
Abstract
Quantitative three-dimensional gait analysis has been used to evaluate the loading at the knee (i.e. external knee adduction moment, EKAM) during level ground walking in individuals with knee osteoarthritis (OA). The magnitude of EKAM can be influenced by some factors, such as knee marker position and foot placement angles in static calibration trials, which may lead to inaccurate functional assessments and intervention planning. This study aimed to clarify the effects of knee position during static calibration trials on the evaluation of knee loading during gait in individuals with medial knee OA. Seventeen individuals with medial knee OA completed three different static standing trials; (1) knee flexed at 0 degrees, (2) knee flexed at 15 degrees, and (3) knee flexed at 30 degrees before walking at their self-selected speed. A sixteen-camera three-dimensional VICON gait analysis system with four AMTI force platforms was used to collect the EKAM, knee adduction angular impulse (KAAI), knee joint center (KJC), and other knee kinematic and kinetic variables during gait. A repeated measures ANOVA was used to investigate the differences between conditions. The 1st peak of EKAM, the 1st peak EKAM arm, KAAI, and knee extension moment were significantly increased at the 15-degree and 30-degree conditions in comparison with the 0-degree condition (P < 0.05). Additionally, the knee flexion moment and knee external rotation moment were significantly reduced at the 15-degree and 30-degree conditions in comparison with the 0-degree condition (P < 0.05). All biomechanical variables were influenced by the localization of the KJC during static calibration trials. The changes in knee position during static trials significantly affected the 1st peak EKAM, KAAI, and other knee kinematics and kinetics variables during gait. Therefore, future studies should consider keeping the participants’ knees in a consistent position during static trials between visits, as the variations in knee position could mask or exaggerate the differences between groups and interventions.
Similar content being viewed by others

Introduction
The loading at the knee during gait has been proven to be correlated with the development and progression of knee osteoarthritis (OA)1,2. However, it is difficult to measure the knee joint loading directly in vivo and it has been reported that external knee adduction moment (EKAM) is a significant predictor of the loading at the medial compartment of the knee during walking3,4, although it is only one of the predictors for knee OA3,4,5. Previous studies reported that individuals with medial knee OA demonstrated greater EKAM in comparison with age-matched healthy counterparts6,7. Earlier investigators reported that with every one unit (% Nm/Bw*Ht) increase in the EKAM, the risk of progression of medial compartment knee OA will be increased over 6 times2, moreover, increased EKAM is associated with decreased knee joint space width8. Therefore, biomechanical interventions for medial knee OA such as gait modifications9, knee bracing10, and lateral wedges11 target a reduction in EKAM.
The calculation of the EKAM is based on the standard inverse dynamics modeling, which allows accurate objective gait analyses12. However, some biomechanical factors have been proven to influence the calculation of EKAM. According to the data published in the literature, both knee marker position and foot position in the standing calibration trial could impact the peak value of EKAM during dynamic walking trials12,13,14,15. Nagano’s study indicated that forward displaced knee markers in the static trial led to reduced EKAM, increased external knee flexion moment, and knee flexion angle during walking14. Thewlis et al.13 reported that sagittal plane knee moment was significantly changed due to the shifting of static tibial coordinate system origin in the standing calibration trial. The latest study showed that the 20° toe-in angle in the standing calibration trial led to a significantly greater 1st peak of EKAM during gait in comparison with the 20° toe-out angle15.
The effects of marker position, foot placement angles, and standing posture in the static trial on lower extremities’ kinematic and kinetic patterns during gait have been explored by previous studies12,14,15,16. However, it is not yet clear how the variation of knee position in static standing trials could influence the EKAM during walking trials. One previous study reported the effects of knee flexion angle in a standing calibration trial on knee joint kinetics during dynamic walking, however, the effects of knee flexion were simulated by virtual marker displacement (in Visual 3D software), and only one participant was included in the study.
The knee position during static calibration may influence the dynamic trial, however, the knee position during static trial was according to participants assuming their comfortable position and no previous study explored the EKAM during gait by providing a clear description of knee position during static calibration trial. Therefore, this is important to studies, which aim to explore the biomechanical differences between groups and treatments, as the changes between conditions and visits may be influenced by the knee position during static calibration.
The purpose of the current study was to clarify the effects of knee position in standing calibration trials on EKAM and other knee kinematic and kinetic variables during gait. Based on one previous study, the medial translation of the static tibial coordinate system origin could increase the peaks of EKAM during gait13. Therefore, the primary hypothesis of this study was that the increase in knee flexion during static trail would increase the 1st peak of EKAM during gait. Additionally, we also expected that increased knee flexion angle during static trail would lead to greater 2nd peak of EKAM and KAAI.
Methods
Participants
All experiments were approved by the China Ethics Committee of Registering Clinical Trials (ChiECRCT-20180005). This study is in accordance with the principles of the Declaration of Helsinki. Before data collection, the purpose of this study and the procedures involved were fully explained to each participant, and written informed consent was signed before their enrollment.
Participants were recruited from the outpatients of the Chinese orthopedic department in Shuguang Hospital affiliated with the Shanghai Chinese Traditional Medicine (SCTM) University. The eligibility criteria for participation in the study were (1) aged 40 years and above; (2) diagnosed with mild-moderate medial knee OA confirmed by an X-ray (i.e., Kellgren & Lawrence grade II or III); (3) could walk independently without any assistance. Participants were excluded if they had: (1) known learning disability, (2) any other musculoskeletal diseases that influenced gait pattern; and (3) a history of lower limb surgery.
Instrumentation
Anatomic knee alignment was measured using posteroanterior radiographs. A three-dimensional motion analysis system of sixteen cameras (VICON T40s infrared motion cameras, Oxford Metrics, Oxford, UK) sampled at 100 Hz and four 400 × 600 mm force plates (OR6-6, AMTI, Watertown, USA) sampling at 1000 Hz embedded flush in the ground were used to collect the lower limb kinematics and ground reaction force (GRF) during level ground walking.
Forty-four reflective VICON markers (14 mm diameter) were attached with double-sided tape to the lower limbs of the participants which included the anterior superior iliac spine (ASIS), posterior superior iliac spine (PSIS), iliac crest, greater trochanter, medial/lateral femoral epicondyles, lateral/medial malleolus, 1st, 2nd, and 5th metatarsal heads and heel calcaneus of both limbs. The foot was assumed to be a single-segment body. These markers were used as anatomical markers to define the local coordinate system and joint center of each segment. Additional four non-collinear markers affixed on rigid cluster plates were positioned on the anterior-frontal aspect of the bilateral leg, thigh, and around the pelvis with 1.5 m elastic bandages (Fabrifoam, USA). The Calibrated Anatomical System Technique (CAST) technique was employed to determine the trajectory of these rigid segments and anatomical significance during the dynamic trials17. The marker motion data and force data were timely synchronized in the VICON motion capture system.
Sample size
The sample size for this study was calculated using the software G*Power (Version 3.1.9.6, University of Kiel, Germany), using an F-test statistical design (for EKAM) repeated measures with an effect size of 0.41 reported by a previous study15, sample power of 80%, and an alpha value of 0.05. The analysis showed that at least 15 participants would be adequate to power this study.
Procedures
The current study involved a within-subject repeated design where each participant was tested in three conditions. The three static positions used to analyze the same dynamic trials were with the knee flexed as follows: (a) 0 degrees, (b) 15 degrees, (c) 30 degrees (Fig. 1). Considering the kinematic and kinetic data may be influenced by different types of shoes, participants were asked to wear the same type of standard shoes (Huili, Shanghai Huili Footwear Co. Ltd, China) which were offered by investigators.

Knee placement over the force plate during the three static positions. (a) = 0 degrees, (b) = 15 degrees, (c) = 30 degrees.
Participants performed three static standing trials with 5 s hold in each trial and 1 min between trials according to the randomized block. During the static trial, the participants were instructed to flex their knees to the required angle. One researcher used an angle protractor angle finder ruler (HS1024C, HANS.W, China) to guide the participant to flex their knee for the selected angles during static trials (Fig. 1). The proposed knee flexion angles were randomized by using block randomization (http://www.jerrydallal.com/random/randomize.htm). The participants were instructed to walk at their self-selected speed and gait data were collected from five successful trials. The successful trial was that in which the participant walked at their usual comfortable speed, and landed the whole foot of the test limb on the force plates without changing their gait pattern18.
Data analysis
The five successful dynamic trials and three standing calibration trials captured and digitized with VICON NEXUS (VICON, Oxford Metrics PLC, UK) were exported as c3d files for further analysis with software VISUAL 3D (Version 6.01.16, C-Motion, USA). The kinematics data and analog data were filtered using the low-path Butterworth algorithm with a cutoff frequency of 6 Hz for the kinematics and 25 Hz for the analog data19. Inverse dynamics approaches were used to calculate the kinetic data. Joint moments were normalized to participants’ body mass (Nm/kg). Kinetic and kinematic values were extracted for the symptomatic side. For participants with bilateral medial knee OA, the more symptomatic side was deemed as the test limb18. The coordinate position of knee joint center (KJC) during standing calibration trials was defined as the midpoint between the medial and the lateral femoral epicondyles in global coordinate system (GCS). The coordinate position of ankle joint center (AJC) during standing calibration trials was defined as the midpoint between the lateral and the medial malleolus in GCS. The position of the KJC in relation to the AJC was calculated in the GCS. In order to allow for meaningful comparison and discussion of the moment data, the 0° condition was used as a reference13.
The primary outcome of the study was to account for the variation in the 1st peak of EKAM between the same level ground walking trials using different static standing positions. The 1st peak of EKAM was defined as the peak EKAM in the 1st half of the stance phase (from 1 to 33%).
Statistical analysis
The average of the peak value of the biomechanical outcomes from trials in 3 conditions was exported to the SPSS (Version 16.0, IBM Corporation, USA). Shaprio-Wilk tests were used to assess the normality of the selected parameters. The repeated measures ANOVA with pairwise comparison (Bonferroni adjustment) was performed to examine the difference in kinematics and kinetics data during the same walking trials. The significance was set to a 95% confidence interval (P < 0.05).
Results
Participants’ characteristics
Seventeen individuals with knee OA (10 males and 7 females) participated in this study. The radiographic OA characteristics of participants were detailed in Table 1.
The 15° and 30° conditions resulted in anterior, medial, and distal translations of the KJC in relation to the AJC during static calibration trials (P < 0.05). No significant difference in knee joint axis was found between conditions (P > 0.05, Tables 2, 3, and Fig. 2).

The coordinate position of knee joint center (KJC) based on different knee flexion angle during static trials: α) 0°condition, β) 15°condition, γ) 30°condition. Note that difference in the coordinate position of KJC in relation to ankle joint center (AJC) was based on the different knee flexion angle during static trials, the 15° and 30° conditions resulted in an anterior, medial and distal translation. The Z-axis (blue) was defined by the vector from KJC to Hip joint center (HJC) (direction from distal to proximal, proximal as positive), the medial–lateral axis (red) (X-axis) was defined by the vector from KJC to medial femur epicondyles (direction from left to right, right as positive), the anterior–posterior axis (green) (Y-axis) was determined by the cross-product between the Z-axis and the X-axis (direction from posterior to anterior, anterior as positive).
The 1st peak of EKAM during gait was altered with the static standing knee position; where 15° and 30° were significantly greater than 0° (P < 0.05) with a 3.89% and a 5.97% increase. No significant difference between all conditions in 2nd peak EKAM was found (P > 0.05). In comparison with 0°, both 15° and 30° showed significantly increased 1st peak of EKAM arm (P < 0.05). No significant difference in 2nd EKAM arm was found between conditions (P > 0.05). Compared with 0°, both 15° and 30° showed significant increases in KAAI (P < 0.05). No significant difference in 1st peak of EKAM, 1st peak EKAM arm, and KAAI between 15° and 30° conditions was found (P > 0.05) (Table 4, Fig. 3).

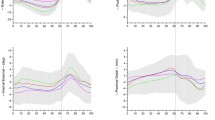
The averaged (N = 17) external knee adduction moment (EKAM) in the three conditions (the solid line represented 0 degrees, the dot dash line represented 15 degrees, the dash line represented 30 degrees).
Other knee kinetics and kinematics variables that showed significant differences between conditions were sagittal plane knee angle at initial contact, sagittal plane knee angle at early stance, peak knee flexion angle in the gait cycle (GC), peak knee internal rotation angle in GC, peak knee external rotation angle in GC, peak knee flexion moment, and peak knee extension moment (P < 0.05). Compared with 30°, both 0° and 15° showed significant increases in sagittal plane knee angle at initial contact, sagittal plane knee angle at early stance, peak knee flexion angle in GC, and decreased peak knee internal rotation angle in GC (P < 0.05), however, no significant difference between 0° and 15° was found (P > 0.05). Compared with 30°, both 0° and 15° showed significantly greater peak knee external rotation angle in GC (P < 0.05). Knee flexion moment decreased with an increased knee flexion angle during static trials whilst knee extension moment and peak knee external rotation angle increased (P < 0.05) (Table 4).
Discussion
Previous studies demonstrated that the shifting of the location of knee markers in the standing calibration trials could affect the knee kinetics and kinematics variables in healthy13,14, however, no study reported the impact of performing different static knee positions on the knee loading and the other kinematics and kinetics variables. The current study aimed to investigate how different knee positions assumed in static calibration trials could affect 1st peak of EKAM, 2nd peak of EKAM, KAAI, and other knee kinematic and kinetic variables during level ground walking in individuals with medial knee OA.
The results demonstrated that when adopting knee flexion from 0° to 30° static positions, each 15° increment in knee flexion angle during static produced 1.54°-2.16° decrements in knee flexion during gait. This finding was in accordance with the findings of one previous study, which reported the loss of knee flexion during gait was 1.33° with each 15° increment in knee flexion angle during static20. This could be explained by the anterior translation of the KJC caused by the increased knee flexion angle (i.e., 15° and 30° conditions) during static trials. The normal vertical alignment of the limb (“zero” position) should be a straight line from the hip joint center, through the femoral epicondyle, to the lateral malleolus20. When the subject’s limb cannot be positioned in normal alignment, the deviation is identified as an abnormal zero position. Murray’s study indicated that hyperextension of the knee during static trials would lead to increased knee flexion during gait20,21. Therefore, the reduction in knee flexion during gait was a compensatory change due to the increased knee flexion angle during static trials.
The different knee flexion angle positions during the static trial had effects on the 1st peak of EKAM during gait. Moreover, the increase in 1st peak EKAM was associated with the increase in KAAI during gait. The increase in the 1st peak of EKAM and KAAI could explained by the increase in the EKAM arm, as the magnitude of EKAM is mainly determined by the GRF and the EKAM arm4. Both the 15° and 30° conditions showed medial translation of the KJC during static trials, indicating that the perpendicular distance between the GRF and KJC was reduced. However, the medial translation of the KJC during static trials would lead to opposite effects on the 1st peak of EKAM during gait due to the compensatory effect. One previous study demonstrated that the medial translation of the KJC caused by knee marker placement during static trials led to an increase in the 1st peak of EKAM during gait13. Althomali and colleagues also reported that medial translation of the KJC due to a 20-degree toe-in foot placement during static trials significantly increased the 1st peak of EKAM during gait15. Consequently, the static knee position should be taken into account when measuring the EKAM and KAAI during walking.
In comparison with the 0° condition, the 15° and 30° conditions increased the 1st peak of EKAM by 4.38% and 5.97%, respectively. One previous study showed that significant improvements in pain were observed only in knee OA patients who, in a gait laboratory using lateral wedges, exhibited at least a 2% reduction in the 1st peak of EKAM11. Therefore, changes in knee position during static calibration might lead to inaccurate clinical interpretations and, consequently, inappropriate clinical strategies.
The decrease in knee flexion moment and the increase in knee extension moment were observed alongside the reduction in knee flexion angle during gait. These findings were consistent with a previous study that reported a positive correlation between the peak knee flexion moment and the knee flexion angle during stance22. The decrease in knee flexion moment and the increase in knee extension moment could be explained by the reduced knee flexion angle during gait, which is caused by the anterior translation of the KJC during static trials. Thewlis’s study also reported significant changes in knee flexion and extension moments during gait by anterior translation of the KJC in relation to the AJC during static trials, however, no significant change in 1st peak of EKAM was found13. This discrepancy might be due to the differences in participant characteristics between the studies, as the participants in the current study were individuals with knee OA.
The impact of knee position during static trial is likely either further exaggerated or decrease the 1st peak of EKAM and knee flexion moment further between assessments in individuals with knee OA which could lead to inappropriate functional assessment and intervention planning. Therefore, the position of the knee during static trials is important for investigators to obtain accurate knee moments from quantitative gait analysis in individuals with knee OA.
The limitation of the study
Our study had some limitations. Firstly, a previous study indicated that variations in the KJC had a much greater effect on the 1st peak knee flexion moment at slower speeds23. However, the current study did not investigate the effects of knee position on the EKAM at different walking speeds. Therefore, future studies need to explore the effects of knee position on EKAM at varying walking speeds, as individuals with more severe knee OA have significantly slower walking speeds than those with less severe knee OA24. Secondly, the foot position during static trial calibration has been proven to affect the 1st peak of EKAM during level ground walking15. However, we did not restrict foot position (e.g., 0° positions) during static trials, which may also exaggerate or decrease the knee moment during gait.
Conclusion
The results of the current study confirmed that changes in knee position during static trials significantly affected the 1st peak EKAM, KAAI, knee flexion moment, knee extension moment, peak knee internal rotation angle, peak knee external rotation angle, knee flexion angle at initial contact, and peak knee flexion angle in early stance and GC. This implies that the static knee position is one of the key factors that could affect the calculation of the knee loading during level ground walking in individuals with knee OA. Therefore, it is important for subjects to keep the knee in a consistent position during static trials in a repeat measure design or randomized clinical trials as the variations in knee position between visits could mask or exaggerate the differences between groups and interventions.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Ishii, Y. et al. Knee adduction moment is correlated with the increase in medial meniscus extrusion by dynamic ultrasound in knee osteoarthritis. Knee38, 82–90. https://doi.org/10.1016/j.knee.2022.07.011 (2022).
Miyazaki, T. et al. Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann. Rheum. Dis.61, 617–622 (2002).
Thorp, L. E. et al. Relationship between pain and medial knee joint loading in mild radiographic knee osteoarthritis. Arthritis Rheum.57, 1254–1260. https://doi.org/10.1002/art.22991 (2007).
Trepczynski, A. et al. Modulation of the relationship between external knee adduction moments and medial joint contact forces across subjects and activities. Arthritis Rheumatol.66, 1218–1227. https://doi.org/10.1002/art.38374 (2014).
Manal, K. et al. A more informed evaluation of medial compartment loading: The combined use of the knee adduction and flexor moments. Osteoarthr. Cartil.23, 1107 (2015).
Amin, S. et al. Knee adduction moment and development of chronic knee pain in elders. Arthritis Rheum.51, 371–376. https://doi.org/10.1002/art.20396 (2004).
Kim, W. Y. et al. A new biomechanical model for the functional assessment of knee osteoarthritis. The Knee11, 225–231. https://doi.org/10.1016/S0968-0160(03)00068-1 (2004).
Sharma, L. et al. Knee adduction moment, serum hyaluronan level, and disease severity in medial tibiofemoral osteoarthritis. Arthritis Rheum.41, 1233–1240. https://doi.org/10.1002/1529-0131(199807)41:7%3c1233::AID-ART14%3e3.0.CO;2-L (1998).
Wang, S. et al. Effects of foot progression angle adjustment on external knee adduction moment and knee adduction angular impulse during stair ascent and descent. Hum. Mov. Sci.64, 213–220. https://doi.org/10.1016/j.humov.2019.02.004 (2019).
Moyer, R. F. et al. Biomechanical effects of valgus knee bracing: A systematic review and meta-analysis. Osteoarthr. Cartil.23, 178–188. https://doi.org/10.1016/j.joca.2014.11.018 (2015).
Felson, D. T. et al. The efficacy of a lateral wedge insole for painful medial knee osteoarthritis after prescreening: A randomized clinical trial. Arthritis Rheumatol.71, 908–915. https://doi.org/10.1002/art.40808 (2019).
Szczerbik, E. & Kalinowska, M. The influence of knee marker placement error on evaluation of gait kinematic parameters. Acta Bioeng. Biomech.13, 43–46 (2011).
Thewlis, D. J., Richards, D. & Bower, J. Discrepancies in static knee marker placement based on different anatomical landmarks produce effects greater than previously simulated. J. Appl. Biomech.24, 185–190 (2008).
Nagano, H. et al. Modelling knee flexion effects on joint power absorption and adduction moment. The Knee22, 490–493. https://doi.org/10.1016/j.knee.2015.06.016 (2015).
Althomali, O. W. et al. The effect of foot position during static calibration trials on knee kinematic and kinetics during walking. Gait Posture99, 133–138. https://doi.org/10.1016/j.gaitpost.2022.11.007 (2023).
McMulkin, M. L. & Gordon, A. B. The effect of static standing posture on dynamic walking kinematics: Comparison of a thigh wand versus a patella marker. Gait Posture30, 375–378. https://doi.org/10.1016/j.gaitpost.2009.06.010 (2009).
Cappozzo, A. et al. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. (Bristol, Avon)10, 171–178. https://doi.org/10.1016/0268-0033(95)91394-t (1995).
Hinman, R. S. et al. Lateral wedge insoles for medial knee osteoarthritis: Effects on lower limb frontal plane biomechanics. Clin. Biomech. (Bristol, Avon)27, 27–33. https://doi.org/10.1016/j.clinbiomech.2011.07.010 (2012).
Jones, R. K. et al. The biomechanical effects of a new design of lateral wedge insole on the knee and ankle during walking. Hum. Mov. Sci.32, 596–604 (2013).
Perry, J. & Burnfield, J. Gait Analysis: Normal and Pathological Function (SLACK Incorporated, 1992).
Murray, M. P., Drought, A. B. & Kory, R. C. Walking patterns of normal men. J. Bone Joint Surg.46, 335–360 (1964).
Fukaya, T., Mutsuzaki, H. & Mori, K. Relations between external moment and movement of the knee joint during the stance phase in patients with severe knee osteoarthritis. J. Orthop.16, 101–104. https://doi.org/10.1016/j.jor.2018.12.014 (2019).
Holden, J. P. & Stanhope, S. J. The effect of variation in knee center location estimates on net knee joint moments. Gait Posture7, 1–6. https://doi.org/10.1016/s0966-6362(97)00026-x (1998).
Astephen, J. L. et al. Biomechanical changes at the hip, knee, and ankle joints during gait are associated with knee osteoarthritis severity. J. Orthop. Res. off. Publ. Orthop. Res. Soc.26, 332–341. https://doi.org/10.1002/jor.20496 (2008).
Acknowledgements
This study was supported by the National Natural Science Foundation of China (No. 81973875, 81503592, 81774342), Shanghai chronic musculoskeletal disease clinical medical research center (20mc1920600), financially supported by Program for Shanghai High-Level Local University Innovation Team (SZY20220315), and Shanghai Key Clinical Specialty "Traditional Chinese Medicine Orthopaedic Traumatology" (shslczdzk03901).
Funding
Funding was provided by National Natural Science Foundation of China (Grant no. 81973875,81774342), Shanghai chronic musculoskeletal disease clinical medical research center (Grant no. 20mc1920600), financially supported by Program for Shanghai High-Level Local University Innovation Team (Grant no. SZY20220315), Shanghai Key Clinical Specialty "Traditional Chinese Medicine Orthopaedic Traumatology" (Grant no. shslczdzk03901).
Author information
Authors and Affiliations
Contributions
Min Zhang conceived the original study idea and drafted the final manuscript. Jian Pan, and Jiehang Lu collected and processed the experimental data (related to the biomechanical measurements). Bo Chen recruited participants for this study. Hongsheng Zhan made substantial revisions to the final manuscript. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors have no conflict of interest regarding any of the material in the manuscript and meet the criteria for authorship as defined as submission guidelines.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Zhang, M., Lu, J., Chen, B. et al. The influence of knee position during static calibration trials on evaluation of knee loading during gait in individual with medial knee osteoarthritis. Sci Rep 14, 21692 (2024). https://doi.org/10.1038/s41598-024-72934-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-72934-7
- Springer Nature Limited