
Abstract
Breast cancer (BC) screening plays a major role in the prevention of BC through early detection and timely treatment. This study aims to determine the level of uptake of BC screening and associated factors. A community-based analytical cross-sectional study was conducted in Dodoma City, Tanzania from July to December 2020. The study included women aged 8 years and above without a known history of breast cancer. Multivariable logistic regression was used to determine the socio-demographic factors associated with BC screening. P value < 0.05 was considered significant. A total of 354 study participants were included in the present study. The mean age of participants was 31.0 ± 11.8 years. The majority of study participants (67.5%, n = 239) were aware of BC screening. However, only (35.3%, n = 125) reported to have ever practised BC screening. Breast self-examination was the most (16.4%, n = 58) frequently used method for BC screening among study participants. Lack of knowledge of all methods of BC screening was the barrier that was perceived by the vast majority (60.2%, n = 213) of the study participants. Having low family income was the only predictor of failure to practice BC screening. In this study, most of the women were aware of BC, however, few of them had undergone breast cancer (BC) screening at the time of the interview. The study also found that the main barrier to BC screening was the lack of knowledge about BC among the study participants. Immediate measures are necessary to increase women's awareness of BC. Such as community sensitization on the importance of screening, can help improve the uptake of BC screening and the early detection of BC.
Similar content being viewed by others

Introduction
Breast cancer (BC) is the leading cause of cancer-related deaths among women globally and its prevalence is on the increase despite stringent measures that are taken in various countries for its mitigation1,2,3. In 2018, it was reported that 15.3% (over 2 million) of all cancer cases were related to BC and also a total of 685,000 cancer-related deaths among women were due to BC2. Additionally, the global annual incidence rate for BC has been reported to be 5.8% 4. Considering the burden of BC in sub-Saharan Africa, there is underreporting of BC in this region due to a shortage of cancer registries that help in providing cancer-related data. This fact is evidenced by the noticeably disproportionate mortality of BC concerning the low reported burden compared to developed countries5. According to 2020 Global Can Data 186,598 BC cases were reported in Africa with 87,787 BC-related deaths6.
In Tanzania, BC continuously be a devastating disease and remains the second in terms of prevalence and mortality among women. In 2018, it was estimated that 337,000 cases of BC were newly diagnosed with 1303 BC-related related deaths7,8. It is projected that by the year 2040, both the incidence and mortality of BC in Tanzania will escalate by more than 120%9. The data provided concerning the prevalence and incidence of BC in Tanzania do not reveal the actual burden of the disease because most of the studies done in Tanzania are clinicopathologic and only a few of the studies address the epidemiological aspects of the disease in the country, this contributes greatly to underreporting of prevalence, incidence rate, mortality rate and many other epidemiological parameters.
BC screening is of paramount importance in providing secondary prevention of diseases. However, in Tanzania, this is still a challenge due to the substantial lack of BC screening. The only available screening centre at the referral and consultant hospitals do not provide wide coverage for BC screening in the country. This contributes to the late detection of BC among patients10. The reported level of awareness on various issues related to BC among women in most of the developing countries including Tanzania is disproportionate to the level of uptake of BC screening in most developing countries. This is attributed to several factors including having negative perceptions and barriers which both together limit the accessibility of BC screening services for most women. A few studies done in developing countries have reported significantly low uptake of BC screening, for example studies done in Namibia, Ghana, Kenya and Burkina Faso reported 23.1%11, 51.9%4, 12%12, and 7.5%11, respectively.
The uptake of BC screening is influenced by various factors including sociodemographic characteristics, sociocultural factors, health-seeking behaviour, health insurance, knowledge of BC risk factors, and obstetric factors like the number of living children11,13,14,15. Data reporting on BC screening among women in Tanzania is scanty despite the high prevalence, incidence rate and mortality of the disease; this is due to a lack of comprehensive and accessible nationwide BC screening programmes. Therefore, this study aims to assess the prevalence of uptake of BC screening and factors associated as well as barriers to BC screening.
Materials and methods
Study design and area
This was a cross-sectional analytical community-based study using a quantitative approach. The study was conducted in Dodoma City which is located in the Dodoma region for six months (July-December 2020). According to the 2022 Tanzania Housing and Population Census, the estimated population of the Dodoma region was 3,085,625 of whom 1,512,760 and 1,572,865 were males and females, respectively with a fertility rate of 12.2%16, while the number of women with the possibility of giving birth (15–49 years) in the Dodoma region was 5.1%.
Study population
This study included women from different streets in Dodoma city. The inclusion criteria for the study participants were: all women aged 18 years and above, residents of the selected study site for at least 1 year, without having breast cancer, and agreed voluntarily to participate in the study. All women who were very sick, and mentally ill and those who refused to participate in the study were excluded.
Sample size and sampling technique
The sample size was estimated using the formula for calculating the prevalence of a single population established by Kish Leslie17 as was applied in the previous study considering the following assumptions: Standard normal variables (z score) of 1.96 at 95% confidence interval, proportion (p) of women who had BC screening of 51.9% in Ghana4, and 5% level of significance (α = 0.05). The final sample size was adjusted for a non-response rate of 10% and the total sample size estimated was 354. Dodoma city was selected conveniently from seven districts of the Dodoma region. This is because Dodoma is one of the fastest-growing cities in the country, with a high rate of urbanization. This has resulted in a heterogeneous population consisting of people who have migrated from villages to the city. Households were selected using systematic random sampling from which the study participants were obtained. The researchers decided to go on right or left from the starting point. Then the study participants from the households were selected using a simple lottery replacement random sampling method. Pieces of paper were cut and labelled with numbers 1 and 2 and placed in a container which was tightly covered. The container was shaken vigorously to allow the mixing up of the pieces of paper. The container was opened and pieces of paper were poured on the surface to allow the study participants to pick. Those who selected number 2 were recruited in the study.
Definition of variable
BC screening uptake was considered a categorical variable and responses were dichotomized into “yes” and “no”. All study participants who responded “yes” to the question which was asking “Have you ever had BC screening”? to any of the four screening methods (BSE, CBE, Mammography and Ultrasound) were considered to have screened for BC. Additionally, other items were included in measuring BC screening such as “Have you ever heard about BC screening”.
The perceived barrier is the estimation of the level of challenge of social, personal, environmental, and economic obstacles to a specified behavior such as the BC screening procedure.
Factors influencing the uptake of breast cancer screening are attributes that can lead a woman to decide on doing BC screening.
Data collection and research tool
A structured interviewer-administered questionnaire was used for data collection. The questionnaire was adapted from a previous study18 and modified to make it easily understandable including translating it into Swahili local language. A person who was fluent in both English and Swahili was used to translate the questionnaire. To ensure the validity of the questionnaire, we analyzed its internal consistency using Cronbach’s alpha coefficient19. We pretested the questionnaire before and after translation among 30 women from a different site. We modified some of the questions that were not clear. We validated the questionnaire based on a Cronbach’s alpha value of ≥ 0.719. In this study, we found Cronbach’s alpha of 0.714 and 0.823 for perceived barrier and practice of breast cancer screening, respectively, which shows that the questionnaire is reliable.
There were three parts in the questionnaire which consisted of sociodemographic characteristics, practices of BC screening, and barriers for BC screening. The face-to-face interviewer method was used to collect the required data. Four research assistants (registered nurses) with experience in data collection were involved in the process of data collection. To avoid participants sharing information, the interview was done at a bit far distance. Approximately, it took 15 to 20 min for one participant.
Data analysis
Data were analysed using SPSS software version 25.0. Descriptive statistics were used to summarize both categorical and continuous variables in frequencies and percentages and mean ± standard deviation (SD), respectively. Inferential statistics involved the use of binary logistic regression analysis in determining the predictors of BC screening. All variables with p ≤ 0.2 in univariate analysis were fitted into multivariable analysis for controlling confounding factors. Odds ratios (ORs) at 95% confidence interval (CI) were determined to assess the predictability of the independent variables. A two-tailed p < 0.05 was considered statistically significant.
Ethical approval
Ethical approval from the Research Ethical Committee of the University of Dodoma was obtained prior to data collection. All the methods were performed in accordance with relevant institutional guidelines and regulations.
Informed consent
Written informed consent was obtained from all study participants.
Results
Sociodemographic characteristics of the study participants
The social demographic characteristics of the study participants are shown in Table 1. A total of 354 study participants’ data were analysed in the present study. The mean age of the study participants was 31.0 ± 11.8 years (range: 18–85 years). The majority 72.3% (n = 256) of study participants were in the age group between 18 and 34 years. Almost half of the study participants 45.5% (n = 161) had primary education. Also, the vast majority 62.7% (n = 222) of the study participants had a family income of less than 1.4 USD (100,000 TZS) per day. Additionally, over half 57.3% (n = 203) of the study participants were married.
Awareness and uptake of BC screening among study participants
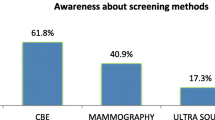
Concerning awareness of BC screening among participants, the majority 67.5% (n = 239) of the study participants reported being aware of BC screening (mean = 13.2, 95% CI = 12.8–13.7). Almost one-third 35.3% (n = 125) of the study participants reported they had ever screened for BC (mean = 35.3, 95% CI = 30.3–40.3). The most frequently used method for BC screening was breast self-examination, which comprised 16.4% (n = 78), followed by clinical breast examination which accounted for 14.7% (n = 52). Mammography was the least 1.4% (n = 5) used method for BC screening in this study. Of those who reported having had BC screening, most of them 19.5% (n = 69) could have BC screening at any time and only 8.8% (n = 31) of the study participants had BC screening by using breast self-examination method every month for women who aged ≥ 20 years, which is the recommended time interval for BC screening20. Furthermore, it was found that those who practised breast self-examination, only (n = 10, 2.8%) were found to perform breast self-examination between 2 and 3 days after menstruation, which is recommended for women who are still getting menstruation and regularly on a monthly bases for menopausal or postmenopausal women20 (Table 2).
Perceived barriers to BC screening among study participants
Table 3 shows the perceived barriers to BC screening. Lack of knowledge of BC was the barrier that was perceived by the vast majority 60.2% (n = 213) of the study participants. Lack of money was the second most 52.5% (n = 186) common perceived barrier by the study participants. Lack of privacy during BC screening was the least 16.4% (n = 58) perceived barrier for BC screening among participants.
I. Multivariable regression analysis for factors associated with BC screening among study participants
After controlling for confounders (age, level of education, marital status, religion, and awareness of breast cancer) in multivariable regression analysis, only family income remained statistically significantly associated with BC screening. Study participants with family income less than 100,000 TZS per month equivalent to less than 1.4 USD per day had a 73% significantly less chance of BC screening (95% CI = 0.08–0.93, p = 0.038). Likewise, study participants who had family income between 100,000 and 500,000 TZS per month had 75% significantly less chance of BC screening (95% CI = 0.07–0.88, p = 0.031). Religion showed marginal statistical significance with BC screening in which study participants who were either Christians 3.97 (95% CI = 0.86–18.38, p = 0.078) or Muslims 4.44 (95% CI = 0.94–20.89, p = 0.060) had increased odds of BC screening compared with study participants that had traditional beliefs even though the difference did not reach statistical significance.
Another variable that showed marginal statistical significance with BC screening was level of education, whereby study participants with primary education had 53% less chance of BC screening (95% CI = 0.21–1.05, p = 0.064). Other variables including age, marital status, and awareness of BC screening although did not show a statistical association with BC screening, still they showed a trend of increased odds towards BC screening (Table 4).
Discussion
Breast cancer screening helps early detection, particularly in settings where treatment modalities for breast cancer are still an enigma. This greatly contributes to the red flag of poor clinical outcomes of the patients with BC as a result of late detection of the disease. We aimed to determine the level of uptake of BC screening and factors associated as well as barriers to BC screening in Dodoma city which is a rapidly growing city in Tanzania. The main findings in this study include a low level of uptake of BC screening and the association of low family income with low uptake of BC screening. Additionally, lack of knowledge of BC among study participants was reported to be the major barrier to BC screening.
Although BC screening has been found to significantly reduce the burden of BC and also improve clinical outcomes of patients through early detection, the uptake of BC screening in developing countries is still significantly low. This contributes to late detection and poor outcomes for patients with BC in most developing countries. The uptake of BC screening of 35.3% obtained in this study was similar to the 33.8% uptake of BC screening which was reported in a study done by Emma et al. in Tanzania18 but lower than 51.9% of uptake of BC screening reported in Ghana 4. However, other studies done in Indonesia, Nigeria, and Saudi Arabia reported significantly low levels of uptake of BC screening 18.7%15, 9.9%21, 16.2%22, respectively. Despite Ghana and Tanzania being low-middle income countries, the prevalence of modern FP use in Ghana was associated with the difference in the age of study participants, the Ghanaian study included the population of young reproductive age, such women are more likely to have more knowledge.
One of the reasons for the discrepancy in the uptake rates for BC screening observed in various studies is due to the difference in methods of BC screening used, for example, studies which used a single method of BC screening, particularly mammography have reported significantly low rate of uptake of BC screening21, this may be explained by the fact that the coverage of the availability of mammography in most of developing countries is still a challenge which prompts utilization of other methods of BC screening. The disproportion of awareness of BC and uptake of BC screening observed in different studies helps to explain the existing discrepancy in the uptake rates of BC screening in various studies. There is a larger number of studies which have reported a high level of awareness of BC screening among women in both developed and developing countries which is not reflected by the level of uptake of BC screening. This is evidenced by high level of awareness of BC screening in this study, however, the uptake rate of BC screening was significantly low similar to the findings in the studies done by Emma et al. and Alshahrani et al.18,23. Socio-cultural factors and beliefs could also influence the uptake of BC screening among participants in a given study. In countries that exercise strict social and cultural norms for example interaction of women with men has been found to have a low uptake rate of BC screening despite being developed22,24.
Various sociodemographic factors have been found to influence the uptake of BC screening among women. In this study, it was found that women who had low family income had reduced odds for BC screening. This indicates that women in families with high family income have high chance of screening for BC. Other studies have also reported a positive association between low family income and reduced uptake of BC screening15,22,25,26,27. Good family income plays a major role in facilitating BC screening among women through various ways including transport, access to media such as new paper, internet and television, and attending seminars among many others28,29. Additionally, it has been found that good income is linked with good socioeconomic status such high level of education, health insurance, and marital status which all together influence positively BC screening28,30.
The association of formal education with BC screening among women has been reported by many studies albeit few studies which have reported a converse relationship between the two variables. In this study women with education level ranging from primary to tertiary had increased odds of BC screening compared to women with informal education. This was also observed in the studies of Ayanore et al.,29, Opoke et al.31, Mousavi et al.32, and Islam et al.33. High level of formal education which is one of the indicators of high socioeconomic status has a positive influence on health-seeking behaviour. Women who acquire formal education in their lifetime tend to increase the possibility of engaging themselves in various health-seeking behaviours including BC screening, unlike women who are not privileged to obtain formal education in their life. This is reflected by low rate of uptake BC screening among women residing in rural areas where there is a challenge of getting formal education29,34,35.
Awareness is a standalone factor in prevention of diseases including BC through screening. Increased awareness of BC significantly improves early detection of BC which in turn helps to improve the clinical outcome of patients with BC. In this study, it was observed that women who were aware of BC were 3 times more likely to embark on BC screening compared with women who were not aware of BC. This was also found in the studies of Ngani et al.27, Solika et al.15, and Abiyu et al.36. In any community globally, it is highly stipulated that raising awareness among people in a given community is mandatory as a primary prevention approach of diseases that is why the World Health Organization (WHO) as well as Centre for Disease Control (CDC) and many other global health organizations emphasis on the importance of these disease prevention approach37,38.
Barriers to BC screening contribute largely to inadequate screening practices among women especially in developing countries. This leads to delay early detection of BC and contribute to increased morbidity and poor prognosis. Early detection of BC aids in timely presentation of symptomatic BC for treatment and down-staging39. For both qualitative and quantitative studies done previously, it has been clearly shown that lack of awareness and knowledge of BC among women is associated significantly with failure of most women to screen for BC globally11,22,28,40 which is similar to the finding in this study. This experience is even more common in developing countries such as Tanzania where provision of public health is still a challenge. The observed high percentage of women that lack awareness and knowledge of BC in developing countries is attributed to lack of formal education among women.
Challenges with family income and not having BC were other factors that were perceived as barriers to BC screening among study participants in the present study. Similarly, other two previous studies29,41 reported that low family income hinders women from accessing health facilities for BC screening, having ability to own sources of information such as television22. Studies have shown that, women who perceive that have no BC do not see the importance of going or practising BC screening42. Others fear of BC screening because they are afraid of receiving a positive diagnosis43. It is imperative to have a holistic approach in improving means of raising awareness and knowledge of BC among women so as to change their minds towards BC screening.
Our study had some limitations. One of the limitations was that in this study it was not possible to analyze the uptake of BC screening for each screening method because some of the methods for example, mammograph and ultrasound were used by very few study participants. This limited us to perform regression analysis and for that reason we could not determine the factors associated with uptake with BC as per specific screening methods. Another limitation was that the uptake of BC screening was self-reported which is usually associated with information bias. Selection of the study subjects was by using convenience sampling method, this might have contributed to selection bias. Also, our findings lack generalizability due to the reason that, participants were taken from one area making the sample not representative of the whole country.
Conclusion
This study revealed that the majority of women were aware of BC. However, few of them reported to practise BC screening by the time when they were interviewed. Additionally, it was observed that lack of knowledge of BC among study subjects was the main barrier towards BC screening. From these findings, it can be learned that the rate of uptake of BC screening is still quite low and therefore, immediate measures including increasing the level of women’s awareness of BC to improve the uptake of BC screening and increase early detection of BC as well. We also recommend further study that will be more objective with a valid and sensitive instrument to enable more analytical process with a larger population of respondents.
Data availability
The dataset used for this study can only be accessed upon reasonable request from the corresponding author.
References
World Health Organization. Breast cancer. 2021.
World Health Organization. Current and future burden of breast cancer: global statistics for 2020 and 2040. 2022.
Osei-Afriyie, S. et al. Breast cancer awareness, risk factors and screening practices among future health professionals in Ghana: a cross-sectional study. PLoS ONE 16(6), 1–17 (2021).
Wuur, M. M., Duodu, D. A. & Tarkang, E. E. Factors that influence breast cancer screening among women of reproductive age in the Nandom Municipality Ghana. BMC Womens Health 22, 1–8 (2022).
GRACE NHCVRM. New World Bank country classifications by income level: 2022–2023. 2022.
Anyigba, C. A., Awandare, G. A. & Paemka, L. Breast cancer in sub-Saharan Africa: the current state and uncertain future. Exp. Biol. Med. 246, 1377–1387 (2021).
Chao, C. A. et al. Understanding women’s perspectives on breast cancer is essential for cancer control: Knowledge, risk awareness, and care-seeking in Mwanza Tanzania. BMC Public Health 20, 1–11 (2020).
Mayor, S. Service review: improving breast cancer care in Tanzania. Lancet Oncol. 18, 430 (2017).
Breast Cancer Initiative. Tanzania Breast Health Care Assessment 2017: An assessment of breast cancer early detection, diagnosis and treatment in Tanzania. Available https://ww5.komen.org/breastcancertanzania. 2017;:1–62.
Philipo, G. S. et al. Feasibility of fine-needle aspiration biopsy and rapid on-site evaluation for immediate triage in breast cancer screening in Tanzania. JCO Glob. Oncol. https://doi.org/10.1200/GO.20.00279 (2021).
Ba, D. M. et al. Prevalence and determinants of breast cancer screening in four sub-Saharan African countries: a population-based study. BMJ Open. 10, 1–8 (2020).
Antabe, R., Kansanga, M., Sano, Y., Kyeremeh, E. & Galaa, Y. Utilization of breast cancer screening in Kenya: What are the determinants?. BMC Health Serv Res. 20, 1–9 (2020).
Marmarà, D., Marmarà, V. & Hubbard, G. Health beliefs, illness perceptions and determinants of breast screening uptake in Malta: a cross-sectional survey. BMC Public Health. 17, 1–19 (2017).
Akuoko, C. P. et al. Barriers to early presentation and diagnosis of breast cancer among African women living in sub-Saharan Africa. PLoS One. 12, 1–18 (2017).
Solikhah, S., Lianawati, L., Matahari, R. & Rejeki, D. S. S. Determinants of breast cancer screening practice among women in Indonesia: a nationwide study. Asian Pacific J Cancer Prev. 22, 1435–1441 (2021).
National Bureau of Statistics. Nukuu :Mipango, Wizara ya Fedha na Takwimu, Ofisi ya Taifa ya Tanzania Na Ofisi ya Rais, Fedha na Mipango Serikali, Ofisi ya Mtakwimu Mkuu wa Zanzibar. 2022.
Kish, L. Sampling survey (John WIley & sons, 1965).
Morse, E. P., Maegga, B., Joseph, G. & Miesfeldt, S. Breast cancer knowledge, beliefs, and screening practices among women seeking care at district hospitals in dar es Salaam, Tanzania. Breast Cancer (Auckl) https://doi.org/10.4137/BCBCR.S13745 (2014).
Taber, K. S. The use of cronbach’s alpha when developing and reporting research instruments in science education. Res. Sci. Educ. 48, 1273–1296 (2018).
Bk, M. & Kaphle, H. P. Breast self-examination: Knowledge, practice and associated factors among 20 to 49 years aged women in Butwal sub-metropolitan, Rupandehi Nepal. PLoS ONE 18(6), e0286676 (2023).
Nja, G. M. et al. Socio-demographic determinants of mammography uptake among women of 40 years and above in Calabar, South-South, Nigeria: a cross-sectional study. Pan African Med. J. https://doi.org/10.11604/pamj.2022.43.76.32683 (2022).
Abdel-Aziz, S. B. et al. Perceived barriers to breast cancer screening among Saudi women at primary care setting. Asian Pacific J. Cancer Prev. 18, 2409–2417 (2017).
Alshahrani, M. et al. Knowledge, attitudes, and practices of breast cancer screening methods among female patients in primary healthcare centers in Najran Saudi Arabia. J. Cancer Educ. 34, 1167–1172 (2019).
Altirifi HI, Elsanousi OM, Bedri S. 2022 Very poor practices regarding breast cancer screening among Sudanese female workers at a secondary-level hospital: a cross-sectional study. Pan Afr Med J. 41.
Kangmennaang, J., Mkandawire, P. & Luginaah, I. Breast cancer screening among women in Namibia: explaining the effect of health insurance coverage and access to information on screening behaviours. Glob. Health Promot. 26, 50–61 (2019).
Maheswaran, R., Pearson, T., Jordan, H. & Black, D. Socioeconomic deprivation, travel distance, location of service, and uptake of breast cancer screening in North Derbyshire, UK. J. Epidemiol. Commun. Health 60(3), 208–212 (2006).
Ngan, T. T., Jenkins, C., Minh, H. V., Donnelly, M. & O’Neill, C. Breast cancer screening practices among Vietnamese women and factors associated with clinical breast examination uptake. PLoS ONE 17(5), e0269228 (2022).
Karimi, S. E., Rafiey, H., Sajjadi, H. & Nejad, F. N. Identifying the social determinants of breast health behavior: a qualitative content analysis. Asian Pacific J. Cancer Prevent.: APJCP. 19(7), 1867 (2018).
Ayanore, M. A. et al. Self-reported breast and cervical cancer screening practices among women in Ghana : predictive factors and reproductive health policy implications from the WHO study on global AGEing and adult health. BMC Women’s Health https://doi.org/10.1186/s12905-020-01022-5 (2020).
Coughlin, S. S. Social determinants of breast cancer risk, stage, and survival. Breast Cancer Res. Treat. https://doi.org/10.1007/s10549-019-05340-7 (2019).
Lasong, J. et al. Determinants of modern contraceptive use among married women of reproductive age: a cross-sectional study in rural Zambia. BMJ Open. 10, 1–10 (2020).
Mousavi, F. & Shojaei, P. Health belief model and determinants of breast self-examination performance. Int. J. Cancer Manag. https://doi.org/10.5812/ijcm.111509 (2021).
Islam, R. M., Billah, B., Hossain, M. N. & Oldroyd, J. Barriers to cervical cancer and breast cancer screening uptake in low-income and middle-income countries: a systematic review. Asian Pacific J. Cancer Prevent.: APJCP. 18(7), 1751 (2017).
Westgard, C. M., Rogers, A., Bello, G. & Rivadeneyra, N. Health service utilization, perspectives, and health-seeking behavior for maternal and child health services in the Amazon of Peru, a mixed-methods study. Int. J. Equity Health 18, 1–2 (2019).
Agbokey F, Kudzawu E, Dzodzomenyo M, Ae-ngibise KA, Owusu-agyei S, Asante KP. Knowledge and Health Seeking Behaviour of Breast Cancer Patients in Ghana. 2019;2019.
Assefa, A. A., Abera, G. & Geta, M. Breast cancer : targets and therapy breast cancer screening practice and associated factors among women aged 20–70 years in Urban settings of SNNPR. Ethiopia 13, 9–19. https://doi.org/10.2147/BCTT.S286441 (2021).
WHO. Health promotion and disease prevention through population-based interventions, including action to address social determinants and health inequity. 2023.
CDC. Global Health Strategy.
Ginsburg, O. et al. Breast cancer early detection: a phased approach to implementation. Cancer 126, 2379–2393 (2020).
Srinath, A., Van Merode, F., Rao, S. V. & Pavlova, M. Barriers to cervical cancer and breast cancer screening uptake in low- and middle-income countries: a systematic review. Health Policy Plan. 38, 509–527 (2023).
Islam, R. M., Bell, R. J., Billah, B., Hossain, M. B. & Davis, S. R. Awareness of breast cancer and barriers to breast screening uptake in Bangladesh: a population based survey. Maturitas. 2016(84), 68–74 (2013).
Mascara, M. & Constantinou, C. Global perceptions of women on breast cancer and barriers to screening. Curr. Oncol. Reports 23, 1–9 (2021).
Loving, V. A., Aminololama-Shakeri, S. & Leung, J. W. T. Anxiety and its association with screening mammography. J. Breast Imaging 3, 266–272 (2021).
Funding
This work did not receive financial support from any source.
Author information
Authors and Affiliations
Contributions
AAJ, MBM, TJM, JJY: conception, designing, and data curation, AAJ, JJ: methodology, statistical analysis, and writing the first draft of the manuscript. All authors reviewed the manuscript critically before submission for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Joho, A.A., Mdoe, M.B., Masoi, T.J. et al. Perceived barriers and factors influencing uptake of breast cancer screening among women: a population-based cross-sectional study. Sci Rep 14, 12291 (2024). https://doi.org/10.1038/s41598-024-62218-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-62218-5
- Springer Nature Limited