
Abstract
This study evaluated the outcomes of a bare metal stent (BMS), DCB alone, atherectomy plus a drug-coated balloon (AT + DCB) and AT alone for the treatment of femoropopliteal artery occlusion. Four groups were included in this retrospective cohort study: 119 patients underwent the BMS procedure, 89 patients underwent DCB alone, 52 patients underwent AT + DCB, and 61 patients underwent AT alone. Patients were followed-up at 1, 6, 12 and 24 months after the procedure, the clinical outcomes and complications were assessed, and the primary outcomes were primary patency and restenosis. AT + DCB showed a lower bailout stent, and BMS displayed a higher retrograde puncture, flow-limiting dissection and postdilation (p < 0.05). For all procedures, the walking distance, ABI and pain score post-procedure were significantly improved compared with the pre-procedure values (p < 0.001). The restenosis rate was higher in BMS (21.0%) and AT alone (24.6%) than in DCB (10.1%) alone and AT + DCB (11.5%) (p = 0.04); there was no difference in amputation or clinically driven target lesion revascularization among procedures. The primary patency rates were 77.7%, 89.4%, 88.0% and 73.7% in the BMS, DCB alone, AT + DCB and AT alone groups at 24 months, respectively (p = 0.03), while the secondary patency and main adverse events (stroke, MI and death) were similar. Proximal concavity, proximal target vessel diameter ≥ 5 mm, runoff number ≥ 2 and DCB use were protective factors for primary patency. Our results suggested that AT + DCB and DCB alone were associated with higher primary patency, and DCB devices (combined with/without AT) should be the preferred choice for FP lesions.
Similar content being viewed by others

Introduction
Femoropopliteal (FP) artery stenosis/occlusion is one of the most common lower extremity arterial occlusions, and approximately 10–15% of patients with claudication will develop critical limb-threatening ischemia within 5 years, resulting in a higher risk of amputation and death1,2,3. With the advancement of interventional technology and devices, endovascular procedures have gradually become the first choice for treating FP lesions. Bare metal stent (BMS) and drug-coated balloon (DCB) angioplasty are the most commonly used procedures and can increase the limb salvage rate and patency of the target lesion4,5. However, the restenosis rate of BMSs and DCBs is still high due to challenging lesions, such as long-segment occlusion, and BMSs may affect subsequent therapy in the future6,7, while long-segment occlusion and significant plaque burden also affect the delivery of anti-proliferative drugs and the long-term outcomes of DCB angioplasty8,9,10.
The atherectomy (AT) procedure can increase the efficiency of DCB and improve the long-term results by removing plaque to obtain more lumen and reduce dissection and bailout stenting. Previous reports have demonstrated that the clinical outcomes of AT combined with DCB are better than those of DCB alone and BMS11,12,13,14. Further studies have confirmed that the effect of AT followed by DCB angioplasty is better than that of AT followed by ordinary balloon angioplasty. The advantages of AT combined with DCB have been confirmed not only in FP lesions but also in lesions below the knee and severe calcified lesions15,16,17,18, which could reduce the incidence of flow-limiting dissection and bailout stenting and improve the long-term outcome of DCB angioplasty19,20,21.
However, in the face of long-segment FP occlusion, the best choice of therapy is still one of the main problems faced by vascular physicians. Direct comparative study of BMS, DCB or AT alone and AT plus DCB is the best way to solve this issue. Nevertheless, there is still a lack of literature comparing the clinical outcomes of these procedures. In this retrospective study, we analyzed the procedural and follow-up data of these four procedures in the therapy of complex FP occlusion.
Methods
Study design and population
This study is a retrospective cohort study that included patients with chronic total FP occlusion in a university affiliated hospital from January 2019 to June 2021. Patients with symptomatic occlusion lesions in the femoropopliteal artery were eligible, and all patients were diagnosed via computed tomography angiography (CTA) and digital subtraction angiography (DSA). This study was approved by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University. All patients provided written informed consent, and all information of the participants was collected anonymously. All methods in this study were performed in accordance with relevant guidelines and regulations.
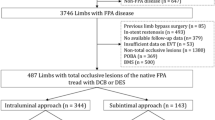
A total of 321 patients were included in this study (Fig. 1). All patients were informed in detail about all therapeutic choices and the potential best option for managing the disease, and the final treatment decision was made by the patients and guardians based on their judgment. Finally, 119 patients underwent BMS angioplasty (BMS), 89 patients underwent DCB angioplasty alone (DCB alone), 61 patients were treated with ordinary balloon angioplasty (AT alone), and 52 patients were treated with AT combined with DCB angioplasty (AT + DCB). The clinical data were collected from the medical records, including baseline data, lesion characteristics, complications and outcomes.

Flowchart of the study procedure. DCB drug-coated balloon, AT atherectomy, CD-TLR clinically driven target lesion revascularization.
The inclusion and exclusion criteria for patient selection are listed as follows.
Inclusion criteria:
-
(1)
Patient age: ≥ 18 years;
-
(2)
At least one runoff artery below the knee;
-
(3)
Rutherford categories 2–6;
-
(4)
Length of the target lesion: at least 5 cm;
-
(5)
Inflow artery stenosis < 30%;
-
(6)
Unilateral lower extremity arterial occlusion;
-
(7)
Complete follow-up data.
Exclusion criteria:
-
(1)
Arterial embolism of the lower extremity;
-
(2)
Inflow artery stenosis ≥ 50% or inflow not successfully treated;
-
(3)
Distal outflow occlusions to the target lesion;
-
(4)
Previous major amputation of the limb;
-
(5)
In-stent reocclusion of the target limb;
-
(6)
Severe target limb or systemic infection;
-
(7)
Anticipated life expectancy < 1 year;
-
(8)
Hypersensitivity or contraindications to paclitaxel, antiplatelet, or anticoagulation therapy;
-
(9)
Occlusion involving the common femoral artery and/or beyond the P2 segment of the popliteal artery;
-
(10)
Other contraindications to anesthesia or the procedure.
Endovascular procedures and medicine therapy
All patients underwent endovascular procedures under local anesthesia, and most patients underwent retrograde access of the contralateral femoral artery (or antegrade access when the ipsilateral femoral artery was available) for endovascular procedures. If the guide wire could not pass through the occluded lesion antegradely, retrograde puncture at the distal normal artery segment was used to pass through the lesion, and then the guide wire was confirmed to be located in the distal true lumen via angiography. In the BMS group, ordinary balloon catheters were used to gradually predilate the occlusion lesion of the target vessel, followed by placement of a BMS (laser-engraved bare metal stent, all stents were self-expanding stents). Patients in the DCB alone group were treated with a drug-coated balloon (Orchid, AcoTec, Beijing, China) for final angioplasty after predilation, and bailout stenting (self-expanding stents) was performed if flow-limiting dissection or recoil (> 30%) occurred after DCB angioplasty.
In the AT group, the mechanical atherectomy system was used to obtain a larger lumen, followed by ordinary balloon angioplasty (AT alone) or drug-coated balloon angioplasty (AT + DCB), and bailout stenting was used for cases with flow-limiting dissection or recoil > 30%. Flow-limiting dissection was defined as grade C or above dissection22. The final angiography was performed to assess the runoff vessel and embolization after the procedure. Three different AT devices were used in this study: 65 patients (30 with DCB) underwent the laser atherectomy procedure (Turbo‑Elite laser catheter, Spectranetics; Philips Medical Systems, Inc), 21 patients (10 with DCB) underwent the directional atherectomy procedure (Turbo-Hawk, Medtronic, Minneapolis, MN, USA), and 27 patients (12 with DCB) underwent the rotational atherectomy procedure (Straub Medical, Becton Dickenson, NJ, USA).
All patients received dual antiplatelet therapy consisting of aspirin (100 mg/d) and clopidogrel (75 mg/d) for at least 3 days before the procedure and then continued to take dual antiplatelet medical therapy (aspirin 100 mg/d and clopidogrel 75 mg/d) for 6 months after the procedure. Meanwhile, atorvastatin (20 mg/d) was given for lipid-lowering therapy, and beraprost sodium was given for adjuvant medicine therapy (120 µg/d), followed by long-term oral single antiplatelet drug and statin therapy.
Assessment and definition
All patients were followed-up at 30 days and 6, 12 and 24 months after the procedure. Follow-up data included clinical symptoms, the Rutherford classification, ankle brachial index (ABI) values and ultrasound and/or CTA results. The morphology of proximal lesions was defined as concave proximal and convex proximal. The cutoff time for safety and clinical endpoint analysis was 24 months. The primary outcomes were the patency of target vessels at 24 months after the procedure. Primary patency was defined as a target lesion without obvious restenosis (< 50%) or clinically driven target lesion revascularization (CD-TLR); secondary patency was defined as patency maintained after secondary endovascular therapy in patients with reocclusion after the procedure. The secondary outcomes were amputation rate, all-cause mortality and CD-TLR, and CD-TLR was defined as any repeated endovascular therapy or bypass surgery associated with Rutherford grade deterioration and/or an increase in the original wound size and/or new wound appearance22,23,24. Significant restenosis was defined as > 50% based on angiography- or ultrasound examination-derived velocity parameters (peak systolic velocity ratio ≥ 2.4). The major adverse events (MAEs) included myocardial infarction (MI), stroke and all-cause death. Limb pain was assessed by the visual analog scale (VAS), with a score ranging from 0 to 10, and a higher value indicated more severe pain25. The calcification degree was assessed by using the proposed peripheral arterial calcium-scoring system (PACSS). This system included grades 0 to 4; grades 0 and 1 were defined as non/mild calcification, grade 2 was defined as medium calcification, and grades 3–4 were defined as severe calcification26.
Statistical analysis
All data were collected in an Excel file (Version 2013, Microsoft, Redmond, Washington) and analyzed using SPSS v. 22.0 (SPSS, Chicago, IL, USA) software. Categorical variables are presented as numbers (percentages) and were compared using the Chi-square test or Fisher’s exact test. Continuous variables are presented as the mean and standard deviation (SD). The normal distribution was tested by using the Shapiro‒Wilk test and then compared by using one-way analysis of variance and Student–Newman‒Keuls test. The primary patency, secondary patency and overall survival rate of patients were analyzed using the Kaplan‒Meier method and were compared by the log-rank test. To confirm risk factors for restenosis, univariate and multivariate Cox hazard regression analyses were performed with all baseline and procedural variables. The variate with p < 0.20 was used as the covariate after univariate analysis, multivariate analysis was performed, and the hazard ratio (HR) and 95% confidence interval (CI) of risk factors were calculated. p values < 0.05 were considered statistically significant.
Results
Demographic characteristics and baseline data
This study included a total of 321 limbs of 321 patients with FP occlusion (Fig. 1); 119 patients received the BMS procedure, 89 patients received DCB angioplasty alone, 52 patients underwent AT combined with DCB angioplasty (AT + DCB), and 61 patients underwent AT angioplasty alone. There were no significant differences in demographic and baseline characteristics among these four procedures (Table 1). No differences in Rutherford category, pre-ABI, claudication distance, VAS pain score or medicine therapy were confirmed among the four procedures (p > 0.05).
Lesion and procedural characteristics
The occluded lesion and procedural characteristics are listed in Table 2. In this case cohort study, all lesions were occlusions, and the main manifestations were TASC C/D lesions. The proximal and distal diameters of the target vessels were similar among the four procedures. There was no difference in the morphological type of the proximal plaque cap, runoff number of BTK, predilation, bailout stent, distal embolization or closure device (p > 0.05), while the rate of bailout stent in the AT + DCB procedure was significantly less than that in the DCB and AT alone procedures (p < 0.05). However, a higher retrograde puncture rate, postdilation, flow-limiting dissection and stent number were confirmed in the BMS procedure than in the other three procedures (p < 0.01), and the procedure time in the DCB-alone procedure was higher than that in the other three procedures (p < 0.05).
Short-term and mid-term outcomes and complications
All patients completed the endovascular procedure, and the technical success rate was 100%. Perforation and distal embolization occurred in the AT and DCB procedures, but no differences were confirmed (Table 3). Perforation was treated via stent angioplasty, and distal embolization was treated via a thrombus aspiration catheter. There were no significant differences in the access complications or main adverse events (stroke, MI, death and deep vein thrombosis) at 1 month (p > 0.05). The postwalking distance, post-ABI and post-VAS score were similar in the four procedures.
The walking distance and ABI after the procedure were significantly higher than those before the procedure among the four procedures (p < 0.001), and the VAS pain score was significantly decreased after the procedure compared with before the procedure (p < 0.001). The restenosis rate was higher in the BMS (21.0%) and AT alone (24.6%) groups than in the DCB (10.1%) alone and AT + DCB (11.5%) groups (p = 0.04); there was no difference in the CD-TLR rate among the four procedures; however, a higher CD-TLR tendency was confirmed in the BMS (16.8%) and AT alone (21.3%) groups (p = 0.09). No difference was confirmed in the amputation rate among the four procedures (p > 0.05).
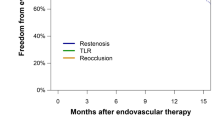
The cumulative stroke, MI and death rates were similar among the four procedures, and no difference was confirmed between the procedures (p > 0.05). The survival rates were 94.1%, 95.5%, 96.1% and 93.4% in the BMS, DCB alone, AT + DCB and AT alone procedures at 24 months, respectively (Fig. 2a, p > 0.05). The primary patency of the target lesion was 77.7%, 89.4%, 88.0% and 73.7% in the BMS, DCB alone, AT + DCB and AT alone groups at 24 months, respectively. The primary patency in the DCB alone and AT + DCB groups was higher than that in the BMS and AT alone groups (Fig. 2b, p = 0.03), while the secondary patency rates were 87.5%, 92.9%, 92.0% and 85.9% in the BMS, DCB alone, AT + DCB and AT alone groups at 24 months, respectively (Fig. 2c, p > 0.05).

Kaplan‒Meier survival analysis for cumulative survival (a), primary (b) and secondary (c) patency rates of the four procedures. The number at risk represents the number of evaluable participants at the beginning of each follow-up interval. BMS bare metal stent, DCB drug-coated balloon, AT + DCB atherectomy + drug-coated balloon, AT atherectomy, mon month, No. number.
Univariate and multivariate analyses for predictors of restenosis
Univariate regression analysis was used to determine the potential risk factors related to restenosis (Table 4), and multivariate regression analysis was used to confirm the independent risk factors for restenosis. A prewalking distance < 50 m (HR: 1.95; 95% CI: 1.03–3.67, p = 0.04) was an independent risk factor for restenosis. Proximal concavity (HR: 0.49; 95% CI: 0.27–0.89, p = 0.02), proximal target vessel diameter ≥ 5 mm (HR: 0.32; 95% CI: 0.12–0.85, p = 0.02), runoff number ≥ 2 (HR: 0.45; 95% CI: 0.22–0.91, p = 0.02) and DCB use (HR: 0.24, 95% CI: 0.11–0.57, p = 0.001) were potential protective factors for restenosis.
Discussion
Long-segmental occlusion of FP lesions is still a challenging problem for PAD therapy, in which BMS plays a major role. AT technology using different plaque removal systems is more conducive to obtaining the lumen and reducing the incidence of flow-limiting dissection, but the effectiveness of the application of AT alone is still controversial14,27,28, and some studies have proven that the clinical outcome of AT combined with the DCB procedure is better11,12. However, there is still a lack of head-to-head comparisons of BMS, DCB alone, AT + DCB, and AT alone procedures to determine the best therapy modality for FP lesions. Our study showed that the survival rate, CD-TLR and secondary patency of the four procedures were not significantly different, but AT combined with DCB and DCB alone revealed a higher primary patency rate. The walking distance, ABI and post-VAS pain score of the four procedures were significantly improved compared with those before the procedure, and there was no difference in complications, amputation rate or major adverse events for the four procedures. These data confirmed that these techniques remain effective therapeutic methods for FP lesions, but the BMS procedure has a higher incidence of flow-limiting dissection, postdilatation and restenosis.
Compared with traditional angioplasty procedures, DCB angioplasty improves the long-term patency rate and limb salvage rate of patients, but complex lesions such as long-segment occlusion, restenosis and severe calcification may affect the drug delivery efficiency of DCB balloons, thus affecting the outcome of the procedure9,10,29,30. However, the AT procedure could improve the effect of vessel preparation and is more conducive to the use of DCBs. Further studies have shown that AT devices combined with DCBs show higher patency21,31,32. Our study demonstrated that the AT procedure followed by DCB angioplasty has a higher primary patency and lower restenosis rate for FP occlusion. The ordinary BMS procedure indicated a higher incidence of flow-limiting dissection when compared with DCB alone, and AT combined with the DCB procedure showed lower rates of flow-limiting dissection and bailout stenting. Although some previous reports have indicated that AT combined with the DCB procedure may improve primary patency11,12,15, our study demonstrated that there was no difference between AT combined with DCB and DCB alone in terms of primary patency.
The AT device can reduce the plaque/thrombus load of occlusive lesions, thereby obtaining larger lumens, which is more conducive to the delivery and utilization of DCB drugs. Previous studies confirmed that the primary patency of AT combined with DCB is significantly higher than that of DCB alone and BMS11,21. More importantly, this procedure can preserve potential opportunities for future therapy. The long-term patency of the AT procedure combined with ordinary balloon/stent angioplasty does not show a corresponding advantage. Some studies have even shown that the primary patency of AT combined with ordinary balloon angioplasty is not better than that of balloon angioplasty alone14. Another study suggests that the long-term outcome of AT combined with DCB angioplasty is significantly better than that of AT combined with ordinary balloon angioplasty or DCB angioplasty alone33. Our data revealed that the primary patency of AT alone followed by balloon or bailout stenting is lower than that of AT combined with DCB. Further studies have confirmed that the bailout stenting of AT combined with DCB is also significantly lower than that of AT alone and DCB alone14,33. Therefore, DCB (combined with/without AT) should be the first choice for long-segment FP occlusion in clinical practice.
Restenosis is the main factor affecting the long-term patency of FP lesions. Several studies have found that severe calcification, long-segment occlusion, in-stent restenosis, TASC C/D lesions, runoff number and other factors are closely related to restenosis29,34,35. In our study, we determined the potential risk factors by regression analysis. A prewalking distance < 50 m was an independent risk factor for restenosis, while proximal concave lesion, proximal artery diameter ≥ 5 mm and runoff number ≥ 2 were protective factors. These data are consistent with most of the conclusions from previous studies. Our study found that the morphology of the proximal concave occlusion was associated with a lower retrograde puncture rate and incidence of restenosis. These data suggest that the morphology of the occlusion cap may have a potential impact on the technical success and clinical outcomes of angioplasty, while larger proximal diameters and more runoff vessels indicate a lower incidence of restenosis. Furthermore, our data confirmed that the use of DCB balloons is the key factor in reducing the incidence of restenosis and maintaining long-term patency.
Limitations
Although this study conducted a head-to-head comparison of the four procedures of BMS, DCB alone, AT + DCB and AT alone on FP occlusion lesions, there are also obvious limitations in this study. First, this study is not a prospective, randomized controlled trial, and its results may be affected by potential confounding factors. Second, this study is not a multicenter data analysis, and the selection bias of patients and devices used may affect the generalizability of the conclusions. Third, our research did not include all the devices being used; thus, our findings need further verification. Our conclusions still need to be confirmed by multicenter, prospective, large-sample RCT studies in the future.
Conclusions
Our data suggest that the DCB procedure (combined with/without AT) shows higher primary patency and that the AT combined with DCB procedure has a lower incidence of flow-limiting dissection and bailout stenting; thus, DCB devices (combined with/without AT) should be the first therapeutic choice for patients with FP lesions. We believe that this study can provide some evidence for the debate on the best procedure for FP occlusion.
Data availability
The data from this study are available from the corresponding author upon reasonable request.
References
Fowkes, F. G. R. et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 382, 1329–1340 (2013).
Gerhard-Herman, M. D. et al. 2016 AHA/ACC guideline on the management of patients with lower extremity peripheral artery disease: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 135(12), e686–e725 (2017).
Conte, S. M. & Vale, P. R. Peripheral arterial disease. Heart Lung Circ. 27(4), 427–432 (2018).
Mohapatra, A. et al. Nationwide trends in drug-coated balloon and drug-eluting stent utilization in the femoropopliteal arteries. J. Vasc. Surg. 71, 560–566 (2020).
Katsanos, K., Spiliopoulos, S., Paraskevopoulos, I., Diamantopoulos, A. & Karnabatidis, D. Systematic review and meta-analysis of randomized controlled trials of paclitaxel-coated balloon angioplasty in the femoropopliteal arteries: Role of paclitaxel dose and bioavailability. J. Endovasc. Ther. 23, 356–370 (2016).
Kansal, A. et al. Endovascular treatment of femoro-popliteal lesions. Clin. Cardiol. 42, 175–183 (2019).
Schneider, P. A. et al. Treatment effect of drug-coated balloons is durable to 3 years in the femoropopliteal arteries: Long-term results of the IN.PACT SFA randomized trial. Circ. Cardiovasc. Interv. 11, e005891 (2018).
Tepe, G. et al. Drug-eluting balloon therapy for femoropopliteal occlusive disease. J. Endovasc. Ther. 22, 727–733 (2015).
Mietz, S., Lehmann, T. & Teichgraber, U. Multivariable regression analysis of clinical data from the randomized-controlled EffPac trial: Efficacy of femoropopliteal drug-coated balloon angioplasty. Cardiovasc. Interv. Radiol. 43, 840–849 (2020).
Fanelli, F. et al. Calcium burden assessment and impact on drug-eluting balloons in peripheral arterial disease. Cardiovasc. Interv. Radiol. 37, 898–907 (2014).
Wei, L. et al. Directional atherectomy and drug-coated balloon angioplasty vs. bare nitinol stent angioplasty for femoropopliteal artery lesions. Vasa 51, 275–281 (2022).
Lin, F., Wang, H., Ding, W., Chen, G. & Zhang, Z. Atherectomy plus drug-coated balloon versus drug-coated balloon only for treatment of femoropopliteal artery lesions: A systematic review and meta-analysis. Vascular 29, 883–896 (2021).
Deloose, K. et al. Combining the Passeo-18 Lux drug-coated balloon and the pulsar-18 bare metal stent: 12- and 24-month outcomes of the BIOLUX 4EVER investigator-initiated trial. J. Endovasc. Ther. 27, 936–945 (2020).
Wu, Z. et al. Atherectomy combined with balloon angioplasty versus balloon angioplasty alone for de novo femoropopliteal arterial diseases: A systematic review and meta-analysis of randomised controlled trials. Eur. J. Vasc. Endovasc. Surg. 62, 65–73 (2021).
Sixt, S. et al. Drug-coated balloon angioplasty after directional atherectomy improves outcome in restenotic femoropopliteal arteries. J. Vasc. Surg. 58, 682–686 (2013).
Cha, J. J. et al. Clinical outcomes of atherectomy plus drug-coated balloon versus drug-coated balloon alone in the treatment of femoropopliteal artery disease. Korean Circ. J. 52, 123–133 (2022).
Zeller, T. et al. Orbital atherectomy prior to drug-coated balloon angioplasty in calcified infrapopliteal lesions: A randomized, multicenter pilot study. J. Endovasc. Ther. 29, 874–884 (2022).
Kokkinidis, D. G. et al. Two-year outcomes of orbital atherectomy combined with drug-coated balloon angioplasty for treatment of heavily calcified femoropopliteal lesions. J. Endovasc. Ther. 27, 492–501 (2020).
Rodoplu, O. et al. Efficacy of rotational atherectomy followed by drug-coated balloon angioplasty for the treatment of femoropopliteal lesions-comparison with sole drug-coated balloon revascularization: Two-year outcomes. Ann. Vasc. Surg. 73, 222–233 (2021).
Cai, Z. et al. Midterm outcome of directional atherectomy combined with drug-coated balloon angioplasty versus drug-coated balloon angioplasty alone for femoropopliteal arteriosclerosis obliterans. Ann. Vasc. Surg. 64, 181–187 (2020).
Kavala, A. A., Kuserli, Y., Turkyilmaz, G., Yesiltas, M. A. & Turkyilmaz, S. Comparison of drug-coated balloon angioplasty alone and directional atherectomy combined with drug-coated balloon angioplasty in patients with lower extremity peripheral arterial disease with claudication. Ann. Vasc Surg. 90, 162–171 (2023).
Armstrong, E. J. et al. Dissections after infrainguinal percutaneous transluminal angioplasty: A systematic review and current state of clinical evidence. J. Endovasc. Ther. 26, 479–489 (2019).
Shammas, N. W. et al. Safety and 1-year revascularization outcome of SilverHawk atherectomy in treating in-stent restenosis of femoropopliteal arteries: A retrospective review from a single center. Cardiovasc. Revasc. Med. 13, 224–227 (2012).
Patel, M. R. et al. Evaluation and treatment of patients with lower extremity peripheral artery disease: Consensus definitions from Peripheral Academic Research Consortium (PARC). J. Am. Coll. Cardiol. 65, 931–941 (2015).
Farrar, J. T., Young, J. P. Jr., LaMoreaux, L., Werth, J. L. & Poole, R. M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 94, 149–158 (2001).
Joye, J. The PATRIOT (peripheral approach to recanalization in occluded totals) study results. Am. J. Cardiol. 100, S24 (2007).
Sharma, P. et al. Effectiveness and safety of atherectomy versus plain balloon angioplasty for limb salvage in tibioperoneal arterial disease. J. Vasc. Interv. Radiol. 34(3), 428–435 (2023).
Oh, K. et al. Comparison of outcomes for balloon angioplasty, atherectomy, and stenting in the treatment of infrapopliteal disease for chronic limb-threatening ischemia. J. Vasc. Surg. 77, 241–247 (2023).
Roh, J. W. et al. Risk factors for restenosis after drug-coated balloon angioplasty for complex femoropopliteal arterial occlusive disease. Ann. Vasc. Surg. 55, 45–54 (2019).
Caradu, C. et al. Systematic review and updated meta-analysis of the use of drug-coated balloon angioplasty versus plain old balloon angioplasty for femoropopliteal arterial disease. J. Vasc. Surg. 70, 981-995.e10 (2019).
Loffroy, R. et al. Percutaneous mechanical atherothrombectomy using the Rotarex®S device in peripheral artery in-stent restenosis or occlusion: A French retrospective multicenter study on 128 patients. Quant. Imaging Med. Surg. 10, 283–293 (2020).
Yang, S., Li, S., Hou, L. & He, J. Excimer laser atherectomy combined with drug-coated balloon versus drug-eluting balloon angioplasty for the treatment of infrapopliteal arterial revascularization in ischemic diabetic foot: 24-month outcomes. Lasers Med. Sci. 37, 1531–1537 (2022).
Foley, T. R. et al. Mid-term outcomes of orbital atherectomy combined with drug-coated balloon angioplasty for treatment of femoropopliteal disease. Catheter Cardiovasc. Interv. 89, 1078–1085 (2017).
Pan, T. et al. Anemia as a risk factor for restenosis in femoropopliteal arterial disease after drug-coated balloon angioplasty. Vascular 31, 948–953 (2022).
Ichihashi, S. et al. Vessel calcification as a risk factor for in-stent restenosis in complex femoropopliteal lesions after Zilver PTX paclitaxel-coated stent placement. J. Endovasc. Ther. 26, 613–620 (2019).
Acknowledgements
The language of this article was edited by American Journal Experts (AJE). Prof. Leilei Pei from the Department of Medical Statistics of Xi’an Jiaotong University oversaw the statistical analysis of this manuscript.
Author information
Authors and Affiliations
Contributions
Study design, J.Q., N.D. and L.Y.; data collection and data analysis, J.Q., N.D., Y.H., L.C., Y.L., J.D. and L.Y.; writing, J.Q., Y.H. and L.Y.; revision and review manuscript, J.Q., N.D., Y.H., L.C., Y.L., J.D. and L.Y.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, L., Quan, J., Dong, J. et al. Comparison of mid-outcome among bare metal stent, atherectomy with or without drug-coated balloon angioplasty for femoropopliteal arterial occlusion. Sci Rep 14, 63 (2024). https://doi.org/10.1038/s41598-023-50511-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-50511-8
- Springer Nature Limited