
Abstract
Information about the morphology of the intracranial pressure waveform, as well as the variations in intracranial pressure (ICP) and compliance in pediatric patients are essential to diagnose and predict the progression of various neurological conditions. However, there is no information on the morphology of the IP waveform in neurologically healthy pediatric patients. In the present study, intracranial compliance was therefore analyzed in neurologically healthy patients with the aid of a noninvasive device. The study was an observational, cross-sectional study. Fifty-five neurologically healthy participants were included. Data on intracranial compliance with the patient in two positions, lying down (0°) and seated (45°), were collected with a noninvasive extracranial sensor, which allowed the intracranial pressure waveforms to be recorded. The values of the ratio P2/P1 were then analyzed. A questionnaire (with a scale from zero to ten, where ten corresponds to the highest level of satisfaction) was applied for patients to evaluate their satisfaction with the sensor. Patients were 10 years old (average), and most of them were (58%). Mean P2/P1 ratio was 0.94 (sd = 0.14) in the supine position and 0.91 (sd = 0.15) in the seated position. Participants were satisfied with the length of time for which the equipment was used (9.8, sd = 0.71). The device did not cause any discomfort. The noninvasive method used was well accepted by the patients. Intracranial compliance values were determined by analysis of the P2/P1 ratio in neurologically healthy pediatric population.
Trial registration: Brazilian Registry of Clinical Trials Identifier: RBR-5j74ddg.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Static intracranial pressure (ICP) in children and adolescents is considered raised when it is between 18 and 20 mmHg. Intracranial hypertension (ICH) is frequently secondary to traumatic lesions but can also occur in patients with, for example, hydrocephalus, brain tumors or abnormalities in venous drainage in the central nervous system (CNS)1,2.
Invasive monitoring of ICP is not suitable for all patients with suspected ICH (lack of level 1 evidence). Use of a catheter with an intraventricular transducer (the gold standard) can expose the patient to risks such as CNS infection and obstructions3. Apart from the risk of hemorrhage and infection that can occur caused by the surgical procedure, other disadvantages of this method include the need to restrict these procedures to a neurosurgical environment and the high cost4,5,6,7.
In infants there are two further possibilities for assessing ICP indirectly and noninvasively by means of neurological examination: palpation of the anterior fontanelle and serial measurements of head circumference. Although these investigative methods are used for pediatric screening, neither of them is used when dealing with patients with acute and severe neurological conditions. Complementary alternative noninvasive measures for evaluating possible changes in ICP have been developed and include transcranial Doppler ultrasound and measurement of the optic nerve sheath diameter, among others3,5,6.
In spite of constant improvements in these methods, none of them has been able to quantify ICP in absolute values or to achieve levels of accuracy that are sufficiently high to enable them to be used to guide therapeutic decisions in clinical practice5,6,7. Use of these techniques is contraindicated in healthy patients even for research purposes, which makes discussion of the topic difficult, and consequently there are few articles on the subject2. Studies evaluating intracranial compliance and ICP in children therefore use values measured in patients with neurological abnormalities such as traumatic brain injury (TBI), craniosynostosis or hydrocephalus. In other words, there are to date no references for ICP values in healthy pediatric individuals8.
Studied for the first time in 1881, ICP waveform morphology was described by Wendelber1,2,9,10,11. With the advent of new technologies, changes in ICP can be evaluated from the morphology of the waveform3,8,9.
Intracranial compliance can be considered an indirect measure of ICP as it quantifies the relationship between changes in intracranial volume and pressure5,8,9,11,12,13,14,15. Reduced compliance constitutes a risk to the central nervous system as small changes in intracranial volume can cause a disproportional increase in ICP, potentially culminating in ICH.
The ICP waveform has three different peaks. The first peak (P1, or “percussion wave”) is the result of arterial pressure transmitted from the choroid plexus to the cerebral ventricle. The second peak (P2) corresponds to the tidal wave and is related to intracranial compliance. The last peak (P3) is the result of aortic valve closure. Changes in these peaks represent changes in both arterial blood pressure and cerebral blood volume. In normal circumstances, P1 is larger than the other peaks. When ICP changes, the relative amplitudes of the peaks change as well (Fig. 1)9,10,13,14,15. For normal ICP, the amplitudes of the peaks are such that P1 > P2 > P3. However, as intracranial compliance decreases and ICP increases, the morphology of the waveform changes and the amplitude of P2 increases in relation to P1 and P310,11.

Intracranial pressure waveform. Note: Brasil S. et al. 2021 were responsible for another advance in the understanding of the ICP waveform. In a class I wave, P1 is greater than the other two peaks, suggesting normal ICP. In a class II waveform, P2 increases slightly and becomes equal to or slightly greater than P1, suggesting potential pathological alterations. In class III, P2 and P3 are greater than P1, probably indicating a pathological condition. In a class IV waveform, the peaks are no longer identifiable, or P2 and P3 become markedly higher than P1, reflecting decompensation of ICP parameters.
The noninvasive ICP sensor used in the present study was developed as an alternative for noninvasive monitoring of ICP and compliance and the design is based on results and waveforms obtained using gold-standard methods (intraventricular catheter) in adult patients. Using a novel approach, the sensor provides accurate monitoring of intracranial compliance by mathematical analysis of the morphology of the ICP waveform without the need for an invasive catheter. The technique used involves capturing small variations in cranial volume by means of a pin connected to a displacement sensor on the surface of the skin in the frontotemporal region. The resulting skull deformations are recorded by the system in the form of pressure waves, and the relationship between the peaks of these waves determines whether compliance is or is not preserved10,11,13,14,16.
In light of the difficulties in objectively measuring ICP in the pediatric population, the risks of using invasive methods and the limited knowledge of intracranial compliance in children, this study sought to analyze intracranial compliance in neurologically healthy pediatric patients in a novel manner by means of a noninvasive sensor and to analyze the ICP waveforms obtained using the sensor. The study also investigated whether there was a correlation between baseline variables (e.g., vital signs and demographic data) and intracranial compliance.
Methodology
Study design and ethical considerations
The study was an observational, cross-sectional study and was carried out in a high-complexity, exclusively pediatric hospital in Southern Brazil. The protocol for the clinical trial was approved by the local ethic committee under CAAE reference no. 42229121.80000.0097 between February 2021 and August 2022, and Brazilian Registry of Clinical Trials Identifier: RBR-5j74ddg. Informed consent was obtained from the patients’ legal representatives. This work was in accordance with the principles of the Helsinki Convention and its subsequent amendments, as well as the Brazilian guidelines provided for in resolution 466/2012, with the data given in writing after approval.
Inclusion criteria
To be eligible for the study, participants had to meet the following inclusion criteria: male or female; aged between 2 and 17 years 11 months and 29 days; normal neurological findings in tests carried out by a qualified physician; absence of any signs or symptoms associated with intracranial hypertension (e.g., headache, vision changes, nausea, vomiting, irritability, cognitive changes, altered level of consciousness, papilledema) based on a previously completed questionnaire; signature of a voluntary informed-consent form (VICF) by one the participant’s parents or by his/her legal guardian; and signature of a voluntary informed-assent form (VIAF) by the participant him/herself.
As the study started in February 2021, during the Covid-19 pandemic, when sanitary restrictions were imposed worldwide, it was decided to carry out the study in a single center and that neurologically healthy participants would take part in the study in a hospital setting.
The following exclusion criteria were used: individuals who had recently undergone surgery involving the scalp; recent sedation; skull deformities that prevented the sensor being put in position; extensive injury to the scalp; patients with any neurological abnormalities; chronic diseases; low-quality ICP waveform signal from the noninvasive sensor; refusal of parents or legal guardian to sign the VICF/VIAF; request by participants/parents/legal guardian to leave the study for some reason; and participants who did not have all the necessary clinical information.
Data collection
The first stage consisted of the collection of sociodemographic data (age in years, sex, preexisting diseases); vital signs (systolic and diastolic blood pressure, temperature, oxygen saturation, heart rate and respiratory rate); weight, height, and head circumference. Each patient was then assessed by a neurologist, who performed a neurological examination. If the results of the examination were normal, noninvasive ICP monitoring was carried out with the noninvasive sensor. The data were collected and stored with Cognito Forms, an electronic data-capture system that complies with the General Data Protection Law (GDPL) and the confidentiality of the study.
Lastly, a questionnaire was applied to determine user satisfaction with the device. The questions covered the level of satisfaction in a 0–10 scale (where zero was the lowest and 10 the highest rate). The satisfaction was assessed after a thorough explanation by researchers about the device and the way it works. The satisfaction covered questions about time using the noninvasive sensor; and the level of discomfort when using the device.
Neurological assessment
The neurological assessment was essential to exclude any participants with abnormalities that could affect changes in compliance. To this end, the physician looked for signs and symptoms suggestive of changed ICP, such as an altered level of consciousness, headache, vomiting, nausea, vision changes, sleepiness, poor school performance, inattention, irritability, dizziness and seizure episodes. The same physician then analyzed the results of the neurological examination. This included pupillary and other pairs of cranial nerves reflexes assessment; muscle strength and deep tendon reflex; static and dynamic balance; motor coordination; the presence or absence of Kernig’s and Brudzinski’s sign; and skull deformities.
Complementary examinations related to the reason for hospitalization were also checked, and patients were examined before being discharged from hospital after they had completed the procedure and when they no longer had any clinical or pain-related complaints and were not using medication known to interfere with intracranial compliance.
Use of the noninvasive sensor to monitor and interpret the waveforms and the waveform parameters associated with intracranial compliance
The noninvasive method described here was developed in 2008 by researchers at the University of São Paulo. Braincare® wireless system is currently provided by Braincare Desenvolvimento e Inovação Tecnológica S.A. The device detects nanometric expansion of the outer surface of the bones of the skull caused by changes in ICP. It consists of a sensor on a strap that is attached firmly to the individual’s head. A pin in the sensor is in contact with the surface of the person’s head and keeps the device in the frontotemporal region. Bone deformations produced by changes in ICP cause the pin to move, bending the cantilever beam in the sensor, which captures these micro deformations by means of strain gauges16.
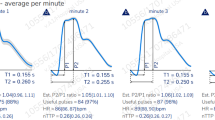
Each patient was monitored in two different positions for five minutes at a time with the noninvasive sensor. First, the patient remained supine (0°) for five minutes and then seated at an angle of 45° for the same length of time. The sensor can collect, filter, amplify and digitize the signal being monitored, and a report is produced with the associated parameters at 1-min intervals (supplemental material 1).
After the ICP had been monitored, the software saved the data in files that were subsequently loaded into the Braincare® system for analysis. The result is a report containing the time to peak (TTP) and the ratio P2/P1. The TTP was defined as the time from the beginning of the pulse to the moment when the ICP reaches its highest point (P1 or P2). The ratio P2/P1 is a measure of intracranial compliance and was defined as the ratio of the amplitude of P2 to the amplitude of P1 (R = AmpP2/AmpP1). The noninvasive monitoring data were obtained by analyzing the morphology of the ICP waveform (Supplemental material 01)16.
Based on studies carried out with the device in adults with a variety of clinical conditions that influenced intracranial compliance, the value of P2/P1 in the adult population can be interpreted as follows: values > 1.2 are suggestive of changed compliance; values between 1 and 1.2 may be associated with changed compliance and suggest that further observation of the patient is needed; and values between 0.65 and 1 are considered normal13,14,16,17,18,19,20,22,23,25,26,27.
Statistical analysis and sample-size calculation
The analyses were carried out by an independent statistician, who was neither a physician nor a principal investigator. The descriptive analyses were reported in terms of mean, median, minimum value, maximum value and standard deviation, and the qualitative variables were described in terms of frequency and percentage. The data were tested for normality with the Kolmogorov Smirnov test; a positive result was considered to indicate a normal distribution (p < 0.05). Pearson and Spearman correlation tests were performed between all the baseline variables (such as age, weight, height, sex, heart rate, respiratory rate, diastolic pressure, systolic pressure, and oxygen saturation on examination) and the outcome of interest (mean P2/P1). Weak, intermediate, and strong correlations (r) (r < 0.3; 0.3 > r < 0.6; r > 0.61, respectively) were given with their respective values of p. Values of p < 0.05 were considered to indicate statistical significance. The data were organized in an Excel® spreadsheet and analyzed with Stata version 14.1, StataCorp LP, USA.
Because of the novel nature of the study and, consequently, the lack of any information in the literature on the ratio P2/P1, it was decided for the purposes of calculating sample size that the first ten patients recruited on the study would serve as the basis for identifying the number of individuals needed to ensure a mean with 99.9% confidence (mean P2/P1 = 0.9 and standard deviation = 0.12, i.e., the margin of error was considered to be 0.12/0.9 = 13%). Based on the margin of error and standard deviation of the first ten patients and assuming a t distribution, it was found that 16 patients would be the minimum required number to assess the primary objective of the study.
Ethical approval
The study was an observational, cross-sectional study and was carried out in a high-complexity, exclusively pediatric hospital in Southern Brazil. The protocol for the clinical trial was approved by the local ethic committee under CAAE reference no. 42229121.80000.0097 and Brazilian Registry of Clinical Trials Identifier: RBR-5j74ddg. Informed consent was obtained from the patients’ legal representatives.
Results
Characteristics of the study population
Initially, 61 neurologically healthy children were invited to be monitored with the noninvasive monitor. Of these, five were excluded because of the poor quality of the waveforms, and one patient declined to take part in the study (Fig. 2).

Flowchart with patients’ inclusion. Note: Adapted from CONSORT.
Overall, 55 children were included in the study, of whom 58.2% were males. Mean age was 10.0 years old, mean weight 39.08 kg, mean BMI 15.95 kg/m2 and mean head circumference 53.12 cm. All the children were well-nourished and had normal height and weight for their age according to the World Health Organization (WHO) growth curve. None of the children had neurological comorbidities. The group analyzed did not have abnormal vital signs in their respective age groups (Table 1 and Supplementary table 2).
Primary outcome: assessment of intracranial compliance
Intracranial compliance was monitored with the noninvasive sensor in each patient (supine at 0° and seated at 45°), giving a total of 110 readings. The mean of the ratio P2/P1 in the supine position (0° inclination) was 0.94 (sd = 0.14) and in the seated position (45° inclination) was 0.91 (sd = 0.15).
It should be noted that the median P2/P1 ratio values in the supine position were 0.91, and in the sitting position, they were 0.90. The interquartile range for both positions (0° and 45° of inclination) varied from 0.86 to 1.05.
Figure 3A and B show the distribution of the ratio P2/P1 in the two positions (0° and 45° inclination).

The P2/P1 ratio in the supine and seated positions. Legend: A shows the values of P2/P1 for each patient position; B shows the corresponding figures for each patient position with the monitor on the left or right side of the patient’s head.
Secondary outcome: participant satisfaction with the use of the device
Analysis of the answers to the questionnaire revealed that the participants gave the maximum score for the explanation about the use of the sensor and a score below the maximum for the question about the length of time for which the sensor was used. According to the answers, the participants did not experience any discomfort when using the device (Table 2).
Exploratory outcomes: correlations between baseline variables and compliance
The Pearson correlation analyses showed that participants’ vital signs did not influence the ratio P2/P1 (Supplementary material 3). When the variables age and P2/P1 were compared, no significant correlation was found in either position, supine (R: − 0.038; p: 0.78) or seated (R: − 0.24; p: 0.083). However, there was a tendency towards an inverse correlation in the seated position (45° inclination) (Fig. 4A and B).

Correlation between P2/P1 and age. Legend: A. P2/P1 01 = monitoring in the supine position/0°. B. P2/P1 02 = monitoring in the seated position/45º.
An inverse correlation was observed between head circumference and P2/P1 in the seated position (R: − 0.3 and p: 0.028) (Fig. 5A and B).

Correlation between P2/P1 and Cephalic Circumference. Legend: A. P2/P1 01 = monitoring in the supine position/0°. B. P2/P1 02 = monitoring in the seated position/45º.
Correlations with other variables (weight, height, heart rate, respiratory rate, systolic pressure, diastolic pressure and oxygen saturation) did not show a statistically significant response. These relations can be seen in the supplementary material 3.
As mentioned previously in the methodology section, children were monitored with the sensor for five minutes. The minute-by-minute analysis of the waveform showed it was difficult to obtain uniform signals. That could be seen in the points in the graph, when the line returned to the baseline (supplementary graph 4).
Discussion
Assessment of ICP, its variations over the cardiac cycle and cardiac pulsatility in pediatric patients, as well as measurement of intracranial compliance, remains a major challenge to date. This is the first study to present descriptive analyses of variations in the ratio P2/P1 in neurologically healthy pediatric population.
The epidemiologic variables and vital signs of the study population were all within a normal range, and all the participants were considered well-nourished. Consequently, no significant correlations were identified between P2/P1 and weight, age, BMI or height, confirming the normal nature of the sample and indicating that none of these factors are likely to have influenced the intracranial compliance measurements.
The most important finding of this study was the range of normal values for the ratio P2/P1 in neurologically healthy, well-nourished patients, for which the interquartile range varied from 0.86 to 1.05 when the results for both positions used were considered.
Another important finding in the group studied was that the mean of the ratio P2/P1 in the supine position (0°) was 0.94 (sd = 0.14) and in the seated position (45°) 0.91 (sd = 0.15), corroborating the findings in the literature, which show that P2/P1 can change as a result of the “stress” generated by the change in posture. Under normal/ “healthy” conditions, a reduction in ICP is therefore expected when an individual changes from a supine position to a seated or standing position. Hence, the small postural change from supine (0°) to seated (45°) in this study further confirms the good health of the study population25.
Studies evaluating the Brain4Care® device in adult and pediatric patients have only recently been undertaken, and many are still in progress. There are, however, published studies using this technique with neurologically affected adults13,14,16,17,18,19,20,22,23,25,26,27.
In one of these studies, the authors investigated the correlation and agreement between the ICP waveform morphology determined by the noninvasive method and by the gold-standard invasive method in 18 patients hospitalized for stroke. There was a strong correlation and agreement between the waveform morphologies determined the two methods, and the ratio P2/P1 measured by the noninvasive method had a cutoff point of 1.06, corroborating the normal range of values found in the present study of pediatric patients and further confirming the normal values of ICP in our sample24.
To date, the only published study investigating probable normal ICP values with a noninvasive sensor in a pediatric population is that by Ballestero et al. The authors evaluated four groups of patients; three of these consisted of patients with some degree of ventricular dilation (with or without hydrocephalus), and the fourth was a control group consisting of 28 patients considered neurologically healthy who were being followed up regularly in the pediatric outpatient unit22.
The patients monitored in the study by Ballestero et al. varied from four months to 17 years (n = 28), and the mean value of P2/P1 in the supine position (in the healthy patients) was 0.75 (0.43–1.06). The values for our patients differed from these, probably because of the sample size, age factor or different methodology. Ballestero et al. evaluated children with an open fontanelle, which can interfere in the result for ICP. Furthermore, the authors used the first version of the noninvasive sensor and only monitored patients in one position, unlike in the present study, in which the wireless version of the sensor was used, and patients were monitored in two positions (supine and seated) as it is known that compliance can change in different positions22.
The results for patient satisfaction with the use of the device indicated that the sensor not only was easy to handle, caused minimal discomfort and did not produce any pain, but also could be easily understood by the pediatric patients. Because it is portable and small and can be secured to the head painlessly with the straps, the device is easy to use in routine clinical practice.
A curious finding in our study was the inverse correlation between head circumference and P2/P1 in the supine position. Although a similar result was not observed for age, there was a tendency toward the same inverse correlation. One explanation for this may be related to heart rate, which is higher in very young infants27,28.
Another explanation may be related to bone thickness. One study investigated skull thickness in pediatric patients and compared the findings with the corresponding figures for adults. The thickness of different parts of the skull (parietal, temporal and occipital bones) in children was analyzed using stereotactic electroencephalography (SEEG) by Rabbani et al., who confirmed that advancing age is typically associated with an increase in the thickness of the calvaria. Hence, the sensor may be more sensitive when measuring ICP in pediatric patients. Further studies and analyses are needed to corroborate these suggestions29,30.
Limitations
A number of limitations were identified in the study. The first one is related to the sensor, which is sensitive to movements, no matter how small, such as blinking or opening or closing the mouth, as well as the use of a pacifier and even external sounds, such as crying. To ensure good-quality results when monitoring, pediatric patients must therefore be relaxed and still. No sedation of any kind was used as some medications influence ICP18.
Another limitation is that as the patients were neurologically healthy, ICP was not measured using invasive methods (ICP/collection of CSF and measurement of CSF pressure), which prevented any real time comparison being made.
Conclusion
In this innovative study, we have described an estimation of ICP values by means of analysis of the ratio P2/P1 in a neurologically normal pediatric population. Most of the patients evaluated had P2/P1 values between 0.86 and 1.05, the probable range of normal values when the interquartile range is considered as reference. The noninvasive method studied here can be used in children and is well accepted by this population in terms of usability and handling.
Because of the exploratory nature of our study, we recommend that further studies be carried out with this noninvasive device in order to better understand ICP in the pediatric population and how the device can be used in clinical practice in patients with suspected ICH.
Data availability
The data sets generated and/or analyzed during the current study are not publicly available because we do not authorization from the local research ethics committee but are available from the corresponding author upon request and approval from the local research ethics committee.
References
Kukreti, V., Mohseni-Bod, H. & Drake, J. Management of raised intracranial pressure in children with traumatic brain injury. J. Pediatr. Neurosci. 9(3), 207–215. https://doi.org/10.4103/1817-1745.147572 (2014) (PMID: 25624921; PMCID: PMC4302538).
Pedersen, S. H., Lilja-Cyron, A., Astrand, R. & Juhler, M. Monitoring and measurement of intracranial pressure in pediatric head trauma. Front. Neurol. 14(10), 1376. https://doi.org/10.3389/fneur.2019.01376 (2020) (PMID:32010042;PMCID:PMC6973131).
Moraes, F. M. & Silva, G. S. Noninvasive intracranial pressure monitoring methods: A critical review. Arq. Neuropsiquiatr. 79(5), 437–446. https://doi.org/10.1590/0004-282X-ANP-2020-0300 (2021) (PMID: 34161530).
Tadevosyan, A. & Kornbluth, J. Brain herniation and intracranial hypertension. Neurol. Clin. 39(2), 293–318. https://doi.org/10.1016/j.ncl.2021.02.005 (2021) (Epub 2021 Mar 31 PMID: 33896520).
Aimierska, A. et al. Compliance of the cerebrospinal space: comparison of three methods. Acta Neurochir. Wien. 163(7), 1979–1989. https://doi.org/10.1007/s00701-021-04834-y (2021) (Epub 2021 Apr 14. PMID: 33852065; PMCID: PMC8195969).
Swanson, J. W. et al. Evaluation of optical coherence tomography to detect elevated intracranial pressure in children. JAMA Ophthalmol. 135(4), 320–328. https://doi.org/10.1001/jamaophthalmol.2017.0025 (2017) (PMID:28241164;PMCID:PMC5470406).
Bartsikhovsky, T., Klar, M. M., Bekerman, I., Nagieva, S. & Tal, S. Diagnostic tool for initial evaluation of the intracranial pressure on computed tomography in pediatric patients with headache. PLoS One 14(5), e0216812. https://doi.org/10.1371/journal.pone.0216812 (2019) (PMID:31086412;PMCID:PMC6516648).
Czosnyka, M. & Czosnyka, Z. Origin of intracranial pressure pulse waveform. Acta Neurochir. (Wien) 162(8), 1815–1817. https://doi.org/10.1007/s00701-020-04424-4 (2020) (Epub 2020 Jun 13 PMID: 32535797).
Rabelo, N. N. et al. The historic evolution of intracranial pressure and cerebrospinal fluid pulse pressure concepts: Two centuries of challenges. Surg. Neurol. Int. 14(12), 274. https://doi.org/10.25259/SNI_53_2021 (2021) (PMID:34221605;PMCID:PMC8247667).
Benson, J. C., Madhavan, A. A., Cutsforth-Gregory, J. K., Johnson, D. R. & Carr, C. M. The Monro-Kellie Doctrine: A review and call for revision. AJNR Am. J. Neuroradiol. https://doi.org/10.3174/ajnr.A7721 (2022) (Epub ahead of print. PMID: 36456084).
Sonig, A. et al. The historical evolution of intracranial pressure monitoring. World Neurosurg. 138, 491–497. https://doi.org/10.1016/j.wneu.2020.03.028 (2020) (Epub 2020 Mar 14 PMID: 32179192).
Canac, N., Jalaleddini, K., Thorpe, S. G., Thibeault, C. M. & Hamilton, R. B. Review: Pathophysiology of intracranial hypertension and noninvasive intracranial pressure monitoring. Fluids Barriers CNS. 17(1), 40. https://doi.org/10.1186/s12987-020-00201-8 (2020) (PMID:32576216;PMCID:PMC7310456).
Ocamoto, G. N. et al. Intracranial compliance concepts and assessment: A scoping review. Front. Neurol. 25(12), 756112. https://doi.org/10.3389/fneur.2021.756112 (2021) (PMID:34759884;PMCID:PMC8573119).
Brasil, S., Solla, D.J.F., Nogueira, R.C., Jacobsen Teixeira, M., Malbouisson, L.M.S., Paiva, W.S. Intracranial compliance assessed by intracranial pressure pulse waveform. Brain Sci. 11(8), 971. https://doi.org/10.3390/brainsci11080971. (2021). PMID: 34439590; PMCID: PMC8392489. 163(7), 1979-1989. https://doi.org/10.1007/s00701-021-04834-y. Epub 2021 Apr 14. PMID: 33852065; PMCID: PMC8195969
Brasil, S. et al. Noninvasive intracranial pressure waveforms for estimation of intracranial hypertension and outcome prediction in acute brain-injured patients. J. Clin. Monit. Comput. 18, 1–8. https://doi.org/10.1007/s10877-022-00941-y (2022) (Epub ahead of print. PMID: 36399214; PMCID: PMC9673225).
Andrade, R. A. P. et al. A nanometer resolution wearable wireless medical device for non invasive intracranial pressure monitoring. IEEE Sensors J. https://doi.org/10.1109/JSEN.2021.3090648 (2021).
Hu, X., Xu, P., Scalzo, F., Vespa, P. & Bergsneider, M. Morphological clustering and analysis of continuous intracranial pressure. IEEE Trans. Biomed. Eng. 56(3), 696–705. https://doi.org/10.1109/TBME.2008.2008636 (2009) (Epub 2008 Nov 7. PMID: 19272879; PMCID: PMC2673331).
Folchini, C. M. et al. From disease to noninvasive intracranial monitoring. Arq. Neuropsiquiatr. 80(5), 539–542. https://doi.org/10.1590/0004-282X-ANP-2021-0298 (2022) (PMID: 35293558).
Vilela, G. H. et al. Validation of a new minimally invasive intracranial pressure monitoring method by direct comparison with an invasive technique. Acta Neurochir. Suppl. 122, 97–100. https://doi.org/10.1007/978-3-319-22533-3_19 (2016).
Brasil, S. et al. Cerebral hemodynamics and intracranial compliance impairment in critically Ill COVID-19 patients: A pilot study. Brain Sci. 11(7), 874. https://doi.org/10.3390/brainsci11070874 (2021) (PMID:34208937;PMCID:PMC8301789).
Cabella, B. et al. Validation of a new noninvasive intracranial pressure monitoring method by direct comparison with an invasive technique. Acta Neurochir. Suppl. 122, 93–96. https://doi.org/10.1007/978-3-319-22533-3_1 (2016).
Ballestero, M. F. M., Frigieri, G., Cabella, B. C. T., de Oliveira, S. M. & de Oliveira, R. S. Prediction of intracranial hypertension through noninvasive intracranial pressure waveform analysis in pediatric hydrocephalus. Childs Nerv. Syst. 33(9), 1517–1524. https://doi.org/10.1007/s00381-017-3475-1 (2017).
Frigieri, G. et al. Analysis of a non-invasive intracranial pressure monitoring method in patients with traumatic brain injury. Acta Neurochir. Suppl. 126, 107–110. https://doi.org/10.1007/978-3-319-65798-1_2315 (2018).
de Moraes, F. M. et al. Waveform morphology as a surrogate for ICP monitoring: A comparison between an invasive and a noninvasive method. Neurocrit. Care. 37(1), 219–227. https://doi.org/10.1007/s12028-022-01477-4 (2022) (Epub 2022 Mar 24. PMID: 35332426; PMCID: PMC8947812).
Nagai Ocamoto, G. et al. Noninvasive intracranial pressure monitoring in chronic stroke patients with sedentary behavior: A pilot study. Acta Neurochir. Suppl. 131, 55–58. https://doi.org/10.1007/978-3-030-59436-7_12 (2021) (PMID: 33839818).
Dias, C. Analysis of a Noninvasive intracranial pressure monitoring method in patients with traumatic brain injury. 2016 Marc. Protocol 262–13 (University of Porto).
Fleming, S. et al. Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: A systematic review of observational studies. Lancet 377(9770), 1011–1018. https://doi.org/10.1016/S0140-6736(10)62226-X (2011) (PMID:21411136;PMCID:PMC3789232).
Hassett, C. E. et al. Assessment of cerebral autoregulation using invasive and noninvasive methods of intracranial pressure monitoring. Neurocrit. Care https://doi.org/10.1007/s12028-022-01585-1 (2022).
Xie, Z. H. et al. Effect of different parts of skull thickness on stereotactic electroencephalogram in children. Zhonghua Yi Xue Za Zhi. 98(28), 2238–2241. https://doi.org/10.3760/cma.j.issn.0376-2491.2018.28.005 (2018) (Chinese PMID: 30078277).
Rabbani, C. C. et al. Association of intracranial hypertension with calvarial and skull base thinning. Otol. Neurotol. 40(6), e619–e626. https://doi.org/10.1097/MAO.0000000000002249 (2019) (PMID: 31045889).
Acknowledgements
In memoriam Prof. Sérgio Mascarenhas. The authors wish to thank the Brain4care team; the patients and their parents or legal guardians; and the administrative and care team at the hospital.
Funding
Financial support was provided by Braincare Desenvolvimento e Inovação Tecnológica S.A., who provided two noninvasive monitors and remuneration for the coordinator of the clinical trial.
Author information
Authors and Affiliations
Contributions
Study concepts: S.C.V.K., C.M.F., G.R.M., L.M.O., M.M.F., M.C.R., F.A.M., A.K.M. Study design: S.C.V.K., C.M.F., M.C.R., F.A.M., A.K.M. Development and validation: S.C.V.K., M.C.R., F.A.M., A.K.M. Application: S.C.V.K., C.M.F. Data analysis and interpretation: S.C.V.K., C.M.F., L.M.O., M.M.F., M.C.R., F.A.M., A.K.M. Statistical analysis: C.M.F., L.M.O., M.M.F. Manuscript preparation and editing: S.C.V.K., C.M.F., L.M.O. Manuscript review: S.C.V.K., C.M.F., G.R.M., L.M.O., M.M.F., M.C.R., F.A.M., A.K.M.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Karuta, S.C.V., Folchini, C.M., Fachi, M.M. et al. Observational study of intracranial compliance analysis in neurologically healthy pediatric patients using a non-invasive device. Sci Rep 14, 19482 (2024). https://doi.org/10.1038/s41598-024-69938-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-69938-8
- Springer Nature Limited