
Abstract
Undernourishment is a persistent public health problem contributing to increased mortality in children under five in low-income countries, likely exacerbated by socio-economic disparities within communities. This paper aimed to examine the effect of wealth-related inequality on undernutrition in children under five in low, lower-middle, and upper-middle-income countries (LMICs). We analyzed cross-sectional data from the demographic and health survey program collected between 2017 and 2022 from 24 LMICs. Children born within 5 years preceding the survey were included in the analysis. Child undernutrition was the dependent variable (measured by stunting, wasting, and underweight) and country-level wealth-based inequality was the independent variable assessed by concentration index values stratified by the World Bank’s income categories. Within country inequality of child undernutrition was determined by concentration index (C) values with 95% confidence intervals (95% CI) and sub-group analysis by place of residence and sex of the child. We then fit bootstrapped meta-regression to check the variation in inequality of child undernutrition across different income category countries. The analysis was controlled by potential confounding variables. From the total sample size of 334,502 children included in the study, 35% were undernourished. Wealth-related inequality in child undernutrition was observed in 11 countries, consistently across income categories. Child undernutrition was highly concentrated among the poor households of Türkiye [C: − 0.26, 95% CI − 0.31 to − 0.20], and Cameroon [C: − 0.19, 95% CI − 0.22 to − 0.17], and relatively it was less concentrated among the poor in Liberia [C: − 0.07, 95% CI − 0.11 to − 0.04], and Gambia [C: − 0.07, 95% CI − 0.11 to − 0.04]. There is no difference in undernutrition associated with inequality between the three broad LMIC categories. The wealth-related inequality in child undernutrition within many of the included countries is still very significant. However, the economic category of countries made no difference in explaining wealth-related inequality in child undernutrition. Inter-sectoral collaboration to fight poverty and render special attention to the disadvantaged population segments would potentially help to address the observed inequity.
Similar content being viewed by others

Introduction
While global mortality in children under five has declined over recent decades, sub-national data for Low and Middle-Income Countries (LMICs) shows considerable raise especially in five sub-Sahara Africa (SSA)1. The relatively increased mortality in children under 5 years in LMICs is likely attributable to undernutrition, exacerbated by socio-economic disparities within communities2,3. Indeed, the United Nations recognizes that undernourishment and severe food insecurity have been increasing in most African countries4. Undernutrition in young children results in underweight, stunting, and wasting as an immediate outcome5. Strategies to address socio-economic disparities associated with undernutrition and subsequent mortality in young children are urgently needed6.
The effect of childhood undernutrition is not limited to death and complications for the affected person. Undernutrition in early childhood has long-term consequences for the child and has intergenerational adverse effects7,8. Child undernutrition refers to an insufficient intake of energy and nutrients to meet the body’s need to maintain a state of health9. It is usually measured as either a combination of stunting (too short for age), underweight (too thin for age), wasting (too thin for height), or deficiencies in vitamins and minerals. Despite many targeted interventions globally, approximately 149 million (22.3%), 85 million (12.6%), and 45 million (6.6%) children under the age of five are estimated to have stunting, underweight, and wasting respectively in the world10,11.
There is substantial variation in the global distribution of undernutrition between different income countries. An aggregate data in 2020 showed the highest prevalence (50–55%) of childhood stunting in low-income countries like Timor, Burundi, and Eritrea, while it was as low as (1.5–2.0%) in high-income countries including Australia, Belgium, Chili, Greece, and Germany12. Similar disparities were observed for wasting with the highest prevalence in Djibouti (21%) and South Sudan (22%), whereas it was below 0.5% in Australia, Belgium, Chile, and the USA13. Furthermore, underweight was below 0.5% in Australia, Chile, Estonia, Germany, and the USA; and it was between 27 and 39% in Burundi, Chad, Djibouti, Sudan, and Eritrea14.
In addition to the disparities between countries of varying economic categories, socio-economic status is a common risk factor for child undernutrition within countries15,16. Evidence indicated that wealth and/or income of the household have a strong negative link with inequity in child undernutrition17. In countries such as Bangladesh, Pakistan, Nepal, India and Ethiopia the wealth-related gap in child undernutrition measures has been very high and increasing in some the areas18,19,20. On the other hand, the educational status of the mother, place of residence (rural/urban), and number of siblings are factors that create variation in the health status of the population including childhood level of nutrition21. Studies also uncover that seeking medical care whenever the child is ill22, and better child vaccination23 are protective factors against child undernutrition24,25,26,27.
Many economically better-off countries have now minimized and eliminated undernutrition28,29. Despite their success, the highest magnitude of undernutrition remains concentrated among the poorest economic group in many countries28. However, the extent to which the economically well-off countries managed the gap of undernutrition between the poorest and richest categories of the population remains unanswered. Therefore, this analysis set out to assess the wealth-based disparities in nutritional status among children under five in lower, lower-middle, and upper-middle-income countries. We further tested the effect of country level income category on equity differences in undernutrition.
Methods
Study design and setting
In this study, we used cross-sectional data collected from Low Income (LI), Lower Middle Income (LMI), and Upper-Middle-Income (UMI) countries by the Demographic and Health Survey (DHS) program. We categorized countries based on the 2020’s World Bank economic classification system30. A total of 11 LI countries that have a Gross National Income (GNI) per capita of 1035 US$ or less; eight LMI countries which have a GNI per capita between US$ 1036 and US$ 4045; and four UMI countries with a GNI per capita of between US$ 4046 and US$ 12,535 were included in the study. The population density of LI countries estimated to be 51.5 people per square kilometer and have a population growth rate of 2.6% per year31. Whereas the population growth rate for LMI countries is 1.3% per year and 135 people per square kilometer31. On the other side, the population density for UMI countries is 47 people per square kilometer, and the population growth rate is 0.2%31.
Data sources and study participants
The information sources for this study were the DHS program of data collections from 24 countries that were published between 2017 and 2022. The included countries are from the three economic categories described earlier. Accordingly, Burundi (2016–17), Ethiopia (2019), Gambia (2019–20), Guinea (2018), Haiti (2017–18), Liberia (2019–20), Mali (2018), Niger (2017), Rwanda (2019–20), Sierra Leone (2019), and Tajikistan (2017) were from LI category; Bangladesh (2017–18), Benin (2017–18), Cameroon (2018), Mauritania (2019–21), Nigeria (2018), Pakistan (2017–18), Papua New Guinea (2016–18), and Senegal (2019) were LMI countries; and Albania (2017–18), Maldives (2016–17), India (2019–21), and Türkiye (2018) were UMI countries.
The DHS data was collected by dividing a country into enumeration areas (EA). An EA is a counting unit generated for the population census/survey. The DHS data being collected takes EAs as a sampling cluster, a further stage of sampling was then conducted to identify study participants. The DHS program collects data using five types of questionnaires. Among those, we considered children born in the 5 years before the interview, or the kids’ file component, and took children under the age of five as the study population. Questions related with the children’s module were answered by the mother/caregiver. We made use of the characteristics of the child, the mother/caregiver and the household in our analysis.
The DHS data are nationally representative data for population, family, and maternal and child health issues that provide data for a wide range of monitoring and impact evaluation indicators in the areas of population, health, and nutrition32,33. The DHS program works with country-specific agencies to conduct a household sample survey covering a range of population health indicators. The primary objective of the DHS is to provide up-to-date estimates of key demographic and health indicators34. The DHS datasets were obtained from the DHS Program website upon request35.
Variables and measurement
Dependent variable
Undernutrition variables were estimated from measured body weight and height readings. Indicators of undernutrition were defined as stunting if the height-for-age Z-score is less than 2 standard deviations below the population mean; wasting if the weight for height Z-score is less than 2 standard deviations below the population mean, and similarly underweight if the weight-for-age Z-score is less than -2 standard deviations below the population mean36. We then classified undernutrition for the child participants with at least one of the above other indicators of undernutrition.
For a descriptive analysis purpose we calculated the proportion (prevalence) of all measures of undermatron (stunting, wasting and underweight) and overall undernutrition from overall children included in the analysis.
Independent variable
Regarding the household’s wealth, the DHS program uses the wealth index37 which serves as a composite score of the household’s living standard, considering the country’s context. The wealth index was calculated using easy-to-collect data on the household’s ownership of selected assets, and materials then, the final wealth quintile was obtained after a valuation and analysis using the principal component analysis tools38. The households were then categorized into either the poorest, poor, middle, rich, or richest quintile groups. To classify the region as urban or rural, the DHS program uses country-specific urban-to-rural classification methods and reports accordingly.
Bias
The DHS data program collects data by dividing the country into different sizes of EAs and an equal amount of households taken as a sample from each of the EA. This end-up with a disproportionate sample size allocation to the EAs. We used sample and cluster weights to adjust for sampling errors.
Statistical approach
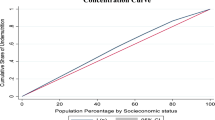
We used concentration index (C) and concentration curves to assess the economic inequality in child nutritional status. Concentration curves were plotted considering the cumulative percentage of child undernutrition (y-axis) against the cumulative percentage of the population, ranked by wealth status variables (x-axis) (Supplementary file 1). To quantify equity differences, concentration index values were computed with the respective 95% confidence interval. The concentration index is twice the area between the concentration curve and the line of equality (the 45° line). The concentration index value ranges from − 1 to + 1. The convention is when the index value is negative the curve lies above the line of equality, indicating the disproportionate concentration of child undernutrition among the poor, and when it is positive it lies below the line of equality, showing the disproportionate child undernutrition among the rich39.
We did a sub-grouping analysis by place of residence and sex of the child. Additionally, a meta-regression test to check if there is a significant difference in nutritional status inequality among countries with different economic categories. For our regression model, we used the country-level wealth-based inequality in undernutrition as measured by concentration index values, and the countries’ economic category according to the World Bank’s definition was the independent variable30. We controlled the model with various variables including the country’s income inequality as measured by the Gini index40. Concentration index of undernutrition by maternal education: maternal education divided into four categories including no formal education, primary education, secondary education and higher education levels. Furthermore, we used concentration of undernutrition by number of under 5 years’ old children in the household, child vaccination status for Bacille Calmette-Guérin (BCG), one dose of pentavalent vaccine, and the first dose of measles-containing vaccine.
Considering the skewness of the distribution of the outcome variable and the few number of cases (24 countries), we employed the non-parametric bootstrapped regression with 1000 replications. We then tested the normal distribution of residuals. The variables with p-value < 0.05 was considered as significantly associated with the outcome variable. We used Stata version – 14 and Microsoft Excel spreadsheet version 2016 for the analysis. To display the level of child undernutrition in different countries and economic categories, the QGIS version 3.24.3 software was used. All the analyses were adjusted for clusters and sample weights.
We did aggregate level simple regression between level of undernutrition (stunting, wasting and underweight) as a dependent and the country’s overall income difference measure (Gini index value) as an independent variable. Because the distribution of the outcome variable is skewed to the right to all of the variables, we tend to use non-parametric non- bootstrapped regression with 1000 replications after checking log transformation is not working as well.
Patient and public involvement
As the data sources were obtained from the DHS Program, there was no patient and public involvement.
Ethical approval and informed consent
The authors analyzed publicly available secondary data obtained from the DHS program database. There was no additional ethical approval sought by the authors.
Result
Child nutritional status
Of the total sampled 24 countries, we obtained 334,502 for height-for-age, 334,071 for weight-for-height, and 331,541 for weight-for-age measures, respectively. There were 110,386 cases (33%) of stunting, 50,111 cases (15%) of wasting, and 89,516 cases (27%) of underweight yielding an overall child undernutrition rate of 35% (8.5% to 47.4%). The proportion of undernutrition was highest (47.4%) in India (UMIC), followed by Ethiopia, a LIC, (38.9%), and Bangladesh (35.1%) a LMIC. While it was lowest (8.5%) in Türkiye (UMIC), Gambia (LIC) (10.3%), and Albania (11.5%) which is a UMIC (Fig. 1) (The details are available in supplementary file 2).

The status of child undernutrition in 24 lower, lower-middle, and upper-middle-income countries, 2017–2022.
Wealth-related Inequalities in child undernutrition
Wealth-related inequality in child undernutrition status was observed in 12 out of 24 countries included in the analysis, consistently across all World Bank economic classifications (supplementary file 1 visually shows the wealth based variation in undernutrition). Furthermore, child undernutrition was highly concentrated among the poor households of Türkiye [C: − 0.26, 95% CI − 0.31 to − 0.20], Cameroon [C: − 0.19, 95% CI − 0.22 to − 0.17], and Haiti [C: − 0.18, 95% CI − 0.20 to − 0.15]. Undernutrition was relatively less concentrated among the poor in Liberia [C: − 0.07, 95% CI − 0.11 to − 0.04], and Gambia [C: − 0.07, 95% CI − 0.11 to − 0.04] (Table 1).
The results indicated that there is more inequity in urban areas compared to the rural settings in most of the countries. For instance, if we see the urban–rural differences in stunting, the inequalities in Rwanda were on average 19% (C = − 0.19) more pronounced in the poor living in urban areas than in the rural. On the contrary, in Albania being poor in urban or rural communities did not show any difference. On the other side, the urban–rural equity gap in wasting was highest 22% (C = − 0.22) in poor communities of urban residents in Türkiye, whereas in Mali there was no inequality difference between urban and rural residents. Regarding underweight, the inequality difference was also higher (26% (C = − 0.26) in urban communities of Rwanda, and there was no inequality difference between urban and rural India. The overall gap in child undernutrition by place of residence was wider in Maldives (64%) and Rwanda (23%), whereas, in Sierra Leone, and Mali inequalities in child undernutrition were similar for urban and rural residents (Fig. 2) (Supplementary file 3).

The status of urban to rural inequality gap in child undernutrition in the 24 lower, lower middle, and upper-middle-income countries.
Regarding inequalities within the sex of the child, the male-to-female difference in the concentration index of stunting was very close to zero in all of the countries. Coming to wasting, almost all countries had a minimal gap between male and female children, in Rwanda the gap was relatively higher C = 0.15. On the other side, inequalities for child underweight, and overall undernutrition was almost equal to zero for all countries. The same applies to overall undernutrition (Supplementary file 3).
Factors affecting the wealth-related inequalities in child undernutrition
We ran a bootstrapped regression using linear regression commands to test if there is any significant difference in the concentration index values because of the difference in the economic category of the country. The results of the test suggested that the concentration index of the countries did not significantly vary across different economic categories. The only variable that has a significant association with inequity in child undernutrition was the concentration of maternal level of education (Coef.: 1.15; 95% CI 0.66, 1.64) (Fig. 3) (details are available at supplementary file 4). Our sensitivity analysis has also revealed that there is no association between country level wealth variation and undernutrition measures (Supplementary file 5).

Factors affecting child undernutrition status in 24 selected low, lower middle, and upper-middle-income countries, 2017–2022.
Discussion
Our findings indicate, on average, one in three of the under-five child was undernourished regardless of the country’s economic status. This finding is consistent with other studies reporting that low-income countries are disproportionately affected by severe undernutrition41,42. Child undernutrition in these countries will undoubtedly cause severe health consequences for affected individuals throughout their lifespan43. Evidence shows that nutritionally disadvantaged children develop a range of health conditions including impaired cognitive function, resulting in further socio-economic disadvantage. This results in intergenerational social and economic disadvantage within low-income countries exacerbating the risk and adverse consequences of undernourishment in their vulnerable population groups44,45.
Apart from the differences in child undernutrition across the countries, wealth-related within-country inequality in childhood undernutrition was observed. In our study, a significant gap, which favors wealthier households, in all forms of child undernutrition was demonstrated. In countries like Burundi and Cameroon, the inequity was the highest. Earlier reports also indicated that wealth-related equity gaps in child undernutrition are common across all corners of the world19,46. This would be attributed to the economic status of the households which impacts their capability to ensure food security and to access health services whenever a child is ill47,48. Regardless of the success in minimizing the prevalence of undernutrition, countries are still challenged by an equity gap in child nutrition indicators. For instance, Cameroon has a 4.4% prevalence of stunting but has the highest gap among the poor and rich quintiles. Similarly, Haiti and Cameroon have the lowest prevalence of underweight. Meanwhile, the difference in underweight between children from the better off and the poorest family ranks among the countries with the highest inequity.
The other major concern related to child undernutrition status is the difference between being urban and rural residents and between sex groups. The concentration index values suggested that inequalities in child undernutrition were concentrated in poor communities of urban areas, than that of rural communities. In almost all countries, the three nutritional indicators have shown wider equity gaps in urban settings than the rural ones. This can be explained by the highly uncertain urban income which mainly comes from wage employment, trading, and self-employment which are more unstable and unequal than farming-based income sources49,50. In rural settings, life is relatively stable and relaxed, where people do agriculture and animal husbandry for a living creating a favorable environment to feed their children51. On the other hand, even though the gap is small, the equity gap in stunting is consistently higher among male children regardless of a country’s economic category52. Concerning wasting and being underweight in many countries, the equity gap is higher among female children. There is evidence indicating the prevalence of undernourishment is higher among female children in LMICs53.
Going through the analysis result for the 24 countries, one can observe significant inequity in child nutritional status regardless of a country’s economic category. Five (45.5%) of the countries from the low-income category, three (33.3%) countries from the lower middle-income category, and one (25%) country from the upper middle-income category of the countries have significant inequity in stunting of children favoring the highest wealth quintile. Consistently, our bootstrapped Meta-regression analysis revealed that there is no significant difference in the level of inequity of undernutrition in low, lower-middle, and upper-middle-income countries.
The overall finding implies that there is child undernutrition across the world and it gets worst in low-income countries. However, inequality among the poor and rich is prevalent in countries regardless of their economic category. The poor in low, lower-middle, and upper-middle-income countries are still disadvantaged regardless of the country’s economic status. When we relate this fact with the consequences of undernutrition, the existing situation forces the poor to live in cyclical poverty. If a child is undernourished, she/he will not be performing well in school and at work and consequently will earn less compared to those grown in a better condition45,54,55. Similarly, various chronic health problems and hospital admission among people who have a history of childhood undernourished are higher7,56. The intergenerational effect of undernutrition is also the other issue of concern. A child born from an undernourished mother is at a higher risk of death8, and would be less effective at the workplace57.
The strengths of this study include using nationally representative big sample data from 24 countries, and we did sub-group analysis by place of residence and sex of the child despite other studies focusing only on the wealth of the household. We also checked if there are differences in childhood undernutrition inequality in economically different countries descriptively and using a meta-regression analysis. The limitations include, as we have used DHS data, which is vulnerable to recall bias and may compromise the findings. Moreover, we used the most recent data from 24 countries of which some date back to 2016/17 which may not indicate the country’s current status in child undernutrition and wealth-related inequality.
Conclusion
The findings of our analysis indicated that the magnitude of undernutrition varies across different income category countries, while inequity in all indicators of undernutrition is evident in all three economic groups. Therefore, stakeholders working to address the persistently high level of child undernourishment in low-income countries need to realize the double burden of high prevalence and deep inequality mainly affecting children of disadvantaged communities. Comprehensive interventions that target those the most vulnerable populations are urgently needed. Furthermore, better-off counties with a lesser burden of undernourishment should pay due attention to the unacceptably high equity gap that affects the less advantaged groups within affected countries. More importantly, fighting poverty and targeted treatment of the disadvantaged would potentially decrease undernutrition among the poor in countries of all economic categories.
Data availability
We used publicly available data from the Demographic and Health Survey database upon a reasonable request. Link to the DHS Program website: http://dhsprogram.com/data/available-datasets.cfm.
References
Unicef. UN-IGME-Subnational-Under-five-Mortality-Estimates.pdf. Published online (2021).
Katoch, O. R. Determinants of malnutrition among children: A systematic review. Nutrition 96, 111565. https://doi.org/10.1016/j.nut.2021.111565 (2022).
Ahmad, D., Afzal, M. & Imtiaz, A. Effect of socioeconomic factors on malnutrition among children in Pakistan. Futur. Bus. J. 6(1), 1–11. https://doi.org/10.1186/s43093-020-00032-x (2020).
United Nations Development Program. The SDGs in Action. Published 2023. Accessed 1 May 2023. https://www.undp.org/sustainable-development-goals
Verma, P. & Prasad, J. B. Diabetes & Metabolic Syndrome: Clinical Research & Reviews Stunting, wasting and underweight as indicators of under-nutrition in under five children from developing Countries: A systematic review. Diabetes Metab. Syndr. Clin. Res. Rev. 15(5), 102243. https://doi.org/10.1016/j.dsx.2021.102243 (2021).
Victora, C. G. et al. Revisiting maternal and child undernutrition in low-income and middle-income countries: Variable progress towards an unfinished agenda. Lancet. 397(10282), 1388–1399. https://doi.org/10.1016/S0140-6736(21)00394-9 (2021).
Van Abeelen, A. F. M. et al. Famine in the young and risk of later hospitalization for COPD and asthma. PLoS One. 8(12), 4–11. https://doi.org/10.1371/journal.pone.0082636 (2013).
Khatun, W., Alam, A., Rasheed, S., Huda, T. M. & Dibley, M. J. Exploring the intergenerational effects of undernutrition: Association of maternal height with neonatal, infant and under-five mortality in Bangladesh. BMJ Glob. Heal. 3(6), 1–12. https://doi.org/10.1136/bmjgh-2018-000881 (2018).
Young, E. M. Food and Development (Routledge, 2012).
WHO. Malnutrition. WHO Key Factsheet. Published 2021. Accessed 10 Jun 2022. https://www.who.int/news-room/fact-sheets/detail/malnutrition
WHO. Underweight Among Children Under 5 Years of Age 166–172 Published online (2022).
World BanK. Prevalence of Stunting, Height for Age (% of Children Under 5) (2022).
World BanK. Prevalence of Wasting, Weight for Height (% of Children Under 5) (2022).
Max Roser, H. R. Hunger and Undernourishment. Our world in Data. Published 2019. Accessed 14 Jun 2022. https://ourworldindata.org/hunger-and-undernourishment
Akombi, B. J., Agho, K. E., Renzaho, A. M., Hall, J. J. & Merom, D. R. Trends in socioeconomic inequalities in child undernutrition: Evidence from Nigeria demographic and health survey (2003–2013). PLoS ONE 14(2), 1–13. https://doi.org/10.1371/journal.pone.0211883 (2019).
UNICEF, WHO WB. The UNICEF/WHO/WB Joint Child Malnutrition Estimates (JME) group released new data for 2021.
Vollmer, S., Harttgen, K., Kupka, R. & Subramanian, S. V. Levels and trends of childhood undernutrition by wealth and education according to a composite index of anthropometric failure: evidence from 146 demographic and health surveys from 39 countries. BMJ Glob. Heal. 2(2), 1–8. https://doi.org/10.1136/bmjgh-2016-000206 (2017).
Chowdhury, M. R. K. et al. Prevalence and factors associated with severe undernutrition among under-5 children in Bangladesh, Pakistan, and Nepal: A comparative study using multilevel analysis. Sci. Rep. 13(1), 1–12. https://doi.org/10.1038/s41598-023-36048-w (2023).
Porwal, A. et al. Socio-economic inequality in anthropometric failure among children aged under 5 years in India: Evidence from the Comprehensive National Nutrition Survey 2016–18. Int. J. Equity Health. 20(1), 1–10. https://doi.org/10.1186/s12939-021-01512-4 (2021).
Fenta, H. M., Zewotir, T. & Muluneh, E. K. Disparities in childhood composite index of anthropometric failure prevalence and determinants across Ethiopian administrative zones. PLoS ONE 16, 1–17. https://doi.org/10.1371/journal.pone.0256726 (2021).
Wambua, B. N., Omoke, K. J. & Mutua, T. M. Effects of socio - economic factors on food security situation in Kenyan dry lands ecosystem. Asian J. Agric. Food Sci. 2 (2014).
Matsumura, M. & Gubhaju, B. Women’s status, household structure and the utilization of maternal health services in Nepal. Asia-Pacific Popul. J. 16(1), 23–44 (2001).
Mm, K. Factors associated with being underweight, overweight and obese among ever-married non-pregnant urban women in Bangladesh. Singap. Med. J. 8(50), 804–813 (2009).
Kumar, A., Kumari, D. & Singh, A. Increasing socioeconomic inequality in childhood undernutrition in urban India: Trends between 1992–93, 1998–99 and 2005–06. Health Policy Plan. 30(8), 1003–1016. https://doi.org/10.1093/heapol/czu104 (2015).
Burchi, F. Child nutrition in Mozambique in 2003: The role of mother’s schooling and nutrition knowledge. Econ. Hunger. Biol. 8(3), 331–345 (2010).
de Menezes, R. C. E. et al. Determinants of stunting in children under five in Pernambuco, northeastern Brazil. Rev. Saude Publica 45(6), 1079–1087. https://doi.org/10.1590/S0034-89102011000600010 (2011).
Mk, S. M. Socio-economic determinants of severe and moderate stunting among under-five children of rural Bangladesh. Malays. J. Nutr. 17(1), 105–118 (2011).
Atinmo, T., Mirmiran, P., Oyewole, O. E., Belahsen, R. & Serra-Majem, L. Breaking the poverty/malnutrition cycle in Africa and the Middle East. Nutr. Rev. 67(suppl_1), S40–S46. https://doi.org/10.1111/j.1753-4887.2009.00158.x (2009).
Müller, O. & Krawinkel, M. Malnutrition and health in developing countries. JAMC 173(3), 279–286. https://doi.org/10.1007/s12541-016-0082-0 (2005).
Nada Hamadah, catherine van rompaey eric metreau. New World Bank country classifications by income level: 2021–2022.
Nations TU. Population of Low-Income Countries.
Wikipedia. Demographic and Health Surveys.
Adetunji, J. A., Shelton, J. D. Ethical Issues in the Collection, Analysis and Dissemination of DHS Data in Sub-Sahara Africa 1–21 Published online (2011).
World Health Organization. Global Vaccine Action Plan 2011–2020. (2013). https://doi.org/10.1016/j.vaccine.2013.02.015
The DHS Program. The DHS Program - Available Datasets 1–15 Published online (2011). http://dhsprogram.com/data/available-datasets.cfm
World Health Organization. WHO Anthro Survey Analyser Quick Guide. (2019). https://cdn.who.int/media/docs/default-source/child-growth/child-growth-standards/software/anthro-survey-analyser-quickguide.pdf?sfvrsn=dc7ddc6f_6
Rutstein, S. Steps to construct new DHS Wealth Index. Wealth Index Constr. 6 (2020).
The DHS Program. The DHS Program: Wealth Index. Published 2016. Accessed 1 May 2023. https://dhsprogram.com/topics/wealth-index/#:~:text=Generated with a statistical procedure known as principal,wealth on various population%2C health and nutrition indicators.
Donnell, O. O., Wagstaff, A. & Lindelow, M. Analyzing Health Equity Using Household Survey Data: A Guide to Techniques and Their Implementation (The World Bank, 2008).
CIA. Gini Index Coefficient – Distribution of Family Income.
Mohammed, S. H., Habtewold, T. D., Arero, A. G. & Esmaillzadeh, A. The state of child nutrition in Ethiopia: an umbrella review of systematic review and meta-analysis reports. BMC Pediatr. 20(1), 1–10. https://doi.org/10.1186/s12887-020-02301-8 (2020).
Wuehler, S. E. & Biga, H. A. Situational analysis of infant and young child nutrition policies and programmatic activities in Niger. Matern. Child. Nutr. 7(SUPPL. 1), 133–156. https://doi.org/10.1111/j.1740-8709.2010.00307.x (2011).
Matrins, V. J. B. et al. Long-lasting effects of undernutrition. Int. J. Environ. Res. Public Health 8(6), 1817–1846. https://doi.org/10.3390/ijerph8061817 (2011).
Wells, J. C. et al. The double burden of malnutrition: Aetiological pathways and consequences for health. Lancet 395(10217), 75–88. https://doi.org/10.1016/S0140-6736(19)32472-9 (2020).
Nugent, R., Levin, C., Hale, J. & Hutchinson, B. Economic effects of the double burden of malnutrition. Lancet 395(10218), 156–164. https://doi.org/10.1016/S0140-6736(19)32473-0 (2020).
Singh, S. K., Srivastava, S. & Chauhan, S. Inequality in child undernutrition among urban population in India: A decomposition analysis. BMC Public Health 20(1), 1–15. https://doi.org/10.1186/s12889-020-09864-2 (2020).
Yayo, N. M. Dynamics of inequality in child under-nutrition in Ethiopia. Int. J. Equity Health 20(1), 1–30. https://doi.org/10.1186/s12939-021-01478-3 (2021).
Sanoussi, Y., Ahinkorah, B. O., Banke-Thomas, A. & Yaya, S. Assessing and decomposing inequality of opportunity in access to child health and nutrition in sub-Saharan Africa: Evidence from three countries with low human development index. Int. J. Equity Health 19(1), 1–16. https://doi.org/10.1186/s12939-020-01258-5 (2020).
Nijman, J. & Dennis, Y. Urban inequalities in the twenty first century economy. Appl. Geogr. 117(102188), 1–8 (2020).
Cao, T. & Akita, T. Urban and Rural Dimensions of Income Inequality in Vietnam. (2008). http://ci.nii.ac.jp/naid/110006631256/
S. S. Difference Between Urban and Rural.
Thompson, A. L. Greater male vulnerability to stunting? Evaluating sex differences in growth, pathways and biocultural mechanisms. Ann. Hum. Biol. 48(6), 466–473. https://doi.org/10.1080/03014460.2021.1998622 (2021).
Li, Z., Kim, R., Vollmer, S. & Subramanian, S. V. Factors associated with child stunting, wasting, and underweight in 35 low- and middle-income countries. JAMA Netw. Open 3(4), 1–18. https://doi.org/10.1001/jamanetworkopen.2020.3386 (2020).
O’Connell, S. A. & Smith, C. Economic growth and child undernutrition. Lancet Glob. Health 4(12), e901–e902. https://doi.org/10.1016/S2214-109X(16)30250-9 (2016).
Tzioumis, E. & Adair, L. S. Childhood dual burden of under- and overnutrition in low- and middle-income countries: A critical review. Food Nutr. Bull. 35(2), 230–243. https://doi.org/10.1177/156482651403500210 (2014).
Green, R., Sutherland, J., Dangour, A. D., Shankar, B. & Webb, P. Global dietary quality, undernutrition and non-communicable disease: A longitudinal modelling study. BMJ Open 6(1), 1–9. https://doi.org/10.1136/bmjopen-2015-009331 (2016).
Martorell, R. & Zongrone, A. Intergenerational influences on child growth and undernutrition. Paediatr. Perinat. Epidemiol. 26(SUPPL. 1), 302–314. https://doi.org/10.1111/j.1365-3016.2012.01298.x (2012).
Author information
Authors and Affiliations
Contributions
F.B.: Conceptualization; data curation; formal analysis; investigation; methodology; project administration; supervision; writing original draft; review and editing. K.Y.: Conceptualization; project administration; formal analysis; writing original draft; review and editing. F.T.B.: formal analysis; writing; review and editing. E.A.: supervision; review of the draft manuscript and editing. M.W.: Conceptualization; supervision; review of the draft manuscript and editing. All authors have read and approved the final version of the manuscript, and the corresponding author has full access to all of the data in this study and takes complete responsibility for the accuracy of the data analysis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Birhanu, F., Yitbarek, K., Bobo, F.T. et al. Undernutrition in children under five associated with wealth-related inequality in 24 low- and middle-income countries from 2017 to 2022. Sci Rep 14, 3326 (2024). https://doi.org/10.1038/s41598-024-53280-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-53280-0
- Springer Nature Limited