
Abstract
Quantitative body composition affects the prognosis of patients with Mycobacterium avium complex pulmonary disease (MAC-PD). However, whether the qualitative body composition obtained indirectly through computed tomography (CT) affects their prognosis is debatable. We retrospectively analyzed patients with MAC-PD who underwent non-contrast CT at MAC-PD diagnosis. The cross-sectional area of the erector spinae muscle (ESM area), the Hounsfield unit of the erector spinae muscle (ESM HU), and the cross-sectional area of subcutaneous fat (SQF area) were measured at the level of the first lumbar vertebra. Myosteatosis were defined below the median value of ESM HU for each sex. Of 377 patients, 45 (11.9%) died during the follow-up. Patients who died were older and had a lower ratio of females (33.3%). In body compositions, SQF area and ESM HU were lower in the patients who died. In multivariable analysis, a low ESM HU was associated with increased mortality (ESM HU adjusted hazard ratio [aHR] 0.95, 95% confidence interval [CI] 0.93–0.97) through body composition. SQF area revealed protective effects in MAC-PD patients with body mass index ≥ 18.5 kg/m2 (aHR 0.98, 95% CI 0.95–1.00). In conclusion, the decrease in ESM HU, which indirectly reflects myosteatosis, is associated with mortality in patients with MAC-PD.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
The incidence of Mycobacterium avium complex (MAC) pulmonary disease (MAC-PD), accounting for a large proportion of nontuberculous mycobacteria (NTM) pulmonary disease (NTM-PD), is continuously increasing1,2. As NTM-PD has high unsuccessful treatment outcome3 and mortality4 rates, it is essential to reduce modifiable risk factors in addition to medical treatment. Among the widely known modifiable risk factors5, low body mass index (BMI) affects NTM-PD development6 and mortality7. However, even with the same BMI, there can be variations in the ratio of muscle to fat. It's established that both muscle and fat exert independent impacts on the development8 and prognosis of NTM-PD9. Therefore, evaluating the influence of each patient's body composition becomes imperative. Furthermore, considering reduced survival rates among cancer patients and cirrhosis patients based on the distribution of fat, even with the same total body fat mass and percentage, it might be worth considering fat distribution in NTM-PD patients as well10,11.
Aging or inflammation-induced lipolysis can induce ectopic fat infiltration, leading to the presence of fat within the skeletal muscle. This condition is referred to as myosteatosis12. Through the utilization of computed tomography (CT) scans in NTM-PD diagnosis, it is possible to differentiate between muscle and fat13, enabling quantitative measurements14. Furthermore, muscle attenuation measured in Hounsfield units provides a non-invasive means to assess myosteatosis15. In two previous studies, the cross-sectional area of the erector spinae muscle (ESM area) and Hounsfield unit (HU) of the erector spinae muscle (ESM HU) were measured with CT to predict MAC-PD prognosis based on body composition9,16. However, as the results for ESM HUs are inconsistent, further research is necessary.
Thus, this study aimed to investigate the prognostic significance of myosteatosis and quantitative body composition measured at the first lumbar vertebra (L1) level using chest CT regarding the survival of patients with MAC-PD.
Results
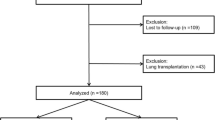
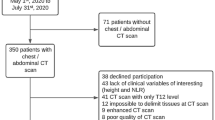
A retrospective cohort of 963 patients diagnosed with MAC-PD between 2005 and 2018 at the tertiary referral hospital was eligible for analysis. After excluding 586 people (received transplantation, follow-up period < 6 months, diagnosed with cancer, no CT image at diagnosis, inappropriate CT for measure body composition), 377 participants were included in the final analysis (Fig. 1).

Flow chart of participants with Mycobacterium avium complex pulmonary disease (MAC-PD). MAC, Mycobacterium avium complex; CT, computed tomography.
Baseline characteristics
Table 1 presents baseline characteristics of patients with MAC-PD in the entire group and subgroups according to sex. The females were younger (61.7 years vs. 68.6 years) and had better nutritional status represented by the prognostic nutritional index (PNI)17 than males. Acid-fast bacilli (AFB) positivity, CT scores, treatment times, and BMI did not statistically differ between males and females. However, individual body compositions differed. In females, the cross-sectional area of subcutaneous fat (SQF area) was > 70% higher than that in males based on the median value. In contrast, ESM area and ESM HU were low; therefore, the fat composition ratio was higher in females than that in males.
The different characteristics of survivors and deceased patients with MAC-PD are presented in Table 2. Of 377 patients with MAC-PD (mean age, 63.9 years), 45 (11.9%) died during the 4.5-year follow-up. Among the deceased patients, respiratory diseases (n = 18) were the primary cause of death, while other causes of death included sepsis (n = 5), cardiovascular diseases (n = 4), cerebrovascular diseases (n = 3), Alzheimer’s disease (n = 1), kidney diseases (n = 1), connective tissue diseases (n = 2), hematologic diseases (n = 2), and other diseases (n = 9). The group that died was older (74.1 years vs. 62.5 years) and had a higher percentage of males (66.7% vs. 27.1%) than the survivor group. Patients with MAC-PD in the group that died had a lower BMI, more underlying diseases, poor CT scores, more cavities measured using CT, and poor nutritional status than survivors. However, no differences were observed between the death and survivor groups in AFB positivity and treatment times. In body compositions, SQF area and ESM HU were lower in the group that died. However, the ESM area did not differ between both groups. In subgroup analysis, the differences in all the CT-measured body compositions were significant in females, but in males, SQF area and ESM area were significantly different between the survivor and deceased patient groups (Supplementary Tables S1–S2).
Correlation between each CT-measured body composition
We examined the correlation among the three measured body composition values (ESM area, ESM HU, and SQF area) and observed significant correlations between ESM area and ESM HU and SQF area and ESM HU in total participants, as illustrated in Fig. 2a–c. However, when analyzed by sex, a significant correlation was observed between SQF area and ESM HU, as well as between SQF area and ESM area (Fig. 2d–f).

Correlation analysis for each CT-measured body composition (a–c) and correlation analysis for each CT-measured body composition stratified by sex (d–f) were represented using scatter plots. ESM HU, L1 spine level of Hounsfield unit of the erector spinae muscle; HU, Hounsfield unit; ESM area, L1 spine level of the cross-sectional area of the erector spinae muscle; SQF area, L1 spine level of the cross-sectional area of subcutaneous fat.
Prognostic effect of CT-measured body composition, ESM area, ESM HU, and SQF area on mortality
Table 3 presents the Cox proportional hazard model analysis results evaluating the effect of each body composition value at diagnosis on all-cause mortality of patients with MAC-PD. Regarding the body composition, the SQF area and ESM HU in univariable analysis were associated with decreased mortality of patients with MAC-PD. Multivariable analysis was performed on three models. Model 1 was adjusted for age, sex, and BMI, model 2 was adjusted for sex and considered correlations among continuous variables (Age, BMI, PNI, ESM area, ESM HU, and SQF area) (Supplementary Table S3), and model 3 was adjusted for significant variables in the univariable analysis. In the multivariable analysis, ESM HU continuously had a significantly lower hazard of death. In model 1 and 3, a one-unit increase in ESM HU corresponded to an adjusted hazard ratio (aHR) of 0.95 (95% confidence interval [CI] 0.93–0.97). In model 2, the adjusted hazard ratio associated with a one-unit increase in ESM HU was 0.96 (95% CI 0.94–0.98).
In addition, the effect of ESM HU on the mortality of MAC-PD was consistent in the subgroup analysis according to sex. The aHR values for death in model 3 were 0.93 (95% CI 0.88–0.97, Supplementary Table S4) in males and 0.94 (95% CI 0.91–0.97, Supplementary Table S5) in females.
As body composition differences according to BMI groups were observed (Supplementary Table S6), subgroup analysis according to BMI was also performed. ESM HU had a significantly lower hazard of death (aHR 0.93, 95% CI 0.89–0.97) in the BMI < 18.5 kg/m2 group. ESM HU (aHR 0.92, 95% CI 0.88–0.97) and SQF area (aHR 0.98, 95% CI 0.95–1.00) were significant prognostic factors for death in the BMI ≥ 18.5 kg/m2 group (Supplementary Tables S7–S8).
Relation of myosteatosis with mortality
ESM HU was associated with MAC-PD mortality; therefore, we classified patients into two groups based on ESM HU: myosteatosis and non-myosteatosis groups. There was a difference in survival between the myosteatosis and non-myosteatosis groups. Patients with MAC-PD and myosteatosis had a lower survival probability than those without myosteatosis (p < 0.001, Fig. 3). In addition, the differences in survival rate according to myosteatosis in each subgroup according to sex and BMI were observed (Supplementary Fig. S1).

Kaplan–Meier curve stratified by myosteatosis in patients with MAC-PD. ESM HU, L1 spine level of Hounsfield unit of the erector spinae muscle; Myosteatosis, patients with MAC-PD who had < 40.54 HU in males and < 36.06 HU in females; Non-myosteatosis, patients with MAC-PD who had ≥ 40.54 HU in males and ≥ 36.06 HU in females.
Discussion
Few studies have shown the impact of the qualitative CT-measured body composition on the prognosis of patients with MAC-PD, and each finding is conflicting. In our study, myosteatosis—represented by a lower ESM HU—was associated with mortality in patients with MAC-PD independently of the other covariates, including sex and BMI. In addition, subcutaneous fat protected against mortality in patients with MAC-PD and BMI ≥ 18.5 kg/m2. There were different effects of fat tissue in skeletal muscles, which was the main factor in lowering the ESM HU18, and subcutaneous fat on mortality of patients with MAC-PD in our study.
Previous studies have revealed that obesity has a positive impact on the prognosis of chronic diseases, such as cancer19, chronic heart disease, and chronic obstructive pulmonary disease20,21. This phenomenon is known as the obesity paradox. However, it has been suggested that not only BMI but also various aspects of body composition such as muscle, fat mass, and myosteatosis have additional prognostic effects22,23,24. In NTM-PD, low BMI is a known risk factor for both its developing6 and mortality7,25. However, research on the impact of specific body composition, especially myosteatosis, on NTM-PD prognosis remains limited. During the aging process or inflammation-induced lipolysis, the redistribution of fat leads to lipid infiltration into skeletal muscles, resulting in intramyocellular lipids that possess distinct characteristics from subcutaneous fat12,18. It enhances the secretion of pro-inflammatory cytokines and can be associated with metabolic disorders, such as insulin resistance and inflammation12. Myosteatosis is also associated with reduced muscle strength, compromised physical performance, and decreased physical activity26,27,28. Therefore, early detection of myosteatosis is essential. In our result, myosteatosis was associated with a poor prognosis in MAC-PD, underscoring the importance of investigating myosteatosis in MAC-PD patients to consider early therapeutic interventions.
For the subcutaneous fat, similar to patients with cancer22, a protective effect in BMI ≥ 18.5 kg/m2 group was observed in our study. Subcutaneous adipose tissue has a higher rate of leptin secretion than other visceral adipose tissue29. Leptin is associated with the production of host-protecting cytokines, such as tumor necrosis factor-α and interleukin-1230. Therefore, in the BMI ≥ 18.5 kg/m2 group with a higher proportion of subcutaneous fat (Supplementary Table S6), the potential secretion of leptin against NTM might be associated with a protective effect on mortality in patients with MAC-PD.
Unlike previous studies9, the ESM area did not affect mortality in our study. We measured muscle mass through the ESM area at a specific level. However, even if muscle mass was measured in the same cross-sectional area, actual total body mass and estimated value differences may occur depending on muscle distribution or height. ESM area can be adjusted with height, weight, or BMI. However, it was not considered in our analysis because the variable could be estimated twice during statistical analysis, resulting in overfitting.
This study has several strengths. First, a low ESM HU at diagnosis was associated with increased mortality of patients with MAC-PD. Therefore, myosteatosis could be used to determine treatment initiation for early-stage patients before radiological deterioration. Determining treatment initiation in MAC-PD has always been controversial, and radiological changes, such as cavity development, are suggested markers of treatment initiation7. If myosteatosis could predict the mortality of patients with MAC-PD, it may be helpful to classify the group that needs preemptive treatment in advance when diagnosing MAC-PD. Second, our study suggests the possibility of adjuvant non-pharmacological treatment in MAC-PD. As myosteatosis is associated with a poor prognosis in patients with MAC-PD, prognosis improvement can be expected if there is a way to reduce myosteatosis. Previous studies have revealed that higher muscle attenuation is associated with increased muscle strength26, and exercise can decrease myosteatosis31. Therefore, exercise can be considered as one of non-pharmacological treatment to increase the ESM HU. To verify this, it is necessary to confirm the effect of physical activity and exercise on MAC-PD development or prognosis as a follow-up study.
Despite these strengths, this study has some limitations. First, this was a single-center study, and regional and national differences should be considered in interpreting the results. Second, we measured the body composition at diagnosis, and the CT-measured body composition values may change during follow-up. However, due to the limitations of retrospective studies, there was inadequate follow-up CT information. In future prospective studies, it is necessary to investigate the value of CT-measured body composition in the course of disease progression and whether this value is associated with prognosis. Third, we excluded the participants with malignancy co-morbidities. Given the prevalence of multiple co-morbidities in NTM-PD32, further analysis is warranted encompassing patients with diverse co-morbidities. Finally, when determining myosteatosis, the median value of ESM HU was considered as the cut-off in the patient group. However, to determine a statistically accurate cut-off value, comparing the ESM HU between the control and deceased groups is necessary. Therefore, it is necessary to identify the cut-off value that will be the standard ESM HU in future studies.
In conclusion, our study revealed that a low ESM HU, which indirectly reflects myosteatosis, was associated with increased mortality in patients with MAC-PD. Therefore, it is necessary to consider the impact of qualitative body composition as well as quantitative body composition when evaluating MAC-PD prognosis.
Methods
Ethical standards
The study protocol was reviewed and approved by the Institutional Review Board of the Severance Hospital Ethics Committee (IRB Approval Number: 4–2022-0523). Informed consent was waived by the Institutional Review Board of the Severance Hospital Ethics Committee. All methods were performed in accordance with the Declaration of Helsinki.
Study population
Patients with MAC-PD diagnosed based on 2007 American Thoracic Society and Infectious Disease Society of America guidelines were eligible for this study13. We excluded patients with co-morbidities, such as transplantation and malignancies, which have the potential to significantly influence mortality, those with a short follow-up duration (< 6 months), those without a CT image at diagnosis, and those with inappropriate CT scans for measure body composition. Inappropriate CT included motion artifacts within the images, a slice thickness exceeding 5 mm, inadequate inclusion of the L1 level, absence of available soft kernel-reconstructed images, and a lack of available noncontrast CT images33.
Data collection and definition
Data on clinico-demographic factors, including age, sex, height, weight, BMI, smoking history, medical history, AFB smear and culture, laboratory findings and chest CT findings at the time of diagnosis, and anti-MAC treatment history were collected. The primary clinical outcome was all-cause mortality during the follow-up. The death outcome was confirmed by collecting medical records and referring to Statistics Korea for data on the causes of death between 2005 and 2018. Myosteatosis is fat infiltration into the skeletal muscles and was defined as the ESM HU value. Less than the median value of ESM HU led to classification as myosteatosis and more than the median value of ESM HU to classification as non-myosteatosis. Owing to the difference in ESM HU distribution between males and females, the median of ESM HU criterion was applied differently according to sex.
Radiologic measurement
Body composition was measured using non-contrast chest CT before and after 3 months of diagnosis with MAC-PD. Chest CT scans were obtained from the level of the supraclavicular fossae to the adrenal glands under an inspiratory breath-hold with the following scanning parameters: tube voltage of 120 kVp, reference tube current of 100 mAs, average pitch of 1, and volume CT dose index < 7.0 mGy. After scanning, axial images were reconstructed using a slice 1 mm thick and a slice increment of 1 mm with a medium-smooth convolution kernel. Thereafter, CT images were transferred to a software system (Aquarius iNtuition; Version 4.4.11, TeraRecon, Durham, North Carolina, The United States of America) for analysis. The program was used to measure three body compositions: ESM area, ESM HU, and SQF area. After reconstructing the CT images at 3 mm slice thickness and intervals, a single evaluator measured body compositions at the middle of the L1 vertebra. For the erector spinae muscle, manual segmentation was done using a region of interest drawn along the muscle outline avoiding the edges to reduce partial volume averaging from the muscle-fat interface. Subsequently, based on the area histogram, pixels with the predefined threshold of − 29 to + 150 HU were incorporated for the analysis of the ESM. Semi-automatic segmentation was performed for the subcutaneous fat with a threshold of − 190 to − 30 HU (Fig. 4).

Computed tomography images show how body compositions are measured. (a) An image measuring the cross-sectional area of subcutaneous fat at L1 spine level (blue area). (b) An image measuring the cross-sectional area and Hounsfield unit of erector spinae muscles at L1 spine level (yellow area surrounded by red lines indicates muscle with a threshold of − 29 to + 150 HU; red and green areas indicate intermuscular fat with − 200 to − 100 HU and − 100 to − 30 HU, respectively).
Another evaluator measured the CT score, which is the variable related to the severity of NTM-PD, according to a prior published scoring system34. A total CT score of 30 was allocated to determine each patient's overall extent of lung lesions. Both readers were blinded to the clinical information, including medical history and outcomes.
Statistical analysis
Categorical variables are presented as numbers and percentages. Continuous variables with normal distribution are presented as mean and standard deviation, and those with non-normal distribution are presented as median (interquartile range [IQR]). The Chi-square and Fisher’s exact tests were used to compare categorical variables. In contrast, the Student’s t-test and Mann–Whitney U-test were used to compare continuous variables. We conducted Cox proportional hazard regression analysis to assess the hazard ratio of body composition in relation to mortality of patients with MAC-PD. The log-rank test was conducted to compare the mortality between the myosteatosis and non-myosteatosis groups. A two-tailed statistical significance was defined as a p-value < 0.05. SPSS (Version 26.0, IBM corporation, Armonk, New York, The United States of America) and R software (version × 64 4.2.1, R Foundation for Statistical Computing, Vienna, Austria) were used to perform all statistical analyses.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Kumar, K. & Loebinger, M. R. Nontuberculous mycobacterial pulmonary disease: Clinical epidemiologic features, risk factors, and diagnosis: The nontuberculous mycobacterial series. Chest 161, 637–646. https://doi.org/10.1016/j.chest.2021.10.003 (2022).
Boyle, D. P., Zembower, T. R., Reddy, S. & Qi, C. Comparison of clinical features, virulence, and relapse among Mycobacterium avium complex species. Am. J. Respir. Crit. Care Med. 191, 1310–1317. https://doi.org/10.1164/rccm.201501-0067OC (2015).
Aliberti, S. et al. Real-life evaluation of clinical outcomes in patients undergoing treatment for non-tuberculous mycobacteria lung disease: A ten-year cohort study. Respir. Med. 164, 105899. https://doi.org/10.1016/j.rmed.2020.105899 (2020).
Fleshner, M. et al. Mortality among patients with pulmonary non-tuberculous mycobacteria disease. Int. J. Tuberc. Lung Dis. 20, 582–587. https://doi.org/10.5588/ijtld.15.0807 (2016).
Hayashi, M. et al. Prognostic factors of 634 HIV-negative patients with Mycobacterium avium complex lung disease. Am. J. Respir. Crit. Care Med. 185, 575–583. https://doi.org/10.1164/rccm.201107-1203OC (2012).
Song, J. H., Kim, B. S., Kwak, N., Han, K. & Yim, J. J. Impact of body mass index on development of nontuberculous mycobacterial pulmonary disease. Eur. Respir. J. https://doi.org/10.1183/13993003.00454-2020 (2021).
Jhun, B. W. et al. Prognostic factors associated with long-term mortality in 1445 patients with nontuberculous mycobacterial pulmonary disease: A 15-year follow-up study. Eur. Respir. J. https://doi.org/10.1183/13993003.00798-2019 (2020).
Kartalija, M. et al. Patients with nontuberculous mycobacterial lung disease exhibit unique body and immune phenotypes. Am. J. Respir. Crit. Care Med. 187, 197–205. https://doi.org/10.1164/rccm.201206-1035OC (2013).
Asakura, T. et al. Quantitative assessment of erector spinae muscles in patients with Mycobacterium avium complex lung disease. Respir. Med. 145, 66–72. https://doi.org/10.1016/j.rmed.2018.10.023 (2018).
Aleixo, G. F. P. et al. Myosteatosis and prognosis in cancer: Systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 145, 102839. https://doi.org/10.1016/j.critrevonc.2019.102839 (2020).
Ebadi, M. et al. Myosteatosis in cirrhosis: A Review of diagnosis, pathophysiological mechanisms and potential interventions. Cells https://doi.org/10.3390/cells11071216 (2022).
Li, C. W. et al. Pathogenesis of sarcopenia and the relationship with fat mass: Descriptive review. J. Cachexia Sarcopenia Muscle 13, 781–794. https://doi.org/10.1002/jcsm.12901 (2022).
Griffith, D. E. et al. An official ATS/IDSA statement: Diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am. J. Respir. Crit. Care Med. 175, 367–416. https://doi.org/10.1164/rccm.200604-571ST (2007).
Cho, Y. H. et al. Association of chest CT-based quantitative measures of muscle and fat with post-lung transplant survival and morbidity: A single institutional retrospective cohort study in Korean population. Korean J. Radiol. 20, 522–530. https://doi.org/10.3348/kjr.2018.0241 (2019).
Goodpaster, B. H., Kelley, D. E., Thaete, F. L., He, J. & Ross, R. Skeletal muscle attenuation determined by computed tomography is associated with skeletal muscle lipid content. J. Appl. Physiol. 1985(89), 104–110. https://doi.org/10.1152/jappl.2000.89.1.104 (2000).
Akahori, D. et al. Body composition changes successfully classify prognosis in patients with Mycobacterium avium complex lung disease. J. Infect 79, 341–348. https://doi.org/10.1016/j.jinf.2019.07.014 (2019).
Moon, S. W. et al. Impact of prognostic nutritional index on outcomes in patients with Mycobacterium avium complex pulmonary disease. PLoS ONE 15, e0232714. https://doi.org/10.1371/journal.pone.0232714 (2020).
Wronska, A. & Kmiec, Z. Structural and biochemical characteristics of various white adipose tissue depots. Acta Physiol. (Oxf.) 205, 194–208. https://doi.org/10.1111/j.1748-1716.2012.02409.x (2012).
Strulov Shachar, S. & Williams, G. R. The obesity paradox in cancer-moving beyond BMI. Cancer Epidemiol. Biomark. Prev. 26, 13–16. https://doi.org/10.1158/1055-9965.EPI-16-0439 (2017).
Guo, Y. et al. Body mass index and mortality in chronic obstructive pulmonary disease: A dose-response meta-analysis. Med. (Baltim.) 95, e4225. https://doi.org/10.1097/MD.0000000000004225 (2016).
Giri Ravindran, S. et al. The obesity paradox in chronic heart disease and chronic obstructive pulmonary disease. Cureus 14, e25674. https://doi.org/10.7759/cureus.25674 (2022).
Ebadi, M. et al. Subcutaneous adiposity is an independent predictor of mortality in cancer patients. Br. J. Cancer 117, 148–155. https://doi.org/10.1038/bjc.2017.149 (2017).
Caan, B. J. et al. Explaining the obesity paradox: The association between body composition and colorectal cancer survival (C-SCANS study). Cancer Epidemiol. Biomark. Prev. 26, 1008–1015. https://doi.org/10.1158/1055-9965.EPI-17-0200 (2017).
Lee, C. M. & Kang, J. Prognostic impact of myosteatosis in patients with colorectal cancer: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 11, 1270–1282. https://doi.org/10.1002/jcsm.12575 (2020).
Kim, H. J. et al. BACES score for predicting mortality in nontuberculous mycobacterial pulmonary disease. Am. J. Respir. Crit. Care. Med. 203, 230–236. https://doi.org/10.1164/rccm.202004-1418OC (2021).
Goodpaster, B. H. et al. Attenuation of skeletal muscle and strength in the elderly: The health ABC study. J. Appl. Physiol. 1985(90), 2157–2165. https://doi.org/10.1152/jappl.2001.90.6.2157 (2001).
Ahn, H. et al. Updated systematic review and meta-analysis on diagnostic issues and the prognostic impact of myosteatosis: A new paradigm beyond sarcopenia. Ageing Res. Rev. 70, 101398. https://doi.org/10.1016/j.arr.2021.101398 (2021).
Visser, M. et al. Muscle mass, muscle strength, and muscle fat infiltration as predictors of incident mobility limitations in well-functioning older persons. J. Gerontol. A Biol. Sci. Med. Sci. 60, 324–333. https://doi.org/10.1093/gerona/60.3.324 (2005).
Van Harmelen, V. et al. Leptin secretion from subcutaneous and visceral adipose tissue in women. Diabetes 47, 913–917. https://doi.org/10.2337/diabetes.47.6.913 (1998).
Raso, G. M. et al. Leptin potentiates IFN-gamma-induced expression of nitric oxide synthase and cyclo-oxygenase-2 in murine macrophage J774A.1. Br. J. Pharmacol. 137, 799–804. https://doi.org/10.1038/sj.bjp.0704903 (2002).
Ramirez-Velez, R., Ezzatvar, Y., Izquierdo, M. & Garcia-Hermoso, A. Effect of exercise on myosteatosis in adults: A systematic review and meta-analysis. J. Appl. Physiol. 1985(130), 245–255. https://doi.org/10.1152/japplphysiol.00738.2020 (2021).
Lee, S. W., Park, Y., Kim, S., Chung, E. K. & Kang, Y. A. Comorbidities of nontuberculous mycobacteria infection in Korean adults: Results from the National Health Insurance Service-National Sample Cohort (NHIS-NSC) database. BMC Pulm. Med. 22, 283. https://doi.org/10.1186/s12890-022-02075-y (2022).
Fuchs, G. et al. Quantifying the effect of slice thickness, intravenous contrast and tube current on muscle segmentation: Implications for body composition analysis. Eur. Radiol. 28, 2455–2463. https://doi.org/10.1007/s00330-017-5191-3 (2018).
Kim, H. S. et al. Serial CT findings of Mycobacterium massiliense pulmonary disease compared with Mycobacterium abscessus disease after treatment with antibiotic therapy. Radiology 263, 260–270. https://doi.org/10.1148/radiol.12111374 (2012).
Funding
This study was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant Number: HC21C0015). The funding source had no role in the study process, including the study design, data collection, statistical analysis, or data interpretation.
Author information
Authors and Affiliations
Contributions
Y.A.K. and H-J.L. contributed to conceptualization and methodology. Y.A.K. and E.C. contributed to writing of original manuscript and statistical analysis. H-J.L, Y.P, S.Y.K. contributed to data acquisition. M.S.P and Y.S.K contributed data interpretation. All authors contributed to review and editing.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chung, E., Park, Y., Kim, S.Y. et al. Myosteatosis as a prognostic factor of Mycobacterium avium complex pulmonary disease. Sci Rep 13, 13680 (2023). https://doi.org/10.1038/s41598-023-40984-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-40984-y
- Springer Nature Limited