
Abstract
Hypertension is often associated with metabolic syndrome (MetS) and serves as a risk factor of MetS and its complications. Blood pressure circadian rhythm in hypertensive patients has been suggested to contribute to cardiovascular consequences and organ damage of hypertension. But circadian changes of BP and their response to drugs have not been clearly investigated in non-human primates (NHPs) of MetS with hypertension. Here, we identified 16 elderly, hypertensive MetS rhesus monkeys from our in-house cohort. With implanted telemetry, we investigate BP changes and its circadian rhythm, together with the effect of antihypertensive drugs on BP and its diurnal fluctuation. MetS hypertensive monkeys displayed higher BP, obesity, glucose intolerance and dyslipidemia. We also confirmed impaired 24-h BP circadian rhythm in MetS hypertensive monkeys. Importantly, Eplerenone, a mineralocorticoid receptor blocker, exerts multiple beneficial effects in MetS hypertensive monkeys, including BP reduction, 24-h BP circadian rhythm restoration and decreased plasma concentration of inflammation factors and advanced glycation end-products. In summary, we identified a naturally-developed hypertensive MetS NHP model, which is of great value in the studies on pathogenesis of MetS-associated hypertension and development of novel therapeutic strategies. We also provided multiple novel mechanistic insights of the beneficial effect of Eplerenone on MetS with hypertension.
Similar content being viewed by others
Introduction
Hypertension is frequently present in patients with metabolic syndrome (MetS) and an important risk factor for cardiovascular-related morbidity and mortality1,2. Both insulin resistance (IR) and obesity elevate blood pressure (BP) via increased oxidative stress, inflammation, salt retention and impaired generation of nitric oxide3. Hypertensive patients with MetS have severe IR, together with elevated blood adipokines, such as leptin, tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6) and resistin, which not only over-activate the sympathetic nervous system and rennin-angiotensin-aldosterone system, but also promote inflammation, endothelial dysfunction and atherosclerosis4,5,6. Collectively, these factors contribute to the worsening of hypertension and significantly increase cardiovascular morbidity and mortality.
In the recently-published Guideline for Managing BP, thiazide-type diuretics, Ca2+ channel blockers (CCBs), angiotensin-converting enzyme inhibitors (ACEIs) and angiotensin receptor blockers (ARBs) are recommended as first-line drugs for the treatment of hypertension7. However, the use of α- or β-blockers as an initial treatment is controversial8,9,10. ACEIs, ARBs and CCBs have beneficial effects on MetS by reducing inflammation11, increasing insulin sensitivity12 and improving the secretion of adiponectin13. It has been shown that another class of anti-hypertensive drugs, the mineralocorticoid receptor (MR) blockers, have greater BP lowering effects and cardiovascular benefits14,15,16,17.
The cardiovascular system exhibits a distinct temporal organization, particularly with respect to diurnal variations in BP and heart rate (HR)18. Arterial BP has a circadian variation, usually expressed as a 10–20% drop during the night and a rapid rise upon awakening. This pattern is typically disturbed in hypertensive patients19. Several lines of evidence suggest that, in addition to contributing to elevated BP in cardiovascular outcomes, disturbed 24-h BP circadian rhythm is associated with increased incidence of cardiovascular events and mortality20. These studies indicate that it is important to manage the circadian rhythm of BP in hypertension therapy21,22. There is growing interest in how current and newly-discovered medications that lower BP affect the circadian pattern23.
As a consequence of their phylogenetic proximity to humans, non-human primates (NHPs) are particularly relevant species for preclinical studies. Prior studies have shown that NHPs naturally develop symptoms of MetS and hypertension similar to those in humans24,25. However, their innate aggressiveness and the difficulty of training NHPs make it hard to measure cardiovascular parameters under conscious and freely-moving conditions. Most examinations have to be performed under anesthesia or restraint, which not only affect BP, but also make it impossible to assess the circadian rhythm. Therefore, very few studies on the circadian BP rhythm are available, other than those in normal marmosets that show a circadian rhythm similar to humans26,27,28. To date, no data are available for other NHPs and in particular there are no comparative data from normotensive and hypertensive NHPs, due to the lack of suitable measurement devices and a well-characterized stable population of animals.
In the current study, we established a NHP model with both MetS and hypertension. And with an implanted telemetry system to continuously record BP, we tested the BP-lowering effects and the restoration of impaired 24-h BP circadian rhythm by Eplerenone (an MR blocker) in the MetS hypertensive NHP model. We also accessed the plasma concentration of inflammation factors and advanced glycation end-products before and after Eplerenone treatment. This study not only provides a valuable tool for assessment of the pathogenesis and pharmacological effects in hypertension in NHPs with MetS, but also sheds light on the novel therapeutic mechanisms of MR antagonists.
Results
Identification and characterization of naturally-developed hypertension in rhesus monkeys with spontaneous MetS
We have reported previously that rhesus monkeys develop typical spontaneous MetS with aging25. Among the 5 MetS parameters, high BP, especially elevated Systolic BP (SBP), presents most frequently25. According to the hypertension-diagnosis standard for humans and NHPs29, we set SBP ≥140 mmHg or diastolic BP (DBP) ≥90 mmHg (average of the last two in-house tests under ketamine anesthesia) as the criteria for hypertension in the monkeys and SBP <130 mmHg/DBP <90 mmHg as normotension. Based on these criteria, from the continuous follow-up data of our previous reported cohort monkeys and other in-house cohort of monkeys, we identified 17 control normotensive (out of 23 control monkeys) and 16 MetS hypertensive monkeys (out of 23 MetS monkeys that did not yet have type 2 diabetes).
The metabolic and anthropometric characteristics of control normotensive and MetS hypertensive monkeys from the latest two tests are summarized in Table 1. Compared with the normotensive group, MetS hypertensive monkeys displayed significantly higher SBP and DBP, together with increased waist circumference, body weight, triglycerides, fasting plasma glucose, fasting insulin, homeostasis model assessment-IR and C-reactive protein. High-density lipoprotein was lower in MetS hypertensive monkeys. However, low-density lipoprotein and total cholesterol were similar in both groups. Plasma glucose levels were significantly higher in MetS hypertensive monkeys than in control normotensive monkeys at 1, 3, 5, 10, 15, 20, 30, 45 and 60 min after glucose challenge (Fig. 1a). Similarly, the area under the curve (AUC) was significantly greater in MetS hypertensive monkeys than in controls (Fig. 1b). The rise in insulin levels induced by glucose and the corresponding AUC showed an increasing trend in the MetS hypertensive group (Fig. 1c,d). Collectively, the data indicate that hypertension is associated with obesity, dyslipidemia and IR in MetS hypertensive monkeys.

Plasma glucose and insulin responses during the intravenous glucose tolerance test.
(a) Glucose excursion. (b) Area under the glucose curve. (c) Insulin excursion. (d) Area under the insulin curve. Data are expressed as mean ± SEM; n = 17 for control normotensive group and 16 for MetS hypertensive group. *P < 0.05, **P < 0.01 vs corresponding control normotension group. MetS, metabolic syndrome.
BP under ketamine anesthesia was comparable to that measured via chronic, implanted telemetry
During follow-up screening, the BP and HR were measured under ketamine anesthesia. To compare the BP level under anesthesia and in freely-moving conditions and to further obtain accurate 24-h BP in conscious monkeys, we implanted the DSI telemetry system into 5 control normotensive and 8 MetS hypertensive monkeys (one of the MetS monkeys was excluded due to a technical problem).
The arterial BP waveforms from both groups recorded by telemetry are shown in Fig. 2a. After 2 weeks of recovery from surgery, we confirmed that the 24-h average BP (SBP and DBP) and HR were stable in both the control normotensive and MetS hypertensive groups throughout 8 continuous days of recording (Fig. 2b,c). The 24-h average values (mean of 8 days) in the MetS hypertensive monkeys were 161.0 ± 6.5 (SBP), 92.1 ± 5.9 (DBP), 113.5 ± 6.3 (mean BP, MBP) and 69.3 ± 3.3 mmHg (pulse pressure, PP), all of which were higher (P < 0.01 for SBP and PP, P < 0.05 for DBP and MBP) than those of the control group (128 ± 4.9, 74.9 ± 3.1, 90.7 ± 3.4 and 53.3 ± 3.0 mmHg) (Fig. 2d). HR was similar in the 2 groups (Fig. 2d), which differed from the results during anesthesia (Table 1). This may be attributed to different responses of the 2 groups of monkeys to anesthesia. We also measured BP with a cuff in anesthetized monkeys and compared the values with those obtained from the telemetry system at the same time and found a close correlation (Supplemental Fig. 1), suggesting that both of methods are suitable in monkeys.

BP recorded by telemetry in control normotensive and MetS hypertensive groups.
(a) Representative waveforms of BP measured by telemetry in control normotensive (left panel) and MetS hypertensive (right panel) monkeys. (b,c) 24-h averaged SBP and DBP (b) and HR (c) of control normotensive (n = 5) and MetS hypertensive groups (n = 7). (d) Averaged SBP, DBP, MBP, PP and HR during the 8 days in panels B and C in control normotensive (n = 5) and MetS hypertensive (n = 7) monkeys (*P < 0.05, **P < 0.01 vs control normotension). (e) Comparison of SBP and DBP recorded by telemetry (09:00–12:00) and cuff (during screening) in control normotensive (n = 5) and MetS hypertensive (n = 7) monkeys. Data are expressed as mean ± SEM. SBP, systolic blood pressure; DBP, diastolic blood pressure; MBP, mean blood pressure; PP, pulse pressure; HR, heart rate; MetS, metabolic syndrome.
In our previous tests, the BP and HR measurements under anesthesia were all performed between 09:00 and 12:00. Since BP and HR have a diurnal variation, we compared the average BP and HR from our last two tests with the 4-day average recorded by telemetry between 09:00 and 12:00. Although the SBP and DBP recorded in the latest 2 tests under anesthesia were slightly lower than those recorded in conscious animals by telemetry in both the control normotensive and MetS hypertensive groups, the differences were not significant (Fig. 2e). These data indicate that repeated BP measurement with well-controlled anesthesia is a convenient and reliable method to identify hypertensive animals from a population of NHPs.
Telemetry and model validation with CCB treatment
To ensure that the implanted BP transmitters were functional and able to detect changes in BP, after baseline recording for 4 days, Amlodipine, a long-acting CCB, was orally delivered to the MetS hypertensive monkeys (Fig. 3a). Control normotensive animals received vehicle during the same period. Consistent with clinical studies30, the SBP, DBP, MBP and PP of these monkeys were significantly decreased upon Amlodipine treatment in a dose-dependent manner, while HR was elevated (Fig. 3b). All of these indices returned to baseline by 3 days after Amlodipine washout (Fig. 3b). The SBP, DBP, MBP, PP and HR of the control normotensive monkeys, which received vehicle, remained unchanged (Fig. 3c), further confirming the capacity of Amlodipine to lower BP and the stability of the telemetry recording.

Effect of Amlodipine on MetS hypertensive monkeys.
(a) Protocol for Amlodipine treatment in MetS hypertensive monkeys. (b,c) SBP, DBP, MBP, PP and HR of control normotensive (n = 5) and MetS hypertensive (n = 7) monkeys. MetS hypertensive monkeys (b) were treated with Amlodipine. Control normotensive monkeys (c) were treated with vehicle during the same periods (*P < 0.05, **P < 0.01 vs baseline values of the corresponding group). Data are expressed as mean ± SEM. SBP, systolic blood pressure; DBP, diastolic blood pressure; MBP, mean blood pressure; PP, pulse pressure; HR, heart rate; MetS, metabolic syndrome.
24-h BP circadian rhythm in rhesus monkeys
Taking advantage of the MetS hypertensive model and the telemetry system, we analyzed the 24-h BP circadian rhythm in the control normotensive and the MetS hypertensive rhesus monkeys. The BP values used to analyze circadian rhythms in both groups of monkeys were the average of 4 days of baseline recording.
The pattern of BP and HR fluctuations over 24 h was similar in both control normotensive and MetS hypertensive monkeys, i.e. higher during the day and lower at night, but the BP variability was decreased in the MetS hypertensive group (Fig. 4a–c, Table 2), consistent with the findings in humans19,31. The amplitudes of SBP, DBP and MBP in the MetS hypertensive group were lower than those in control normotensive monkeys, although only DBP reached significance (P = 0.007) (Table 2). The HR amplitude was similar in the 2 groups (Fig. 4d, Table 2). Overall, these results provide a valuable reference for using rhesus monkeys as a model in which to perform detailed chronobiological cardiovascular studies and for preclinical pharmacological tests on BP control and circadian rhythm.

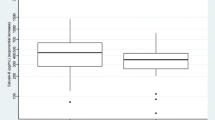
Circadian rhythm of blood pressure in control normotensive and MetS hypertensive groups.
(a–d) Circadian rhythms of SBP (a), DBP (b), MBP (c) and HR (d) of control normotension (n = 5) and MetS hypertensive groups (n = 7). SBP, DBP, MBP and HR were continuously collected as the average of every 20 seconds with the telemetry system. Error bars show the 95% confidence intervals of the amplitude. Data are expressed as mean ± SEM. SBP indicates systolic blood pressure; DBP, diastolic blood pressure; MBP, mean blood pressure; HR, heart rate; MetS, metabolic syndrome.
Effect of MR blocker on hypertensive MetS monkeys
The effect of Eplerenone, a selective MR antagonist, on BP and BP circadian rhythm was evaluated in the MetS hypertensive animals. Baseline measurements of BP and HR were recorded for 4 days, Eplerenone was then administered. During treatment, the monkeys were anesthetized to collect blood samples at baseline, 1 and 14 days after Eplerenone treatment and at 13 days after washout (Fig. 5a). Consistent with clinical reports32, the plasma aldosterone level in MetS hypertensive monkeys was significantly higher than control monkeys and it was further increased after administration of eplerenone by compensation (Fig. 5b). Similarly, plasma renin activity (PRA) also increased significantly after eplerenone treatment (Fig. 5c). In the monkeys that received Eplerenone, the SBP significantly decreased during weeks 1 and 2 of treatment compared with baseline (154.6 ± 6.4 and 148.1 ± 5.7 vs 159.1 ± 6.4 mmHg, P < 0.05) (Fig. 5d). PP was lower than baseline during week 2 of treatment (61.7 ± 4.8 vs 72.0 ± 3.0 mmHg, P < 0.05) (Fig. 5d). HR was elevated 2 weeks after treatment, while MBP and DBP remained unchanged (Fig. 5d). Eplerenone treatment for 2 weeks altered neither plasma potassium and lipid, nor hepatic and kidney function (Supplemental Fig. 2).

Effect of Eplerenone on MetS hypertensive monkeys.
(a) Protocol for Eplerenone treatment. (b) Plasma concentrations of aldosterone of MetS hypertensive (n = 7) and control normotensive (n = 5) monkeys during baseline, Eplerenone (for MetS hypertensive) (30 mg/kg/day, p.o., once a day) or Vehicle (for control normotensive) treatment for 2 days and 2 weeks and washout for 13 days. (c) PRA of MetS hypertensive (n = 7) monkeys during baseline and Eplerenone treatment (30 mg/kg/day, p.o., once a day) for 14 days and washout for 13 days. (d) SBP, DBP, MBP, PP and HR in MetS hypertensive monkeys at baseline and after periods of Eplerenone treatment (n = 7). (e) Plasma concentrations of resistin (left panel) and IL-6 (right panel) of MetS hypertensive monkeys at baseline and after 14 days of Eplerenone treatment (*P < 0.05). (f–i) Comparison of 24-h circadian rhythms of SBP (f), DBP (g), MBP (h) and HR (i) in MetS hypertensive monkeys before and after Eplerenone treatment (n = 7). The error bars in (f–i) show the 95% confidence interval of the amplitude. (j,k) Plasma concentrations of AGE (j) and sRAGE (k) of Control nomotension and MetS hypertensive monkeys at baseline and after 14 days of Eplerenone treatment (*P < 0.05 vs baseline values of the corresponding group). Data are expressed as mean ± SEM. For panels (b,c), *P < 0.05, **P < 0.01 vs baseline, #P < 0.05 vs the corresponding group values of control normotension. MetS, metabolic syndrome; PRA, plasma rennin activity; SBP, systolic blood pressure; DBP, diastolic blood pressure; MBP, mean blood pressure; HR, heart rate; AGE, advanced glycation end-products, sRAGE, soluble receptor of AGE.
Besides its BP-lowering effect, we found that Eplerenone also significantly decreased the plasma concentrations of resistin and IL-6 (Fig. 5e), both of which have been associated with inflammation and hypertension in obesity33. Inhibiting resistin and IL-6, together with inflammation, may also contribute to the cardiac beneficial effect of Eplerenone as anti-hypertensive therapy. However, the other adipokines (adiponectin, leptin, monocyte chemoattractant protein-1 (MCP-1) and TNF-α) were not changed by Eplerenone treatment in our experiments (Supplemental Fig. 3).
Several recent studies have investigated the relationship between BP circadian rhythm and cardiac outcome and have drawn diverse conclusions depending on treatments and populations in different studies21,31,34. And so far, there is no data on the role of Eplerenone in the regulation of 24-h BP circadian rhythm. In this study, we tracked the rhythmicity of diurnal BP patterns before and after Eplerenone treatment. The diurnal variations of SBP, DBP and MBP (indicated by the amplitude) were restored in MetS hypertension monkeys without changing the BP diurnal fluctuation after 2 weeks of treatment, although only that of MBP reached significance (P = 0.004) (Fig. 5f–h, Table 3). The HR amplitude was slightly increased with treatment (Fig. 5i, Table 3). Restoring the pattern of a nocturnal decrease in BP may also contribute to the cardiac beneficial effects of Eplerenone in hypertensive patients.
Advanced glycation end-products (AGEs) have been established to play a key role in the development and progression of multiples cardiovascular diseases and metabolic disorders. Although MR antagonists have been shown to perform beneficial effects on the patients with hypertension and MetS, so far, there is no report on the relationship between MR antagonists and AGEs. We found that 2-week Eplerenone treatment significantly decreased the plasma AGE concentration in MetS hypertensive monkeys to a similar level as in control normotensive ones (Fig. 5j). And Eplerenone treatment did not affect the plasma concentration of soluble receptor of AGE (sRAGE), which inhibits AGE signaling via targeting the receptor of AGEs (RAGE) (Fig. 5k). These data underlie a correlation between MR antagonists and AGE system.
Discussion
In recent decades, unhealthy lifestyles characterized by sedentary behavior and a high intake of calories have driven a burst in the prevalence of MetS. Hypertension presents most frequently within this clinical constellation1,2 and is a critical risk factor for cardiovascular complications and other organ damage. Understanding the pathogenesis will provide novel or more effective therapeutic strategies for hypertension. In the present study, we devised, implemented and validated a set of strategies to establish a natural model of MetS hypertensive rhesus monkeys. We also pursued to elucidate the mechanisms of the beneficial effects of MR blockers, a newly identified anti-hypertensive drug proved to benefit the metabolic disorders.
Hypertension associated with MetS has unique pathophysiological characteristics that provide clinical challenges for both mechanistic studies and successful therapeutic interventions. MetS-related IR, increased plasma insulin and multiple adipokines promote inflammation, endothelial dysfunction and atherosclerosis, all of which contribute to hypertension and consequent cardiovascular events3,4,5,6. Regarding the choice of anti-hypertensive drugs for MetS, ACEIs, ARBs, CCBs and MR blockers have beneficial effects on metabolic diseases11,12,13,17,35,36.
Large-animal models are of great value for pharmacological studies. NHPs are more similar to humans than other species with respect to drug metabolism, lipoprotein profiles, the development of cardiovascular diseases and genetics. In addition, compared with humans, the advantages of our NHP model include drug-naive subjects, well-controlled laboratory conditions with respect to food composition and daily activity and freedom from risk factors such as smoking and alcohol consumption. However, to date, there are no well-characterized MetS NHP models with hypertension. Thus, developing and characterizing NHP models with major diseases is essential for both basic and translational research as well as preclinical drug testing.
Spontaneously-occurring hypertension has been reported previously in NHPs37,38,39. But in those studies, relatively young animals (<10 years) were used and no metabolic index was investigated. Although previous reports from our lab25 and another group24 have shown that NHPs spontaneously develop MetS, hypertension was neither focused on nor deeply investigated in those studies. In the current study, we compared BP levels with repeated cuff measurement under ketamine anesthesia and recorded from freely-moving rhesus monkeys via telemetry. To our knowledge, this is the first time to set up a convenient method to identify a group of monkeys with naturally-developed hypertension and MetS. We performed detailed investigation of cardiovascular circadian rhythms (BP and HR) using data from elderly, freely-moving, control normotensive and MetS hypertensive rhesus monkeys. In addition, both the control normotensive and MetS hypertensive monkeys in our study were relatively old (control normotensive, 18.9 ± 1.1 and MetS hypertensive 18.4 ± 1.2 years), which mimics the condition in aging humans, who have a very high prevalence of both hypertension and MetS.
Using a telemetry system to continuously monitor BP in conscious, freely-moving monkeys, we validated our models with two anti-hypertension drugs, Amlodipine and Eplerenone, which have been shown to improve MetS with hypertension. In all of the prior studies of BP in monkeys25,37,38,39, BP was measured with a cuff in either anesthetized or restrained animals, which is unable to provide 24-h BP. The telemetry system enabled us to continuously and accurately measure BP in conscious, freely-moving monkeys. SBP and DBP showed significant correlations between cuff and telemetric measurements when measured simultaneously in the same animals. Cuff measurements may be more suitable for large scale, long-term studies. Telemetry is a better method to more accurately study the mechanisms of action and efficacy or safety of therapies.
Previous studies have suggested that elevated levels of aldosterone have adverse effects, including cardiovascular dysfunction, hypertension, IR and organ damage40. When MetS hypertensive monkeys were chronically treated with Eplerenone, an MR blocker, BP decreased significantly. In addition, we found that it also reduced the blood concentrations of IL-6 and resistin; this could produce multiple beneficial effects on anti-hypertensive therapy including reducing inflammation, blocking the renin–angiotensin system (RAS), elevating vasorelaxation mediated by nitric oxide, alleviating IR and preventing structural changes in the vasculature33. Furthermore, the potential function of MR blocker in reducing oxidative stress and L-type Ca channel activity in vascular smooth muscle cell might also contributes to the blood pressure lowering effect41. Here we provided 2 novel mechanisms of the protective effect of MR antagonists, including restoration of the impaired 24-h BP circadian rhythm and the decreased plasma AGE level.
Since the outcome of hypertension depends on not only the BP level, but also the circadian rhythm of BP42,43,44, we investigated this readout via telemetry in conscious monkeys. In patients with essential hypertension, losing the nocturnal fall in BP is associated with more serious organ damage than in patients whose BP falls during the night45, indicating the importance of proper evaluation of BP rhythms. Clinically, even with noninvasive measurement of 24-h BP, data collection with ambulatory blood pressure monitors over 24 h or longer can influence patient status, such as sleep quality and mood. These negatively impact assessment of the circadian BP rhythm. But with the implanted telemetry in our monkeys, there was no influence on routine life, further highlighting the uniqueness of the NHP hypertension model with telemetry as an ideal system for preclinical testing of the efficacy of anti-hypertensive drugs, especially newly-developed drugs.
AGEs are a heterogeneous group of reactive derivatives of nonenzymatic glucose-protein condensation reactions, as well as lipid and nucleic acids exposed to reducing sugars. AGEs have been proved to play a key role in the development of both diabetes and hypertension, together with their complications including myocardial infarction, heart failure, chronic renal failure and retinopathy46,47. And multiple studies have shown the correlation between the elevated blood AGE levels and these diseases46,47. Here for the first time, we identified that Eplerenone decreased plasma AGE concentration and is a novel inhibitor of AGE system. Some studies have evaluated the influence of RAS (especially ARBs) on the AGE-RAGE (the receptor of AGEs) axis, but with conflicting conclusions48,49,50,51. From our data, we provided the evidence that blockage of RAS decreases plasma AGEs in the NHP model with MetS and hypertension. Although in a previous study, inhibition of RAS reduced plasma sRAGE (soluble RAGE) level52, in our model, we did not find any change of plasma sRAGE concentration.
Although Eplerenone is a highly selective MR blocker, we can not exclude the possibility that its beneficial effect including the restoration of BP circadian rhythm and AGE levels may be also attributed to its off-target action in addition to the blockage of MR. It has been reported that Eplerenone may induce off-target effects through the androgen receptor, affecting hormone secretion and function53.
In summary, our study established a novel, naturally developed NHP model with both MetS and hypertension, offering a valuable tool for both mechanistic and translational cardiometabolic research. And with this model, we provided novel insights of the therapeutic mechanisms of MR blockers. Besides the previously reported beneficial effect, including BP decreasing and inflammation inhibition, Eplerenone also restores the 24-h BP circadian rhythm and reduced the plasma level of AGEs.
Methods
Animal and Housing
All of the experimental procedures were approved by the Institutional Animal Care and Use Committee of Peking University and were carried out in accord with the principles of laboratory animal care of the National Academy of Sciences/National Research Council. The rhesus monkeys (Macaca mulatta) were from our in-house cohort that was described in a previous report25 and were housed individually in cages in the Laboratory Animal Center of Peking University, with a 12-h light/dark cycle, a temperature range of 18–24 °C and humidity of 40–70%. The monkeys had free access to water and were fed ad libitum with monkey chow (Beijing HFK Bio-Technology Co. Ltd, China), which contains 7–10% crude fat, 16–20% crude protein and 55–65% crude carbohydrate.
Blood Test and Cuff Blood Pressure Measurement
Body weight, waist and hip circumference, glucose tolerance and blood biochemistry were measured every 6 months in all the in-house animals, following procedures described previously25. All of the data used in this study were from the average of the latest two tests. The cuff BP was measured using a mercury sphygmomanometer at 15–30 and 40–50 min after ketamine anesthesia (10 mg/kg, i.m.) and was calculated as the mean of the 2 measurements. HR was recorded on an electrocardiograph (MAC 1200ST, General Electric Co., Fairfield, CT, USA).
PRA was measured using an iodine (125I) angiotensin I radioimmunoassay kit (Beijing North Institute of Biological Technology, Beijing, China), plasma aldosterone was measured with an iodine (125I) aldosterone radioimmunoassay kit (Beijing North Institute of Biological Technology) and the data used for analysis was the average of two tests. Plasma resistin, IL-6, adiponectin, leptin, MCP-1 and TNF-α were assayed with Milliplex kits from Merck (Cat # HADK1MAG-61K and NHPMHMAG-45K). The ELISA kit for plasma AGEs and sRAGE was from Shanghai BlueGene Biotech CO.,LTD., China.
Transmitter Implantation
To obtain continuous 24-h BP under freely-moving conditions in rhesus monkeys, BP was measured with an implantable telemetric transmitter from Data Sciences International, St Paul, MN, USA (DSI, model TL11M2-D70-PCT). The animals were fasted overnight and sedated with ketamine (10 mg/kg, i.m.) and the propofol (3–4 mg/kg) was injected through i.v. for intubation and maintained under inhaled Isoflurane (4% in oxygen for induction, 1.5–2.5% for maintenance) throughout the surgical procedure. Secure the animal in supine position on the surgery table, remove the body hair from all intended incision sites and sterilized with Povidone-iodine. Using a scalpel blade, a 4–5 cm midline incision was made through the skin and abdominal wall. Then the transmitter was inserted and sutured to the abdominal wall intraperitoneally. For arterial cannulation, a 2–3 cm incision was made through the skin over the femoral vessels. Then the femoral artery was isolated and a trocar was used to tunnel subcutaneously from the femoral incision to the transmitter. The arterial BP catheter was passed through the trocar and the catheter was introduced into the femoral artery until its tip was estimated to be in the terminal portion of the abdominal aorta. It was then secured in place by suture ties and the incision was closed. The animals were allowed to recover from surgery for at least 2 weeks before BP recording.
Telemetry and Anti-hypertensive Drug Treatment
During telemetry, the animals were housed in individual recording cages and continuous recordings were made throughout the experiment periods. The BP data were analyzed as the mean of 1 or 24 h. For 24-h recordings, the mean value was from 07:00 to 07:00.
Data were recorded continuously for at least 4 days (baseline) before pharmacological treatment was initiated. All the animals used for telemetry had been trained for 2–3 years to cooperate for oral drug administration. The vehicle (orange juice) or drugs diluted in vehicle were delivered orally between 09:00 and 10:00 every day. Vehicle administration was also performed during baseline recording. Amlodipine besylate (Chempacific, Cat# 33369) was administered once a day between 09:00 and 10:00 for two days (1 mg/kg on day 1 and 3 mg/kg on day 2, p.o.). Eplerenone (30 mg/kg, p.o.) (Jiangxi Yuneng Medicine Chemical Co., Ltd., Ji’an, China and provided by Merck for R&D use only) was administered once a day between 09:00 and 10:00 for 14 days.
Rhythm Analysis
SBP, DBP and MBP, along with HR from each monkey were continuously collected as the average of every 20 seconds with the telemetry system and assessed for the presence of a circadian rhythm by single cosinor analysis. Rhythm by group was assessed by population mean-cosinor analysis. A circadian rhythm was considered to be present if the model could be fitted (F value >3). The model reported two parameters. The MESOR is the median between the highest and lowest values of the fitted cosine. The amplitude is the distance between the MESOR and the highest (or lowest) value of the cosine curve. The amplitude represents the range of the rhythmic change. The cosinor analysis and graphs were performed in Mathemetica 9.0 (Wolfram Research, Inc., Champaign, IL, USA).
Statistical Analysis
All data are expressed as mean ± SEM. Student’s t-test was used to evaluate differences between control and experiment groups. Paired t-test data were compared before and after medication. Data analysis was performed using the SPSS 18.0 software package (SPSS Inc., Chicago IL, USA). Two-sided P < 0.05 was used to denote statistical significance.
Additional Information
How to cite this article: Zhang, Y. et al. Eplerenone restores 24-h blood pressure circadian rhythm and reduces advanced glycation end-products in rhesus macaques with spontaneous hypertensive metabolic syndrome. Sci. Rep. 6, 23957; doi: 10.1038/srep23957 (2016).
References
Franco, O. H. et al. Trajectories of entering the metabolic syndrome: the framingham heart study. Circulation 120, 1943–1950 (2009).
Juhola, J. et al. Combined effects of child and adult elevated blood pressure on subclinical atherosclerosis: the International Childhood Cardiovascular Cohort Consortium. Circulation 128, 217–224 (2013).
Duvnjak, L. & Duvnjak, M. The metabolic syndrome - an ongoing story. J Physiol Pharmacol 60 Suppl 7, 19–24 (2009).
Kashyap, S. R. et al. Insulin resistance is associated with impaired nitric oxide synthase activity in skeletal muscle of type 2 diabetic subjects. J Clin Endocrinol Metab 90, 1100–1105 (2005).
Piya, M. K., McTernan, P. G. & Kumar, S. Adipokine inflammation and insulin resistance: the role of glucose, lipids and endotoxin. J Endocrinol 216, T1–T15 (2013).
Steinberg, H. O. et al. Obesity/insulin resistance is associated with endothelial dysfunction. Implications for the syndrome of insulin resistance. J Clin Invest 97, 2601–2610 (1996).
James, P. A. et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). Jama 311, 507–520 (2014).
Diuretic versus alpha-blocker as first-step antihypertensive therapy: final results from the Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). Hypertension 42, 239–246 (2003).
Dahlof, B. et al. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 359, 995–1003 (2002).
Dasgupta, K. et al. The 2014 Canadian Hypertension Education Program recommendations for blood pressure measurement, diagnosis, assessment of risk, prevention and treatment of hypertension. Can J Cardiol 30, 485–501 (2014).
Sola, S. et al. Irbesartan and lipoic acid improve endothelial function and reduce markers of inflammation in the metabolic syndrome: results of the Irbesartan and Lipoic Acid in Endothelial Dysfunction (ISLAND) study. Circulation 111, 343–348 (2005).
Shiuchi, T. et al. ACE inhibitor improves insulin resistance in diabetic mouse via bradykinin and NO. Hypertension 40, 329–334 (2002).
Makita, S., Abiko, A., Naganuma, Y., Moriai, Y. & Nakamura, M. Potential effects of angiotensin II receptor blockers on glucose tolerance and adiponectin levels in hypertensive patients. Cardiovasc Drugs Ther 21, 317–318 (2007).
Parviz, Y. et al. Emerging cardiovascular indications of mineralocorticoid receptor antagonists. Trends Endocrinol Metab 26, 201–211 (2015).
Pitt, B. et al. Effects of eplerenone, enalapril and eplerenone/enalapril in patients with essential hypertension and left ventricular hypertrophy: the 4E-left ventricular hypertrophy study. Circulation 108, 1831–1838 (2003).
Suzuki, H. et al. Eplerenone, an aldosterone blocker, is more effective in reducing blood pressure in patients with, than without, metabolic syndrome. Ther Adv Cardiovasc Dis 6, 141–147 (2012).
Tirosh, A., Garg, R. & Adler, G. K. Mineralocorticoid receptor antagonists and the metabolic syndrome. Curr Hypertens Rep 12, 252–257 (2010).
Rudic, R. D. Time is of the essence: vascular implications of the circadian clock. Circulation 120, 1714–1721 (2009).
Millar-Craig, M. W., Bishop, C. N. & Raftery, E. B. Circadian variation of blood-pressure. Lancet 1, 795–797 (1978).
Ingelsson, E., Bjorklund-Bodegard, K., Lind, L., Arnlov, J. & Sundstrom, J. Diurnal blood pressure pattern and risk of congestive heart failure. Jama 295, 2859–2866 (2006).
Hermida, R. C., Ayala, D. E., Mojon, A. & Fernandez, J. R. Blunted sleep-time relative blood pressure decline increases cardiovascular risk independent of blood pressure level–the “normotensive non-dipper” paradox. Chronobiol Int 30, 87–98 (2013).
Ohkubo, T. et al. Relation between nocturnal decline in blood pressure and mortality. The Ohasama Study. Am J Hypertens 10, 1201–1207 (1997).
Rothwell, P. M. Limitations of the usual blood-pressure hypothesis and importance of variability, instability and episodic hypertension. Lancet 375, 938–948 (2010).
Tigno, X. T., Gerzanich, G. & Hansen, B. C. Age-related changes in metabolic parameters of nonhuman primates. J Gerontol A Biol Sci Med Sci 59, 1081–1088 (2004).
Zhang, X. et al. Rhesus macaques develop metabolic syndrome with reversible vascular dysfunction responsive to pioglitazone. Circulation 124, 77–86 (2011).
Schnell, C. R. & Wood, J. M. Measurement of blood pressure and heart rate by telemetry in conscious, unrestrained marmosets. Am J Physiol 264, H1509–1516 (1993).
Schnell, C. R. & Wood, J. M. Measurement of blood pressure and heart rate by telemetry in conscious unrestrained marmosets. Lab Anim 29, 258–261 (1995).
Horii, I. et al. Development of telemetry system in the common marmoset–cardiovascular effects of astemizole and nicardipine. J Toxicol Sci 27, 123–130 (2002).
Moss, M. B. & Jonak, E. Cerebrovascular disease and dementia: a primate model of hypertension and cognition. Alzheimers Dement 3, S6–15 (2007).
Rothwell, P. M. et al. Effects of beta blockers and calcium-channel blockers on within-individual variability in blood pressure and risk of stroke. Lancet Neurol 9, 469–480 (2010).
Ayala, D. E. et al. Circadian pattern of ambulatory blood pressure in hypertensive patients with and without type 2 diabetes. Chronobiol Int 30, 99–115 (2013).
Bentley-Lewis, R. et al. Body mass index predicts aldosterone production in normotensive adults on a high-salt diet. J Clin Endocrinol Metab 92, 4472–4475 (2007).
Vlasova, M. et al. Role of adipokines in obesity-associated hypertension. Acta Physiol (Oxf) 200, 107–127 (2010).
Hansson, L. et al. Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the Hypertension Optimal Treatment (HOT) randomised trial. HOT Study Group. Lancet 351, 1755–1762 (1998).
Harano, Y. et al. Improvement of insulin sensitivity for glucose metabolism with the long-acting Ca-channel blocker amlodipine in essential hypertensive subjects. Metabolism 44, 315–319 (1995).
Komoda, H., Inoue, T. & Node, K. Anti-inflammatory properties of azelnidipine, a dihydropyridine-based calcium channel blocker. Clin Exp Hypertens 32, 121–128 (2010).
Kraft-Schreyer, N., Kushner, H. & Angelakos, E. T. Development of a nonhuman primate model for spontaneous hypertension. Blood pressures in first-generation offspring. Hypertension 9, III57–63 (1987).
Modi, K. K. & Chakravarti, R. N. Spontaneously occurring hypertension in wild Rhesus monkeys. Klin Wochenschr 53, 363–367 (1975).
Smith, O. A. & Astley, C. A. Naturally occurring hypertension in New World nonhuman primates: Potential role of the perifornical hypothalamus. Am J Physiol Regul Integr Comp Physiol 292, R937–945 (2007).
Sowers, J. R., Whaley-Connell, A. & Epstein, M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med 150, 776–783 (2009).
McCurley, A. et al. Direct regulation of blood pressure by smooth muscle cell mineralocorticoid receptors. Nat Med 18, 1429–1433 (2012).
Muller, J. E. et al. Circadian variation in the frequency of onset of acute myocardial infarction. N Engl J Med 313, 1315–1322 (1985).
Elliott, H. L. 24-hour blood pressure control: its relevance to cardiovascular outcomes and the importance of long-acting antihypertensive drugs. J Hum Hypertens 18, 539–543 (2004).
Parati, G., Ochoa, J. E., Lombardi, C. & Bilo, G. Assessment and management of blood-pressure variability. Nat Rev Cardiol 10, 143–155 (2013).
Pickering, T. G. The clinical significance of diurnal blood pressure variations. Dippers and nondippers. Circulation 81, 700–702 (1990).
Baumann, M. Role of advanced glycation end products in hypertension and cardiovascular risk: human studies. J Am Soc Hypertens 6, 427–435 (2012).
Vasdev, S., Gill, V. & Singal, P. Role of advanced glycation end products in hypertension and atherosclerosis: therapeutic implications. Cell Biochem Biophys 49, 48–63 (2007).
Hartog, J. W. et al. Advanced glycation end-products, anti-hypertensive treatment and diastolic function in patients with hypertension and diastolic dysfunction. Eur J Heart Fail 12, 397–403 (2010).
Monacelli, F. et al. Effects of valsartan therapy on protein glycoxidation. Metabolism 55, 1619–1624 (2006).
Saisho, Y., Komiya, N. & Hirose, H. Effect of valsartan, an angiotensin II receptor blocker, on markers of oxidation and glycation in Japanese type 2 diabetic subjects: blood pressure-independent effect of valsartan. Diabetes Res Clin Pract 74, 201–203 (2006).
Persson, F. et al. Irbesartan treatment reduces biomarkers of inflammatory activity in patients with type 2 diabetes and microalbuminuria: an IRMA 2 substudy. Diabetes 55, 3550–3555 (2006).
Nakamura, K. et al. Telmisartan inhibits expression of a receptor for advanced glycation end products (RAGE) in angiotensin-II-exposed endothelial cells and decreases serum levels of soluble RAGE in patients with essential hypertension. Microvasc Res 70, 137–141 (2005).
Levin, S., McMahon, E., John-Baptiste, A. & Bell, R. R. Prostate effect in dogs with the aldosterone receptor blocker eplerenone. Toxicol Pathol 41, 271–279 (2013).
Acknowledgements
We express our sincere appreciation to Dr. You-Tang Shen for scientific consulting, Drs Chaoqun Wu and Fei Gao for analytical support, Drs Ian Bruce, Jon K. Moon and Heping Cheng for constructive comments on the manuscript and Profs Desheng Zhu, Jiedong Zhang, Caihong Wu and Jianguo Chen for their support of the animal care program. The present study was supported by the National Science and Technology Major Projects for “Major New Drug Innovation and Development” (2013ZX09501014 and 2013ZX09507001); the National Key Basic Research Program of China (2013CB531200 and 2012CB518000); Merck Sharp & Dohme Corp.; the National Natural Science Foundation of China (81270883, 30870996, 81471063, 81170100, 81370234 and 81130073); and the Beijing Science & Technology Project (Z131100006513002).
Author information
Authors and Affiliations
Contributions
X.Z., R.P.X. and Y.Z. conceived and designed the project and experiments. Y.Z., W.Z., Y.L., J.W., Y.P., H.S., N.H., X.H., Y.D., Y.X., C.W., F.Z., J.M., J.Z., D.M., X.S. and X.Z. performed the experiments. Y.Z., C.L. and X.Z. analyzed the data. X.Z., R.P.X. and Y.Z. wrote the paper.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Zhang, Y., Zheng, W., Liu, Y. et al. Eplerenone restores 24-h blood pressure circadian rhythm and reduces advanced glycation end-products in rhesus macaques with spontaneous hypertensive metabolic syndrome. Sci Rep 6, 23957 (2016). https://doi.org/10.1038/srep23957
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep23957
- Springer Nature Limited