishida, K., Hoshino, Y. & Musahl, V. Objectifying the pivot shift test. Sports Med. Arthrosc. Rev. 28(2), 36–40. https://doi.org/10.1097/JSA.0000000000000260 (2020).
Xie, X. et al. Increased incidence of osteoarthritis of knee joint after ACL reconstruction with bone-patellar tendon-bone autografts than hamstring autografts: A meta-analysis of 1,443 patients at a minimum of 5 years. Eur. J. Orthop. Surg. Traumatol. 25(1), 149–159. https://doi.org/10.1007/s00590-014-1459-3 (2015).
Belk, J. W., Kraeutler, M. J., Carver, T. J. & McCarty, E. C. Knee osteoarthritis after anterior cruciate ligament reconstruction with bone-patellar tendon-bone versus hamstring tendon autograft: A systematic review of randomized controlled trials. Arthroscopy 34(4), 1358–1365. https://doi.org/10.1016/j.arthro.2017.11.032 (2018).
Zhao, L. et al. Outcome of bone-patellar tendon-bone vs hamstring tendon autograft for anterior cruciate ligament reconstruction: A meta-analysis of randomized controlled trials with a 5-year minimum follow-up. Medicine (Baltimore0 99(48), e23476. https://doi.org/10.1097/MD.0000000000023476 (2020).
Briggs, K. K., Steadman, J. R., Hay, C. J. & Hines, S. L. Lysholm score and Tegner activity level in individuals with normal knees. Am. J. Sports Med. 37(5), 898–901. https://doi.org/10.1177/0363546508330149 (2009).
Samuelsen, B. T., Webster, K. E., Johnson, N. R., Hewett, T. E. & Krych, A. J. Hamstring autograft versus patellar tendon autograft for ACL reconstruction: Is there a difference in graft failure rate? a meta-analysis of 47,613 patients. Clin. Orthop. Relat. Res. 475(10), 2459–2468. https://doi.org/10.1007/s11999-017-5278-9 (2017).
Migliorini, F., Eschweiler, J., Tingart, M., Niewiera, M. & Rath, B. Bone-patellar tendon-bone versus four strands hamstring grafts for anterior cruciate ligament reconstruction. Muscles Ligaments Tendons J. 10, 1 (2020).
Li, S. et al. A meta-analysis of hamstring autografts versus bone-patellar tendon-bone autografts for reconstruction of the anterior cruciate ligament. Knee 18(5), 287–293. https://doi.org/10.1016/j.knee.2010.08.002 (2011).
Li, S. et al. A systematic review of randomized controlled clinical trials comparing hamstring autografts versus bone-patellar tendon-bone autografts for the reconstruction of the anterior cruciate ligament. Arch. Orthop. Trauma Surg. 132(9), 1287–1297. https://doi.org/10.1007/s00402-012-1532-5 (2012).
Marques, F. D. S. et al. Anterior knee pain after anterior cruciate ligament reconstruction. Orthop. J. Sports Med. 8(10), 2325967120961082. https://doi.org/10.1177/2325967120961082 (2020).
Bram, J. T. et al. How do race and insurance status affect the care of pediatric anterior cruciate ligament injuries?. Clin. J. Sport Med. 30(6), e201–e206. https://doi.org/10.1097/JSM.0000000000000706 (2020).
Keyhani, S., Esmailiejah, A. A., Mirhoseini, M. S., Hosseininejad, S. M. & Ghanbari, N. The Prevalence, zone, and type of the meniscus tear in patients with anterior cruciate ligament (ACL) injury; does delayed ACL reconstruction affects the meniscal injury?. Arch. Bone Jt. Surg. 8(3), 432–438. https://doi.org/10.22038/abjs.2019.39084.2076 (2020).
Kawashima, I. et al. Delayed anterior cruciate ligament reconstruction increases the incidence of medial meniscal bucket handle tears and medial compartment chondral injuries in patients aged 40 years and older. Arch Orthop. Trauma Surg. 141(6), 971–975. https://doi.org/10.1007/s00402-020-03745-4 (2021).
Forrester, L. A., Schweppe, E. A. & Popkin, C. A. Variability in rehabilitation protocols following pediatric anterior cruciate ligament (ACL) reconstruction. Phys. Sports Med. 47(4), 448–454. https://doi.org/10.1080/00913847.2019.1622472 (2019).
Kruse, L. M., Gray, B. & Wright, R. W. Rehabilitation after anterior cruciate ligament reconstruction: A systematic review. J. Bone Jt. Surg. Am. 94(19), 1737–1748. https://doi.org/10.2106/JBJS.K.01246 (2012).
Filbay, S. R. & Grindem, H. Evidence-based recommendations for the management of anterior cruciate ligament (ACL) rupture. Best Pract. Res. Clin. Rheumatol. 33(1), 33–47. https://doi.org/10.1016/j.berh.2019.01.018 (2019).
van Grinsven, S., van Cingel, R. E., Holla, C. J. & van Loon, C. J. Evidence-based rehabilitation following anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 18(8), 1128–1144. https://doi.org/10.1007/s00167-009-1027-2 (2010).
Kakavas, G. et al. Periodization in anterior cruciate ligament rehabilitation: A novel framework. Med. Princ Pract. 30(2), 101–108. https://doi.org/10.1159/000511228 (2021).
Cheney, S., Chiaia, T. A., de Mille, P., Boyle, C. & Ling, D. Readiness to return to sport after ACL reconstruction: A combination of physical and psychological factors. Sports Med. Arthrosc. Rev. 28(2), 66–70. https://doi.org/10.1097/JSA.0000000000000263 (2020).
Lin, K. M., Boyle, C., Marom, N. & Marx, R. G. Graft selection in anterior cruciate ligament reconstruction. Sports Med. Arthrosc. Rev. 28(2), 41–48. https://doi.org/10.1097/JSA.0000000000000265 (2020).
Legnani, C., Ventura, A., Terzaghi, C., Borgo, E. & Albisetti, W. Anterior cruciate ligament reconstruction with synthetic grafts. A review of literature. Int. Orthop. 34(4), 465–471. https://doi.org/10.1007/s00264-010-0963-2 (2010).
Brown, M. J. & Carter, T. ACL allograft: Advantages and when to use. Sports Med. Arthrosc. Rev. 26(2), 75–78. https://doi.org/10.1097/JSA.0000000000000194 (2018).
McGuire, D. A. & Hendricks, S. D. Allograft tissue in ACL reconstruction. Sports Med. Arthrosc. Rev. 17(4), 224–233. https://doi.org/10.1097/JSA.0b013e3181c0cf8a (2009).
Dai, C. et al. Arthroscopic single-bundle anterior cruciate ligament reconstruction with six-strand hamstring tendon allograft versus bone-patellar tendon-bone allograft. Knee Surg. Sports Traumatol. Arthrosc. 24(9), 2915–2922. https://doi.org/10.1007/s00167-015-3569-9 (2016).
Barbour, S. A. & King, W. The safe and effective use of allograft tissue—an update. Am. J. Sports Med. 31(5), 791–797. https://doi.org/10.1177/03635465030310052801 (2003).
Jia, Z. Y. et al. Comparison of artificial graft versus autograft in anterior cruciate ligament reconstruction: A meta-analysis. BMC Musculoskelet. Disord. 18(1), 309. https://doi.org/10.1186/s12891-017-1672-4 (2017).
Grassi, A. et al. Does the type of graft affect the outcome of revision anterior cruciate ligament reconstruction? A meta-analysis of 32 studies. Bone Jt. J. 99(6), 714–723. https://doi.org/10.1302/0301-620X.99B6.BJJ-2016-0929.R2 (2017).
Xerogeanes, J. W. Quadriceps tendon graft for anterior cruciate ligament reconstruction: The graft of the future!. Arthroscopy 35(3), 696–697. https://doi.org/10.1016/j.arthro.2019.01.011 (2019).
Slone, H. S., Romine, S. E., Premkumar, A. & Xerogeanes, J. W. Quadriceps tendon autograft for anterior cruciate ligament reconstruction: A comprehensive review of current literature and systematic review of clinical results. Arthroscopy 31(3), 541–554. https://doi.org/10.1016/j.arthro.2014.11.010 (2015).
Mouarbes, D. et al. Anterior cruciate ligament reconstruction: A systematic review and meta-analysis of outcomes for quadriceps tendon autograft versus bone-patellar tendon-bone and hamstring-tendon autografts. Am. J. Sports Med. 47(14), 3531–3540. https://doi.org/10.1177/0363546518825340 (2019).
Diermeier, T. et al. Quadriceps tendon anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 28(8), 2644–2656. https://doi.org/10.1007/s00167-020-05902-z (2020).
Migliorini, F. et al. Quadriceps tendon autograft for primary ACL reconstruction: A Bayesian network meta-analysis. Eur. J. Orthop. Surg. Traumatol. 30(7), 1129–1138. https://doi.org/10.1007/s00590-020-02680-9 (2020).
Funding
Open Access funding enabled and organized by Projekt DEAL. The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
F.M.: literature search, data extraction, risk of bias assessment, conception and design, drafting, final approval; N.M.: supervision, revision, final approval; A.T.: writing, final approval; E.T.: literature search, data extraction, risk of bias assessment, final approval; F.H.: supervision, final approval; J.E.: drafting, final approval. All authors have agreed to the final version to be published and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Migliorini, F., Torsiello, E., Trivellas, A. et al. Bone-patellar tendon-bone versus two- and four-strand hamstring tendon autografts for ACL reconstruction in young adults: a Bayesian network meta-analysis. Sci Rep 13, 6883 (2023). https://doi.org/10.1038/s41598-023-33899-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-33899-1
- Springer Nature Limited