
Abstract
Due to rapid technological advancements, remote patient monitoring (RPM) technology has gained traction in recent years. While the effects of specific RPM interventions are known, few published reviews examine RPM in the context of care transitions from an inpatient hospital setting to a home environment. In this systematic review, we addressed this gap by examining the impacts of RPM interventions on patient safety, adherence, clinical and quality of life outcomes and cost-related outcomes during care transition from inpatient care to a home setting. We searched five academic databases (PubMed, CINAHL, PsycINFO, Embase and SCOPUS), screened 2606 articles, and included 29 studies from 16 countries. These studies examined seven types of RPM interventions (communication tools, computer-based systems, smartphone applications, web portals, augmented clinical devices with monitoring capabilities, wearables and standard clinical tools for intermittent monitoring). RPM interventions demonstrated positive outcomes in patient safety and adherence. RPM interventions also improved patients’ mobility and functional statuses, but the impact on other clinical and quality-of-life measures, such as physical and mental health symptoms, remains inconclusive. In terms of cost-related outcomes, there was a clear downward trend in the risks of hospital admission/readmission, length of stay, number of outpatient visits and non-hospitalisation costs. Future research should explore whether incorporating intervention components with a strong human element alongside the deployment of technology enhances the effectiveness of RPM. The review highlights the need for more economic evaluations and implementation studies that shed light on the facilitators and barriers to adopting RPM interventions in different care settings.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Introduction
Remote patient monitoring (RPM) technologies are gaining traction in healthcare due to the acceleration of technology development and application of artificial intelligence (AI)1. The global RPM market is projected to expand rapidly in the next few years, with a compound annual growth rate of 18.9% projected between 2021 and 20282. In brief, RPM interventions involve the use of connected electronic tools to record personal health data outside the traditional care setting so that they can be reviewed by a provider at a different location3. There are many core technologies and architectures that enable RPM interventions, which include various kinds of sensors, internet of things (IoT) devices, networking, data centres, cloud computing and blockchain technologies1,4. More recently, the rise of Industry 4.0 has also seen the widespread application of AI, enabling advanced data analytics such as predicting when a patient’s health is declining4.
RPM interventions have been widely adopted across various patient groups and clinical settings, according to the literature. At the earliest life stage, RPM interventions have been deployed to monitor vital signs such as temperature, pulse rate and pulse oxygen concentration of ill or premature newborn infants that require constant monitoring in the neonatology ward to prevent subsequent adverse events5. Towards the end of the life cycle, advances in digital health technologies in geriatric care have given rise to a variety of physical and chemical wearable sensors, wearable sensing platforms and various smart home digital systems to monitor the health of older people while enabling them to maintain a high level of independence6. For adults, various RPM interventions have been designed to monitor patients with various physical and mental health challenges such as chronic obstructive pulmonary disease (COPD)7,8, hip osteoarthritis and arthroplasties9, cancers10, chronic diseases such as diabetes11, those who undergo home dialysis12, neuro-psychiatric conditions13 and more recently, COVID-19 patients who were discharged home from the hospital14. Despite being perceived as promising to facilitate care transition from hospital to home, evidence of RPM interventions deployed on patients with acute conditions such as cardiovascular diseases are mixed in terms of the ability of the interventions to reduce the risk of hospitalisations15,16. This is likely due to heterogeneity in the stages of the disease as well as the severity of the conditions examined. In terms of subjective outcomes, RPM interventions have demonstrated positive outcomes with studies reporting enhanced patient engagement and patient experience10,11. RPM interventions have also shown promise in reduction in the number of hospitalisation days8,10, potentially resulting in health cost reduction in the longer run.
Although a growing body of evidence evaluating various RPM interventions has emerged in recent years, the evidence is highly heterogeneous, resulting in the lack of conclusive insights from the consolidation of the evidence. For instance, a meta-analysis conducted by Noah et al.17 synthesised 27 randomised controlled trials (RCTs) on wearable biosensors but found limited clinical impacts compared to usual care. A more focused review by Iqbal et al.18 examining the impacts of digital sensor alerting systems in remote monitoring reported 9.6% mean decrease in hospitalisation and 3% mean decrease in all-cause mortality. In terms of the cost-effectiveness of RPM interventions, a meta-analysis on RCTs conducted by Klersy et al.19 assessing the cost-effectiveness and the cost-utility of RPM on multidisciplinary heart failure management when compared with the usual care approach found significantly lower number of hospitalisations among those who received RPM interventions but no difference in length-of-stay as compared to those who received standard care. The meta-analysis highlighted that the lack of prospectively and uniformly collected economic data was hindering more solid claims to be made. As such, a systematic review and meta-analysis to examine a broader scope of safety, clinical outcomes, quality of life and cost-related outcomes of various RPM interventions is timely in lieu of the burgeoning studies evaluating technology-based remote monitoring on various patient groups that emerged in the past decade. In addition, the high-cost burden due to prolonged admission in the hospital setting and the need for care integration also propel the use of RPM interventions to facilitate care transition from a hospital environment to a home setting. To the best of our knowledge, there is hardly any published review that examined the impacts of RPM interventions that aimed to facilitate care transition from a hospital environment to a home setting to date. This model of care is increasingly lauded as a virtual care model that is more efficient, sustainable and desirable20. During the COVID-19 pandemic, many health systems around the world were overwhelmed with high occupancy rates in hospitals, especially at the early stage when the world was still fraught with many unknowns and uncertainties with regard to the pathogenesis of the COVID-19 virus. The pandemic has forced health systems around the world to innovate by leveraging RPM interventions to enable continuity in care provision. As the world moves on from the pandemic, reinventing care provision using RPM interventions would require more understanding of their applications and impacts. This review thus aims to address these knowledge gaps. To this end, we pose the following review question: What are the impacts of RPM interventions on clinical outcomes, patient safety, quality of life and cost-related outcomes during the immediate care transition period from hospital to home?
Results
Contexts and characteristics of the included studies
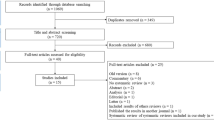
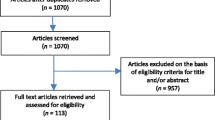
This review identified a total of 30 studies that fulfilled the inclusion criteria and were included in the final synthesis. Figure 1 shows the preferred reporting items for systematic reviews and meta-analyses (PRISMA) flowchart that documents the details of evidence search processes at various stages.

The diagram depicts the evidence search, the number of included and excluded studies, and the reasons for article exclusion.
A total of 29 RCTs were included in this review. Studies were conducted in Australia (n = 1), Austria (n = 1), Brazil (n = 1), Canada (n = 1), Denmark (n = 1), France (n = 1), Pakistan (n = 1), South Korea (n = 1), Spain (n = 1), Thailand (n = 1), Germany (n = 2), Italy (n = 2), The Netherlands (n = 2), China (n = 3) and the US (n = 8). Two studies are multi-country, multi-centre studies, with one of them covering France, Italy and Spain and the other one covering the Czech Republic and Germany.
In terms of the population of interest, nearly half of the studies (13 studies) reported the effects of RPM interventions on patients with coronary diseases, including chronic heart failure, acute coronary disease, patients with an implantable cardioverter-defibrillator (ICD) and congestive heart failure. The next most common population examined was patients with lung conditions such as chronic obstructive pulmonary disease (COPD) and lung transplant (four studies). There were three studies on post-surgical patients, two studies examining infants with low birth weight, two studies examining patients with COVID-19 complications, two studies examining patients diagnosed with cancer, one study examining postpartum women, one study examining patients with affective, neurotic and/or behavioural disorder and one study examining internal medicine patients with a wide range of acute, subacute and chronic diseases of different grades and severities (Table 1).
Risk of bias assessment
The critical appraisal exercise using the RoB 2 appraisal tool identified nine studies (31.03%) as having overall low risk of bias,11 studies (37.93%) as having overall medium risk of bias and nine studies (31.03%) as having overall high risk of bias. Figure 2 displays the graphical visualisation of the overall risk of bias as well as the risk of bias in each category.

We assessed the risk of bias using the revised Cochrane risk-of-bias tool for randomised trials (RoB 2). The tool assesses bias in five domains: risk of bias arising from the randomisation process, risk of bias due to deviations from the intended interventions, risk of bias due to missing outcome data, risk of bias in the measurement of the outcome, risk of bias in the selection of the reported result.
RPM technologies deployed
We identified seven types of technologies based on their functions, ranging from standard communication tools to computer-based systems, to smartphone applications, to web portal, to augmented clinical devices with monitoring capabilities, to wearables and other clinical tools used to assist remote monitoring. Table 2 provides a summary of the technology types with detailed descriptions and the study examples.
Specifically, communication tools refer to information technologies mainly used to assist communication among different parties in different locations. Computer-based systems refer to information systems installed and used on specific computers. Smartphone-based systems are information systems installed and used on specific mobile phones. Websites are webpages accessible from various technological devices through an internet connection. Augmented clinical devices with monitoring capabilities refer to conventional clinical devices that are substantiated with monitoring functions. Wearables for continuous vital signs and activity monitoring capture continuous monitoring data of vital signs and patient activities. Clinical tools for intermittent monitoring are devices that capture episodic patient data.
In terms of technology purpose and function, we identified two general purposes: (i) delivery of existing clinical services remotely, and (ii) delivery of new clinical services. For the first general purpose, we identified seven studies that can be further subdivided into three sub-groups based on their detailed purposes, which include (i) replacing existing monitoring technology with a new one, (ii) replacing in-person follow-up services with remote monitoring, and (iii) replacing inpatient monitoring to enable earlier transition to home or other clinical institutions. For the second general purpose, we identified 20 studies and further classified them into four sub-groups based on their detailed purposes. These include (i) supplementing existing interventions with remote monitoring, (ii) providing new care services which include personalised care, self-management and patient education, (iii) improving patient adherence and patient engagement, and (iv) reducing information asymmetry for caregivers (see Table 3).
In our review of RPM technologies, we identified three primary monitoring modes: alert-driven, scheduled, and unscheduled. In alert-driven mode, clinical staff respond to patients following system alerts or proactive patient contact. Contact initiation in alert-driven mode depends on who receives the alert, be it clinical staff or patients. We found 14 studies employing an alert-driven monitoring mode. Of these, 12 studies used system alerts to notify clinical staff of abnormal conditions21,22,23,24,25,26,27,28,29,30,31,32, while two studies sent alerts only to the patients25,33. For the technology functioning based on scheduled monitoring mode, the user with the monitor role (usually the clinical staff or family caregivers) played proactive roles: they would adhere to schedules to regularly check patients’ conditions. We identified 11 studies adopting a scheduled monitoring mode34,35,36,37,38,39,40,41,42,43,44. On the other hand, four studies adopted unscheduled monitoring mode by performing ad-hoc checks on the monitoring data to detect clinical anomalies45,46,47,48.
Impacts of the RPM interventions on patient safety
Three studies documented the impacts of various RPM interventions on patient safety—operationalised as major complication reduction and/or adverse event such as mortality—as the primary outcomes.
Major complication reduction and adverse event
Pietratonio et al.30 demonstrated that the intervention arm patients who were mostly discharged from the internal medicine ward with a wide range of acute, subacute and chronic diseases of different grades and severities reported fewer major complications, which include rehospitalisation, than control arm patients. Regarding mortality, Scherr et al.21 observed lower death risks in telemonitored patients, and Wintrich et al.31 noted reduced cardiovascular death risks in chronic heart failure patients using alert-enabled remote monitoring.
Impacts of the RPM interventions on adherence
In terms of adherence, four studies examined the impacts of RPM interventions on adherence towards medication or lifestyle prescriptions, while one study examined the impacts on the odds of self-monitoring.
Adherence to medication or lifestyle prescriptions
Blasco et al.35 reported a higher and statistically significant rate of adherence to the exercise routine prescribed to moderate to severe chronic obstructive pulmonary disease (COPD) patients while Geramita et al.27 reported statistically significant lower risk to nonadherence to lifestyle requirements for patients who were enroled in RPM intervention as opposed to patients underwent usual care. As for medication adherence, Gallagher et al.38 found no significant difference between heart patients who were enroled for RPM intervention as compared to patients who were on passive monitoring. On the other hand, Riegel et al.47 found a significant decline in the median adherence towards medication among the control group patients who were not monitored as compared to patients who were monitored with electronic monitoring pill bottles using a medication event monitoring system.
Odds of self-monitoring
When examining patients who underwent lung transplant and were discharged with a tracking technology device, DeVito Debbs et al.49 reported significantly higher odds of self-monitoring among them when comparing to patients who were not discharged with the same remote monitoring device.
Impacts of the RPM Interventions on Clinical Outcomes and Quality of Life
14 studies reported the impacts of RPM interventions on clinical and quality of life outcomes which include mobility function or functional statuses29,39,40,41,42,43,44 occurrence of various physical and mental symptoms26, breathing outcome45, breastfeeding outcome24, various postoperative symptoms and sensations41 and general psychopathological symptom36 as well as duration until return to work25.
Mobility/functional statuses
Seven studies reported mobility or functional status as its primary outcome for RPM interventions. Bernocchi et al.39 reported better mobility outcomes after four months in the form of longer walking distances for rehabilitation patients who were remotely monitored as compared to those who were not remotely monitored. Both Fang et al.40 and Hisam et al.43 similarly reported significantly better mobility outcomes (measured using the 6-min walking test, SF-36 and SF-12) for coronary heart disease patients who were monitored in real-time with a smartphone app as compared to those who were placed on usual care. Moreover, Fang et al.40 also included active and rapid feedback between patients and clinicians as an intervention component alongside the remote monitoring technology. In examining stroke patients monitored with a smartphone application known as WeChat, Li et al.42 nevertheless reported no significant change in their functional statuses, measured using the modified Barthel index, when compared with patients who were not remotely monitored using the application. On the other hand, Li et al.44 reported better and significant mobility and functional status outcomes among COVID-19 patients with complaints of dyspnoea who were discharged home and monitored using a combination of smartphone application and WeChat voice call as compared to those who were discharged but not remotely monitored using the same technologies. Likewise, Somsiri et al.29 reported significantly better functional statuses and increased satisfaction with care scores among patients diagnosed with heart failure and monitored with a smartphone application as compared to those who underwent usual care. DeSilva Schultz et al.41 investigated the effects of telehealth in monitoring post-surgical patients who were discharged from the hospital and reported a significantly higher level of independence (measured using a binary question as to whether they need help to complete self-care) among them as compared to patients who were not monitored using telehealth.
Occurrence of various physical and mental symptoms
Six studies examined the occurrence of a multitude of physical and mental health symptoms to reflect quality of life outcomes and the evidence is mixed. Ahmed et al.24 reported no significant difference in breastfeeding outcomes among women with postpartum depression who were remotely monitored as compared to those who were not remotely monitored. However, de Silva Schultz et al.41 also reported a significantly lower incidence of symptom occurrence, such as loss of appetite among post-surgical patients who were monitored with telehealth as compared to patients who were placed on usual care. Ebert et al.36 similarly reported significantly lesser symptom deterioration among patients with affective, neurotic and/or behavioural disorders randomised to receive an internet-based maintenance treatment programme, online patient education and online support group as compared to patients who were not supported with the same internet-based programmes. Graetz et al.26 also reported a slightly increased but insignificant mental health score among post-surgical patients discharged with a self-monitoring application when compared with patients discharged without a self-monitoring application. In a similar vein, Soh et al.45 also reported better but insignificant breathing outcomes (measured using incentive spirometer index) among post-surgical patients placed on remote monitoring technology (Go-breath application and dashboard) as opposed to patients who were not remotely monitored.
Duration until return to work
Only one study reported duration until return to work to reflect quality of life. Based on a study conducted in The Netherlands, Bouwsma et al.25 reported that women who went through hysterectomy and were placed on follow-up using a web portal after discharge were able to return to work significantly faster than those who were not placed on the same remote monitoring technology.
Impacts of the RPM Interventions on cost-related outcomes
A total of 12 studies investigated the impacts of RPM interventions on cost-related outcomes. Among them, 11 studies examined cost-related outcomes in terms of either frequency or risk of hospital admission/readmission22,31,32,33,34,47,48, length of stay21, number of subsequent outpatient visits23,28 and number of hospital-free days46. Only one study operationalised cost-related outcomes as hospitalisation/non-hospitalisation costs37.
Hospital admission/readmission outcomes and length of stay
Boriani et al.22 showed that in-hospital visits were reduced in the intervention group monitored with a remote monitoring device as compared to the control group patients, and the median delay from device-detected events to clinical decisions made was considerably shorter in the intervention group patients when comparing with the control group. Likewise, Indraratna et al.32 also reported that the risk of 30-day readmission was lower among patients who were remotely monitored. Nevertheless, Jakobsen et al.33 did not report a significant difference in the risk of 100-day readmission among patients who were remotely monitored and not remotely monitored. Riegel et al.47 showed that even though the incidence of rehospitalisation among the intervention group patients monitored with technology was lower, it was not statistically significant when compared with control group patients. Scherr et al.21 also documented a significantly shorter length of stay, while Weintraub et al.34 and Wintrich et al.31 reported a lower risk of hospitalisations among patients monitored with technology as compared to patients who were not monitored with technology. Gray et al.48, on the other hand, reported that infants in the intervention groups monitored using teleconferencing technology experienced shorter lengths of stay than the infants in the control group that received usual care, though the result is insignificant.
Number of outpatient/follow-up visits
Higgins et al.28 reported significantly higher post-surgical outpatient visits among patients who were not remotely monitored as compared to patients who were monitored remotely. Likewise, Hindricks et al.23 reported that the number of unscheduled visits was significantly lower among patients who were remotely monitored as compared to patients who were not remotely monitored. In addition, the total number of follow-up visits (both scheduled and unscheduled) was significantly lower among the remotely monitored patient group as well.
Number of hospital-free days
van Goor et al.46 examined the impact of remote monitoring using a mobile application on patients infected with COVID-19 who were discharged home and found that the mean difference in the number of hospital-free days during the 30 days following randomisation was only 1.7 days less than patients who received standard care. The result was insignificant. However, the index hospital length of stay was 1.6 days shorter (p < 0.001) in the intervention group when compared to the control group.
Hospitalisation/non-hospitalisation costs
Guédon-Moreau et al.37 examined the cost impacts by looking at both the hospitalisation and non-hospitalisation costs per patient-year on patients with very low birthweight infants over a period of 27 months. They found that the mean non-hospitalisation costs per patient-year were significantly lower among patients who were remotely monitored as compared to those who received standard care. In terms of hospitalisation costs, there was no significant difference between patients who were remotely monitored as compared to those who received standard care even though patients who were remotely monitored incurred a slightly lower hospitalisation cost.
Table 4 summarises the results of the impacts of RPM interventions on patient safety, care continuity, quality of life and cost outcomes for all 29 included studies.
Discussion
This review encompasses thirty RCTs investigating seven primary RPM interventions leveraging various technologies, including communication tools, computer-based systems, smartphone apps, web portals, augmented devices, wearables, and standard intermittent monitoring tools. These technologies aim to deliver remote services, supplement on-site interventions, offer personalised care, enhance patient adherence and education, and reduce caregivers’ information asymmetry. Overall, RPM interventions have positively impacted patient safety, evidenced by reduced major complications and adverse events. Outcomes on adherence are rather encouraging as well, with RPM interventions showing an overall upward trend in patient adherence to medication and lifestyle prescription as well as the odds of self-monitoring. In terms of clinical outcomes and quality of life, RPM interventions have shown improvements in the mobility and functional statuses of patients in general. However, the evidence on the risk of various physical and mental symptoms is somewhat mixed. For cost-related outcomes, reduced risks of hospital admission/readmission, length of stay, number of subsequent follow-ups and non-hospitalisation costs are clearly observed. In terms of monitoring mode, there is no stark difference between technologies that utilise alert-driven monitoring mode versus scheduled and unscheduled monitoring modes. Due to the heterogeneity of the interventions and the comparator groups, it is beyond the scope of this review to establish the extent to which other intervention components with strong human elements incorporated alongside the deployment of the technology, such as active phone calls from the healthcare workers, patient training and education and online support groups influence and/or enhance the effects of the RPM interventions. The presence of human elements in terms of provider follow-up, skills training and patient education can affect the overall effects of technological interventions. Follow-up inquiries on the human intervention weaved into the RPM intervention deployment would be pertinent to tease out how much they are augmenting or diminishing the impacts of the whole intervention.
One of the major strengths of this review is the identification and mapping of a wide range of RPM technologies. We searched five academic databases, consulted an information specialist to fine-tune our search strategy, included 30 RCTs and examined a wide range of impacts, from patient safety outcomes to service quality outcomes, to cost outcomes. These evaluations were conducted in 16 countries covering health systems with different developmental stages, signalling the burgeoning pace and relevance of the RPM intervention to deliver effective healthcare and bridge health system gaps, especially in light of the COVID-19 pandemic.
However, the diversity in patient populations, intervention durations, and components across these studies complicate drawing definitive conclusions about RPM’s effects on specific diseases. Also, heterogeneity of the outcome measures derived from this review rule out the possibility of a meta-analysis to be undertaken. It is important to acknowledge that RPM intervention is constantly evolving, and it is possible that we may not have included all pertinent terms in our search process. While we have included respective concepts for ‘remote’ and ‘monitoring’, our search may not have captured the full gamut of the ‘remote monitoring’ concept.
There are a multitude of demographic, system- and individual-level factors that have facilitated the rapid development and adoption of RPM interventions in healthcare. In terms of demographic factors, an ageing population with heightened care needs has been a key driver in the rise in popularity of RPM interventions. This is especially so in recent years whereby the concept of ageing in place is gaining policy attention. RPM interventions are widely regarded as effective nonpharmacological tools that allow physicians to monitor many types of acute and chronic conditions among the older population who require close monitoring but prefer to be tracked in the comfort of their homes without being institutionalised1. At the system level, the ballooning healthcare expenditures and insufficient healthcare resources in terms of manpower and service provision also play key roles in the acceleration of RPM intervention adoption1,5. However, some argue that RPM may not be cost-effective. For instance, Mecklai et al.50 argued that the change of reimbursement rule in the US—the establishment of new billing codes by the Centre of Medicaid Services for Chronic Care RPM in 2019 and a revision in 2020, which enabled reimbursement for the initial setup of RPM interventions and their associated services which include patient education, collection and interpretation of data and treatment management services) may well escalate healthcare expenditures in the health system due to increased RPM intervention uptake. According to the authors’ calculation based on administrative data, a conservative estimate that assumes RPM enrolment and dissemination of the RPM interventions to be limited to patients with multiple chronic conditions alone (which is about 25.4 million patients as of September 2020), and placing a cap of uptake level at 50%, could translate into maximum annual cost per patient enrolled into the RPM programme at US$1,460, with annual health expenditures exceeding US$18 billion50. At the individual level, social and behavioural factors such as influences from family and friends as well as the duration of using the technology play important roles in influencing technology acceptance towards the use of technologies for health tracking purpose51,52. Policymakers and healthcare administrators can take note of these facilitators to test and deploy RPM interventions that could augment and supplement the functional roles of human healthcare workers while addressing the health needs of different segments of populations based on their unique contextual conditions. It is nonetheless important for these technologies to be subjected to constant evaluation not only to assess their impacts but also their acceptability and usability.
It is equally important for policies and practices around RPM interventions to be vigilant of the barriers to technology adoption, including the downsides, risks and unintended consequences that technology can bring. For instance, huge financial commitment entailing high start-up costs and ongoing operational costs, shortfalls in technical skills, which include lack of training, technical support and infrastructure, as well as logistical issues which include licensure, credentialing and malpractice have been presented as barriers to the adoption of RPM interventions53. Another peripheral issue which may impede the adoption of RPM intervention is the challenge of data sharing. Effective implementation of RPM requires integration and consolidation of data from various devices and sources and making them easily available to the practitioners without infringing privacy laws or code of conduct1,24. Equity-related barriers that are associated with the affordability of technology, poor internet connectivity and poor health literacy among certain segments of the population should also be considered54. In addition, cultural considerations, which include a preference for personal touch and face-to-face contact among the population may also hinder the fast adoption of RPM intervention. A review of technology adoption for older people has demonstrated that technology adoption in the healthcare and long-term care settings needs to account for ethical issues such as autonomy/independence, social connectedness and human interactions, objectification, deception and social justice issues55. These are complex issues that require constant reflection on their use. Hence, healthcare practitioners will need to incorporate transparent audit mechanisms when deploying various RPM interventions to minimise their risks and unintended consequences. Policies and best practices around the deployment of these technologies should constantly be improved and amended from time to time to guide safe, responsible and ethical use of RPM interventions in the healthcare setting.
This review found that RPM interventions have increasingly been adopted in various clinical contexts in the past few years. This phenomenon is partially fuelled by the COVID-19 pandemic as well as the lack of healthcare workers during this period. However, we found that the current evidence base is dominated by developed countries in the West. Many developing countries are still grappling with health access issues and would benefit from the incorporation of RPM interventions in the health systems. In addition, there is a dominance of cardiovascular-related conditions in RPM intervention use, while other disease groups are less explored.
As more countries embrace remote monitoring technologies amid the pandemic, further studies are essential to assess their safety, clinical impact, quality of life, and cost-effectiveness, particularly in ensuring patient safety and service quality across various diseases at minimal costs. Additionally, more research is required to identify which devices and specifications offer the greatest clinical value to specific patient groups50. Economically, further evaluations should explore RPM interventions’ cost-effectiveness and benefits, considering both direct savings like reduced hospital stays and indirect costs like lost income or caregiver burdens. Furthermore, the extent to which RPM interventions can be leveraged to bridge health service delivery gaps in developing countries is an important area that needs more exploration.
The review suggests that RPM interventions combining patient education with active monitoring, whether alert-driven or routine, may enhance patient outcomes, meriting deeper empirical investigation.
Lastly, studies on RPM interventions’ implementation facilitators and barriers across care settings are vital for effective knowledge transfer. Such insights that encompass both best practices and suboptimal lessons are especially useful for health systems that are contemplating to scale-up technologies to accelerate the deployment of technology as a tool to meet rising healthcare needs and health demands.
Methods
We conducted a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). The review was registered on the PROSPERO database (ID: 412195). The PRISMA checklist can be found in Supplementary Table 1.
Search strategy
Searches were conducted between February to March 2023 and finalised by 9 March 2023 (Supplementary Table 2). We developed a comprehensive search string that aimed to identify randomised controlled trials (RCTs) examining the impacts of remote patient monitoring (RPM) technologies in the inpatient setting and during the immediate care transition period. Searches were limited to January 2000 to May 2023 to reflect modern advancements in the field of RPM interventions. Ongoing discussion among the authors resulted in the development of two search themes (see Table 5): RPM and related concepts as well as RCTs. A subject librarian was also consulted to refine the search strings. After the finalisation of the search strings, a systematic database search was conducted on PubMed, CINAHL, PsycINFO, Embase and SCOPUS.
Inclusion and exclusion criteria
We also developed a set of inclusion and exclusion criteria to facilitate the screening of the abstracts and full texts (see Table 6).
Data extraction and selection process
A data extraction framework that includes information such as author/year, aim of the study, sample size, participation demographics, intervention components, duration of the intervention, RPM technology deployed and the outcomes examined (clinical outcomes, patient safety, quality of life and cost outcomes) was constructed. This framework was co-developed among all the authors through ongoing discussion until a unanimous agreement was reached. Three authors (S.Y.T., J.S., Y.W.) were involved in the data extraction process, and information was charted and documented in a spreadsheet. The authors subsequently cross-checked a random selection of papers to ensure consistency and relevance of the data extracted based on the framework.
Critical appraisal
We employ the ‘revised Cochrane risk-of-bias tool for randomised trials (RoB 2) to assess the risk of bias of all the RCTs included in the synthesis. RoB 2 is structured to accommodate five domains of bias (risk of bias arising from the randomisation process, risk of bias due to deviations from the intended interventions, risk of bias due to missing outcome data, risk of bias in measurement of the outcome, risk of bias in selection of the reported result). In each domain, signalling questions were posed to guide the appraisals of different features of the trials. The responses to each signalling question ranged from yes (Y), partially yes (PY), partially no (PN), no (N), to no information (NI). Based on the responses to the signalling questions, bias is determined for each domain. Each domain can be judged as having ‘low’ risk of bias, ‘high’ risk of bias or ‘having some concerns’56.
Data synthesis
Due to substantial heterogeneity in the populations of interest and primary outcomes reported, we were unable to perform a meta-analysis. Instead, we opted for a narrative synthesis approach by anchoring to the idea of the thematic synthesis approach proposed by Thomas and Harden57. A thematic synthesis approach entailed, firstly, conducting line-by-line coding of the relevant findings section extracted from the included studies by paying specific attention to the RPM interventions, intervention components and primary outcomes reported in these studies. This is followed by the development of the descriptive sub-themes from these narratives by identifying similarities and differences in the data patterns. These sub-themes then led to the construction of four key analytical themes that are centred on the RPM intervention features and the various impacts resulting from the deployment of these technologies. The first author led the analysis assisted by the third author. The second author audited and cross-checked the analysis, to ensure consistency, coherence and logic were adhered to. The entire data synthesis process underwent several rounds of discussion and iterations until all the authors were satisfied with the analytical themes that captured the functions and applications of all the RPM interventions documented as well as the impacts.
References
Condry, M. W. & Quan, X. I. Remote patient monitoring technologies and markets. IEEE Eng. Manag. Rev. 51, 59–64 (2023).
Fortune Business Insights Research. Remote Patient Monitoring Devices Market Size, Share & Covid-19 Impact Analysis, by Type (Devices{Multi-Parameter Monitoring, Respiratory Monitoring, Blood Glucose Monitoring, Cardiac Monitoring, and Others} and Services), by Application (Oncology, Diabetes, Cardiovascular Diseases, and Others), by End-User (Payers, Providers and Patients), and Regional Forecast, 2021-2028. FBIR. https://www.fortunebusinessinsights.com/remote-patient-monitoring-devices-market-106328. Published 2023. Accessed 12.06.2024.
Hood C., Neal S., Manaoat Van, C. & Mossburg, S. E. Remote Patient Monitoring. AHRQ. https://psnet.ahrq.gov/perspective/remote-patient-monitoring. Published 2023. Accessed 12.06.2024.
Shaik, T. et al. Remote patient monitoring using artificial intelligence: current state, applications, and challenges. WIREs Data Min. Knowl. Discov. 13, e1485 (2023).
Babar, E. T. R. & Rahman, M. U. A smart, low cost, wearable technology for remote patient monitoring. IEEE Sens. J. 21, 21947–21955 (2021).
Chen, C., Ding, S. & Wang, J. Digital health for aging populations. Nat. Med. 29, 1623–1630 (2023).
Fan, K. G., Mandel, J., Agnihotri, P. & Tai-Seale, M. Remote patient monitoring technologies for predicting chronic obstructive pulmonary disease exacerbations: review and comparison. JMIR Mhealth Uhealth 8, e16147 (2020).
Fudim, M., Mirro, M. & Cheng, H. M. Audicor remote patient monitoring: FDA breakthrough device and technology for heart failure management. JACC Basic Transl. Sci. 7, 313–315 (2022).
Kurtz, S. M. et al. Patient perceptions of wearable and smartphone technologies for remote outcome monitoring in patients who have hip osteoarthritis or arthroplasties. J. Arthroplast. 37, S488–S492.e482 (2022).
Mir, O. et al. Digital remote monitoring plus usual care versus usual care in patients treated with oral anticancer agents: the randomized phase 3 CAPRI trial. Nat. Med. 28, 1224–1231 (2022).
Su, D. et al. Diabetes management through remote patient monitoring: the importance of patient activation and engagement with the technology. Telemed. J. E Health 25, 952–959 (2019).
Rosner, M. H. et al. Perspectives from the kidney health initiative on advancing technologies to facilitate remote monitoring of patient self-care in RRT. Clin. J. Am. Soc. Nephrol. 12, 1900–1909 (2017).
Sakamaki, T., Furusawa, Y., Hayashi, A., Otsuka, M. & Fernandez, J. Remote patient monitoring for neuropsychiatric disorders: a scoping review of current trends and future perspectives from recent publications and upcoming clinical trials. Telemed. J. E Health 28, 1235–1250 (2022).
Annis, T. et al. Rapid implementation of a COVID-19 remote patient monitoring program. J. Am. Med. Inf. Assoc. 27, 1326–1330 (2020).
Kuan, P. X. et al. Efficacy of telemedicine for the management of cardiovascular disease: a systematic review and meta-analysis. Lancet Digit Health 4, e676–e691 (2022).
Stevenson, L. W., Ross, H. J., Rathman, L. D. & Boehmer, J. P. Remote monitoring for heart failure management at home. J. Am. Coll. Cardiol. 81, 2272–2291 (2023).
Noah, B. et al. Impact of remote patient monitoring on clinical outcomes: an updated meta-analysis of randomized controlled trials. NPJ Digit. Med. 1, 20172 (2018).
Iqbal, F. M. et al. Clinical outcomes of digital sensor alerting systems in remote monitoring: a systematic review and meta-analysis. NPJ Digit. Med. 4, 7 (2021).
Klersy, C. et al. Economic impact of remote patient monitoring: an integrated economic model derived from a meta-analysis of randomized controlled trials in heart failure. Eur. J. Heart Fail. 13, 450–459 (2011).
Patel, H. Y. & West, D. J. Jr Hospital at home: an evolving model for comprehensive healthcare. Glob. J. Qual. Saf. Health. 4, 141–146 (2021).
Scherr, D. et al. Effect of home-based telemonitoring using mobile phone technology on the outcome of heart failure patients after an episode of acute decompensation: randomized controlled trial. J. Med. Internet Res. 11, e34 (2009).
Boriani, G. et al. The MOnitoring Resynchronization dEvices and CARdiac patiEnts (MORE-CARE) randomized controlled trial: phase 1 results on dynamics of early intervention with remote monitoring. J. Med. Internet Res. 15, e167 (2013).
Hindricks, G. et al. Quarterly vs. yearly clinical follow-up of remotely monitored recipients of prophylactic implantable cardioverter-defibrillators: results of the REFORM trial. Eur. Heart J. 35, 98–105 (2014).
Ahmed, A. H., Roumani, A. M., Szucs, K., Zhang, L. & King, D. The effect of interactive web-based monitoring on breastfeeding exclusivity, intensity, and duration in healthy, term infants after hospital discharge. J. Obstet. Gynecol. Neonatal Nurs. 45, 143–154 (2016).
Bouwsma, E. V. A. et al. Effectiveness of an internet-based perioperative care programme to enhance postoperative recovery in gynaecological patients: cluster controlled trial with randomised stepped-wedge implementation. BMJ Open 8, e017781 (2018).
Graetz, I. et al. Use of a web-based app to improve postoperative outcomes for patients receiving gynecological oncology care: a randomized controlled feasibility trial. Gynecol. Oncol. 150, 311–317 (2018).
Geramita, E. M. et al. Impact of a mobile health intervention on long-term nonadherence after lung transplantation: follow-up after a randomized controlled trial. Transplantation 104, 640–651 (2020).
Higgins, J. et al. Conventional follow-up versus mobile application home monitoring for postoperative anterior cruciate ligament reconstruction patients: a randomized controlled trial. Arthroscopy 36, 1906–1916 (2020).
Somsiri, V., Asdornwised, U., O’Connor, M., Suwanugsorn, S. & Chansatitporn, N. Effects of a transitional telehealth program on functional status, rehospitalization, and satisfaction with care in thai patients with heart failure. Home Health Care Manag. Pract. 33, 72–80 (2021).
Pietrantonio, F. et al. Green line hospital-territory study: a single-blind randomized clinical trial for evaluation of technological challenges of continuous wireless monitoring in internal medicine, preliminary results. Int J. Environ. Res. Public Health 18, 1–12 (2021).
Wintrich, J. et al. Remote monitoring with appropriate reaction to alerts was associated with improved outcomes in chronic heart failure: results from the OptiLink HF study. Circ. Arrhythm. Electrophysiol. 14, e008693 (2021).
Indraratna, P. et al. A smartphone-based model of care to support patients with cardiac disease transitioning from hospital to the community (TeleClinical Care): pilot randomized controlled trial. JMIR Mhealth Uhealth 10, e32554 (2022).
Jakobsen, A. S. et al. Home-based telehealth hospitalization for exacerbation of chronic obstructive pulmonary disease: findings from “the virtual hospital” trial. Telemed. J. E Health 21, 364–373 (2015).
Weintraub, A. et al. A multicenter randomized controlled evaluation of automated home monitoring and telephonic disease management in patients recently hospitalized for congestive heart failure: the SPAN-CHF II trial. J. Card. Fail. 16, 285–292 (2010).
Blasco, A. et al. Evaluation of a telemedicine service for the secondary prevention of coronary artery disease. J. Cardiopulm. Rehabil. Prev. 32, 25–31 (2012).
Ebert, D., Tarnowski, T., Gollwitzer, M., Sieland, B. & Berking, M. A transdiagnostic internet-based maintenance treatment enhances the stability of outcome after inpatient cognitive behavioral therapy: a randomized controlled trial. Psychother. Psychosom. 82, 246–256 (2013).
Guédon-Moreau, L. et al. Costs of remote monitoring vs. ambulatory follow-ups of implanted cardioverter defibrillators in the randomized ECOST study. Europace 16, 1181–1188 (2014).
Gallagher, B. D. et al. Telemonitoring adherence to medications in heart failure patients (TEAM-HF): a pilot randomized clinical trial. J. Card. Fail 23, 345–349 (2017).
Bernocchi, P. et al. Home-based telerehabilitation in older patients with chronic obstructive pulmonary disease and heart failure: a randomised controlled trial. Age Ageing 47, 82–88 (2018).
Fang, J., Huang, B., Xu, D., Li, J. & Au, W. W. Innovative application of a home-based and remote sensing cardiac rehabilitation protocol in chinese patients after percutaneous coronary intervention. Telemed. J. E Health 25, 288–293 (2019).
da Silva Schulz, R. et al. Telephonic nursing intervention for laparoscopic cholecystectomy and hernia repair: a randomized controlled study. BMC Nurs. 19, 38 (2020).
Li, L. et al. A mobile health app for the collection of functional outcomes after inpatient stroke rehabilitation: pilot randomized controlled trial. JMIR Mhealth Uhealth 8, e17219 (2020).
Hisam, A., Haq, Z. U., Aziz, S., Doherty, P. & Pell, J. Effectiveness of mobile health augmented cardiac rehabilitation (MCard) on health-related quality of life among post-acute coronary syndrome patients: a randomized controlled trial. Pak. J. Med. Sci. 38, 716–723 (2022).
Li, J. et al. A telerehabilitation programme in post-discharge COVID-19 patients (TERECO): a randomised controlled trial. Thorax 77, 697 (2022).
Soh, J. Y. et al. A mobile phone–based self-monitoring tool for perioperative gastric cancer patients with incentive spirometer: randomized controlled trial. JMIR Mhealth Uhealth 7, e12204 (2019).
van Goor, H. M. R. et al. Remote hospital care for recovering COVID-19 patients using telemedicine: a randomised controlled trial. J. Clin. Med. 10, 1–10 (2021).
Riegel, B., Stephens-Shields, A., Jaskowiak-Barr, A., Daus, M. & Kimmel, S. E. A behavioral economics-based telehealth intervention to improve aspirin adherence following hospitalization for acute coronary syndrome. Pharmacoepidemiol. Drug Saf. 29, 513–517 (2020).
Gray, J. E. et al. Baby CareLink: using the internet and telemedicine to improve care for high-risk infants. Pediatrics 106, 1318–1324 (2000).
DeVito Dabbs, A. et al. A randomized controlled trial of a mobile health intervention to promote self-management after lung transplantation. Am. J. Transpl. 16, 2172–2180 (2016).
Mecklai, K., Smith, N., Stern, A. D. & Kramer, D. B. Remote patient monitoring - overdue or overused? N. Engl. J. Med. 384, 1384–1386 (2021).
Giger, J. T. et al. Remote patient monitoring acceptance trends among older adults residing in a frontier state. Comput. Hum. Behav. 44, 174–182 (2015).
Zhang, Y., Leuk, J. S. & Teo, W. P. Domains, feasibility, effectiveness, cost, and acceptability of telehealth in aging care: scoping review of systematic reviews. JMIR Aging 6, e40460 (2023).
Alanazi, H. & Daim, T. Health technology diffusion: case of remote patient monitoring (RPM) for the care of senior population. Technol. Soc. 66, 101662 (2021).
Houlding, E. et al. Barriers to use of remote monitoring technologies used to support patients with COVID-19: rapid review. JMIR Mhealth Uhealth 9, e24743 (2021).
Tan, S. Y., Taeihagh, A. & Tripathi, A. Tensions and antagonistic interactions of risks and ethics of using robotics and autonomous systems in long-term care. Technol. Forecast. Soc. Change 167, 120686 (2021).
Sterne, J. A. C. et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. Br. Med. J. 366, l4898 (2019).
Thomas, J. & Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med. Res. Methodol. 8, 45 (2008).
Acknowledgements
We would like to acknowledge Dr Tan, who sadly passed away not long after this work was completed. She continues to inspire us all through her dedication as a researcher and her kindness and support as a colleague. This research is supported by the Singapore Ministry of Health’s National Medical Research Council RIE2025 Centre Grant Programme (Grant number: NMRC/CG3/003/2022-AH/MOH-0010130-00).
Author information
Authors and Affiliations
Contributions
Conceptualisation, S.Y.T. and J.S.; methodology, S.Y.T., J.S. and Y.W.; validation, S.Y.T., J.S. Y.W. and A.Y.; formal analysis, S.Y.T., J.S. and Y.W.; investigation, S.Y.T., J.S. and Y.W.; resources, A.Y.; data curation: S.Y.T., J.S. and Y.W.; writing and editing S.Y.T., J.S. and Y.W.; supervision, S.Y.T. and A.Y.; project administration, A.Y.; funding acquisition, A.Y.; responding to reviewer comments S.Y.T. All authors read and agreed to the published version of the paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Tan, S.Y., Sumner, J., Wang, Y. et al. A systematic review of the impacts of remote patient monitoring (RPM) interventions on safety, adherence, quality-of-life and cost-related outcomes. npj Digit. Med. 7, 192 (2024). https://doi.org/10.1038/s41746-024-01182-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41746-024-01182-w
- Springer Nature Limited