
Abstract
This study aimed to investigate the impact of ocular demodicosis on dry eye disease (DED) and meibomian gland dysfunction (MGD) across different age populations: young (20 to < 40), middle-aged (40 to < 60), and elderly (≥ 60), based on the retrospective medical chart review. In each age subgroup, Demodex infestation and its count were correlated with clinical parameters of DED and MGD. Among the total of 351 subjects, 52.7% had ocular demodicosis, with a mean of 2.31 ± 1.39 mites per four eyelashes (0.58 per lash) in a unilateral eye. In the age subgroup 1 (age < 40; N = 44), subjects with Demodex had significantly higher meibum quality grades. In subgroup 2 (40 ≤ age < 60; N = 122), subjects with Demodex had higher ocular surface disease index scores and higher MG expressibility grades. However, in subgroup 3 (age ≥ 60; N = 185), demographics and all parameters did not differ according to Demodex infestation. Moreover, the number of mites did not correlate with MGD severity in any of the subgroups. In conclusion, age may act as a significant confounding factor in the relationship between ocular Demodex infestation and clinical features of DED and MGD, despite older patients aged 60 years and above being at a higher risk of Demodex infestation and experiencing more severe MGD.
Similar content being viewed by others


Introduction
Demodex mites are parasitic creatures measuring 150–350 μm in length that are commonly found in the eyelid area. While there are several Demodex species, Demodex folliculorum (D. folliculorum) and Demodex brevis (D. brevis) inhabit the human body1. The former resides in eyelash follicles, while the latter is found in meibomian and sebaceous glands of the eyelashes, particularly on the ocular surface2. The infestation of these mites has been linked to conditions such as anterior blepharitis, meibomian gland dysfunction (MGD), and even corneal abnormalities3.
D. folliculorum has been identified as a vector for bacteria, fungi, and viruses4, and may directly penetrate cell membrane to feed, potentially inducing allergies5. Moreover, Demodex infestation may cause superficial corneal neovascularization, phlyctenule-like lesions, corneal infiltration, and opacity6,7,8,9. A recent study, conducted by ocular surface disease experts agreed that itching is the most common symptom in Demodex blepharitis10.
The relationship between Demodex infestation and meibomian gland health remains debated, with studies suggesting both associations and non-associations. A study indicated that ocular Demodex infestation might contribute to ocular surface discomfort, inflammation, and meibomian gland dropout in MGD patients5. Conversely, a study found no significant association between the expressibility and drop-out of meibomian glands and Demodex infestation3. Additionally, D. brevis, which usually inhabits the meibomian glands, has been suggested as a possible cause of repeated chalazia and hordeola rather than MGD in the posterior eyelid11. A recent randomized clinical trial used lotilaner ophthalmic solution to treat Demodex blepharitis, using the cure of collarette as a primary end point, a clinical marker of Demodex-associated anterior blepharitis12.
Earlier studies have shown that the prevalence of ocular Demodex increases with age13,14,15, and one study reported a demodicosis frequency of 77% in individuals aged over 70 years, compared to 8% in those aged 25 years or younger16. Furthermore, it was observed that the higher prevalence of ocular Demodex in elderly patients (41–70 years) was associated with more severe MGD compared to younger patients (18–40 years)x15. However, the pathogenic role of Demodex in MGD is remains controversial, it is recognized that aging could be a significant confound both Demodex infestation and MGD and/or DED, which are age-related conditions.
To assess the effect of age, it is needed to divide chronological age into several periods more than two. Therefore, we divided the adult participants into traditional three age subgroups17: young (20 to < 40), middle (40 to < 60), and old age (≥ 60) to specifically assess the effect of age. In this study, we investigated the prevalence of ocular Demodex in a large number of patients (N = 351) and assessed age-related differences in the association between Demodex infestation and MGD profiles, as well as clinical DED parameters.
Results
Demographics, MMP-9, and clinical parameters of DED
A total of 351 subjects were included in the study. Among them, 166 subjects were categorized as the "No Demodex group," showing no Demodex infestation, while 185 subjects were part of the "Demodex group," with one or more Demodex mites (2.31 ± 1.39) per four epilated eyelashes in a single eye. The average number of mites per 4 eyelashes in a unilateral eye within the complete study population (N = 351) was recorded as 1.22 ± 1.53.
Comparing the demographic details, the Demodex group had an average age of 62.0 ± 12.5 years, significantly higher than the No Demodex group's average age of 55.4 ± 15.5 years (p < 0.001, Table 1). There was no significant difference in the percentage of females between the two groups (66.9% in the No Demodex group and 71.0% in the Demodex group, p = 0.493, Table 1). Regarding clinical parameters of DED, such as the ocular surface disease index (OSDI) score, tear matrix metalloproteinase (MMP)-9 grades, tear osmolarity (Tosm), Sjogren's International Collaborative Clinical Alliance (SICCA) ocular staining score (OSS), tear break-up time (BUT), and tear secretion measured by Schirmer I without anesthesia, no significant differences were observed between the two groups (Table 1). However, the MGD profile grades, including MG expressibility and meibum quality, were worse in the Demodex group (1.63 ± 0.58 and 1.83 ± 0.63, respectively) than in the No Demodex group (1.48 ± 0.64 and 1.55 ± 0.81, respectively; p = 0.018 and p < 0.001, respectively, Table 1).
Furthermore, the Demodex count exhibited positive correlations with age (rs = 0.240, p < 0.001), MG expressibility (rs = 0.144, p = 0.008), and meibum quality grades (rs = 0.180, p = 0.001, Table 2). However, no significant correlations were found between the number of mites and other clinical parameters of DED.
Prevalence of ocular Demodex in different age subgroups
Given the parallel increase in MGD severity and Demodex count with aging (as seen in Table 2), the total subjects were divided into three age-based subgroups: subgroup 1 (age < 40), subgroup 2 (40 ≤ age < 60), and subgroup 3 (age ≥ 60). The prevalence of ocular Demodex in these subgroups was 34.1%, 42.6%, and 63.8%, respectively (Table 3). Subgroup 3 showed a significantly higher prevalence of Demodex compared to subgroups 1 and 2 (p < 0.001 and p < 0.001, respectively, Table 3). The mean number of Demodex mites was also highest in subgroup 3 (1.54 ± 1.63) and significantly lower in subgroup 1 (0.59 ± 0.95, p < 0.001) and subgroup 2 (0.99 ± 1.47, p = 0.002, Table 3).
Differences in demographic and clinical parameters of DED with and without Demodex infestation across different age subgroups
In subjects under 40 years old (subgroup 1), demographics and clinical parameters of DED, except for meibum quality grade, did not differ significantly based on the presence of Demodex infestation. The severity grade of meibum quality was significantly higher (2.00 ± 0.71) in subjects with Demodex compared to those without Demodex (0.96 ± 0.86, p = 0.001, Table 4).
For subjects aged 40–59 years old (subgroup 2), the OSDI score and MG expressibility grade in those with Demodex infestation were significantly higher compared to those without Demodex (45.2 ± 17.7 vs. 37.7 ± 20.2, p = 0.042; 1.57 ± 0.57 vs. 1.33 ± 0.62, p = 0.021, respectively, Table 5).
However, in subjects aged 60 or above, all demographics and clinical parameters of DED did not show significant differences based on Demodex infestation (Table 6).
Association of Demodex count with MGD severity grades and OSDI Scores
The count of Demodex mites did not exhibit a significant correlation with the severity grades of MG expressibility and meibum quality, and OSDI scores in the entire population of subjects with ocular Demodex infestation. Furthermore, no correlation was observed with either grade and score when data was categorized by age (Table 7).
Discussion
Several prior studies have established correlations between ocular Demodex infestation and conditions such as anterior blepharitis, MGD, chalazia, and keratoconjunctivitis11,14,18. The prevalence of ocular demodicosis and the count of infested Demodex mites have been shown to increase with age13,15, and DED is widespread, affecting 5–50% of the global population19. A significant portion of DED cases is attributed to MGD20. Given the well-established influence of aging on DED and MGD development21, we explored whether the higher prevalence of Demodex infestation in older individuals significantly contributes to DED and MGD in elderly populations. Surprisingly, our findings indicate that ocular demodicosis in those over 60 years old may not be linked to the severity of MGD and DED, despite the elevated prevalence of ocular Demodex and mite counts in comparison to younger individuals.
Conversely, ocular demodicosis seemed to influence meibum quality negatively in subjects below 40 years old. As indicated by Liang et al.11, D. brevis, typically residing in meibomian glands, was more common among younger patients with recurring chalazia and hordeola. Furthermore, MGD was detected in 90% of patients with D. brevis under 35 years, and it exhibited a significant correlation with keratitis22. Although this study observed worsened meibum quality in individuals under 40 years old with Demodex infestation, the subjective discomfort, as measured by OSDI scores, did not show significant differences between those with and without ocular demodicosis. Previous research also noted a connection between Demodex infestation and meibum quality in young patients, without a corresponding difference in OSDI scores, consistent with our findings15.
Gao et al. first investigated lipidomic changes associated with Demodex occurrence and they discovered that the levels of (O-acyl)-ω-hydroxy fatty acids (OAHFAs) were elevated in young adults aged 18–40 with ocular demodicosis, employing a liquid chromatography-mass spectrometry system23. This finding is intriguing, as OAHFA is recognized for its role in stabilizing the tear film through the creation of an interface between the non-polar lipid sublayer and the aqueous phase layer24,25. While this is a hypothetical explanation, it is suggested that the meibomian gland may adaptively adjust the levels of OAHFAs to alleviate ocular surface discomfort caused by Demodex mites23. Similarly, the potential contribution of ocular demodicosis to ocular discomfort has yielded inconsistent and controversial results across various studies. For instance, symptom profiles did not significantly differ between individuals with and without Demodex when evaluated using the Dry Eye Questionnaire 5 and OSDI26.
In this investigation, ocular demodicosis was linked to a more pronounced level of MG expressibility and elevated OSDI scores among middle-aged individuals aged over 40 but under 60 years. Ayyildiz et al. observed a similar pattern, demonstrating a significant correlation between OSDI scores and Demodex infestation in individuals who were initially diagnosed with DED and fell within the age range of 40–68 years27. This aligns with findings from the Hirado-Takushima Study conducted in Japan, which reported a substantial increase in the prevalence of MGD during the fifth decade of life, surging to 21.6% compared to the 5.6% rate in the fourth decade.According to the Hirado-Takushima Study in Japan28, the prevalence of MGD in the 5th decade of age abruptly elevated to 21.6% compared to that in the 4th decade, which was 5.6%.
Among elderly individuals (aged ≥ 60 years), no correlations between ocular demodicosis and any parameters were observed in this study. This contrasts with the findings of a study by Sun et al.15, who categorized their study population using a cutoff of 40 years and discovered that elderly subjects (aged 41–70 years) with Demodex infestation exhibited more severe OSDI scores, lower fluorescein tear film BUT, increased corneal fluorescein staining, higher MG dropout, MG orifice plugging, abnormal lid margins, and elevated MG expression compared to those without Demodex15. Additionally, they proposed that the greater number of mites and possibly the prolonged duration of ocular demodicosis might contribute to the heightened susceptibility of the ocular surface's deterioration caused by Demodex in their study15. In fact, while the prevalence of ocular demodicosis was 51.5% in their study involving 202 Chinese subjects15, akin to the prevalence of 52.7% in our study involving the Korean population (Table 1), the average number of Demodex mites per patient was notably higher at 5.36 ± 6.20 per 12 eyelashes (0.45 mites per an epilated eyelash)15, compared to 0.30 mites per lash in our study. Furthermore, the number of mites in the Chinese elderly population with ocular demodicosis, defined as individuals over 40 years, was even more substantial at 10.64 ± 7.50 per 12 lashes (0.89 mites/lash)15, surpassing the 2.37 ± 1.44 per 4 lashes (0.59 mites/lash) in our study for individuals with ocular demodicosis aged 60 years or older. Cheng et al. reported 4.2 ± 3.9 mites per 8 eyelashes (0.53 mites/lash) in a Demodex-positive population with 68.9% prevalence of ocular demodicosis26, similar to the 2.31 ± 1.39 mites per 4 eyelashes (0.58 mites/lash) in our study, and observed no differences in OSDI scores between subjects with and without Demodex infestation26. In contrast, the Caucasian population demonstrated a mean of only 0.2 mites per epilated lash, and neither OSDI scores nor the comorbid MGD proportion were elevated in conjunction with ocular Demodex infestation3. In summary, we suggest that the varying mite counts among elderly subjects from different races and countries could play a substantial role in influencing changes in DED and/or MGD-related parameters.
Interestingly, within the elderly population, no correlation was observed between Demodex count and OSDI score, as evident from the data presented in Table 7 of this study. Furthermore, among subjects with Demodex infestation, OSDI scores did not exhibit significant differences across the three age subgroups (details not presented). Notably, typical symptoms associated with Demodex blepharitis, such as itching and redness10, did not find comprehensive representation in the OSDI questionnaire. The OSDI primarily addresses matters like photophobia, pain, sensations of foreign bodies, and blurring, which might not fully encapsulate the true symptoms of ocular demodicosis in the elderly subgroup.
We propose an alternative explanation: the chronicity of ocular demodicosis, DED, and/or MGD might trigger compensatory stress-relieving signals both physically and psychologically, similar to what is observed in Sjogren’s syndrome, a representative chronic condition29. This mechanism could involve the desensitization or inhibition of polymodal nociceptors due to prolonged or repeated activation30 caused by long-lasting but not severe inflammatory stimuli induced by demodicosis14. This hypothesis is supported by the predominance of Demodex-induced keratitis in the young population22 which aligns with our proposed mechanism. Additionally, in younger patients, the proportion of D. brevis is higher than that of D. folliculorum, which is associated with repeated hordeola and chalazia11. Definite signs of demodicosis in young individuals, such as keratitis, hordeolum, and chalazion, may be easily linked to complaints of subjective ocular surface discomfort, even with a smaller number of Demodex than the elderly.
Our study's findings are subject to limitations arising from its retrospective design. Furthermore, our investigation did not uncover morphological and structural changes of meibomian glands using meibography. Additionally, we opted not to distinguish between D. folliculorum and D. brevis throughout our analyses. Although prior research has indicated that these two species cause blepharitis in distinct locations, a study highlighted that chronic blepharitis linked to D. folliculorum could impact ocular surface function, leading to a range of ocular signs, symptoms, and contributing to MGD-related dry eye and a higher incidence of chalazion31. Consequently, we chose to combine both species for correlational analysis with clinical parameters. However, the exact proportion of D. folliculorum and D. brevis within our cohort remains unknown. Additionally, the retrospective inclusion of hospital-based patients for assessing subjective symptoms might introduce selection bias. Therefore, it is essential to exercise cautious interpretation before concluding that ocular demodicosis, particularly in the elderly population, does not significantly prompt ocular surface discomfort and DED and/or MGD.
For the tear BUT estimation, we utilized the standard strip method instead of employing the quantified liquid dye drop technique. Although it was known that the standard strip method exhibited high test sensitivity and specificity in discriminating between aqueous tear deficiency DED and MGD compared to normal conditions, and the standard strip method might not differ significantly from the liquid dye instillation method32, the tear BUT estimation using fluorescein dye with a fixed volume and concentration, or through non-invasive BUT estimation, would be a better method to establish the relationship between tear film instability and ocular demodicosis.
To our current knowledge, no prior study has examined MGD and DED parameters in relation to ocular Demodex infestation across three distinct age subgroups: the young-aged, middle-aged, and old-aged, categorized with age cutoffs of 40 and 60 years. In conclusion, ocular demodicosis did not exhibit an association with the severity of MGD and DED in patients aged over 60 years. Consequently, it is essential to approach the interpretation of Demodex mite presence in the eyelids of elderly individuals with MGD or DED as a potential pathogenic factor with caution. Similarly, careful consideration is necessary when contemplating Demodex irradiation treatment decisions.
In summary, it is imperative to acknowledge that age can manifest as a noteworthy confounding factor within the context of the correlation between ocular Demodex infestation and the clinical attributes of both DED and MGD. This phenomenon persists despite the higher susceptibility of individuals aged 60 years and older to Demodex infestation, as well as their propensity to encounter more pronounced manifestations of MGD.
Methods
This study was a retrospective cross-sectional comparative cohort study. The whole process properly followed the tenets of the Declaration of Helsinki. The research protocol received approval from the Chung-Ang University Hospital Institutional Review Board (IRB), and considering the retrospective nature of the study design, the requirement for informed consent was waived by the IRB (Approval No. 2011-006-19339).
Subjects
We identified consecutive 351 individuals who were referred to our institute’s dry eye disease (DED) clinic due to ocular surface discomfort and subsequently underwent examinations for clinical parameters related to DED and meibomian gland dysfunction (MGD), as well as diagnostic testing for ocular demodicosis between September 2019 and December 2020. Evaluation for ocular demodicosis was routinely conducted for all patients at our DED clinic who experienced ocular surface discomfort. We excluded subjects who had a systemic immunologic disease, including Sjogren’s syndrome and allergic disease. Additionally, individuals with pterygium were excluded. We also excluded those who were under systemic immune-related treatments or were using topical administration of anti-inflammatory eye drops or anti-glaucomatous eye drops. Furthermore, participants who had worn contact lenses within the previous three months were excluded, as were those who had undergone ocular surgery within the previous six months.
All patients were classified into three distinct age subgroups according to their age: subgroup 1 (age < 40), subgroup 2 (40 ≤ age < 60), and subgroup 3 (age ≥ 60).
Study design
Our study design, based on a retrospective medical chart review, was as follows:
-
1.
Compare demographics and clinical parameters of DED and MGD between subjects with and without ocular demodicosis among all subjects.
-
2.
Correlate age and clinical parameters of DED and MGD with the number of Demodex mites among all subjects.
-
3.
Compare the prevalence of ocular demodicosis and the number of Demodex mites between subjects in each age subgroup.
-
4.
Compare of demographics and clinical parameters of DED and MGD between subjects with and without ocular demodicosis in each age subgroup.
-
5.
Correlate the number of Demodex mites with MGD severity grades only in subjects with Demodex infestation in each age subgroup.
Examination for ocular Demodex infestation
In our investigation, we thoroughly examined a total of eight eyelashes (four lashes per eye) for each patient. This examination was conducted under a slit-lamp microscope. From both the upper and lower lids, we extracted two eyelashes—specifically, one from each half of each lid. Following the method proposed by Gao et al.33, we prioritized lashes exhibiting cylindrical dandruff, also referred to as “sleevs”. These individual lashes were placed onto a slide and covered with a coverslip. To facilitate examination, a 20 μL droplet of saline was gently applied to the coverslip's edge using a pipette. Subsequently, the specimens were meticulously assessed under an optical microscope set at a magnification of 400×. During this examination, Demodex mite counts were meticulously documented for each eye separately.
For analyses, the eye with the greater count of Demodex mites was chosen to avoid duplicate reflection of OSDI scores within a subject. In instances where the mite count was the same in both eyes, one eye was chosen at random.
DED parameters and MGD severity profiles
As part of our evaluation of DED parameters, we systematically assessed the following factors in the specified sequence: tear osmolarity (Tosm), levels of tear matrix metalloproteinase (MMP)-9, tear secretion through Schirmer I without anesthesia, tear break-up time (BUT), Sjogren’s International Collaborative Clinical Alliance (SICCA) ocular staining score (OSS), corneal erosion scores according to the National Eye Institute/Industry (NEI) grading scale, expressibility of the meibomian glands (MG), and quality of the secreted meibum. Furthermore, to gauge the subjective ocular symptoms of DED and their impact on vision-related function, we employed the ocular surface disease index (OSDI) questionnaire34. The assessment for ocular Demodex infestation was conducted after the comprehensive evaluation of DED and MGD.
Tosm was assessed using an I-PEN osmometer (I-MED Pharma Inc., Montreal, QC, Canada). To perform the measurement, a single-use disposable sensor (SUS) was inserted into the I-PEN device. Patients were instructed to open their eyes, and the tip of the SUS was gently placed at a 30°–45° angle, directly onto the palpebral conjunctiva on the inner side of the retracted lower eyelid, ensuring good contact with the palpebral conjunctiva's surface. After maintaining this position for a few seconds, the handheld osmolarity system emitted an audible beep and presented the osmolarity reading in milliosmoles per liter on its LCD screen35.
The tear MMP-9 test was conducted using InflammaDry (Quidel, San Diego, CA, USA), and we followed the guidelines outlined in the product documentation36. To collect tear fluid, a sterile sample collector was gently applied to various areas along the lower palpebral conjunctiva. Subsequently, the collected tear fluid was placed into the immunoassay test cassette. After activating the solution with buffer for 20 s, we verified the intensity of the red line within a designated readout window. In order to assess the diagnostic significance of the MMP-9 assay, we analyzed the results employing a 5-scale grading method. This grading system involved evaluating the depth of the red readout band observed during on-site inspection of MMP-9. Grades were assigned as follows: grade 0 indicating a negative result, grade 1 indicating a trace result, grade 2 indicating a weak positive result, grade 3 indicating a positive result, and grade 4 indicating a strong positive result. These gradings were determined based on a standardized system of photographs that had been established previously37.
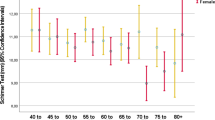
Tear secretion was assessed through the Schirmer I test, a procedure that entailed positioning a Schirmer standard strip (Eagle Vision, Memphis, TN, USA) at the outer 1/3 point of the lower conjunctival fornix. The strip was left in place for 5 min, during which time tear fluid was absorbed, and no analgesic eyedrops were utilized.
The tear break-up time (BUT) measurement was conducted at least 15 min subsequent to the Schirmer I test, in adherence with established protocols38. The process involved placing a droplet of normal saline on a strip paper coated with fluorescein dye (Haag-Streit International, Koniz, Switzerland), followed by gently shaking off the excess. The prepared strip was then delicately positioned on the lower lid margin to facilitate staining of the tear film. The precise moment at which the initial tear film disruption was observed under a cobalt blue filter after the last blink was considered the BUT. This measurement was replicated three times using a stopwatch, and the resultant average value was utilized for analysis.
The ocular staining score was determined by observing each eye through a slit-lamp equipped with a yellow filter following the administration of fluorescein39. We obtained the SICCA score40 and NEI score41 according to established criteria. To assess MGD, we employed two distinct methods: examining MG expressibility of five glands within the central upper lid and evaluating the quality of secreted meibum. The grading for MG expressibility of meibum from five glands ranged from 0 to 3, where 0 indicated all glands were expressible, 1 indicated 3–4 glands were expressible, 2 indicated 1–2 glands were expressible, and 3 indicated no glands were expressible. Additionally, meibum quality was graded from 0 to 3, with each score corresponding to clear, cloudy, cloudy particulate fluid, and toothpaste-like consistency based on previously defined criteria42. A consistent assessment of all clinical parameters related to dry eye disease (DED) was carried out by a single experienced researcher (K.W.K).
The participants were instructed to fill out the OSDI questionnaire, which aimed to evaluate their personal perceptions of ocular symptoms associated with DED and its impact on visual function. The survey was intended to encompass a one-week timeframe leading up to the survey date and encompassed three distinct subscales: ocular symptoms, vision-related daily function, and environmental triggers. A total of twelve questions were presented to the patients, with responses rated on a scale ranging from 0 to 4, where 0 denoted "none" and 4 denoted "always." To determine the OSDI score, the sum of the scores was multiplied by 25 and then divided by the number of questions that were accurately answered43.
Statistical analysis
For statistical analysis, we used SPSS software version 20.0 (SPSS, Inc., Chicago, IL, USA) and Prism software v.8.4.3 (GraphPad, La Jolla, CA, USA). Initially, if the data exhibited a normal distribution with standard deviation, a parametric test was utilized for analysis; otherwise, a non-parametric test was applied. To compare continuous variables between groups, we employed either the parametric Student’s t-test or the non-parametric Mann–Whitney U test. In order to compare categorical data between groups, the Chi-square test was employed. The correlation between continuous variables was assessed using the non-parametric Spearman’s rank correlation test. The datasets are presented as averages and standard deviations (±). Statistical significance was considered at a level of p < 0.05.
Data availability
The datasets generated and analyzed in the current study are available from the corresponding author on reasonable request.
References
English, F. P. & Nutting, W. B. Demodicosis of ophthalmic concern. Am. J. Ophthalmol. 91, 362–372 (1981).
Zhang, A. C., Muntz, A., Wang, M. T. M., Craig, J. P. & Downie, L. E. Ocular Demodex: A systematic review of the clinical literature. Ophthalmic Physiol. Opt. 40, 389–432 (2020).
Rabensteiner, D. F. et al. Demodex mite infestation and its associations with tear film and ocular surface parameters in patients with ocular discomfort. Am. J. Ophthalmol. 204, 7–12 (2019).
Jacobson, J. H. Demodex folliculorum infestation of the eyelids. Trans. Am. Acad. Ophthalmol. Otolaryngol. 75, 1242–1244 (1971).
Pan, S. & Chen, Y. A clinical study on the correlation between Demodex infestation and ocular surface changes in patients with meibomian gland dysfunction. Indian J. Ophthalmol. 69, 2389–2394 (2021).
Kamoun, B. et al. Blepharitis due to Demodex: MYth or reality?. J. Fr. Ophtalmol. 22, 525–527 (1999).
Coston, T. O. Demodex folliculorum blepharitis. Trans. Am. Ophthalmol. Soc. 65, 361–392 (1967).
Heacock, C. E. Clinical manifestations of demodicosis. J. Am. Optom. Assoc. 57, 914–919 (1986).
Morfin Maciel, B. M. Demodicidosis in a female patient treated as allergic blepharoconjunctivitis. A case report. Rev. Alerg. Mex. 50, 232–236 (2003).
Ayres, B. D. et al. Clinical diagnosis and management of Demodex blepharitis: The Demodex Expert Panel on Treatment and Eyelid Health (DEPTH). Eye (Lond). (2023).
Liang, L., Ding, X. & Tseng, S. C. High prevalence of demodex brevis infestation in chalazia. Am. J. Ophthalmol. 157, 342–348 (2014).
Gaddie, I. B. et al. Lotilaner ophthalmic solution 0.25% for Demodex blepharitis: Randomized, vehicle-controlled, multicenter, phase 3 trial (saturn-2). Ophthalmology (2023).
Koo, H. et al. Ocular surface discomfort and Demodex: Effect of tea tree oil eyelid scrub in Demodex blepharitis. J. Korean Med. Sci. 27, 1574–1579 (2012).
Luo, X., Li, J., Chen, C., Tseng, S. & Liang, L. Ocular demodicosis as a potential cause of ocular surface inflammation. Cornea 36(Suppl 1), S9–S14 (2017).
Sun, X. et al. The correlation between Demodex infestation and meibomian gland dysfunction at different ages. BMC Ophthalmol. 22, 388 (2022).
Sedzikowska, A., Oseka, M. & Skopinski, P. The impact of age, sex, blepharitis, rosacea and rheumatoid arthritis on Demodex mite infection. Arch. Med. Sci. 14, 353–356 (2018).
Smelser, N. J. & Baltes, P. B. International Encyclopedia of the Social & Behavioral Sciences, (Elsevier, 2001).
Kemal, M. et al. The prevalence of Demodex folliculorum in blepharitis patients and the normal population. Ophthalmic Epidemiol. 12, 287–290 (2005).
Stapleton, F. et al. TFOS DEWS II epidemiology report. Ocul. Surf. 15, 334–365 (2017).
Nelson, J. D. et al. The international workshop on Meibomian gland dysfunction: Report of the definition and classification subcommittee. Invest Ophthalmol. Vis. Sci. 52, 1930–1937 (2011).
de Paiva, C. S. Effects of aging in dry eye. Int. Ophthalmol. Clin. 57, 47–64 (2017).
Liang, L. et al. Significant correlation between Meibomian gland dysfunction and keratitis in young patients with Demodex brevis infestation. Br. J. Ophthalmol. 102, 1098–1102 (2018).
Gao, H. et al. Changes in meibum lipid composition with ocular Demodex infestation. Transl. Vis. Sci. Technol. 10, 6 (2021).
Butovich, I. A., Uchiyama, E., Di Pascuale, M. A. & McCulley, J. P. Liquid chromatography-mass spectrometric analysis of lipids present in human Meibomian gland secretions. Lipids 42, 765–776 (2007).
King-Smith, P. E., Bailey, M. D. & Braun, R. J. Four characteristics and a model of an effective tear film lipid layer (TFLL). Ocul. Surf. 11, 236–245 (2013).
Cheng, A. M., Hwang, J., Dermer, H. & Galor, A. Prevalence of ocular demodicosis in an older population and its association with symptoms and signs of dry eye. Cornea 40, 995–1001 (2021).
Ayyildiz, T. & Sezgin, F. M. The effect of ocular Demodex colonization on schirmer test and osdi scores in newly diagnosed dry eye patients. Eye Contact Lens. 46(Suppl 1), S39–S41 (2020).
Arita, R. et al. Meibomian gland dysfunction and dry eye are similar but different based on a population-based study: The Hirado-Takushima study in Japan. Am. J. Ophthalmol. 207, 410–418 (2019).
Kim, M., Chun, Y. S. & Kim, K. W. Different perception of dry eye symptoms between patients with and without primary Sjogren’s syndrome. Sci. Rep. 12, 2172 (2022).
Gouin, O. et al. TRPV1 and TRPA1 in cutaneous neurogenic and chronic inflammation: Pro-inflammatory response induced by their activation and their sensitization. Protein Cell 8, 644–661 (2017).
Hao, Y., Zhang, X., Bao, J., Tian, L. & Jie, Y. Demodex folliculorum infestation in Meibomian gland dysfunction related dry eye patients. Front. Med. Lausanne 9, 833778 (2022).
Paugh, J. R. et al. Efficacy of the fluorescein tear breakup time test in dry eye. Cornea 39, 92–98 (2020).
Gao, Y. Y. et al. High prevalence of Demodex in eyelashes with cylindrical dandruff. Invest Ophthalmol. Vis. Sci. 46, 3089–3094 (2005).
Miller, K. L. et al. Minimal clinically important difference for the ocular surface disease index. Archives of Ophthalmology. 128, 94–101 (2010).
Park, J. et al. Evaluation of tear osmolarity measured by I-Pen osmolarity system in patients with dry eye. Sci. Rep. 11, 7726 (2021).
Sambursky, R. et al. Sensitivity and specificity of a point-of-care matrix metalloproteinase 9 immunoassay for diagnosing inflammation related to dry eye. JAMA Ophthalmol. 131, 24–28 (2013).
Kim, M. et al. Assessment of reliability and validity of the 5-scale grading system of the point-of-care immunoassay for tear matrix metalloproteinase-9. Sci. Rep. 11, 12394 (2021).
Yokoi, N. et al. Classification of fluorescein breakup patterns: A novel method of differential diagnosis for dry eye. Am. J. Ophthalmol. 180, 72–85 (2017).
Eom, Y., Lee, J. S., Keun Lee, H., Myung Kim, H. & Suk Song, J. Comparison of conjunctival staining between lissamine green and yellow filtered fluorescein sodium. Can. J. Ophthalmol. 50, 273–277 (2015).
Whitcher, J. P. et al. A simplified quantitative method for assessing keratoconjunctivitis sicca from the Sjögren’s Syndrome International Registry. Am. J. Ophthalmol. 149, 405–415 (2010).
Lemp, M. A. Report of the national eye institute/industry workshop on clinical trials in dry eyes. CLAO J. 21, 221–232 (1995).
Tomlinson, A. et al. The international workshop on Meibomian gland dysfunction: report of the diagnosis subcommittee. Invest. Ophthalmol. Vi.s Sci. 52, 2006–2049 (2011).
Schiffman, R. M., Christianson, M. D., Jacobsen, G., Hirsch, J. D. & Reis, B. L. Reliability and validity of the ocular surface disease index. Arch. Ophthalmol. 118, 615–621 (2000).
Funding
This research was supported by research grant from Biomedical Research Institute, Chung-Ang University Hospital (2022).
Author information
Authors and Affiliations
Contributions
K.W.K designed the study. W.J.L, M.K, and S.H.L collected data. K.W.K, and W.J.L analyzed the data and wrote the manuscript. Y.S.C. and K.W.K. revised the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lee, W.J., Kim, M., Lee, S.H. et al. The varied influence of ocular Demodex infestation on dry eye disease and meibomian gland dysfunction across different age groups. Sci Rep 13, 16324 (2023). https://doi.org/10.1038/s41598-023-43674-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-43674-x
- Springer Nature Limited