
Abstract
The combination of anti-angiogenic treatment and immunotherapy presents a promising strategy against colon cancer. Interleukin-17F (IL-17F) emerges as a critical immune cell cytokine expressed in colonic epithelial cells, demonstrating potential in inhibiting angiogenesis. In order to clarify the roles of IL-17F in the colon cancer microenvironment and elucidate its mechanism, we established a mouse colon carcinoma cell line CT26 overexpressing IL-17F and transplanted it subcutaneously into syngeneic BALB/c mice. We also analyzed induced colon tumor in IL-17F knockout and wild type mice. Our results demonstrated that IL-17F could suppress colon tumor growth in vivo with inhibited angiogenesis and enhanced recruitment of cysteine-cysteine motif chemokine receptor 6 (CCR6) positive immune cells. Additionally, IL-17F suppressed the tube formation, cell growth and migration of endothelial cells EOMA in vitro. Comprehensive bioinformatics analysis of transcriptome profiles between EOMA cells and those treated with three different concentrations of IL-17F identified 109 differentially expressed genes. Notably, a potential new target, Caspase 4, showed increased expressions after IL-17F treatment in endothelial cells. Further molecular validation revealed a novel downstream signaling for IL-17F: IL-17F enhanced Caspase 4/GSDMD signaling of endothelial cells, CT26 cells and CT26 transplanted tumors, while IL-17F knockout colon tumors exhibited decreased Caspase 4/GSDMD signaling. The heightened expression of the GSDMD N-terminus, coupled with increased cellular propidium iodide (PI) uptake and lactate dehydrogenase (LDH) release, revealed that IL-17F promoted pyroptosis of endothelial cells. Altogether, IL-17F could modulate the colon tumor microenvironment with inhibited angiogenesis, underscoring its potential as a therapeutic target for colon cancer.
Similar content being viewed by others


Introduction
Colorectal cancer presents a growing global incidence and mortality burden1, ranking among the foremost fatal cancers2. The challenges of metastatic diseases and drug resistance further highlight the necessity to develop new treatment strategies for colorectal cancer3. Angiogenesis is critical for oxygen and nutrients supplies in cancer proliferation and metastasis. Anti-angiogenic therapy has been clinically applied in the therapeutic management of metastatic colorectal cancer4. However, several issues such as insufficient therapeutic efficacy, reproducibility, and acquired drug resistance have been found in anti-angiogenic therapy which impel further research on tumor angiogenesis5. Additionally, immune cells play pivotal roles in colorectal cancer development6. For example, inflammation can initiate and promote tumorigenesis, and immune suppression induced by diary or gut microbiota can promote colorectal cancer7,8. Immunotherapy could bolster the immune system’s ability to recognize and eradiate cancer cells9. However, while some colorectal cancers are sensitive to certain immunotherapy and show impressive treatment outcomes, others are initially refractory or develop resistance10. Immune cell infiltration into tumors depends on the tumor vasculature, and immune cell types in the tumor microenvironment are also affected by several angiogenic factors11. Conversely, tumor angiogenesis could be promoted or inhibited by innate and adaptive immune cells12. Therefore, the interplay between tumor vasculature and immunity underscores the potential of combined anti-angiogenic treatment and immunotherapy to enhance therapeutic efficacy while mitigating side effects13,14.
The interleukin-17 (IL-17) family, crucial in inflammatory response, has garnered significant attention in cancer research15. Among the six family members (IL-17A to IL-17F), IL-17A exhibits both pro- and anti-tumor effects in colorectal cancer progression16. IL-17F shares the greatest homology and overlapping functions with IL-17A, but manifests distinct effects in colorectal cancer. IL-17F polymorphisms were observed to be mainly protective in colorectal cancer17,18,19. Our previous study revealed IL-17F was expressed in normal colonic epithelial cells and the expression was decreased in colon cancer20. Although the decreased expression of IL-17F in colorectal cancer compared with healthy control was further confirmed21,22, the mechanism for IL-17F exerting its anti-tumor effects remains elusive.
In this study, IL-17F was overexpressed in mouse colon carcinoma cell line CT26, which was further transplanted subcutaneously into BALB/c mice. Compared with IL-17F overexpressing human colorectal cancer cell line HCT116 transplanted into nude mice in our pervious study20, this syngeneic tumor model could provide opportunities to examine the complex interactions between cancer cells and immune cells in the tumor microenvironment23. Moreover, since IL-17F may inhibit colon cancer angiogenesis in our pervious study20, the effects of IL-17F on tumor immune microenvironment, endothelial cells, and the downstream molecular signaling were further studied.
Materials and methods
Cell culture
The mouse colon carcinoma cell line CT26 and mouse endothelial cell line EOMA were obtained from the American Type Culture Collection and cultured in DMEM (GIBCO) supplemented with 10% FCS. Mouse IL-17F cDNA with HA tag was from Sino Biological Inc. (Beijing, China). CT26 cells were electroporated with BglII linearized IL-17F cDNA construct or blank vector control using Bio-Rad Gene Pulser at 250 V, 960 µF. At 48 h after electroporation, transfectants were selected in culture medium supplemented with 100 µg/ml Hygromycin (Roche). Hygromycin resistant monoclones were picked and expanded in the selection medium.
Animal studies
To establish mouse colon cancer model, CT26 cells (1.0 × 106) were subcutaneously implanted into the lower back of 6–8 weeks old BALB/c mice. Tumor growth was monitored with vernier caliper and calculated by the formula tumor size = ab2/2. The a is the larger and b is the smaller of the two dimensions. At 3 weeks after transplantation, tumors were separated into two equal parts: one part was used for fluorescence activated cell sorting (FACS) analysis, the other was fixed in 4% paraformaldehyde or snap-frozen in liquid nitrogen. All mice were housed in pathogen-free facilities on a 12 h light–dark cycle. All protocols and procedures in this study were approved by the Ethics Committee of Wuhan University (Permit No.: WQ20210028).
Colon samples from AOM-DSS treated Il-17f−/− and wild type mice were collected from previous study20.
FACS analysis of tissue cells
Fresh tumor biopsies were scissored into small pieces, and separated into single cells using collagenase IV and cell dissociation solution (Sigma). Single cells were collected and stained. Different fluorescence conjugated anti-mouse CD11b, Gr-1, CD34, CD31, CD3, CD4, CD8, Foxp3, NK1.1, CCR6 were from ebioscience. The stained cells were analyzed using Flow Cell sorter (Beckman Cytoflex S).
Immunohistochemistry
Tumor biopsies were fixed in 4% paraformaldehyde. Paraffin sections were incubated with primary antibodies: anti-mouse CD31 (Abcam), CCR6 (Servicebio), IFNγ (Servicebio), IL-1β (Servicebio), at 4 °C overnight. The sections were then processed with horseradish peroxidase (HRP) conjugated secondary antibodies and Diaminobenzidine (DAB) color development kit (Servicebio). Nuclei were detected by hematoxylin counter-staining. Images were captured using microscopy (Nikon Eclipse C1, Japan).
Tube formation assay
EOMA were treated with conditional mediums from the different CT26 cell clones or different concentrations of IL-17F (PeproTech, USA) for 24 h before tube formation assay. During IL-17F blocking assay, 5 µg/ml neutralizing antibody (eBioscience, Clone RN17) was added into the conditional mediums. The 24-well plates were coated with 300 µl Matrigel (BD354230, USA) and incubated at 37 °C for 30 min for polymerization of the gels. EOMA cells (1.0 × 105) were seeded into each well and incubated in the CO2 incubator at 37 °C for 6 h. Images from five randomly chosen fields in each well were captured using an inverted microscope (Nikon, Japan) in each group. The number of branch points and tube length were measured using Image-Pro Plus software (Media Cybernetics, L.P., Silver Spring, MD, USA). Each experiment was repeated at least three times using different batches of cells.
Real-Time cell growth and migration detection
Cell growth and migration were monitored by Real-Time Cell Analyzer (RTCA, xCELLigence, Roche) 24. EOMA cells were seeded in the E-plates 96 (5000 cells per chamber) and cells were treated with different concentrations (0, 25, 50, 100, 200 ng/ml) of IL-17F. The cell growth was measured as cell index values by detecting electro-resistances every 30 min. EOMA cells were seeded in the upper chambers of CIM-Plates 16 (25,000 cells per chamber) and different concentrations (0, 25, 50, 100, 200 ng/ml) of IL-17F were added into the lower chambers. The cells migrated to the lower chambers and attached to the bottom were detected by electro-resistances every 30 min. When the upper chambers were pretreated with 1:20 diluted Matrigel (BD354230, USA), the EOMA cell number in the upper chambers of CIM-Plates 16 was increased to 40,000 cells per chamber. IL-17F-transfected Clone 1, 2 &3 CT26 cells and vector control transfected CT26 cells were seeded in the E-plates 96 (3000 cells per chamber) and the cell index was detected every 30 min. Data analysis was performed using Real-Time Cell Analyzer software supplied with the instrument.
PI uptake detection
After treatment with different concentrations (0, 25, 50, 100, 200 ng/ml) of IL-17F for 24 h, EOMA cells in 96 well plate were treated with 1 mg/ml PI (Solarbio). Immediately after PI added, the fluorescence, brightfield and digital phase contrast images were captured by the High Content Live Cell Imaging System (Operetta CLS, PERKINELMER, USA). The mean fluorescence intensities and cell numbers were quantified using the software supplied with the instrument.
ELISA and biochemical kit measurement
Cells with the same initial numbers were cultured in the same volume of medium and the supernatant were collected when cells reached 90% confluence. The concentrations of IL-17F in the CT26 cell supernatants were determined using Elisa kits as recommended by the assay manufacturer (biolegend, USA). LDH release by EOMA cells was qualified using LDH Cytotoxicity Assay Kit as recommended by the assay manufacturer (Beyotime, China).
Reverse transcription-quantitative polymerase chain reaction (RT-qPCR)
Cellular RNA was extracted using Trizol method and reverse transcript to cDNA using RT Kit (Toyobo, Osaka, Japan). Quantitative PCR was performed on Bio-Rad CFX96 System using the SYBR Green PCR Master Mix (Takara). The relative RNA levels of each gene were normalized to 18S rRNA. Primers used: 18S rRNA: 5′-GGA CAG GAT TGA CAG ATT GAT AGC-3′ and 5′-TGC CAG AGT CTC GTT CGT TAT C-3′. Il-17f.: 5′-GGG ATT ACA ACA TCA CTC-3′ and 5′-AAC CTG AAG GAA TTA GAA C-3′. Vegf: 5′-CTG CTG TAA CGA TGA AGC CCT G-3′ and 5′-GCT GTA GGA AGC TCA TCT CTC C-3′. Tnfα: 5′-CCT CAC ACT CAG ATC ATC-3′ and 5′-AAC CTG GGA GTA GAC AAG-3′. Ccl20: 5′-TGG GTT TCA CAA GAC AGA TGG C-3′ and 5′-ACT CTT AGG CTG AGG AGG TTC AC-3′. Cd31: 5′-CCA AAG CCA GTA GCA TCA TGG TC-3′ and 5′-GGA TGG TGA AGT TGG CTA CAG G-3′. Ccr6: 5′-CCC GTG TTG TAT GCG TTT ATT GG-3′ and 5′-ACT GGT CTG CCT GGA GAT GTA G-3′. Ifnγ: 5′-CAG CAA CAG CAA GGC GAA AAA GG-3′ and 5′-TTT CCG CTT CCT GAG GCT GGA T-3′. Il-1β: 5′-CTT TGA AGA AGA GCC CAT CC-3′ and 5′-CAC TTG TTG GTT GAT ATT CTG TC-3’. Caspase 4: 5′-GTG GTG AAA GAG GAG CTT ACA GC-3′ and 5’-GCA CCA GGA ATG TGC TGT CTG A-3′. Caspase 3: 5’-CTT CTT CAG AGG CGA CTA C-3′ and 5′-CCA GGA ATA GTA ACC AGG TG-3′. Caspase 1: 5′-GGC ACA TTT CCA GGA CTG ACT G-3′ and 5′-GCA AGA CGT GTA CGA GTG GTT G-3′. The primers were synthesized by Wuhan Tianyi Huayu Gene Technology Co., Ltd (Wuhan, China).
Western blotting
Cellular protein was extracted using RIPA lysis buffer (Boster, China) containing protease and phosphatase inhibitors. The protein concentrations were determined using BCA assay (Beyotime, China). Cellular protein was separated by 10% SDS-PAGE gel, and transferred onto PVDF membrane. The membranes were further blocked and incubated with primary antibodies: anti-IL-17F (R&D), CASP4 (Abmart), CASP1 (Abmart), CASP3 (Abmart), Cleaved-CASP4 (Abmart), N-GSDMD (abcam), β-tublin (Abmart) at 4 °C overnight. Washed membranes were further incubated with HRP-conjugated secondary antibody for 2 h at room temperature. All antibodies were diluted in TTBS buffer with 5% non-fat milk. The blots were obtained by an electrochemiluminescence (ECL) detection system (Bio-Rad Laboratory, Hercules, CA, USA). Signal intensities in the blots were measured by Quantity One software and transformed to the bar graphs.
Bioinformatic data analysis
EOMA cells treated with different concentrations (0, 50, 100, 150 ng/ml) of IL-17F for 24 h were collected in Trizol and sent to Novogene (Beijing, China) for Transcriptome sequencing and analysis. Briefly, RNA was purified and qualified by Agilent 2100 bioanalyzer (Agilent Technologies, CA, USA). cDNA library was prepared and purified with AMPure XP system (Beckman Coulter, Beverly, USA). After cluster generation, the library was sequenced on an Illumina Novaseq platform. After quality control, paired-end clean reads were aligned to the reference genome using Hisat2 v2.0.5. The reads numbers mapped to each gene were counted by FeatureCounts v1.5.0-p3. Gene expression levels were estimated by calculating the FPKM (Fragments Per Kilobase of transcript sequence per Millions base pairs sequenced) of each gene based on the length of the gene and reads count mapped to this gene. Differential expression analysis was performed using the DESeq2 R package (1.20.0). Gene Ontology (GO) enrichment analysis of differentially expressed genes was implemented by the cluster Profiler R package, in which gene length bias was corrected.
Statistical analysis
Values were expressed as mean ± standard deviation. Differences were analyzed using student’s t-test or One-way analysis of variance (ANOVA) by GraphPad software, and P < 0.05 was considered statistically significant.
Results
Overexpression of IL-17F suppressed colon tumorigenesis in vivo
To assess the impact of IL-17F on colon cancer microenvironment, the first step was that mouse colon cancer cell line CT26 cells were stably transfected with mouse IL-17F cDNA or empty vector as control. RT-qPCR analysis demonstrated a substantial increase of the Il-17f mRNA levels in IL-17F-transfected Clone 1, 2 &3 CT26 cells compared with CT26 (blank control) and vector control transfected CT26 cells (vector control) (Fig. 1A). ELISA analysis further confirmed elevated levels of IL-17F in the cultural supernatants of IL-17F-transfected Clone 1, 2 &3 CT26 cells (11.82 ± 1.51 pg/ml in Clone 1, 4.35 ± 0.72 pg/ml in Clone 2, 8.13 ± 1.30 pg/ml in Clone 3), while the levels of IL-17F were undetectable in the cultural supernatants of blank control and vector control (Fig. 1B). Western blot analysis of the cellular proteins corroborated abundant IL-17F expression in the IL-17F-transfected Clone 1, 2 &3 CT26 cells (Fig. 1C). Altogether, IL-17F overexpressing CT26 cell clones were well established. Subsequent assessment of the mRNA levels of cancer related genes Vegf and Tnfα revealed no significant difference among the IL-17F overexpressing Clone 1, 2 &3 CT26 cells, blank control and vector control (Fig. 1D,E). Since IL-17F is reported to induce CCL20 (Cysteine-cysteine motif chemokine ligand 20) mediated inflammation25, the mRNA levels of Ccl20 were checked and significant elevated mRNA levels of Ccl20 were found in the IL-17F overexpressing Clone 1, 2 &3 CT26 cells (Fig. 1F).

Overexpression of IL-17F inhibited colon tumorigenesis in vivo. (A) RT-qPCR analysis of the IL-17F mRNA levels in CT26 (blank control), empty vector transfected CT26 (vector control), and IL-17F-transfected Clone 1, 2 and 3 CT26 cells. (B) Elisa analysis of the IL-17F levels in the cultural supernatant. (C) Western Blot analysis of the IL-17F protein levels in the cells. (D–F) RT-qPCR analysis of the mRNA expression levels in the cells. N = 3; Compared with vector control: *, P < 0.05; ***, P < 0.001. (G) The tumor size, (H) tumor weight, and (I) representive tumor images of the cells transplanted into the lower back of BALB/c mice at three weeks post transplantation. N = 8; Compared with vector control: *, P < 0.05.
To assess the impact of IL-17F on colon cancer microenvironment, the second step was that IL-17F overexpressing CT26 cells were transplanted into the lower back of BALB/c mice while vector transfected CT26 cells were transplanted as controls. Three weeks post-transplantation, tumors derived from IL-17F-transfected Clone 1 CT26 cells were scarcely observed. Tumors derived from Clone 2 cells exhibited a tumor size of 2.06 ± 0.94 mm3 and a tumor weight of 0.021 ± 0.009 g. Tumors derived from Clone 3 cells had a tumor size of 4.79 ± 1.38 mm3 and a tumor weight of 0.027 ± 0.007 g. In contrast, tumors derived from vector control cells displayed a tumor size of 12.50 ± 3.50 mm3 and a tumor weight of 0.087 ± 0.015 g (Fig. 1G–I). These data demonstrated that IL-17F could significantly suppress the growth of CT26 cells in vivo.
IL-17F modified the colon tumor microenvironment
Since CT26 tumors in syngeneic BALB/c mice harbored multiple immune cell infiltrates23, the IL-17F overexpressing CT26 cell derived tumors were disaggregated into single cells, stained and analyzed by FACS, with vector transfected CT26 cell derived tumors as control. The percentages of endothelial CD31 + cells in IL-17F overexpressing tumors (1.94 ± 0.54%) were lower than those in vector control (4.22 ± 0.48%) (Fig. 2A). The percentages of endothelial CD34 + cells in IL-17F overexpressing tumors (5.96 ± 1.32%) were also lower than those in vector control (10.39 ± 2.00%) (Fig. 2B). Tumor sections further revealed differential distribution of CD31 + endothelial cells (Fig. 2C). Some CD31 + cells could be found in the edge regions of IL-17F overexpressing tumors, while more CD31 + cells were detected in the central regions of vector control tumors (Fig. 2C). Tumor vessel density assessed by counting the number of vessels per sectional area revealed that IL-17F overexpressing tumors exhibited significantly lower vessel density compared to vector control tumors (Fig. 2D). RT-qPCR analysis of the tumors revealed significantly elevated mRNA levels of Il-17f and decreased mRNA levels of Cd31 in the IL-17F overexpressing tumors compared with those in the vector control tumors (Fig. 2E).

IL-17F altered the colon tumor microenvironment. (A, B, F) FACS analysis of the transplanted colon tumors (3 samples from clone 2, 4 samples from clone 3 and 4 samples from vector control). *, P < 0.05. (C) Representative immunohistochemical CD31 staining of the transplanted colon tumors. Bar = 50 µm. (D) Tumor vessel density analysis of the transplanted colon tumors. N = 3. (E, G) RT-qPCR analysis of the transplanted colon tumors. N = 3–5. (H) Representative immunohistochemical CD31 staining of AOM-DSS induced colon tumors from wild type and IL-17F knockout (Il-17f −/−) mice. Bar = 100 µm. (I) RT-qPCR analysis of the AOM-DSS induced colon tumors of wild type and IL-17F knockout (Il-17f−/−) mice. N = 3. *, P < 0.05. **, P < 0.01. ***, P < 0.001.
Besides the endothelial markers, various immune cell markers were checked. The percentages of NK1.1 + and CD11b + cells in IL-17F overexpressing tumors were lower than those in vector control tumors (Fig. S1A). At the same time, the percentages of CD11c+, F4/80+, Gr-1+, Gr-1 + CD11b+, CD4+, CD8+, CD4 + CD25+, Foxp3+, IL-17A + cells exhibited no significant differences between IL-17F overexpressing and vector control tumors (Fig. S1A). Since the IL-17F overexpressing CT26 cells had increased expression levels of Ccl20 (Fig. 1F) and the exclusive ligand-receptor relationship of CCR6-CCL20 was well studied in the migration of immune cells26, cysteine-cysteine motif chemokine receptor 6 (CCR6) + cells were checked. The percentages of CCR6 + cells in IL-17F overexpressing tumors (14.08 ± 1.87%) were higher than those in vector control (7.87 ± 1.42%) tumors (Fig. 2F). CCR6 was expressed on various immune cell types, including CD4 + cells, dendritic cells (DCs), and innate lymphoid cells (ILCs)27. Thus, CCR6 and CD4 double staining were performed. About half of the CD4 + cells were CCR6 + and about one fifth of the CCR6 + cells were CD4 + in both IL-17F overexpressing and vector control tumors (Fig. S1A). These data suggested that the CCR6 + cells in the tumors were mixture of innate and adaptive immune cells. Some CCR6 + cells, or IFNγ + cells, or IL-1β + cells could be detected in the IL-17F overexpressing tumors, while such cells were hard to be found in the vector control tumors (Fig. S1B). Interestingly, the CCR6 + cells observed in the IL-17F overexpressing tumors seemed to show their migration path (Fig. S1B). Additionally, RT-qPCR analysis of the tumors revealed the mRNA levels of Ccl20, Ccr6, Ifnγ and Il-1β were significantly higher in the IL-17F overexpressing tumors compared with those in the vector control tumors (Fig. 2G). Altogether, IL-17F overexpression could modify the colon tumor microenvironment by inhibiting angiogenesis and inducing CCL20 mediated recruitment of CCR6 + immune cells.
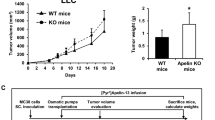
We have reported that Il-17f−/− mice exhibited significantly more tumor numbers and tumor areas in the colons compared to wild type control in the AOM-DSS induced colon cancer model20. Here, the colon tumor sections from Il-17f−/− and wild type mice were stained with CD31, and more CD31 + cells were detected in the basal layer of Il-17f−/− mice (Fig. 2H). RT-qPCR analysis of the tumors revealed the mRNA levels of Cd31 were higher in the Il-17f−/− colon tumor, while the mRNA levels of Ccl20 and Ccr6 were significantly lower in the Il-17f−/− colon tumor compared with those in the wild type colon tumors (Fig. 2I).
IL-17F inhibited the tube formation, cell growth and migration of endothelial cells in vitro
To further clarify the effects of IL-17F on endothelial cells, EOMA (mouse endothelial cell line) cells were treated with IL-17F in vitro. The tube formation of EOMA cells was significantly impaired when these cells were treated with conditional medium from IL-17F overexpressing Clone 1, 2 &3 CT26 cells (Fig. 3A,C). When the IL-17F was blocked by functional neutral antibody, the tube formation of EOMA cells was recovered (Fig. 3A,C). When EOMA cells were treated with different concentrations of IL-17F, the tube formation showed IL-17F dosage dependent inhibition (Fig. 3B,D). Moreover, Real-Time Cell Analyzer (RTCA) analysis by monitoring the electrical impedance of attached cells in the chambers revealed that IL-17F could inhibit the cell growth of EOMA cells (Fig. 3E). IL-17F could also inhibit the migration and infiltration of EOMA cells (Fig. 3F,G). Altogether, IL-17F could inhibit the tube formation, cell growth and migration of endothelial cells in vitro.

IL-17F suppressed the tube formation, cell growth and migration of endothelial cells in vitro. (A) Representative image of the tube formations of EOMA cells treated with conditional medium with and without anti-IL-17F from CT26 (blank control), empty vector transfected CT26 (vector control) and IL-17F-transfected Clone 1, 2 & 3 CT26 cells for 24 h. (B) Representative images of the tube formations of EOMA cells treated with different concentrations of IL-17F for 24 h. The number of branch points and tube length analysis of the tube formations of EOMA cells treated with conditional medium (C) and IL-17F (D). N = 3. *, P < 0.05; **, P < 0.01; ***, P < 0.001. (E) Real-Time Cell Analyzer (RTCA) analysis of the cell growth of EOMA cells treated with different concentrations of IL-17F. (F) RTCA analysis of the cell migration of EOMA cells from uncoated upper chambers to the lower chambers with different concentrations of IL-17F. (G) RTCA analysis of the cell infiltration of EOMA cells from Matrigel pre-coated upper chambers to the lower chambers with different concentrations of IL-17F. N = 3. Compared with the 0 µM control: *, P < 0.05; **, P < 0.01; ***, P < 0.001.
Bioinformatics identified specific targets of IL-17F in endothelial cells
To elucidate the molecular mechanism for the inhibition effects of IL-17F on endothelial cells, bioinformatics analysis was performed. Comparison of the gene transcriptome profiles between EOMA cells and EOMA treated with different concentrations of IL-17F (IL-17F-0 vs IL-17F-50, IL-17F-100, and IL-17F-150) revealed distinct patterns. Specifically, treatment with 50 ng/ml IL-17F resulted in 228 up-regulated differentially expressed genes (DEGs) and 250 down-regulated DEGs (Fig. 4A). Similarly, treatment with 100 ng/ml IL-17F showed 272 up-regulated DEGs and 307 down-regulated DEGs, whereas treatment with 150 ng/ml IL-17F led to 485 up-regulated DEGs and 425 down-regulated DEGs. As IL-17F concentrations increased, more DEGs were identified. These up-regulated DEGs in the three comparisons were further subjected to Venn analysis. The Venn diagram illustrated the number of common genes and unique DEGs expressed among IL-17F-0 vs IL-17F-50, IL-17F-0 vs IL-17F-100 and IL-17F-0 vs IL-17F-150 (Fig. 4B). Total 49 DEGs were found to be the common up-regulated targets of IL-17F independent of its concentration. The down-regulated DEGs in the three comparisons were also subjected to Venn analysis (Fig. 4C). Total 60 DEGs were found to be the common down-regulated targets of IL-17F independent of its concentration. Then, the 109 (49 + 60) overlapping DEGs of the three comparisons were further subjected to Gene Ontology (GO) annotation and a total of 30 functional groups were identified (Fig. 4D). The most enriched group was “positive regulation of cell migration” with 13 DEGs in the group. The second enriched groups were “cytokine mediated signaling pathway” and “receptor ligand activity” groups with 12 DEGs in the groups. Then, the transcription levels of these DEGs were shown as heatmap (Fig. 4E,F). The elevated expression of Ccl20 induced by IL-17F, as observed in CT26 cells and transplanted tumors (Fig. 1F,G), was also evident in endothelial cells. Interestingly, a probable new target of IL-17F: Caspase 4 (Casp4) showed increased expression following IL-17F treatment in the endothelial cells.

Differentially expressed genes (DEGs) were identified by bioinformatic comparisons of EOMA cells treated with different concentrations of IL-17F. (A) Presentation of DEGs in a volcano plot for the comparisons of untreated EOMA verse 50 ng/ml IL-17F treated EOMA cells (IL-17F-0 vs IL-17F-50), untreated EOMA cells verse 100 ng/ml IL-17F treated EOMA cells (IL-17F-0 vs IL-17F-100), untreated EOMA cells verse 150 ng/ml IL-17F treated EOMA cells (IL-17F-0 vs IL-17F-150). Up-regulated genes with Log2 (Fold of Change) > 1 and P < 0.05 were labelled red. Down-regulated genes with Log2 (Fold of Change) < -1 and P < 0.05 were labelled green. Venn diagrams showed the relationship of up-regulated (B) and down-regulated (C) gene numbers among the three comparisons. (D) GO annotation of the 109 overlapping genes (49 + 60) shown in the Venn diagrams. Heatmap represented the transcription levels (FPKM values) of the DEGs (E) belonging to group “positive regulation of cell migration” and DEGs (F) belonging to groups “cytokine mediated signaling pathway” and “receptor ligand activity”.
IL-17F enhanced Caspase 4/GSDMD mediated pyroptosis of endothelial cells
Validation of the increase of Ccl20 and Casp4 expression by IL-17F was performed using RT-qPCR (Fig. 5A). Since Caspase 4 was known to mediate non-canonical pyroptosis28, the expression levels of Caspase 1 (mediating canonical pyroptosis pathway) and Caspase 3 (mediating apoptosis pathway) were also checked. While IL-17F treatment led to significant upregulation of the mRNA and protein levels of Caspase 4 in EOMA cells, the levels of Caspase 1 and Caspase 3 remained unchanged (Fig. 5A,B). It’s reported that autocleavage in Caspase 4 is critical for cleaving GSDMD29, and the resulting GSDMD N-terminus could form pores on the cell membrane to execute pyroptosis30,31. Therefore, the effective cleaved-CASPASE 4 and downstream GSDMD N-terminus were further checked. EOMA cells had significantly increased protein levels of cleaved-CASPASE 4 after 50 and 100 ng/ml IL-17F treatment (Fig. 5C) and increased protein levels of N-terminal GSDMD after 50, 100 and 200 ng/ml IL-17F treatment (Fig. 5D).

IL-17F enhanced Caspase 4/GSDMD mediated pyroptosis of EOMA cells. (A) RT-qPCR analysis of EOMA cells treated with different concentrations of IL-17F. (B–D) Western blot analysis of EOMA cells treated with different concentrations of IL-17F. β-Tubulin was used as the protein loading control. (E) Real-time detection of PI uptake by IL-17F pretreated EOMA cells using Operetta CLS high content analysis system. N = 3; Compared with no IL-17F treatment (0). (F) Representative images of PI uptake by IL-17F pretreated EOMA cells. Images were acquired every 20 min. Bar = 100 µm. (G) Western blot analysis of EOMA cells treated with conditional medium with and without anti-IL-17F from CT26 (blank control), empty vector transfected CT26 (vector control) and IL-17F-transfected Clone 1, 2 & 3 CT26 cells for 24 h. N = 3; Compared with vector control. *, P < 0.05; **, P < 0.01; ***, P < 0.001.
Importantly, IL-17F induced pyroptosis of EOMA cells was evaluated. Firstly, PI uptake by IL-17F pretreated EOMA cells was monitored (Fig. 5E,F). After added into EOMA cell culture medium, PI could be taken into the dying cells and the red fluorescents of PI in the cell nuclei were increased over time. The PI uptake increased much faster in EOMA cells pretreated with 50, 100 and 200 ng/ml IL-17F than that in untreated control cells (Fig. 5E). In 200 ng/ml IL-17F pretreated group, many dead cells became unattached to the culture dish and PI became undetectable (Fig. 5F). Secondly, lactic dehydrogenase (LDH) release was measured to indicate the permeability of the cell membrane and the levels of pyroptosis. The LDH levels in the supernatants of EOMA cells dramatically increased as the IL-17F concentrations increased (Fig. S1C).
The levels of CASPASE 4, cleaved-CASPASE 4 and downstream GSDMD N-terminus in EOMA cells were also increased when these cells were treated with conditional medium from IL-17F overexpressing Clone 1, 2 &3 CT26 cells compared with those in the vector control group (Fig. 5G). Blocking IL-17F with a functional neutral antibody resulted in no significant difference in the levels of CASPASE 4, cleaved-CASPASE 4, and downstream GSDMD N-terminus in EOMA cells compared to the vector control group (Fig. 5G). These results revealed that IL-17F could enhance Caspase 4/GSDMD mediated pyroptosis in EOMA cells.
IL-17F enhanced Caspase 4/GSDMD in colon tumor cells
Since epithelial cells may also express IL-17 receptors on their cell surface, the Caspase 4/GSDMD signaling were examined in the CT26 clones. IL-17F-transfected Clone 1, 2 &3 CT26 cells exhibited significantly higher levels of CASPASE 4, cleaved-CASPASE 4 and downstream GSDMD N-terminus compared with vector control (Fig. 6A). Moreover, the cell growth of IL-17F-transfected Clone 1, 2 &3 CT26 cells were significantly slower than vector control (Fig. 6B). In the transplanted tumor model, the IL-17F overexpressing tumors exhibited higher levels of CASPASE 4, cleaved-CASPASE 4 and downstream GSDMD N-terminus compared with vector control tumors (Fig. 6C). In the AOM-DSS induced tumor model, the Il-17f−/− colon tumor had lower levels of CASPASE 4, cleaved-CASPASE 4 and downstream GSDMD N-terminus compared with wild type colon tumors (Fig. 6D). These results demonstrated that IL-17F could transmit signaling and enhance Caspase 4/GSDMD in the IL-17F expressing colon cells themselves.

IL-17F enhanced Caspase 4/GSDMD signaling in colon tumor cells. (A) Western blot analysis CT26 (blank control), empty vector transfected CT26 (vector control) and IL-17F-transfected Clone 1, 2 &3 CT26 cells. N = 3; Compared with vector control. (B) RTCA analysis of the cell growth of the CT26 cell clones. N = 3; Compared with vector control. (C) Western blot analysis of CT26 cell transplanted tumors. (D) Western blot analysis of Il-17f −/− and wild type colon tumors. N = 3; *, P < 0.05; **, P < 0.01; ***, P < 0.001.
Discussion
The key finding of this study was that IL-17F enhanced Caspase 4/GSDMD mediated pyroptosis of endothelial cells. IL-17F upregulated both the mRNA and protein levels of Caspase 4 in endothelial cells, resulting in increased auto-cleaved CASPASE 4 and subsequent generation of the GSDMD N-terminus. This heightened expression of the GSDMD N-terminus, coupled with increased cellular PI uptake and LDH release, revealed that IL-17F promoted pyroptosis of endothelial cells. The assay blocking IL-17F with a neutralizing antibody further confirmed that IL-17F enhanced Caspase 4/GSDMD signaling. While previous studies have reported IL-17F's inhibitory effects on angiogenesis, the precise underlying mechanism has remained elusive32. This study identified the specific targets of IL-17F in endothelial cells by using a smart bioinformatics analysis. If simply comparing the DEGs in endothelial cells treated with and without IL-17F, the huge information may probably obscure these specific targets. Since the inhibitory effects of IL-17F on endothelial cells were reported with different IL-17F concentrations33,34,35,36, the common DEGs induced by IL-17F were identified in this study by Venn analysis of datasets from untreated endothelial cells vs endothelial cells treated with three different concentrations of IL-17F. These 109 common DEGs were primarily associated with migration, confirming the effect of IL-17F on the cell migration of endothelial cells.
Furthermore, IL-17F could upregulate the expression of Ccl20 in both CT26 and EOMA cells. Since CCL20 is the only known high-affinity cognate ligand for CCR637, the enhanced expression of Ccl20 in both CT26 and endothelial cells could explain the increased infiltration of CCR6 + cells in the IL-17F overexpressing CT26 transplanted tumor microenvironment. Despite the decreased ratios of CD31 + endothelial cells, the increased ratio of CCR6 + cells highlighted the potent recruitment ability of CCL20 induced by IL-17F. Clusters of immune cells with positive IFNγ or IL-1β staining, along with higher mRNA levels of Ifnγ and Il-1β could be detected in the IL-17F overexpressing tumors. Since CCR6 + type 3 innate lymphoid cells recruited by CCL20 exhibited anti-tumor effects38, these data suggested the recruited CCR6 + cells may contribute to the anti-tumor effects of IL-17F.
Since IL-17F uses the same IL-17RA and IL-17RC receptors for the downstream signaling, lots of functions of IL-17F and IL-17A were overlapped39. However, IL-17F was secreted in the epithelial cells in the colon and IL-17A was constrained in immune cells, suggesting different effects between IL-17F and IL-17A in colon. It is also reported that IL-17F, not IL-17A provided protection against colitis40. IL-17F exhibited anti-angiogenesis effects in cancers, while IL-17A could induce tumor angiogenesis41. Thus, IL-17A has both anti-tumor and tumor-promoting effects42,43. Moreover, IL-17F could transmit signaling and enhance Caspase 4/GSDMD into the expressing colon cells themselves and inhibit the cell growth of CT26 cells. The mechanism for the differences between IL-17F and IL-17A could be additional receptor or subunit in different cell types44,45. Although further studies on the different molecular signaling between IL-17F and IL-17A were needed, data in this study revealed potent anti-tumor effects and mechanisms for IL-17F in colon cancer. The findings in this study were consistent with our previous report showing reduced IL-17F mRNA expression in colon cancer20, as well as with two other studies indicating that decreased IL-17F levels in colorectal cancer21,22.
In conclusion, this study revealed that IL-17F could modulate the colon tumor microenvironment with inhibited angiogenesis. Notably, a specific mechanism for the angiogenesis inhibition by IL-17F was identified by bioinformatics analysis. IL-17F enhanced Caspase 4/GSDMD mediated non-canonical pyroptosis of endothelial cells. IL-17F emerges as a promising therapeutic target for colon cancer, capable of exerting multifaceted anti-tumor effects.
Data availability
All other data generated within the article are available upon request from the corresponding author.
References
Murphy, C. C. & Zaki, T. A. Changing epidemiology of colorectal cancer: Birth cohort effects and emerging risk factors. Nat. Rev. Gastroenterol. Hepatol. 21, 25–34 (2024).
Siegel, R. L., Wagle, N. S., Cercek, A., Smith, R. A. & Jemal, A. Colorectal cancer statistics, 2023. CA A Cancer J. Clin. 73, 233–254 (2023).
Lonardi, S. & Pietrantonio, F. New options for late-line treatment of metastatic colorectal cancer. Nat. Rev. Gastroenterol. Hepatol. 21, 76–77 (2024).
Martinelli, E. & Ciardiello, F. Angiogenesis inhibition in metastatic colorectal cancer continuum of care. Lancet 402, 4–5 (2023).
Liu, Z.-L., Chen, H.-H., Zheng, L.-L., Sun, L.-P. & Shi, L. Angiogenic signaling pathways and anti-angiogenic therapy for cancer. Signal Trans. Target. Therapy 8, 198 (2023).
Lee, S. H. et al. Immune microenvironment and lymph node yield in colorectal cancer. Br. J. Cancer 129, 917–924 (2023).
Pelka, K. et al. Spatially organized multicellular immune hubs in human colorectal cancer. Cell 184, 4734-4752.e4720 (2021).
Beyaz, S. et al. Dietary suppression of MHC class II expression in intestinal epithelial cells enhances intestinal tumorigenesis. Cell Stem Cell 28, 1922-1935.e1925 (2021).
Alzamami, A. Implications of single-cell immune landscape of tumor microenvironment for the colorectal cancer diagnostics and therapy. Med. Oncol. 40, 352 (2023).
Mezheyeuski, A. et al. An immune score reflecting pro- and anti-tumoural balance of tumour microenvironment has major prognostic impact and predicts immunotherapy response in solid cancers. eBioMedicine 88, 104452 (2023).
Cao, Y., Langer, R. & Ferrara, N. Targeting angiogenesis in oncology, ophthalmology and beyond. Nat. Rev. Drug Discov. 22, 476–495 (2023).
Zalpoor, H. et al. The roles of metabolic profiles and intracellular signaling pathways of tumor microenvironment cells in angiogenesis of solid tumors. Cell Commun. Signal. 20, 186 (2022).
Choi, Y. & Jung, K. Normalization of the tumor microenvironment by harnessing vascular and immune modulation to achieve enhanced cancer therapy. Exp. Mol. Med. 55, 2308–2319 (2023).
Fang, J. et al. Exploring the crosstalk between endothelial cells, immune cells, and immune checkpoints in the tumor microenvironment: New insights and therapeutic implications. Cell Death Dis. 14, 586 (2023).
Mills, K. H. G. IL-17 and IL-17-producing cells in protection versus pathology. Nat. Rev. Immunol. 23, 38–54 (2023).
Vitiello, G. A. & Miller, G. Targeting the interleukin-17 immune axis for cancer immunotherapy. J. Exp. Med. 217, e20190456 (2020).
Nemati, K., Golmoghaddam, H., Hosseini, S. V., Ghaderi, A. & Doroudchi, M. Interleukin-17FT7488 allele is associated with a decreased risk of colorectal cancer and tumor progression. Gene 561, 88–94 (2015).
Omrane, I. et al. Significant association between IL23R and IL17F polymorphisms and clinical features of colorectal cancer. Immunol. Lett. 158, 189–194 (2014).
Li, G. et al. The associations between interleukin-17 single-nucleotide polymorphism and colorectal cancer susceptibility: A systematic review and meta-analysis. World J. Surg. Oncol. 20, 116 (2022).
Tong, Z. et al. A protective role by interleukin-17F in colon tumorigenesis. PLoS One 7, e34959 (2012).
Al-Samadi, A. et al. Distinctive expression pattern of interleukin-17 cytokine family members in colorectal cancer. Tumor. Biol. 37, 1609–1615 (2016).
Liu, Y. et al. Expression and location of IL-17A, E, F and their receptors in colorectal adenocarcinoma: Comparison with benign intestinal disease. Pathol. Res. Pract. 214, 482–491 (2018).
Sato, Y., Fu, Y., Liu, H., Lee, M. Y. & Shaw, M. H. Tumor-immune profiling of CT-26 and Colon 26 syngeneic mouse models reveals mechanism of anti-PD-1 response. BMC Cancer 21, 1222 (2021).
Roshan Moniri, M. et al. Dynamic assessment of cell viability, proliferation and migration using real time cell analyzer system (RTCA). Cytotechnology 67, 379–386 (2015).
Nozato, K. et al. IL-17F induces CCL20 in bronchial epithelial cells. J. Allergy 2011, 587204 (2011).
Meitei, H. T., Jadhav, N. & Lal, G. CCR6-CCL20 axis as a therapeutic target for autoimmune diseases. Autoimmun. Rev. 20, 102846 (2021).
Wang, C., Kang, S. G., Lee, J., Sun, Z. & Kim, C. H. The roles of CCR6 in migration of Th17 cells and regulation of effector T-cell balance in the gut. Mucosal Immunol. 2, 173–183 (2009).
Kayagaki, N. et al. Caspase-11 cleaves gasdermin D for non-canonical inflammasome signalling. Nature 526, 666–671 (2015).
Devant, P. et al. Structural insights into cytokine cleavage by inflammatory caspase-4. Nature 624, 451–459 (2023).
Shi, J. et al. Cleavage of GSDMD by inflammatory caspases determines pyroptotic cell death. Nature 526, 660–665 (2015).
Wang, K. et al. Structural mechanism for GSDMD targeting by autoprocessed caspases in pyroptosis. Cell 180, 941-955.e920 (2020).
Mikkola, T., Almahmoudi, R., Salo, T. & Al-Samadi, A. Variable roles of interleukin-17F in different cancers. BMC Cancer 22, 54 (2022).
Starnes, T. et al. Cutting edge: IL-17F, a novel cytokine selectively expressed in activated T cells and monocytes, regulates angiogenesis and endothelial cell cytokine production1. J. Immunol. 167, 4137–4140 (2001).
Almahmoudi, R. et al. Interleukin-17F has anti-tumor effects in oral tongue cancer. Cancers 11, 650 (2019).
Xie, Y., Sheng, W., Xiang, J., Ye, Z. & Yang, J. Interleukin-17F suppresses hepatocarcinoma cell growth via inhibition of tumor angiogenesis. Cancer Invest. 28, 598–607 (2010).
Almahmoudi, R. et al. The effect of interleukin-17F on vasculogenic mimicry in oral tongue squamous cell carcinoma. Cancer Sci. 112, 2223–2232 (2021).
Wasilko, D. J. et al. Structural basis for chemokine receptor CCR6 activation by the endogenous protein ligand CCL20. Nat. Commun. 11, 3031 (2020).
Bruchard, M. et al. Recruitment and activation of type 3 innate lymphoid cells promote antitumor immune responses. Nat. Immunol. 23, 262–274 (2022).
Miossec, P. & Kolls, J. K. Targeting IL-17 and TH17 cells in chronic inflammation. Nat. Rev. Drug Discov. 11, 763–776 (2012).
Tang, C. et al. Suppression of IL-17F, but not of IL-17A, provides protection against colitis by inducing Treg cells through modification of the intestinal microbiota. Nat. Immunol. 19, 755–765 (2018).
Chung, A. S. et al. An interleukin-17-mediated paracrine network promotes tumor resistance to anti-angiogenic therapy. Nat. Med. 19, 1114–1123 (2013).
Razi, S., Baradaran Noveiry, B., Keshavarz-Fathi, M. & Rezaei, N. IL-17 and colorectal cancer: From carcinogenesis to treatment. Cytokine 116, 7–12 (2019).
Hurtado, C. G., Wan, F., Housseau, F. & Sears, C. L. Roles for interleukin 17 and adaptive immunity in pathogenesis of colorectal cancer. Gastroenterology 155, 1706–1715 (2018).
Su, Y. et al. Interleukin-17 receptor D constitutes an alternative receptor for interleukin-17A important in psoriasis-like skin inflammation. Sci. Immunol. 4, eaau9657 (2019).
Knizkova, D. et al. CMTM4 is a subunit of the IL-17 receptor and mediates autoimmune pathology. Nat. Immunol. 23, 1644–1652 (2022).
Acknowledgements
The authors thank Dr. Yinping Li for constructive discussions and sharing reagents.
Funding
This work was supported by Basic-Clinical Medicine Co-construction Project of Wuhan University (Grant No.: JCZN2022011).
Author information
Authors and Affiliations
Contributions
Z.T. conceived the project; Y.Z. and M.Y. performed the majority of experiments, acquired data and analyzed the data. R.F., W.L., Z.C., S.L., H.L., C.Z. and Y.C. contributed to the data collection and data analysis. Y.Z., M.Y., and Z.T. wrote the manuscript. All authors reviewed and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhou, Y., Yang, M., Fu, R. et al. Interleukin-17F suppressed colon cancer by enhancing caspase 4 mediated pyroptosis of endothelial cells. Sci Rep 14, 18363 (2024). https://doi.org/10.1038/s41598-024-69436-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-69436-x
- Springer Nature Limited