
Abstract
Investigate the impact of remnant cholesterol (RC) levels on carotid artery intima thickness (CIT) in type 2 diabetes mellitus (T2DM) patients. From September 2021 to September 2023, a prospective multicenter study involved 158 T2DM patients. They were divided into a higher RC group (n = 80) and a lower RC group (n = 78) based on median RC levels. Additionally, 92 healthy volunteers served as the control group. CIT, carotid media thickness (CMT), and carotid intima-media thickness (CIMT) were measured. General clinical data, lab results, CIMT, CIT, and CMT differences among the three groups were compared. Multiple regression analysis explored CIT factors in T2DM patients. 1. No significant sex, age, BMI, high-density lipoprotein cholesterol (HDL-C), T2DM duration, fasting blood glucose, or glycated hemoglobin differences were found among the groups (p > 0.05). 2. CIMT and CIT were significantly higher in T2DM than the control group (p < 0.05). 3. The higher RC group had thicker CIT than the lower RC group (p < 0.05), while CIMT differences were not significant (p > 0.05). Multiple linear regression analysis showed RC as an influencing CIT factor in T2DM patients (β = 0.473, p = 0.005). CIT is significantly thicker in T2DM patients with higher RC than in those with lower RC, and RC is the influence factor of CIT, which suggests that more attention should be paid to the detection of RC in T2DM patients.
Similar content being viewed by others


Introduction
Cardiovascular disease (CVD) continues to be the primary cause of mortality among individuals with T2DM, and its incidence is steadily rising. Dyslipidemia leading to atherosclerosis (AS) is one of the significant risk factors1,2,3. The characteristics of AS-related dyslipidemia include: (1) Elevated triglyceride (TG) levels in serum, including very low-density lipoproteins (VLDLs), intermediate density lipoprotein (IDL), and their remnants, collectively referred to as triglyceride-rich lipoproteins (TRLs); (2) Reduced HDL-C concentrations; (3) Increased low-density lipoprotein cholesterol (LDL-C) levels4,5. Studies have shown that RC can participate in the formation of AS through various mechanisms, including direct accumulation in the arterial wall and increased inflammatory responses6,7,8. RC represents the cholesterol content found in triglyceride-rich remnant lipoproteins, which include VLDLs and intermediate-density lipoproteins (IDLs) in the fasting state, and these two lipoprotein types, along with chylomicron remnants, in the non-fasting state9. Similar to low-density lipoproteins (LDLs), remnant lipoproteins have the potential to infiltrate the arterial intima, leading to cholesterol accumulation and atherosclerosis development. In contrast, triglycerides alone are less likely to contribute to atherosclerosis10. Notably, research from Copenhagen study suggests that elevated remnant cholesterol levels are a stronger predictor of myocardial infarction than any other lipid particle11. Furthermore, remnant cholesterol is particularly indicative of coronary artery disease risk in individuals with normal total cholesterol levels2,12,13.
Currently, the common non-invasive method for assessing early AS is measuring CIMT14,15. However, the pathological process of AS mainly involves the intima layer, especially in the early stages. CIMT includes not only intima layer thickness but also medial layer thickness, with CMT primarily associated with age and hypertension16. Therefore, CIMT may not be the best indicator for early AS assessment, as indicated by the 2019 European Society of Cardiology guidelines, which do not recommend CIMT measurement for asymptomatic patients17. In the past, due to technological limitations, accurate measurement of CIT was challenging. With the widespread use of high-frequency probes, precise and straightforward CIT measurements have become feasible in clinical practice18,19.
This study aims to use a high-frequency ultrasound probe to measure CIT in T2DM patients and explore the influence of RC levels on CIT. This research aims to provide a reference basis for individualized interventions in early clinical management.
Materials and methods
A group of four tertiary hospitals in China, including Xiangyang No. 1 People’s Hospital, Hubei University of Medicine, The Affiliated Yixing Hospital of Jiangsu University, Xiangzhou District People’s Hospital of Xiangyang and First Affiliated Hospital of University of South China conducted this prospective study.
Study participants
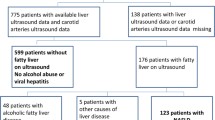
This study was a prospective investigation carried out from September 2021 to September 2023, involving an initial cohort of 653 patients with confirmed type 2 diabetes mellitus (T2DM). Following the application of exclusion criteria, a total of 158 T2DM patients were ultimately enrolled across four tertiary hospitals in China. As there is currently limited international consensus regarding the threshold for elevated RC, the author, following methods reported in previous literature19, divided the patients into two groups based on the median RC value of 0.67 mmol/L in this study. The RC higher group (> 0.67 mmol/L) consisted of 80 cases, including 43 males and 37 females, with ages ranging from 38 to 67 years (mean age: 55.30 ± 6.58 years). The RC lower group (< 0.67 mmol/L) consisted of 78 cases, including 35 males and 43 females, with ages ranging from 39 to 69 years (mean age: 55.00 ± 7.40 years). Additionally, 92 healthy volunteers, matched in terms of sex, age, and body mass index (BMI), were selected as the control group. This control group included 40 males and 52 females, with ages ranging from 41 to 64 years (mean age: 55.02 ± 5.62 years).
Inclusion criteria for participants were as follows: (1) Meeting the diagnostic criteria for T2DM according to The American Diabetes Association (2021)20 without diabetes-related complications; (2) No CIMT thickening or atherosclerotic plaques detected by ultrasound in the carotid arteries. The upper limit values of normal CIMT were defined as less than the upper 90th percentile of CIMT obtained from 24,871 healthy individuals categorized by age and gender groups21; (3) Normal blood pressure, liver function, kidney function, and thyroid function; BMI within the normal range. Exclusion criteria included: (1) Type 1 diabetes; patients with acute diabetes complications (such as diabetic ketoacidosis or hyperglycemic hyperosmolar state) or chronic complications of diabetes (such as diabetic neuropathy, diabetic retinopathy, diabetic nephropathy, diabetic lower extremity arterial disease, or diabetic foot disease)22; (2) Patients with a history of myocardial infarction, heart failure, structural heart disease, cardiomyopathy, severe arrhythmias, stroke, or prior cardiovascular surgery; (3) Patients with other autoimmune diseases or peripheral vascular diseases; (4) Pregnant women; (5) Smokers or heavy alcohol drinkers; (6) Patients who have received long-term statin therapy or other lipid-lowering medications affecting lipid metabolism; (7) Patients with a BMI less than 18.5 kg/m2 or greater than 24 kg/m2; (8) Patients with malignancies; (9) Individuals with poor image quality or those unable to complete the examination. CIT, CMT, and CIMT of carotid artery were measured according to the Standard measurement methods which reported in previous literature23 (Fig. 1).

Flow diagram of subjects among three groups.
Instruments and methods
-
1.
General Information: Recorded data on study subjects include sex, age, BMI (Body Mass Index), systolic blood pressure, diastolic blood pressure, smoking and alcohol history, duration of diabetes, complications, and the use of statin medications. Laboratory measurements comprise fasting blood glucose, hemoglobin A1c (HbA1c), total cholesterol (TC), TG/HDL-C ratio, LDL-C (Low-Density Lipoprotein Cholesterol). RC was calculated according to the formula reported in the literature5, where RC = TC − (LDL-C) − (HDL-C).
-
2.
Instrumentation: The Mindary Resona R9S color Doppler ultrasound diagnostic device was employed, with a probe model L14-3WU operating at a frequency of 11.8 MHz.
-
3.
Ultrasound Examination: The participants lay supine on the examination bed with their necks adequately exposed and connected to an electrocardiogram (ECG). Using a 11.8 MHz high-frequency probe, both sides of the carotid arteries were examined sequentially. The transverse axis was positioned at the carotid artery bifurcation, clearly displaying the carotid artery bifurcation and the region below it for 3 cm. Measurements of CIMT, CIT, and CMT were taken at 1.5 cm, 2.0 cm, and 2.5 cm below the carotid artery bifurcation, corresponding to the R-wave peak on the electrocardiogram. The average of these three measurements was calculated, as depicted in Figs. 1 and 2. Dynamic and static images were stored for a minimum of 3 cardiac cycles during each examination. CIT represents the high-echoic band of the inner wall, CMT corresponds to the low-echoic band of the middle layer, and CIMT is the vertical distance from the high-echoic anterior edge of the outer wall to the high-echoic anterior edge of the inner wall (Fig. 2). All of the above procedures were performed by two experienced senior ultrasound specialists.

The high-frequency probe displays the measurements of carotid artery intima thickness (indicated by the white arrow) and media thickness (indicated by the yellow arrow). (A) Control group; (B) high RC group.
Statistical analysis
Statistical analysis of the data was performed using SPSS 26.0 software. For continuous variables, the Shapiro–Wilk test for normality and Levene’s test for homogeneity of variances were conducted. Normally distributed continuous data were expressed as mean ± standard deviation (SD) and were compared among multiple groups using one-way ANOVA (for homogeneity of variances) and Welch's ANOVA (for inhomogeneity of variances). Post-hoc pairwise comparisons were conducted using the LSD-t test (for homogeneity of variances) and Tamhane’s T2 test (for inhomogeneity of variances). Non-normally distributed continuous data were expressed as median (interquartile range, IQR) and were compared among multiple groups using the Kruskal–Wallis H test. Post-hoc pairwise comparisons were performed using the Bonferroni method. Categorical data were presented as counts. Single-factor linear analysis was performed for laboratory and clinical variables that might influence CIT. Variables with statistically significant differences were included in the multiple-factor linear regression analysis to identify risk factors. The repeatability of measurements within and between operators was assessed using the intra-class correlation coefficient (ICC), where ICC > 0.75 indicated good repeatability, and ICC < 0.4 indicated poor repeatability. Differences were considered statistically significant when p < 0.05 on both sides.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Xiangyang No. 1 People’s Hospital, Hubei University of Medicine (XYYYE20230064). All study participants provided informed consent. All methods in this study were performed in accordance with the relevant guidelines and regulations.
Results
Comparison of general clinical data and laboratory indicators among the three groups
Age, sex, BMI, systolic blood pressure, and diastolic blood pressure showed no statistically significant differences among the three groups (p > 0.05). There was no statistically significant difference in diabetes duration between the low RC and high RC groups (p > 0.05) (Table 1). HDL-C showed no statistically significant differences among the three groups (p > 0.05). When comparing the low RC and high RC groups with the control group, significant differences were observed in TCTG, LDL-C, fasting blood glucose, HbA1c, and RC (p < 0.05). The high RC group had higher TC, TG, and RC compared to the low RC group (p < 0.05). However, there were no statistically significant differences in LDL-C, fasting blood glucose, and HbA1c between the low RC and high RC groups (p > 0.05) (Table 2).
Comparison of CIMT, CIT, and CMT parameters at three locations in the common carotid artery
There was no statistically significant difference in CIMT, CMT, and CIT between the three locations at 1.5 cm, 2.0 cm, and 2.5 cm below the bifurcation of the carotid artery (p > 0.05) (Tables 3). There was also no statistically significant difference in CIMT, CMT, and CIT between the left and right sides (p > 0.05) (Fig. 3).

Comparison of bilateral carotid artery parameters. There was no statistically significant difference in CIMT, CMT, and CIT between the left and right sides.
Comparison of carotid artery parameters among the three groups
Comparison of CMT among the three groups showed no statistically significant differences (p > 0.05). CIMT and CIT were higher in the RC high group and the RC low group compared to the control group (p < 0.05). CIT was thicker in the RC high group than the RC low group (p < 0.05). There was a tendency for CIMT to be higher in the RC high group compared to the RC low group, but the difference between the two groups was not statistically significant (p > 0.05) (Fig. 4).

Comparison of carotid artery parameters among the three groups. CIMT and CIT were higher in the RC high group and the RC low group compared to the control group (p < 0.05). CIT was thicker in the RC high group than the RC low group (p < 0.05).
Univariate and multivariate linear regression analysis of factors influencing CIT in T2DM Patients
Combining general clinical data and laboratory parameters comparisons along with previous research conclusions16, and after collinearity diagnosis, factors including sex, age, BMI, diabetes duration, fasting blood glucose, HbA1c, TC, TG, HDL-C, LDL-C, hypoglycemic agents, lipid-lowering agents, antihypertensive medications, eGFR, Uric acid levels and RC were included in the univariate linear regression analysis. It was found that TC, TG, HDL-C, hypoglycemic agents, lipid-lowering agents, antihypertensive medications and RC are influencing factors for CIT. Furthermore, after conducting a multivariate linear regression analysis, it was determined that RC remains an influencing factor for CIT (β = 0.473, p < 0.01) (Table 4).
Repeatability testing for each group
Ten randomly selected study subjects were chosen from each group, and another senior ultrasound specialist independently repeated the ultrasound measurements to conduct intra-observer and inter-observer repeatability tests. The results showed good consistency for intra-observer and inter-observer measurements of CIMT, CIT, and CMT at 1.5 cm, 2.0 cm, and 2.5 cm (Table 5).
Discussion
This study aimed to investigate the impact of RC levels on CIT in patients with T2DM and to assess whether CIT could serve as a more sensitive marker of early AS compared to CIMT. Our findings demonstrate that T2DM patients with elevated RC levels exhibit significantly thicker CIT compared to those with lower RC levels, suggesting that increased RC may be a key factor in the early development of AS. Furthermore, the data indicates that CIT thickening may precede CIMT thickening, supporting the hypothesis that RC levels provide valuable insights into the early stages of AS and that CIT measurement may offer a more sensitive assessment of early AS in T2DM patients than CIMT.
Patients with T2DM frequently present with cardiovascular risk factors, such as lipid abnormalities, making them particularly susceptible to CVD. In these patients, dyslipidemia, including elevated TG and VLDL, is common and contributes significantly to the vascular complications associated with diabetes24,25. While current clinical guidelines for lipid management in T2DM focus primarily on LDL-C, emerging evidence suggests that RC may play a significant role in residual cardiovascular risk, even when LDL-C is effectively controlled2,7,26. RC has the capacity to penetrate the arterial wall, where it is taken up by macrophages and smooth muscle cells, leading to inflammation, foam cell formation, and cholesterol accumulation within the arterial intima, ultimately contributing to atherosclerotic plaque formation27,28. Previous studies have established a link between elevated RC levels and subclinical atherosclerosis, including CIMT thickening and carotid plaque formation29,30,31.
In this study, RC levels were calculated using a formula based on commonly measured clinical parameters, including total cholesterol (TC), HDL-C, and LDL-C. Given the lack of established thresholds for elevated RC, we followed previous literature by categorizing patients into high RC (> 0.67 mmol/L) and low RC (< 0.67 mmol/L) groups based on the median RC value of 0.67 mmol/L in our T2DM cohort5. Our results indicate that patients with higher RC levels have significantly thicker CIT compared to those with lower RC levels. Given the established association between elevated RC levels and increased cardiovascular risk, the observed link between higher RC levels and increased CIT in T2DM patients suggests that CIT may serve as a valuable marker for identifying individuals at elevated risk for CVD.
It is noteworthy that our study utilized fasting RC values; however, the role of non-fasting RC in atherogenesis warrants further investigation. Non-fasting RC levels may provide additional insights into residual cardiovascular risk in T2DM patients, as RC levels fluctuate between fasting and non-fasting states, with higher levels typically observed postprandially due to the influx of TG-rich lipoproteins32. Non-fasting hyperlipidemia has been identified as a significant predictor of CVD, as demonstrated by studies such as the Copenhagen City Heart Study. This prospective 26-year follow-up study, involving 13,000 individuals from the Danish general population, revealed that non-fasting triglyceride levels exceeding 5 mmol/L predicted a 17-fold increase in the risk of myocardial infarction in women and a fivefold increase in men33. Additionally, sex-specific responses to remnant lipoproteins have been observed, with women potentially being more sensitive to the effects of RC, particularly during menopause when estrogen levels decline. Elevated TG, a precursor to RC, has been shown to disproportionately affect women, contributing to their heightened CVD risk in the context of elevated RC34. While our study did not find significant sex differences among the three groups, which helped avoid potential confounding effects, future research should consider sex-specific responses when evaluating cardiovascular risk and treatment strategies in T2DM patients.
Carotid ultrasound, a non-invasive and widely used technique, is commonly employed to assess subclinical atherosclerosis by measuring CIMT and predicting future cardiovascular events24,35,36. However, some studies have questioned the added value of CIMT in cardiovascular risk prediction when used in isolation, as CIMT may not capture the earliest morphological changes associated with AS. Early atherosclerosis is characterized by endothelial dysfunction and the migration and proliferation of vascular smooth muscle cells beneath the intima, leading to intimal thickening37. This study suggests that CIT measurement may have greater value in early AS research compared to CIMT. We observed no significant differences in CMT among the three groups, nor were there statistically significant differences in age or blood pressure, suggesting that diabetes and lipid abnormalities do not significantly impact CMT, which is primarily influenced by age and blood pressure. Both CIMT and CIT were found to be thicker in the T2DM group compared to the normal control group, with the high RC group exhibiting thicker CIT compared to the low RC group. Although there was a trend toward increased CIMT in the high RC group compared to the low RC group, the difference was not statistically significant. Furthermore, there were no significant differences in fasting blood sugar, HbA1c, diabetes duration, HDL-C, and LDL-C between the high RC and low RC groups, indicating that RC may have a greater impact on CIT than CIMT, and that CIT thickening may precede CIMT thickening. This further supports the notion that CIMT may not sensitively reflect early intimal changes during AS development.
Regression analysis identified TC, TG, HDL-C, hypoglycemic agents, lipid-lowering agents, antihypertensive medications and RC as factors influencing CIT; however, multiple-factor regression analysis revealed RC as the primary determinant of CIT in T2DM patients.
In conclusion, T2DM patients with higher RC levels exhibit greater CIT thickening compared to those with lower RC levels, suggesting that CIT thickening may occur earlier than CIMT thickening. This implies that T2DM patients with elevated RC levels may be at higher risk for developing AS and, consequently, at increased risk for CVD. Therefore, when managing lipid levels in T2DM patients without existing CVD, clinicians should consider RC levels in addition to TC, HDL-C, and LDL-C. The use of high-frequency ultrasound to assess CIT in T2DM patients can aid in understanding their early AS status, identifying high-risk individuals for cardiovascular events, and providing a basis for early intervention and personalized treatment.
This study has several limitations. First, due to the absence of international guidelines for established RC thresholds, this study, along with others, suggests that RC is an independent risk factor for cardiovascular diseases. Our findings may contribute to the future development of guidelines for RC threshold values. Second, the RC levels used in this study were derived indirectly using a calculation formula. While calculated RC is considered a practical substitute for direct RC measurement, it may overestimate or underestimate RC levels to some extent. Lastly, future research should include a larger and more diverse population of T2DM patients, conduct longitudinal studies, and directly measure RC levels for a more comprehensive analysis.
Conclusions
Our multicenter study revealed that higher RC levels in T2DM patients relate to thicker CIT, with RC as an influencing factor. Meanwhile, high-frequency ultrasound can serve as a convenient, safe, and effective means to detect carotid artery thickness in T2DM patients.
Data availability
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
References
Li, W. et al. Impact of type 2 diabetes mellitus on recurrent myocardial infarction in China. Diab. Vasc. Dis. Res. 13, 395–404 (2016).
Quispe, R. et al. Remnant cholesterol predicts cardiovascular disease beyond ldl and apob: A primary prevention study. Eur. Heart J. 42, 4324–4332 (2021).
Cui, X. et al. Scutellariae radix and coptidis rhizoma improve glucose and lipid metabolism in t2dm rats via regulation of the metabolic profiling and mapk/pi3k/akt signaling pathway. Int. J. Mol. Sci. 19, 3634 (2018).
Libby, P. The changing landscape of atherosclerosis. Nature 592, 524–533 (2021).
Sandesara, P. B. et al. The forgotten lipids: Triglycerides, remnant cholesterol, and atherosclerotic cardiovascular disease risk. Endocr. Rev. 40, 537–557 (2019).
Wadström, B. N. et al. Elevated remnant cholesterol and atherosclerotic cardiovascular disease in diabetes: A population-based prospective cohort study. Diabetologia 66, 2238–2249 (2023).
Burnett, J. R., Hooper, A. J. & Hegele, R. A. Remnant cholesterol and atherosclerotic cardiovascular disease risk. J. Am. Coll. Cardiol. 76, 2736–2739 (2020).
Ohmura, H. Contribution of remnant cholesterol to coronary atherosclerosis. J. Atheroscler. Thromb. 29, 1706–1708 (2022).
Nordestgaard, B. G., Langsted, A. & Freiberg, J. J. Nonfasting hyperlipidemia and cardiovascular disease. Curr. Drug Targets 10, 328–335 (2009).
Nakajima, K. & Tanaka, A. Atherogenic postprandial remnant lipoproteins; Vldl remnants as a causal factor in atherosclerosis. Clin. Chim. Acta 478, 200–215 (2018).
Doi, T., Langsted, A. & Nordestgaard, B. G. Elevated remnant cholesterol reclassifies risk of ischemic heart disease and myocardial infarction. J. Am. Coll. Cardiol. 79, 2383–2397 (2022).
Jørgensen, A. B. et al. Genetically elevated non-fasting triglycerides and calculated remnant cholesterol as causal risk factors for myocardial infarction. Eur. Heart J. 34, 1826–1833 (2013).
Stürzebecher, P. E., Katzmann, J. L. & Laufs, U. What is ‘remnant cholesterol’?. Eur. Heart J. 44, 1446–1448 (2023).
Takase, M. et al. Carotid intima media thickness and risk factor for atherosclerosis: Tohoku medical megabank community-based cohort study. J. Atheroscler. Thromb. 30, 1471–1482 (2023).
Tanaka, A. et al. Effect of ipragliflozin on carotid intima-media thickness in patients with type 2 diabetes: a multicenter, randomized, controlled trial. Eur. Heart J. Cardiovas. Pharmacother. 9, 165–172 (2023).
Xu, M. et al. The diagnostic value of radial and carotid intima thickness measured by high-resolution ultrasound for ischemic stroke. J. Am. Soc. Echocardiogr. 34, 72–82 (2021).
Mach, F. et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: Lipid modification to reduce cardiovascular risk. Eur. Heart J. 41(1), 111–188 (2020).
Jin, S. et al. Differential value of intima thickness in ischaemic stroke due to large-artery atherosclerosis and small-vessel occlusion. J. Cell Mol. Med. 25, 9427–9433 (2021).
Qian, S. et al. Remnant cholesterol and common carotid artery intima-media thickness in patients with ischemic stroke. Circ. Cardiovas. Imaging 14(4), 010953 (2021).
Classification and diagnosis of diabetes: standards of medical care in diabetes—2021. Diabetes Care 2021; 44: S15-S33
Engelen, L. et al. Reference intervals for common carotid intima-media thickness measured with echotracking: Relation with risk factors. Eur. Heart J. 34, 2368–2380 (2013).
Papatheodorou, K. et al. Complications of diabetes 2017. J. Diabetes Res. 2018, 3086167 (2018).
Wikstrand, J. Methodological considerations of ultrasound measurement of carotid artery intima-media thickness and lumen diameter. Clin. Physiol. Funct. Imaging 27, 341–345 (2007).
Moretti, J. et al. Normal pediatric values of carotid artery intima-media thickness measured by b-mode ultrasound and radiofrequency echo tracking respecting the consensus: A systematic review. Eur. Radiol. 34(1), 654–661 (2024).
Hamilton, M. P., Odette Gore, M. & Ayers, C. R. Adiponectin and cardiovascular risk profile in patients with type 2 diabetes mellitus: parameters associated with adiponectin complex distribution. Diabetes Vasc. Dis. Res. 3, 190–194 (2011).
Hu, X. et al. The role of remnant cholesterol beyond low-density lipoprotein cholesterol in diabetes mellitus. Cardiovasc. Diabetol. 21, 117 (2022).
Nakajima, K. & Tanaka, A. Postprandial remnant lipoproteins as targets for the prevention of atherosclerosis. Curr. Opin. Endocrinol. Diabetes Obes. 25, 108–117 (2018).
Doi, T., Langsted, A. & Nordestgaard, B. G. Lipoproteins, cholesterol, and atherosclerotic cardiovascular disease in east Asians and Europeans. J. Atheroscler. Thromb. 30, 1525–1546 (2023).
Lin, A., Nerlekar, N. & Rajagopalan, A. Remnant cholesterol and coronary atherosclerotic plaque burden assessed by computed tomography coronary angiography. Atherosclerosis 284, 24–30 (2019).
Masson, W. et al. Discordant lipid pattern and carotid atherosclerotic plaque. Importance of remnant cholesterol. Arq. Bras. Cardiol. 108(6), 526–532 (2017).
Liu, B. et al. Association of remnant cholesterol and lipid parameters with new-onset carotid plaque in Chinese population. Front. Cardiovasc. Med. 9, 903390 (2022).
Nordestgaard, B. G. Triglyceride-rich lipoproteins and atherosclerotic cardiovascular disease: New insights from epidemiology, genetics, and biology. Circ. Res. 118, 547–563 (2016).
Nordestgaard, B. G. et al. Nonfasting triglycerides and risk of myocardial infarction, ischemic heart disease, and death in men and women. JAMA 298, 299–308 (2007).
Nordestgaard, B. G. & Freiberg, J. J. Clinical relevance of non-fasting and postprandial hypertriglyceridemia and remnant cholesterol. Curr. Vasc. Pharmacol. 9, 281–286 (2011).
Wikstrand, J. Methodological considerations of ultrasound measurement of carotid artery intima–media thickness and lumen diameter. Clin. Physiol. Funct. Imaging 27, 341–345 (2007).
Spence, J. D. Assessment of atherosclerosis: should coronary calcium score and intima-media thickness be replaced by ultrasound measurement of carotid plaque burden and vessel wall volume?. Curr. Opin. Lipidol. 34, 126 (2023).
Xu, M. et al. The independent and add-on values of radial intima thickness measured by ultrasound biomicroscopy for diagnosis of coronary artery disease. Eur. Heart J. Cardiovas. Imaging 20, 889–896 (2019).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Key R&D Plan of Hubei Province (grant no: 2022BCE004), Hubei Provincial Health Commission Research Project (grant no: WJ2023F072), Key Projects in Xiangyang Medical and Health Field (grant no:2022YL26A and 2022YL52B) and Innovative Research Program of Xiangyang No.1 People's Hospital (grant no: XYY2023QT03).
Author information
Authors and Affiliations
Contributions
J.Q.Z.: conceptualization; R.L. and T.X.: methodology; L.G., C.H.C., W.L.Y., S.C. and Y.P.: data collection.; C.H.C., L.G., and T.X.: data curation; J.Q.Z. and R.L.: writing—original draft preparation; M.F. and J.F.G: writing-review and editing; A.H.Z., and X.A.S.: visualization; J.F.G. and J.Q.Z.: supervision; J.Q.Z: project administration. All authors have read and agreed to the published version of the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Liu, R., Xu, T., Gan, L. et al. Influence of remnant cholesterol levels on carotid intima thickness in type 2 diabetes patients. Sci Rep 14, 20893 (2024). https://doi.org/10.1038/s41598-024-71780-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-71780-x
- Springer Nature Limited