
Abstract
Alcohol production and consumption have been prohibited in Iran for over four decades, leading to a typical underestimation of its consumption. This study aimed to assess the prevalence of alcohol consumption, its associated factors, and estimate per capita alcohol consumption among Iran’s adult population. In this population-based survey, 27,874 adults from across Iran were selected using systematic proportional-to-size cluster sampling. Alcohol consumption was evaluated through a modified Persian version of the STEPS questionnaires from previous studies, applied over different timespans. Per capita consumption was calculated using the quantity-frequency method, expressed in liters of pure alcohol. Adjusted odds ratios were reported for associates of alcohol consumption concerning metabolic risk factors, sociodemographic elements, and lifestyle variables. The prevalence of lifetime alcohol consumption was 6.9% (95% CI 6.5–7.2) in the adult population, with a notable sex difference (males: 13.7% [95% CI 13–14.4]; females: 1.4% [95% CI 1.1–1.6]). The 12 month prevalence was 3.8% (95% CI 3.6–4.1). For individuals aged 18 and older, the per capita alcohol consumption in Iran was 0.12 L. Factors such as being a lifetime smoker, younger, wealthier, and having 7–12 years of education were significantly linked to higher alcohol consumption. Significant associations were also observed between alcohol consumption and having a history of heart attacks (OR = 2.04, 95% CI 1.44–2.89), and physical injuries (OR = 1.88, 95% CI 1.34–2.64). The estimated lifetime and 12-month prevalence of alcohol use in our study were higher among some of the subpopulations. The findings also revealed a complex relationship between alcohol consumption, behavioral risk factors, and metabolic profiles. Consequently, immediate preventive measures tailored to each factor’s association with alcohol use are recommended.
Similar content being viewed by others

Introduction
Globally, the harmful use of alcohol is responsible for 3 million deaths every year, which represents 5.3% of all deaths1. The recent Global Burden of Diseases (GBD) study identifies alcohol as the primary risk factor for the 25–49 age group regarding attributable burden2,3. Between 2010 and 2019, there was an annualized increase of 0.5% in alcohol use, contributing to a significant rise in the percentage of attributable Disability-Adjusted Life Years (DALYs)2,4. Alcohol per capita consumption (APC), the total amount of pure alcohol consumed by individuals5, has risen from 5.4 L in 2005 to 6.2 L in 2018 among individuals aged over 15 years worldwide6,7. Research indicates a link between alcohol consumption and various non-communicable diseases (NCDs), mental and behavioral disorders, and injuries, including road traffic incidents, drowning, poisoning and falls8. Additionally, the consumption of bootleg or adulterated alcohol can lead to methanol poisoning, causing hospitalizations and deaths9,10. The harmful use of alcohol also leads to significant social and economic losses to individuals and society1.
In Iran, a Muslim-majority country in the Middle East, alcohol production, consumption, and trade are criminalized11. Also, there is a social stigma linked to alcohol consumption in this country12. These factors contribute to lower APC and prevalence of alcohol use in Iran compared to majority non-Muslim countries10. However, they have also delayed comprehensive scientific research and healthcare policy development13,14. Despite the alcohol ban, alcoholic beverages have the potential to be illicitly manufactured in residential settings and illegally transported into the country, subsequently being distributed through underground channels15. Consequently, there is no official data on the production or sales of alcoholic products15,16.
To the best of our knowledge, few studies have measured Iran’s APC, and up-to-date information about alcohol consumption in Iran is limited9,16,17,18,19. However, the increasing trend of alcohol consumption20, alongside its association with various NCDs and mental disorders, necessitates a current and detailed report to formulate appropriate population-wide policies and action plans. This study aims to determine the prevalence of alcohol consumption among Iran's adult population, classified by demographics and socio-economic status, and estimate the APC to assess the pattern of alcohol use in 2021. Understanding these patterns is crucial for health authorities to combat the harmful use of alcohol and its extensive negative impacts.
Materials and method
The World Health Organization (WHO) initiated the STEPwise Approach to NCD Risk Factor Surveillance (STEPS) in 2000, offering a standardized method for global data collection, processing, and dissemination21. STEPS is a large-scale, population-based, sequential cross-sectional study that continuously monitors key risk factors for NCDs. In Iran, eight surveys have been conducted based on the WHO STEPS methodology22. The current study is part of the most recent STEPS, carried out in 202123. The data collection phase comprised three steps: first, data were collected using the STEPS questionnaire through participant interviews; second, physical examinations were conducted; and third, laboratory assessments were performed on adults over 2523.
Study population
Data collection began in January 2020 and was partially completed by February 2020, when it was suspended due to the COVID-19 outbreak in Iran. It resumed approximately a year later with COVID-19 safety measures in place, and the remaining data were collected between February and April 2021. A total of 28,520 individuals from urban and rural areas across all 31 provinces of Iran were selected using a multistage clustered probability design to create a nationally representative sample. Of these, 27,874 chose to participate in the first step, 27,745 in the second, and 18,119 in the third. The primary reason for non-response was unwillingness to participate. All participants were at least 18 years old and resided in urban or rural areas of one of the 31 provinces of Iran at the time of data collection. Individuals with mental disorders who might not be able to complete the questionnaires, people whose physical conditions prevented them from participating in an anthropometry measurement, people who were unable to provide laboratory samples, and pregnant women were excluded from the study. After obtaining written informed consent, trained in-home interviewers collected a broad range of information on sociodemographic characteristics, household assets, healthcare utilization, health behaviors, history of metabolic risk factors, anthropometric measures, and laboratory data (only for individuals aged ≥ 25 years).
All of the core questions of the WHO STEPS questionnaire and most of the expanded questions were included in this survey’s questionnaire. Also, due to national concerns and policies for the prevention and control of NCDs, some modified and newly added questions were included in the questionnaire. A team of experts in the fields of epidemiology, population health sciences, health education, medicine, oral health, geriatrics, and nutrition was formed to design and validate STEPS 2021 questionnaires in Iran. The protocol was explained comprehensively, and with further details elsewhere23.
Alcohol consumption assessment
For the alcohol consumption assessment part of the STEPS study, a Persian-translated version of earlier STEPS questionnaires, modified for the Iranian cultural and religious context, was used23. Alcohol consumption prevalence, a key variable of this study, was assessed over three timespans: lifetime, past 12 months, and past 30 days. Binge drinking was also measured over the past 12 months and 30 days, using the Bettering the Evaluation and Care of Health (BEACH) definition of consuming six or more standard drinks on one occasion24. In line with the STEPS protocol, we used a regular cup (approximately 250-300 cc) as the standard measure for beer and wine, and a smaller cup (about 50 cc) for hard liquors such as vodka, whiskey, tequila, cognac, rum, and their domestic equivalents.
APC, another main variable, is defined as the total amount of alcohol consumed in liters of pure alcohol by the population over 15 years old in a calendar year25. As our study included individuals aged 18 and older, we reported the APC for the 18 + age group. Several methods exist to calculate APC9,26. The social stigma toward alcohol consumption in Muslim-majority countries and the low prevalence and frequency of alcohol use led to an underestimation of methods such as yesterday and last week27,28. As a result, the method that we employed in this study is the Quantity-Frequency (QF) method, which is one of the preferred methods to calculate APC in Muslim-majority countries with very low drinking levels9. QF is among the earliest methods to assess alcohol use and is most useful when information about occasional high and low drinking days is not required and time is limited29. We employed the below formula of the QF method for calculating APC:
In this formula, F represents the frequency of alcohol consumption, which we asked questions about in the past 12 months during this study, Q is the amount of alcohol consumed in a typical day of drinking, and α is a constant number that refers to the amount of pure alcohol per alcoholic drink. We used the Iranian Ministry of Health’s routinely used definition of a standard drink, which is 13 g of pure alcohol9. APC was calculated by multiplying the estimated number of drinking days in the past 12 months by the daily quantity of drinks and then multiplying the result by 13 to calculate the total alcohol consumed annually in grams.
Definition of variables
For socioeconomic stratification in this survey, the Wealth Index (WI) was computed based on data regarding household assets obtained from questionnaires. This index was then divided into five levels, ranging from the least wealthy (first quintile) to the most wealthy (fifth quintile). Education levels were recorded in four distinct categories: none, 1–6 years, 7–11 years, and 12 or more years. The living environment of the participants was classified as either urban or rural. The ages of the participants were grouped into seven brackets: 18–24, 25–34, 35–44, 45–54, 55–64, 65–70, and above 70. BMI was calculated using the evaluated height and weight for each individual entered the second step of the study. Obesity was defined as a Body Mass Index (BMI) of more than 30 according to references30.
The cardiometabolic conditions and other diseases assessed in this study were identified based on participants' self-reports of having the condition or taking medication for its treatment, as outlined in the questions of the STEPS questionnaire tool. The history of heart attacks variable was investigated via related questions in the questionnaire asking whether the individual had a history of heart attacks in his/her lifetime or not. The physical injuries variable was assessed via the same method and considered positive if the individual reported a history of physical injury(s) during the past 12 months prior to the study.
Data analysis
Data cleaning adhered to WHO STEPS guidelines21, and due to the complex design of the study, statistical analyses were performed using the ‘survey’ package in R software version 4.0.5 to provide weighted estimations based on the most recently available data on the population of Iran, extracted from the Iran Census 201623. We considered p-values below 0.05 as statistically significant. Baseline characteristics were presented using weighted means (standard deviation (SDs)) for continuous variables and numbers (weighted percentages) for categorical variables. To investigate the association between sociodemographic characteristics and alcohol consumption and the association between alcohol consumption and the non-communicable diseases investigated in this study, we used multiple and univariate logistic regression models to estimate odds ratios (ORs) and 95% confidence intervals (CIs). Initially, each variable was analyzed using a bivariate regression model. Subsequently, a multiple model was developed, incorporating multiple variables informed by the results of the bivariate analysis. Bivariate analyses were performed to estimate crude ORs, and all variables with p-value < 0.2 (including age, sex, wealth index, level of education and smoking, and conditions of diabetes, hypertension, hypercholesterolemia, history of heart attack(s), stroke, physical injuries, and obesity) entered the multiple model to calculate adjusted ORs.
Ethical considerations
All eligible individuals were informed about the study's objectives and methods. Participation was voluntary, with written consent obtained from all participants. Ethical approval was granted by the ethics committee of Tehran University of Medical Sciences (IR.TUMS.NIHR.REC.1398.006). The funding source played no role in the study’s design, data collection, analysis, interpretation, manuscript writing, or decision to submit the paper.
Results
Overview
The study included 27,874 adults aged 18 and older (mean age (SD): 45.7 (0.1); 55.4% females). Among these participants, 43.6% had more than 12 years of education, and 75% were urban residents.
Alcohol consumption scale of Iran’s population
The mean lifetime alcohol consumption prevalence was 6.9% (95% CI 6.5–7.2) for the entire population, 1.4% (95% CI 1.1–1.6) for females, and 13.7% (95% CI 13–14.4) for males. Using the Quantity-Frequency (QF) method, the study calculated the Alcohol Per Capita Consumption (APC) as 0.120 L of pure alcohol (95% CI 0.081–0.159). The 12 month prevalence of alcohol consumption was 3.8% (95% CI 3.6–4.1), with 0.9% for females (95% CI 0.7–1) and 7.5% for males (95% CI 7–8.1). In the past 30 days, 2.1% of participants (95% CI 1.9–2.2) reported alcohol consumption, with 0.5% females (95% CI 0.3–0.6) and 4% males (95% CI 3.6–4.4). The overall prevalence of binge drinking in the past 12 months was 1.7% (95% CI 1.5–1.8) (Table 1). Males were nearly four times more likely to consume alcohol than females (OR 3.8, 95% CI 3–4.9) (Table 2). The highest alcohol consumption rates, including binge drinking, were observed in the 18–24 and 25–34 age groups, decreasing with age. In all age groups, males had higher prevalence rates than females (Table 1).
Associates of alcohol consumption
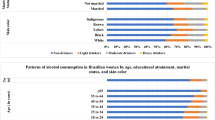
Table 2 shows the crude and adjusted odds ratios for sex-categorized variables. Generally, the adjusted odds for lifetime alcohol consumption were significantly higher among males (OR = 3.84, 95% CI 2.99–4.94), smokers (OR = 4.17, 95% CI 3.58–4.85), and the wealthiest compared to the poorest (OR = 1.49, 95% CI 1.18–1.87) (Fig. 1). Also, it has been shown that the adjusted odds of lifetime alcohol consumption significantly decrease with age (OR = 0.98, 95% CI 0.97–0.98). Individuals with 7–12 years of education had the highest odds of alcohol consumption (OR = 2.23, 95% CI 1.58–3.15).

Forest plot of lifetime alcohol consumption correlates and associated metabolic diseases and risk factors analyzed by adjusted ORs.
Multivariable logistic regression revealed that individuals reporting lifetime alcohol consumption had significantly greater odds of having a history of heart attacks (OR = 2.04, 95% CI 1.44–2.89), and physical injuries (OR = 1.88, 95% CI 1.34–2.64). The study also found positive associations between lifetime alcohol consumption and certain metabolic diseases and risk factors, but negative associations with stroke and diabetes. However, these associations were not significant (Table 3, Fig. 1).
Discussion
This study evaluated alcohol consumption prevalence among Iranians aged 18 and older. The findings indicate that approximately 3.9 million and 2.2 million individuals over 18 in Iran have consumed alcohol at least once in their lifetime and in the past 12 months, respectively.
The lifetime and 12 month prevalence rates of alcohol consumption in our study are lower than the global average but higher than the figures estimated by the WHO for EMR countries6. It’s important to note that the WHO’s estimates refer to populations aged over 15 years. Additionally, our study showed a lower lifetime prevalence of alcohol consumption than that reported in four Iranian provinces in 201515. Part of this difference can be attributed to the setting of the studies. The 2015 study was a street-based study, and the participants faced less stigma when disclosing facts about their alcohol consumption. Essentially, the prohibition of alcohol consumption in Iran and other Muslim-majority countries usually leads to under-reporting of alcohol use17,31. Our study likely reflects this difference, which is due to underreporting and suggests that the actual prevalence may be higher than reported. Compared to other countries, the prevalence of binge drinking in the last month and last 12 months was notably lower in our study32,33,34.
A higher prevalence of alcohol consumption was observed in male participants compared to females, aligning with both national9,15,35, and international studies6,36,37. This gender disparity in alcohol consumption could be attributed to cultural and religious norms, as women typically adhere more closely to cultural and religious principles that discourage alcohol use37. Consistent with other research, our study found that binge drinking was more prevalent among males38,39,40,41.
This study indicates that the highest prevalence of alcohol consumption in the past month, past 12 months, and over a lifetime occurred in the 18–34 age group for both sexes. The higher prevalence of alcohol consumption in this age group is likely influenced by various developmental and cultural factors42. Young adults are prone to consuming larger quantities of alcohol, leading to more adverse effects, and individuals between 20 and 34 years old experience the highest mortality rates related to alcohol consumption43.
The results also demonstrated that alcohol consumption prevalence is higher among cigarette smokers across all age groups. Correspondingly, higher instances of binge drinking were noted among smokers, aligning with research showing a link between tobacco and alcohol use44.
Moreover, a greater prevalence of alcohol consumption was observed among urban residents and individuals with higher education levels, highlighting the impact of social factors, living conditions, and education on alcohol consumption in Iran. Studies within Iran have shown similar patterns, with higher alcohol consumption among high school and university students45,46,47. These findings are consistent with results from other countries48,49,50. Research on the geographical relationship with alcohol consumption presents mixed results; some studies report higher consumption in urban areas51, while others find increased consumption in rural settings52.
In our study, individuals with a higher wealth index exhibited increased alcohol consumption, with the wealthiest group consuming 1.5 times more than those in the lowest wealth index category. Numerous studies have established a direct association between socio-economic status and alcohol consumption, yet an inverse relationship exists between harmful drinking patterns, such as binge drinking, and socio-economic status53,54,55,56,57,58.
Research indicates that in societies where alcohol consumption is stigmatized due to legal and religious prohibitions, as well as criminalization, there is a tendency for alcohol users to underreport their usage. This underreporting is particularly pronounced when questions pertain to recent consumption (past day or week), while queries about the past month or year tend to yield more accurate results. In contrast, in countries without such prohibitions, questioning about last day or week alcohol consumption tends to be more reliable, effectively addressing recall bias and serving as a better tool for calculating APC9,28,59. Given the legal and social stigma associated with alcohol in Iran, our survey considered the most recent recall period as the last month. The Quantity-Frequency (QF) method was used for annual APC calculation, although it entails more recall bias than the “last week” method60. The survey results showed that Iran’s APC (0.120L) is lower than the global (6.4L) and regional (0.6L) averages6. It’s important to note that while these international figures typically pertain to individuals over 15 years old, our study focused on those over 18, which might contribute to some of the observed differences. Compared to the QF calculation by Amin-Esmaeili et al. in 2011, the APC reported in this study showed a 50% increase9.
The results from the multiple logistic regression model in our study indicated a significant positive correlation between alcohol consumption and various non-communicable diseases and metabolic syndromes, including hypertension, hypercholesterolemia, heart attacks, obesity, and physical injuries. Interestingly, the data suggested a decrease in the risk of diabetes mellitus and stroke associated with alcohol consumption. Particularly noteworthy is the elevated and significant risk linked with heart attacks, obesity, and physical injuries. Various studies have explored the relationship between alcohol consumption and non-communicable diseases. Identified patterns include the J-shaped curve, illustrating a dose–response relationship between alcohol intake and the odds of metabolic syndrome61, and the U-shaped pattern, where heavy drinkers face a significantly higher risk, unlike low and moderate consumers62. While some studies suggest a linear relationship between alcohol consumption and metabolic syndrome63,64, others find no significant correlation65,66. The growing body of research underscoring the link between lifetime alcohol consumption and its detrimental effects, especially the risk of metabolic syndrome, highlights the urgent need for preventive measures against alcohol consumption3,67,68.
Despite the challenges posed by the COVID-19 pandemic, this study's data collection was conducted face-to-face, adhering to health guidelines and social distancing. This national study encompasses a large sample size from across the country. A key feature of this study is its alignment with the WHO’s STEPS methodology, enabling comparisons with global studies. In response to the stigma surrounding alcohol consumption in Iran, interviewers were specifically trained to gather data discreetly and privately. Another strength of this study lies in its assessment of comorbidities associated with alcohol consumption. Conditions like hypercholesterolemia and diabetes were evaluated using both laboratory data and medical history, and participants' blood pressure was measured during their assessment.
This study is subject to some limitations. Firstly, its cross-sectional design poses challenges in identifying potential reverse associations between alcohol consumption and assessed outcomes, as well as in establishing causality. As a household survey, it does not include individuals living in residential facilities, institutions with restricted access, or those who are homeless, where alcohol consumption prevalence might differ. Additionally, the reliance on self-reporting could lead to underreporting, particularly since alcohol consumption is illegal and socially stigmatized in Iran. This study focuses on individuals over 18 years old, which limits the comparability of the Alcohol Per Capita Consumption (APC) results with other national and international studies that often include those aged 15 and older. Furthermore, restricted access to recent alcohol consumption data (last week) made it impossible to employ the “last week” method alongside the Quantity-Frequency (QF) method. Consequently, calculating APC using a combination method was not feasible9. A key limitation of our study is the low prevalence of alcohol consumption in the Iranian population, potentially due to under-reporting or genuinely lower consumption levels. This led to smaller sample sizes for recent consumption periods (past 12 months and 30 days), limiting the power and reliability of our statistical analyses. The impact of COVID-19 on changes in alcohol consumption levels could be significant during the pandemic based on the literature, but measuring this impact was beyond the scope of our study, and it was another limitation of the current research.
Conclusion
In this population-based study, we estimated the prevalence of alcohol consumption over multiple timespans, finding the highest rates among males and younger age groups. This underscores the need for targeted prevention strategies within these demographics in public health policies. The potential hazardous effects of even lifetime alcohol consumption call for appropriate preventive measures to address this public health concern. Moreover, focusing on harm reduction interventions among those with lower socioeconomic status is crucial to mitigate the adverse impacts of harmful alcohol use. Our findings also highlight a positive correlation between alcohol consumption and metabolic syndrome. To reduce the possible negative effects of alcohol on individuals' metabolic profiles, implementing preventive strategies against alcohol consumption, particularly its harmful patterns, is a critical priority.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
World Health Organization (WHO) Alcohol, <https://www.who.int/news-room/fact-sheets/detail/alcohol> (2018).
Murray, C. J. L. et al. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. The Lancet 396, 1223–1249. https://doi.org/10.1016/S0140-6736(20)30752-2 (2020).
GBD. Alcohol Collaborators. 2022. Population-level risks of alcohol consumption by amount, geography, age, sex, and year: a systematic analysis for the Global Burden of Disease Study 2020. Lancet (London, England) 400, 185–235. https://doi.org/10.1016/s0140-6736(22)00847-9 (2020).
Park, S. H. & Kim, D. J. Global and regional impacts of alcohol use on public health: Emphasis on alcohol policies. Clin. Mol. hepatol. 26, 652–661. https://doi.org/10.3350/cmh.2020.0160 (2020).
World Health Organization (WHO) Alcohol, total per capita (15+) consumption, <https://www.who.int/data/gho/indicator-metadata-registry/imr-details/4759#:~:text=Definition%3A,alcohol%2C%20adjusted%20for%20tourist%20consumption.> (2018).
World Health Organization (WHO) Global status report on alcohol and health 2018, <https://www.who.int/publications/i/item/9789241565639> (2018).
World Bank. Total alcohol consumption per capita (liters of pure alcohol, projected estimates, 15+ years of age), <https://data.worldbank.org/indicator/SH.ALC.PCAP.LI?end=2018&start=2000&view=chart> (2018).
Rehm, J. et al. The relationship between different dimensions of alcohol use and the burden of disease-an update. Addiction (Abingdon, England) 112, 968–1001. https://doi.org/10.1111/add.13757 (2017).
Amin-Esmaeili, M. et al. Methods for calculation of per capita alcohol consumption in a Muslim majority country with a very low drinking level: Findings from the 2011 Iranian mental health survey. Drug Alcohol Rev. 37, 874–878. https://doi.org/10.1111/dar.12847 (2018).
Al-Ansari, B., Thow, A.-M., Day, C. A. & Conigrave, K. M. Extent of alcohol prohibition in civil policy in Muslim majority countries: The impact of globalization. Addiction 111, 1703–1713. https://doi.org/10.1111/add.13159 (2016).
Chegeni, M. et al. Alcohol consumption in Iran: A systematic review and meta-analysis of the literature. Drug Alcohol Rev. 39, 525–538. https://doi.org/10.1111/dar.13093 (2020).
Nikfarjam, A. et al. The frequency of alcohol use in Iranian urban population: The results of a national network scale up survey. Int. J. health policy Manag. 6, 97–102. https://doi.org/10.15171/ijhpm.2016.103 (2017).
Lankarani, K. B. & Afshari, R. Alcohol consumption in Iran. The Lancet 384, 1927–1928. https://doi.org/10.1016/S0140-6736(14)62279-0 (2014).
GBD. Iran Collaborators. 2022. Health system performance in Iran: a systematic analysis for the Global Burden of Disease Study 2019. Lancet (London, England) 399, 1625–1645. https://doi.org/10.1016/s0140-6736(21)02751-3 (2019).
Mehrabi, M. et al. Prevalence and correlates of lifetime alcohol use among adult urban populations in Iran: A knowledge, attitude, and practice study. J Psychoact. Drugs 51, 290–297. https://doi.org/10.1080/02791072.2019.1578909 (2019).
Moradinazar, M. et al. Prevalence of drug use, alcohol consumption, cigarette smoking and measure of socioeconomic-related inequalities of drug use among Iranian people: Findings from a national survey. Subst. Abuse Treat. Prev. Policy 15, 39. https://doi.org/10.1186/s13011-020-00279-1 (2020).
Amin-Esmaeili, M. et al. Alcohol use disorders in Iran: Prevalence, symptoms, correlates, and comorbidity. Drug Alcohol Depend. 176, 48–54. https://doi.org/10.1016/j.drugalcdep.2017.02.018 (2017).
Hosseinkhani, Z. et al. Prevalence of alcohol consumption in most at-risk groups in Iran: A systematic review and meta-analysis. J. Subst. Use https://doi.org/10.1080/14659891.2021.2018728 (2021).
Rezaei, N. et al. Alcohol consumption and related disorders in Iran: Results from the National Surveillance of Non-Communicable Diseases’ Survey (STEPs) 2016. PLOS Global Public Health 2, e0000107. https://doi.org/10.1371/journal.pgph.0000107 (2022).
Eskandarieh, S., Hajebi, A., Noroozi, A., Haghdoost, A. A. & Baneshi, M. R. Epidemiology of alcohol abuse in Iran. Asia Pac. J. Med. Toxicol. 3, 22–22. https://doi.org/10.22038/apjmt.2014.2905 (2014).
World Health Organization. WHO STEPS surveillance manual : the WHO STEPwise approach to chronic disease risk factor surveillance / Noncommunicable Diseases and Mental Health, World Health Organization, <https://apps.who.int/iris/handle/10665/43376> (2005).
Djalalinia, S. et al. Protocol design for large-scale cross-sectional studies of surveillance of risk factors of non-communicable diseases in Iran: STEPs 2016. Arch Iran Med. 20, 608–616 (2017).
Djalalinia, S. et al. Protocol design for surveillance of risk factors of non–communicable diseases during the COVID-19 pandemic: An experience from Iran STEPS survey 2021. Arch. Iran Med. 25, 634–646. https://doi.org/10.34172/aim.2022.99 (2022).
Charles, J., Valenti, L. & Miller, G. Binge drinking. Aust. Fam. Physician 40, 569 (2011).
World Health Organization (WHO) Alcohol, recorded per capita (15+ years) consumption (in litres of pure alcohol), <https://www.who.int/data/gho/indicator-metadata-registry/imr-details/462> (2022).
Kehoe, T., Gmel, G., Shield, K. D., Gmel, G. & Rehm, J. Determining the best population-level alcohol consumption model and its impact on estimates of alcohol-attributable harms. Popul. Health Metrics 10, 6. https://doi.org/10.1186/1478-7954-10-6 (2012).
Stockwell, T. et al. Estimating under- and over-reporting of drinking in national surveys of alcohol consumption: Identification of consistent biases across four English-speaking countries. Addiction 111, 1203–1213. https://doi.org/10.1111/add.13373 (2016).
Stockwell, T., Zhao, J. & Macdonald, S. Who under-reports their alcohol consumption in telephone surveys and by how much? An application of the ‘yesterday method’ in a national Canadian substance use survey. Addiction 109, 1657–1666. https://doi.org/10.1111/add.12609 (2014).
Allen, J. P. et al. Assessing Alcohol Problems: A Guide for Clinicians and Researchers (U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute on Alcohol Abuse and Alcoholism, 2003).
Weir, C. B. & Jan, A. BMI classification percentile and cut off points. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK541070/ (StatPearls Publishing, Treasure Island (FL), 2024).
AlMarri, T. S. K. & Oei, T. P. S. Alcohol and substance use in the Arabian Gulf region: A review. Int. J. Psychol. 44, 222–233. https://doi.org/10.1080/00207590801888752 (2009).
Kanny, et al. Vital signs: Binge drinking prevalence, frequency, and intensity among adults - United States, 2010. MMWR Morb. Mortal Wkly. Rep. 61, 14–19 (2012).
Castro, D. S. et al. Sociodemographic characteristics associated with binge drinking among Brazilians. Drug Alcohol Depend. 126, 272–276. https://doi.org/10.1016/j.drugalcdep.2012.05.017 (2012).
Lim, W.-Y. et al. Trends in alcohol consumption in Singapore 1992–2004. Alcohol Alcohol. 42, 354–361. https://doi.org/10.1093/alcalc/agm017 (2007).
Nikfarjam, A. et al. National population size estimation of illicit drug users through the network scale-up method in 2013 in Iran. Int. J. Drug Policy 31, 147–152. https://doi.org/10.1016/j.drugpo.2016.01.013 (2016).
Kerr, W. C. et al. Early life health, trauma and social determinants of lifetime abstention from alcohol. Alcohol Alcohol. (Oxford, Oxfordshire) 51, 576–583. https://doi.org/10.1093/alcalc/agw041 (2016).
Ulaş, H., Binbay, T., Kırlı, U., Elbi, H. & Alptekin, K. The epidemiology of alcohol use in Izmir, Turkey: Drinking pattern, impairment and help-seeking. Soc. Psychiatry Psychiatr. Epidemiol. 52, 887–899. https://doi.org/10.1007/s00127-017-1345-5 (2017).
Mohamed, S. & Ajmal, M. Multivariate analysis of binge drinking in young adult population: Data analysis of the 2007 survey of lifestyle, attitude and nutrition in Ireland. Psychiatry Clin. Neurosci. 69, 483–488. https://doi.org/10.1111/pcn.12284 (2015).
Substance Abuse and Mental Health Services Administration(SAMHSA) National Survey on Drug Use and Health (NSDUH). Table 2.46B—Alcohol use, binge alcohol use, and heavy alcohol use in the past month among persons aged 18 or older, by demographic characteristics: Percentages, 2013 and 2014, <https://www.samhsa.gov/data/sites/default/files/cbhsq-reports/NSDUHDetailedTabs2017/NSDUHDetailedTabs2017.pdf> (2014).
Padrão, P. et al. Alcohol consumption in Mozambique: Regular consumption, weekly pattern and binge drinking. Drug Alcohol Dependence 115, 87–93. https://doi.org/10.1016/j.drugalcdep.2010.10.010 (2011).
Soler-Vila, H. et al. Binge drinking in Spain, 2008–2010. Alcohol. Clin. Exp. Res. 38, 810–819. https://doi.org/10.1111/acer.12275 (2014).
Schulenberg, J. E. & Maggs, J. L. A developmental perspective on alcohol use and heavy drinking during adolescence and the transition to young adulthood. J. Stud. Alcohol, Suppl. https://doi.org/10.15288/jsas.2002.s14.54 (2002).
Centers for Disease Control and Prevention(CDC) Alcohol Related Disease Impact (ARDI), <www.cdc.gov/ARDI> (
McKee, S. A. & Weinberger, A. H. How can we use our knowledge of alcohol-tobacco interactions to reduce alcohol use?. Ann. Rev. Clin. Psychol. 9, 649–674. https://doi.org/10.1146/annurev-clinpsy-050212-185549 (2013).
HamidianRad, M. & Zeinali, A. The prevalence of drug and alcohol use among students of Urmia universities. Etiadpajohi. 12, 175–192 (2019).
Abbasi-Ghahramanloo, A., Fotouhi, A., Zeraati, H. & Rahimi-Movaghar, A. Prescription drugs, alcohol, and illicit substance use and their correlations among medical sciences students in iran. Int. J. High Risk Behav. Addictn. 4, e21945–e21945. https://doi.org/10.5812/ijhrba.21945 (2015).
Mohammadkhani, S. H. Prevalence of cigarette smoking, alcohol drinking and illegal drugs use among Iranian adolescents. J. Kerman Univ. Med. Sci. 19, 32–48 (2012).
Chu, J. J., Jahn, H. J., Khan, M. H. & Kraemer, A. Alcohol consumption among university students: A Sino-German comparison demonstrates a much lower consumption of alcohol in Chinese students. J. Health, Popul. Nutr. 35, 25. https://doi.org/10.1186/s41043-016-0062-0 (2016).
Davoren, M. P., Shiely, F., Byrne, M. & Perry, I. J. Hazardous alcohol consumption among university students in Ireland: A cross-sectional study. BMJ Open 5, e006045. https://doi.org/10.1136/bmjopen-2014-006045 (2015).
Mekonen, T., Fekadu, W., Chane, T. & Bitew, S. Problematic alcohol use among university students. Front. Psychiatr. https://doi.org/10.3389/fpsyt.2017.00086 (2017).
Im, P. K. et al. Patterns and trends of alcohol consumption in rural and urban areas of China: Findings from the China Kadoorie Biobank. BMC Public Health 19, 217. https://doi.org/10.1186/s12889-019-6502-1 (2019).
Donath, C. et al. Alcohol consumption and binge drinking in adolescents: Comparison of different migration backgrounds and rural vs. urban residence—a representative study. BMC Public Health 11, 84. https://doi.org/10.1186/1471-2458-11-84 (2011).
Fontes Marx, M., London, L., Harker, N. & Ataguba, J. E. Assessing Intertemporal Socioeconomic Inequalities in Alcohol Consumption in South Africa. Front. Public Health https://doi.org/10.3389/fpubh.2021.606050 (2021).
Katikireddi, S. V., Whitley, E., Lewsey, J., Gray, L. & Leyland, A. H. Socioeconomic status as an effect modifier of alcohol consumption and harm: analysis of linked cohort data. Lancet Public health 2, e267–e276. https://doi.org/10.1016/S2468-2667(17)30078-6 (2017).
Probst, C., Kilian, C., Sanchez, S., Lange, S. & Rehm, J. The role of alcohol use and drinking patterns in socioeconomic inequalities in mortality: A systematic review. Lancet Public Health 5, e324–e332. https://doi.org/10.1016/S2468-2667(20)30052-9 (2020).
Grittner, U., Kuntsche, S., Gmel, G. & Bloomfield, K. Alcohol consumption and social inequality at the individual and country levels—results from an international study. Eur. J. Publ. Health 23, 332–339. https://doi.org/10.1093/eurpub/cks044 (2013).
Bloomfield, K., Grittner, U., Kramer, S. & Gmel, G. Social inequalities in alcohol consumption and alcohol-related problems in the study countries of the EU concerted action ‘gender, culture and alcohol problems: A multi-national study’. Alcohol Alcohol 41, i26-36. https://doi.org/10.1093/alcalc/agl073 (2006).
Jones, L., Bates, G., McCoy, E. & Bellis, M. A. Relationship between alcohol-attributable disease and socioeconomic status, and the role of alcohol consumption in this relationship: A systematic review and meta-analysis. BMC Public Health 15, 400–400. https://doi.org/10.1186/s12889-015-1720-7 (2015).
Stockwell, T., Zhao, J., Chikritzhs, T. & Greenfield, T. K. What did you drink yesterday? Public health relevance of a recent recall method used in the 2004 Australian national drug strategy household survey. Addiction (Abingdon, England) 103, 919–928. https://doi.org/10.1111/j.1360-0443.2008.02219.x (2008).
Stockwell, T. et al. Under-reporting of alcohol consumption in household surveys: A comparison of quantity–frequency, graduated–frequency and recent recall. Addiction 99, 1024–1033. https://doi.org/10.1111/j.1360-0443.2004.00815.x (2004).
Yoon, Y. S., Oh, S. W., Baik, H. W., Park, H. S. & Kim, W. Y. Alcohol consumption and the metabolic syndrome in Korean adults: The 1998 Korean National Health and Nutrition Examination Survey. Am. J. Clin. Nutr. 80, 217–224. https://doi.org/10.1093/ajcn/80.1.217 (2004).
Wakabayashi, I. Association between alcohol drinking and metabolic syndrome in Japanese male workers with diabetes mellitus. J. Atheroscle. Thromb. 18, 684–692. https://doi.org/10.5551/jat.7435 (2011).
Fan, A. Z. et al. Patterns of alcohol consumption and the metabolic syndrome. J.Clin. Endocrinol. Metab. 93, 3833–3838. https://doi.org/10.1210/jc.2007-2788 (2008).
Gigleux, I. et al. Moderate alcohol consumption is more cardioprotective in men with the metabolic syndrome. J. Nutr. 136, 3027–3032. https://doi.org/10.1093/jn/136.12.3027 (2006).
Buja, A. et al. Alcohol consumption and metabolic syndrome in the elderly: Results from the Italian longitudinal study on aging. Eur. J. Clin. Nutr. 64, 297–307. https://doi.org/10.1038/ejcn.2009.136 (2010).
Wilsgaard, T. & Jacobsen, B. K. Lifestyle factors and incident metabolic syndrome: The Tromsø Study 1979–2001. Diabet. Res Clin. Pract. 78, 217–224. https://doi.org/10.1016/j.diabres.2007.03.006 (2007).
Park, S. H. Association between alcohol consumption and metabolic syndrome among Korean adults: Nondrinker versus lifetime abstainer as a reference group. Subst. Use Misuse 47, 442–449. https://doi.org/10.3109/10826084.2011.648043 (2012).
Fan, A. Z. et al. Lifetime alcohol drinking pattern is related to the prevalence of metabolic syndrome. The Western New York Health Study (WNYHS). Eur. J. Epidemiol. 21, 129–138. https://doi.org/10.1007/s10654-005-5457-y (2006).
Acknowledgements
The authors extend their heartfelt gratitude to the Deputy of Health and the Deputy of Research and Technology at the Ministry of Health and Medical Education, the National Institute for Health Research, the World Health Organization, and numerous scholars and experts in related fields. Also, this study was supported by I.R. Iran’s National Institute of Health Research, Tehran University of Medical Sciences, Iran. (Contract No:241/9839) We sincerely thank all participants and the scientific and executive partners from the medical universities who contributed to this project. Your collaboration and support have been invaluable to the success of this study.
Author information
Authors and Affiliations
Contributions
Conceptualization: F.F., N.R., A.H.; Data Curation: M.N., E.G., M.Y., N.A.; Formal Analysis: M.N., E.G., M.Y., N.A.; Investigation: F.F. and all of co-authors; Methodology: F.F., A.H., E.G., N.R.; Project Administration: A.H., R.H., S.A., MM.R., E.F., Y.F., S.R., M.A., N.F.; Supervision: R.H., Y.F., S.D., A.K., E.F., A.M.; Validation: F.F., A.H., S.A., N.R.; Writing—Original Draft Preparation: A.H.; Writing—Review and Editing: S.A., MM.R., K.R., A.M., H.J., A.H.; Visualization: M.N., N.A.; All authors reviewed the manuscript, critically commented on the draft and provided their approval for the submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hajebi, A., Nasserinejad, M., Rezaei, N. et al. Alcohol consumption among Iranian population based on the findings of STEPS survey 2021. Sci Rep 14, 16819 (2024). https://doi.org/10.1038/s41598-024-66257-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-66257-w
- Springer Nature Limited