
Abstract
We used Mendelian randomization to estimate the causal effects of the liver enzymes, alanine aminotransferase (ALT), alkaline phosphatase (ALP) and gamma glutamyltransferase (GGT), on diabetes and cardiovascular disease, using genetic variants predicting these liver enzymes at genome wide significance applied to extensively genotyped case-control studies of diabetes (DIAGRAM) and coronary artery disease (CAD)/myocardial infarction (MI) (CARDIoGRAMplusC4D 1000 Genomes). Genetically higher ALT was associated with higher risk of diabetes, odds ratio (OR) 2.99 per 100% change in concentration (95% confidence interval (CI) 1.62 to 5.52) but ALP OR 0.92 (95% CI 0.71 to 1.19) and GGT OR 0.88 (95% CI 0.75 to 1.04) were not. Genetically predicted ALT, ALP and GGT were not clearly associated with CAD/MI (ALT OR 0.74, 95% CI 0.54 to 1.01, ALP OR 0.86, 95% CI 0.64 to 1.16 and GGT OR 1.08, 95% CI 0.97 to 1.19). We confirm observations of ALT increasing the risk of diabetes, but cannot exclude the possibility that higher ALT may protect against CAD/MI. We also cannot exclude the possibility that GGT increases the risk of CAD/MI and reduces the risk of diabetes. Informative explanations for these potentially contradictory associations should be sought.
Similar content being viewed by others


Introduction
Observational studies usually show some measures of liver function, such as alanine aminotransferase (ALT), alkaline phosphatase (ALP) and gamma glutamyltransferase (GGT), associated with higher risk of cardiovascular disease (CVD) and type 2 diabetes mellitus (T2DM). Among these liver enzymes, gamma glutamyltransferase (GGT) is most strongly positively associated with both CVD1,2 and T2DM3,4, although GGT is a non-specific marker of liver function. Alanine aminotransferase (ALT) is more clearly positively associated with T2DM4,5 than with CVD6,7 while the role of alkaline phosphatase (ALP)8,9 is unclear. Apart from the difficulties of separating out the roles of these correlated liver enzymes, observational studies are open to unmeasured confounding by factors such as alcohol use, pre-existing disease, lifestyle and socioeconomic position, making it uncertain whether liver function could be a valid target of intervention or is even etiologically relevant to these major complex chronic diseases.
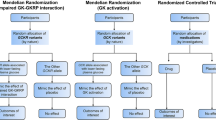
In this situation comparing the risk of CVD and T2DM by genetically determined liver function, i.e., Mendelian randomization (MR), provides a way forward. MR takes advantage of the random allocation of genetic endowment at conception to provide randomization analogous to the randomization in randomized controlled trials10,11 and is an increasingly popular means of obtaining un-confounded estimates. No previous MR study has examined the role of liver enzymes in CVD and T2DM. To clarify their roles, we assessed the association of genetically predicted liver enzymes (ALT, ALP and GGT) with ischemic heart disease (IHD) using large extensively genotyped case-control studies of coronary artery disease (CAD)/myocardial infarction (MI) and T2DM12,13,14,15. Given the role of the liver in lipid and glucose metabolism, we also similarly assessed the associations of these liver enzymes with lipids and glucose metabolism using and large extensively genotyped cross-sectional studies of lipids16 and glycemic traits17.
Results
At genome wide significance GWAS gave 4 SNPs independently predicting ALT, 14 SNPs independently predicting ALP and 26 SNPs independently predicting GGT18. One SNP, rs2954021 (TRIB1), predicted both ALT and ALP, meaning that it is pleiotropic. Supplementary Table 1 gives the information extracted for each SNP for CAD/MI and T2DM.
Genetic associations with CAD/MI
Genetically predicted ALT was not clearly associated with CAD/MI using IVW and all SNPs (see Supplementary Fig. S1b), after excluding potentially pleiotropic SNPs or using more conservative methods, although all the estimates for ALT were in the direction of lower risk but with confidence intervals including the null value (Table 1). Genetically predicted ALP was inversely associated with CAD/MI using IVW (see Supplementary Fig. S2b) or any other method, but this association was not robust to exclusion of potentially pleiotropic SNPs with the exclusion of rs579459 in ABO contributing most to the difference. Genetically predicted GGT was not clearly associated with CAD/MI using IVW (see Supplementary Fig. S3b) or any other method, although the direction was towards higher risk but the confidence intervals included the null value. There was no evidence that the MR-Egger intercepts differed from the null for the associations of ALT, ALP or GGT with CAD/MI, particularly after excluding potentially pleiotropic SNPs (Table 1).
Genetic associations with T2DM
Genetically predicted ALT was positively associated with T2DM using IVW with directionally similar estimates for most SNPs (see Supplementary Fig. S1a). The estimate was very similar after excluding potentially pleiotropic SNPs but this association was not robust to the MR-Egger method which gave much less weight to the SNP (rs2954021) from PNPLA3. Genetically predicted ALP was not clearly associated with T2DM using IVW (see Supplementary Fig. S2a). Genetically predicted GGT was inversely associated with T2DM using IVW (see Supplementary Fig. S3a), and the estimates were directionally similar using other methodological approaches, but the confidence intervals included the null value. There was no evidence that the MR-Egger intercepts differed from the null for the associations of ALT, ALP or GGT with T2DM, particularly after excluding potentially pleiotropic SNPs (Table 1).
Genetic associations with lipids and glycemic traits
Genetically predicted ALT, ALP and GGT tended to be inversely related to both LDL- and HDL- cholesterol (Table 2). Among people without diabetes, genetically predicted ALT, ALP and GGT tended to have associations with measures of glucose metabolism directionally consistent with the respective estimates for T2DM, but most confidence intervals included the null value (Table 3). There was no evidence that the MR-Egger intercepts differed from the null for the associations of ALT, ALP or GGT with lipids or glycemic traits (Tables 2 and 3).
Discussion
This novel study is consistent with most previous observational studies showing higher ALT associated with a higher risk of T2DM4,19. Our findings are also consistent with observed positive associations of GGT with ischemic heart disease (IHD)1,2. Our study is also suggestive of an inverse association of ALT with IHD, and of GGT with T2DM. As such, this study considering each liver enzyme independently has confirmed some previous observations but raised questions about the role of ALT in IHD and of GGT in diabetes which may previously have been obscured by correlations between markers of liver function.
MR provides a means of obtaining un-confounded estimates, because genetic make-up is randomly allocated at conception and so is unlikely to be influenced by confounders, such as lifestyle, heath status or socioeconomic position. The risk of chance associations generated by the underlying data structure is reduced by using separate samples for liver enzymes and the outcomes20, which is unlikely to be negated by the 5–6% overlap between the samples used to obtain genetic association with the exposures and with the outcomes. All the studies are largely of people of European descent with genomic control12,14,15,16,17,18,21,22,23 which reduces bias from hidden genetic relations. We used SNPs to predict liver enzymes which were from GWAS and were strongly associated with liver enzymes to reduce the risk of false positives. We also checked whether the SNPs used to predict liver enzymes could be associated with the outcomes directly rather than via liver enzymes and repeated the analysis with those potentially pleiotropic SNPs excluded. Nevertheless despite checking the assumptions of Mendelian randomization rigorously, limitations exist. First, given the use of separate samples we could not test whether the associations of liver enzymes with the outcomes vary by level of liver enzymes, by age or by sex, although causal relations are usually consistent. Second, we cannot be certain that the SNPs do not have unknown direct effects on IHD and T2DM. We excluded SNPs with known pleiotropic effects including the SNP (rs2954021) that predicted both ALT and ALP and the estimates were similar for GGT and ALT but less so for ALP, because of the role of rs579459 from the ABO gene. Third, estimates may be sensitive to analytic choices, but were generally similar, using weighted median estimates, although the MR-Egger estimates had much wider confidence intervals but gives consistent estimates in the unlikely event of all SNPs being invalid but satisfying the InSIDE assumption24. Although the exact functionality of all the SNPs used to predict liver enzymes is not entirely clearly, some of them are expressed in the liver, for example all the 4 SNPs (rs738409 (PNPLA3), rs2954021 (TRIB1), rs6834314 (MAPK10, HSD17B1) and rs10883437 (CPN1)) related to ALT are expressed mainly in liver according to data in the Human Protein Altas (http://www.proteinatlas.org/)25,26, making a causal role plausible and making MR-Egger estimates very conservative24. Fourth, canalization, i.e., compensatory mechanisms that drive some of the association of genetic variants with liver enzymes, might result in different associations in MR than would be obtained from interventions changing liver enzymes. However, whether such canalization exists is unknown. Fifth, GGT, ALT and ALP are not only markers of liver disease but are also affected by bone diseases (Paget disease, osteomalacia, rickets), primary and secondary hyperparathyroidism, kidney and pancreatic dysfunction (GGT is primarily present in these cells) and drug use (phenobarbital and phenytoin), so although the estimates represent the effects of each specific liver enzyme they may not only represent liver function27,28.
The findings for these liver enzymes concerning T2DM show some consistency with observational studies, where ALT is usually positively associated with T2DM4,5 and has been found associated with death from diabetes related causes29. ALT is thought to cause diabetes via insulin resistance30 with hepatic steatosis aggravating insulin resistance and creating a vicious cycle31. Consistent with this hypothesis genetically predicted ALT also showed indications of a positive association with insulin resistance (Table 3). However, the reason for ALT causing insulin resistance remains elusive. Observationally, ALP is not clearly associated with T2DM11,32, consistent with these results. Observationally, GGT is also usually positively associated with diabetes3,4, even using methods that enable correlated exposures, such as liver enzymes to be disentangled4. However, our analysis suggests the association for genetically predicted GGT might be in the other direction; confirmation of this result is required.
The findings for the associations of genetically predicted ALT and GGT with IHD are somewhat consistent with observational studies. GGT is often positively associated with IHD1,2, and our findings are consistent with this interpretation, although the confidence intervals included the null value. ALT usually has a neutral association with IHD6, our findings are consistent with a neutral association but cannot rule out an inverse association. The findings for the association of genetically predicted ALP with IHD are difficult to interpret because the negative association depends on rs579459 (near ABO) when the reasons for blood groups being associated with IHD are not currently fully understood. It is not clear whether rs579459 is operating via alterations in liver function, is directly functionally relevant to IHD by some yet to be identified mechanism or is a correlate of other factors directly causing IHD.
Overall, these findings indicate complex relations of liver enzymes with IHD and diabetes that may be directionally different even though diabetes is a strong risk factor for IHD. However, it has recently been discovered that key causal factors for IHD may have directionally different relations with IHD and diabetes, such as LDL cholesterol or statins33,34, which clearly has important implications for prevention and treatment of both conditions. No accepted mechanistic explanation for these paradoxical relation exists, a mechanism via LDL receptor-mediated transmembrane cholesterol transport has been suggested35, which is plausible but does not clearly relate to liver function. We have previously suggested a mechanism via sex hormones36. Sex hormone receptors are expressed in the liver37 and the liver is an important site for sex hormone metabolism38 and catabolism39,40. Randomized controlled trials have shown that estrogen reduces the risk of diabetes41 and testosterone improves glucose metabolism42,43; regulators have warned of the cardiovascular risk of testosterone44. However, such an explanation might not explain the different effects of statins, because uncertainties remain as to whether statins affect the liver or cause liver injury or dysfunction45, although statins lower sex hormones46.
This novel Mendelian randomization study has confirmed some observations concerning poorer liver function, such as ALT likely causing diabetes, but has also raised the possibility of complex effects on IHD. Liver function has complex enzyme and disease specific effects on major non-communicable diseases. Greater understanding of the underlying etiology is needed. As such whether intervening on liver function would improve diabetes without affecting its major consequence, i.e., cardiovascular disease, is unclear. This study also shows the importance of using genetic evidence to identify and select targets of intervention, but leaves several unanswered questions concerning the role of liver function in diabetes and cardiovascular disease. Further investigation is required.
Methods
Genetically predicted liver enzymes
Single nucleotide polymorphisms (SNPs) strongly associated with ALT, ALP and GGT at genome wide significance (p-value < 5 × 10−8) were obtained from genome wide association studies (GWAS). Any highly correlated SNPs (in linkage disequilibrium) (r2 ≥ 0.8) were discarded to retain SNPs with a smaller p-value and/or larger effect size. SNP Annotation and Proxy Search (http://www.broad.mit.edu/mpg/snap/ldsearchpw.php) was used to ascertain these correlations (linkage disequilibrium) using the same catalog as the relevant GWAS. Whether any of the selected SNPs were related to CAD/MI or T2DM directly rather than through liver enzymes (pleiotropic effects) was assessed from their known traits/phenotypes obtained from a comprehensive genotype to phenotype cross-reference, Ensembl (http://www.ensembl.org/index.html).
Genetically predicted CAD/MI, diabetes, lipids and glycemic traits
Data on CAD/MI have been contributed by CARDIoGRAMplusC4D investigators and have been downloaded from www.CARDIOGRAMPLUSC4D.ORG. CARDIoGRAMplusC4D provides two large overlapping case-control studies largely in people of European descent, one genotyped using 1000 Genomes (60,801 CAD cases, 123,504 controls) and the other genotyped using Hapmap with limited genotyping (63,746 CAD/MI, 130,681 controls) but with more extensive genotyping for a subset (22,233 CAD/MI cases, 64,762 controls)12,14,22. Genetic associations with T2DM are from an extensively genotyped case (n = 34,840)-control (n = 114,981) study largely of people of European descent from the DIAbetes Genetics Replication and Meta-analysis consortium, http://diagramconsortium.org/index.html.15 Genetic associations with lipids (inverse normal transformed effect sizes) are from the Global Lipids Genetic Consortium Results of 188,577 people mainly of European ancestry http://csg.sph.umich.edu//abecasis/public/lipids2013/ including low-density lipoprotein (LDL)- cholesterol, high-density lipoprotein (HDL)-cholesterol and triglycerides16. Data on glycemics glycemic traits, including glycated hemoglobin (HbA1c) (%) (n = 46,368)23, fasting glucose (FG) (mmol/L) (n = 122,743)17, log transformed β-cell function (HOMA-B) (n = 98,372)17, and insulin resistance (HOMA-IR) (n = 98,372)17, are in people of European descent without diabetes, and have been contributed by MAGIC investigators and have been downloaded from www.magicinvestigators.org.
Statistical analyses
Un-confounded estimates of the association of each liver enzyme with CAD/MI, T2DM, lipids and glycemic traits were obtained from separate sample instrumental variable analysis by combining SNP-specific Wald estimates47, with the standard error approximated using Fieller’s theorem48, using inverse variance weighting (IVW) with fixed effects49. The Wald estimate is the ratio of the estimate of SNP on outcome to SNP on liver enzyme.
Sensitivity analyses
We conducted two sensitivity analyses to assess whether the estimates were robust to methodological choices. First, we repeated the analysis excluding SNPs that might be associated with the relevant outcome directly rather than via liver enzymes, i.e., pleiotropic effects which might violate the exclusion-restriction assumption of instrumental variable analysis. Second, when each SNP contributed less than 50% of the weight, we used a weighted median estimate which may generate correct estimates even when 50% of the SNPs included violate the instrumental variable assumptions50. When a single SNP contributed more than 50% we used MR-Egger regression because it may generate correct estimates even when all the SNPs are invalid instruments as long as the instrument strength independent of direct effect (InSIDE) assumption is satisfied24. We also examined the value of the intercept term from the MR-Egger regression which gives the average directional pleiotropic effect across genetic variants, i.e., the average direct effect of a variant on the outcome. A p-value of <0.05 indicates the presence of directional pleiotropy across the genetic variants included in the analysis50. MR-Egger has a lower false positive rate than IVW but a higher false negative rate24.
All statistical analyses were conducted using Stata version 13.1 (StataCorp LP, College Station, TX) and R version 3.3.0 (R Foundation for Statistical Computing, Vienna, Austria). Ethical approval from an Institutional Review Board is not required, since this study only uses publicly available data.
Additional Information
How to cite this article: Liu, J. et al. Liver Enzymes and Risk of Ischemic Heart Disease and Type 2 Diabetes Mellitus: A Mendelian Randomization Study. Sci. Rep. 6, 38813; doi: 10.1038/srep38813 (2016).
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
Fraser, A. et al. Gamma-glutamyltransferase is associated with incident vascular events independently of alcohol intake: analysis of the British Women’s Heart and Health Study and Meta-Analysis. Arteriosclerosis, thrombosis, and vascular biology 27, 2729–2735, doi: 10.1161/ATVBAHA.107.152298 (2007).
Ghouri, N., Preiss, D. & Sattar, N. Liver enzymes, nonalcoholic fatty liver disease, and incident cardiovascular disease: a narrative review and clinical perspective of prospective data. Hepatology (Baltimore, Md.) 52, 1156–1161, doi: 10.1002/hep.23789 (2010).
Kunutsor, S. K., Abbasi, A. & Adler, A. I. Gamma-glutamyl transferase and risk of type II diabetes: an updated systematic review and dose-response meta-analysis. Annals of epidemiology 24, 809–816, doi: 10.1016/j.annepidem.2014.09.001 (2014).
Xu, L. et al. Liver enzymes and incident diabetes in China: a prospective analysis of 10 764 participants in the Guangzhou Biobank Cohort Study. Journal of epidemiology and community health 69, 1040–1044, doi: 10.1136/jech-2015-205518 (2015).
Sattar, N. et al. Elevated alanine aminotransferase predicts new-onset type 2 diabetes independently of classical risk factors, metabolic syndrome, and C-reactive protein in the west of Scotland coronary prevention study. Diabetes 53, 2855–2860 (2004).
Ford, I. et al. The inverse relationship between alanine aminotransferase in the normal range and adverse cardiovascular and non-cardiovascular outcomes. International journal of epidemiology 40, 1530–1538, doi: 10.1093/ije/dyr172 (2011).
Ruhl, C. E. & Everhart, J. E. Elevated serum alanine aminotransferase and gamma-glutamyltransferase and mortality in the United States population. Gastroenterology 136, 477–485 e411, doi: 10.1053/j.gastro.2008.10.052 (2009).
Kunutsor, S. K. et al. Serum Alkaline Phosphatase and Risk of Incident Cardiovascular Disease: Interrelationship with High Sensitivity C-Reactive Protein. PloS one 10, e0132822, doi: 10.1371/journal.pone.0132822 (2015).
Malenica, M. et al. Use of Databases for Early Recognition of Risk of Diabetic Complication by Analysis of Liver Enzymes in Type 2 Diabetes Mellitus. Acta informatica medica: AIM: journal of the Society for Medical Informatics of Bosnia & Herzegovina: casopis Drustva za medicinsku informatiku BiH 24, 90–93, doi: 10.5455/aim.2016.24.90-93 (2016).
Lawlor, D. A., Harbord, R. M., Sterne, J. A., Timpson, N. & Davey Smith, G. Mendelian randomization: using genes as instruments for making causal inferences in epidemiology. Statistics in medicine 27, 1133–1163, doi: 10.1002/sim.3034 (2008).
Goldberg, D. M., Martin, J. V. & Knight, A. H. Elevation of serum alkaline phosphatase activity and related enzymes in diabetes mellitus. Clinical biochemistry 10, 8–11 (1977).
Schunkert, H. et al. Large-scale association analysis identifies 13 new susceptibility loci for coronary artery disease. Nature genetics 43, 333–338, doi: 10.1038/ng.784 (2011).
The Coronary Artery Disease (C4D) Genetics Consortium. A genome-wide association study in Europeans and South Asians identifies five new loci for coronary artery disease. Nature genetics 43, 339–344, doi: 10.1038/ng.782 (2011).
The CARDIoGRAMplusC4D Consortium. Large-scale association analysis identifies new risk loci for coronary artery disease. Nature genetics 45, 25–33, doi: 10.1038/ng.2480 (2013).
Morris, A. P. et al. Large-scale association analysis provides insights into the genetic architecture and pathophysiology of type 2 diabetes. Nature genetics 44, 981–990, doi: 10.1038/ng.2383 (2012).
Global Lipids Genetics, C. Discovery and refinement of loci associated with lipid levels. Nature genetics 45, 1274–1283, doi: 10.1038/ng.2797http://www.nature.com/ng/journal/v45/n11/abs/ng.2797.html#supplementary-information (2013).
Dupuis, J. et al. New genetic loci implicated in fasting glucose homeostasis and their impact on type 2 diabetes risk. Nature genetics 42, 105–116, doi: 10.1038/ng.520 (2010).
Chambers, J. C. et al. Genome-wide association study identifies loci influencing concentrations of liver enzymes in plasma. Nature genetics 43, 1131–1138, doi: 10.1038/ng.970 (2011).
Goessling, W. et al. Aminotransferase levels and 20-year risk of metabolic syndrome, diabetes, and cardiovascular disease. Gastroenterology 135, 1935–1944, 1944 e1931, doi: 10.1053/j.gastro.2008.09.018 (2008).
Taylor, A. E. et al. Mendelian randomization in health research: using appropriate genetic variants and avoiding biased estimates. Economics and human biology 13, 99–106, doi: 10.1016/j.ehb.2013.12.002 (2014).
Devlin, B. & Roeder, K. Genomic control for association studies. Biometrics 55, 997–1004 (1999).
Nikpay, M. et al. A comprehensive 1,000 Genomes-based genome-wide association meta-analysis of coronary artery disease. Nature genetics 47, 1121–1130, doi: 10.1038/ng.3396 (2015).
Soranzo, N. et al. Common variants at 10 genomic loci influence hemoglobin A(1)(C) levels via glycemic and nonglycemic pathways. Diabetes 59, 3229–3239, doi: 10.2337/db10-0502 (2010).
Burgess, S., Bowden, J., Fall, T., Ingelsson, E. & Thompson, S. G. Sensitivity analyses for robust causal inference from Mendelian randomization analyses with multiple genetic variants. Epidemiology (Cambridge, Mass.) (2016).
Human Protein Atlas available from www.proteinatlas.org.
Uhlen, M. et al. Proteomics. Tissue-based map of the human proteome. Science (New York, N.Y.) 347, 1260419, doi: 10.1126/science.1260419 (2015).
Burtis, C. Tietz Textbook of Clinical Chemistry. (ER Ashwood. Philadelphia, WB Saunders Company, 1994).
Ashwood, B. a. Tietz NW: Textbook of Clinical Chemistry. Third edition edn, (PA, WB Saunders Company, Philadelphia, 1999).
Schooling, C. M., Kelvin, E. A. & Jones, H. E. Alanine transaminase has opposite associations with death from diabetes and ischemic heart disease in NHANES III. Annals of epidemiology 22, 789–798, doi: 10.1016/j.annepidem.2012.08.003 (2012).
Jacobs, M. et al. The association between the metabolic syndrome and alanine amino transferase is mediated by insulin resistance via related metabolic intermediates (the Cohort on Diabetes and Atherosclerosis Maastricht [CODAM] study). Metabolism: clinical and experimental 60, 969–975, doi: 10.1016/j.metabol.2010.09.006 (2011).
Lonardo, A., Lombardini, S., Ricchi, M., Scaglioni, F. & Loria, P. Review article: hepatic steatosis and insulin resistance. Alimentary pharmacology & therapeutics 22 Suppl 2, 64–70, doi: 10.1111/j.1365-2036.2005.02600.x (2005).
Tibi, L., Collier, A., Patrick, A. W., Clarke, B. F. & Smith, A. F. Plasma alkaline phosphatase isoenzymes in diabetes mellitus. Clinica chimica acta; international journal of clinical chemistry 177, 147–155 (1988).
Fall, T. et al. Using Genetic Variants to Assess the Relationship Between Circulating Lipids and Type 2 Diabetes. Diabetes 64, 2676–2684, doi: 10.2337/db14-1710 (2015).
Swerdlow, D. I. et al. HMG-coenzyme A reductase inhibition, type 2 diabetes, and bodyweight: evidence from genetic analysis and randomised trials. Lancet (London, England) 385, 351–361, doi: 10.1016/S0140-6736(14)61183-1 (2015).
Besseling, J., Kastelein, J. J., Defesche, J. C., Hutten, B. A. & Hovingh, G. K. Association between familial hypercholesterolemia and prevalence of type 2 diabetes mellitus. Jama 313, 1029–1036, doi: 10.1001/jama.2015.1206 (2015).
Schooling, C. M., Au Yeung, S. L. & Leung, G. M. Why do statins reduce cardiovascular disease more than other lipid modulating therapies? European journal of clinical investigation 44, 1135–1140, doi: 10.1111/eci.12342 (2014).
Pelletier, G. Localization of androgen and estrogen receptors in rat and primate tissues. Histology and histopathology 15, 1261–1270 (2000).
Tsuchiya, Y., Nakajima, M. & Yokoi, T. Cytochrome P450-mediated metabolism of estrogens and its regulation in human. Cancer letters 227, 115–124, doi: 10.1016/j.canlet.2004.10.007 (2005).
Chouinard, S. et al. Inactivation by UDP-glucuronosyltransferase enzymes: the end of androgen signaling. The Journal of steroid biochemistry and molecular biology 109, 247–253, doi: 10.1016/j.jsbmb.2008.03.016 (2008).
Raftogianis, R., Creveling, C., Weinshilboum, R. & Weisz, J. Chapter 6: Estrogen Metabolism by Conjugation. JNCI Monographs 2000, 113–124 (2000).
Margolis, K. L. et al. Effect of oestrogen plus progestin on the incidence of diabetes in postmenopausal women: results from the Women’s Health Initiative Hormone Trial. Diabetologia 47, 1175–1187, doi: 10.1007/s00125-004-1448-x (2004).
Hou, W. W., Tse, M. A., Lam, T. H., Leung, G. M. & Schooling, C. M. Adolescent testosterone, muscle mass and glucose metabolism: evidence from the ‘Children of 1997’ birth cohort in Hong Kong. Diabetic medicine: a journal of the British Diabetic Association 32, 505–512, doi: 10.1111/dme.12602 (2015).
Grossmann, M., Hoermann, R., Wittert, G. & Yeap, B. B. Effects of testosterone treatment on glucose metabolism and symptoms in men with type 2 diabetes and the metabolic syndrome: a systematic review and meta-analysis of randomized controlled clinical trials. Clinical endocrinology 83, 344–351, doi: 10.1111/cen.12664 (2015).
Schooling, C. M. & Leung, G. M. Testosterone and cardiovascular risk. The lancet. Diabetes & endocrinology 3, 682, doi: 10.1016/S2213-8587(15)00281-8 (2015).
Banach, M. et al. Statin intolerance - an attempt at a unified definition. Position paper from an International Lipid Expert Panel. Archives of medical science: AMS 11, 1–23, doi: 10.5114/aoms.2015.49807 (2015).
Schooling, C. M., Au Yeung, S. L., Freeman, G. & Cowling, B. J. The effect of statins on testosterone in men and women, a systematic review and meta-analysis of randomized controlled trials. BMC medicine 11, 57, doi: 10.1186/1741-7015-11-57 (2013).
Wald, A. The Fitting of Straight Lines if Both Variables are Subject to Error. The Annals of Mathematical Statistics 11, 284–300, doi: 10.1214/aoms/1177731868 (1940).
Fieller, E. C. Some Problems in Interval Estimation. Journal of the Royal Statistical Society. Series B: Methodological 16(2), 175–185 (1954).
Burgess, S. et al. Using published data in Mendelian randomization: a blueprint for efficient identification of causal risk factors. European journal of epidemiology 30, 543–552, doi: 10.1007/s10654-015-0011-z (2015).
Bowden, J., Davey Smith, G., Haycock, P. C. & Burgess, S. Consistent Estimation in Mendelian Randomization with Some Invalid Instruments Using a Weighted Median Estimator. Genet Epidemiol 40, 304–314, doi: 10.1002/gepi.21965 (2016).
Acknowledgements
Data on coronary artery disease/myocardial infarction have been contributed by CARDIoGRAMplusC4D investigators and have been downloaded from www.CARDIOGRAMPLUSC4D.ORG. Data on glycaemic traits have been contributed by MAGIC investigators and have been downloaded from www.magicinvestigators.org. We thank all authors that contributed to the databases we used including DIAGRAM GWAS, Global Lipids Genetics Consortium Results and The Human Protein Atlas. This study only uses publicly available data and involves no funding source.
Author information
Authors and Affiliations
Contributions
J.X. Liu conducted the literature review, the analysis and drafted the manuscript. S.L. Lin checked the analysis. S.L. Au Yeung and C.M. Schooling conceptualized ideas, designed and directed the analytic strategy and supervised the study from conception to completion, with assistance from G.M. Leung. S.L. Au Yeung, S.L. Lin and C.M. Schooling revised drafts of the manuscript. All the authors contributed to the interpretation of the data, critically revising the paper and approval of the final version.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Liu, J., Au Yeung, S., Lin, S. et al. Liver Enzymes and Risk of Ischemic Heart Disease and Type 2 Diabetes Mellitus: A Mendelian Randomization Study. Sci Rep 6, 38813 (2016). https://doi.org/10.1038/srep38813
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep38813
- Springer Nature Limited
This article is cited by
-
Gamma-glutamyltransferase, arterial remodeling and prehypertension in a healthy population at low cardiometabolic risk
Journal of Human Hypertension (2021)
-
Serum alkaline phosphatase levels and the risk of new-onset diabetes in hypertensive adults
Cardiovascular Diabetology (2020)
-
A phenome-wide association study of ABO blood groups
BMC Medicine (2020)
-
The effect of liver enzymes on adiposity: a Mendelian randomization study
Scientific Reports (2019)
-
Early maternal circulating alkaline phosphatase with subsequent gestational diabetes mellitus and glucose regulation: a prospective cohort study in China
Endocrine (2019)