
Abstract
The discounting of delayed rewards, also known as temporal or delay discounting, is intrinsic to everyday decisions and can be impaired in pathological states such as addiction disorders. Preclinical and human studies suggest a role for dopaminergic function in temporal discounting but this relationship has not yet been verified using molecular imaging of the living human brain. Here, we evaluated dopaminergic function in temporal discounting using positron emission tomography (PET) with two different dopaminergic ligands assessing three populations in whom temporal discounting has been shown to be impaired. First, we show using [11C]raclopride PET that in pathological gamblers, greater temporal discounting correlates with decreased ventral striatal binding potential, convergent with translational findings of lower nucleus accumbens D2/D3 receptor density in high-impulsive rodents. Temporal discounting also correlates with lower ventral striatal dopamine release in response to high-reward magnitude suggesting that dopamine-mediated devaluation of larger delayed rewards may drive choice preferences. Second, we show using [18F]fluorodopa PET that in Parkinson’s disease, temporal discounting correlates with greater left caudate dopaminergic terminal function. Finally, in subjects with Parkinson’s disease and dopamine medication-induced behavioral addictions, temporal discounting is further correlated with greater dopaminergic terminal function in the anterior putamen. These findings provide insights into the relationship between striatal dopamine function and temporal discounting, and its potential role in pathological disorders and mechanisms underlying treatment interventions.
Similar content being viewed by others

Introduction
The weighting of choices as a function of time is intrinsic to everyday decisions. These choices include daily decisions, about whether to diet, to fit into a swimsuit for the summer or more substantial decisions, such as choosing to stay in school for future career plans. Delay or temporal discounting is a form of decisional impulsivity characterized by a choice of an immediate smaller reward over a larger delayed reward. Temporal discounting can be measured using intertemporal choice tasks in which subjects choose between immediate and larger delayed rewards.1 There is much interindividual variability and the discounting of delayed rewards is a core impairment across diverse behavioral addictions (BA), such as pathological gambling (PG), and substance addictions in humans.2 In rodents, greater temporal discounting predicts the inability to inhibit nicotine seeking during abstinence and greater sensitivity to nicotine cues,3 faster acquisition of cocaine self-administration,4 persistent cocaine seeking during extinction and greater context-associated relapse.5 Greater temporal discounting has also been shown to be increased in Parkinson’s disease (PD) patients compared with healthy volunteers6 suggesting that there may be a potential pathophysiological role for the neurobiology of PD in temporal discounting, although psychosocial mechanisms are likely to contribute as well.7 Furthermore, PD patients with dopaminergic medication-related PG or compulsive shopping have been shown to have greater temporal discounting compared with those without BAs.8, 9, 10
Converging evidence implies a role for dopamine in temporal discounting. Single-unit striatal recordings in primates during the presentation of reward-predicting stimuli show that dopaminergic activity increases monotonically with magnitude and also decreases with delay to reflect the subjective devaluation of the delayed reward.11 Greater temporal discounting is also associated with lower dopamine reactivity in the nucleus accumbens core and shell measured using electrically evoked dopamine release.3 Nucleus accumbens lesions are also associated with increased temporal discounting.12 These observations suggest that enhanced temporal discounting may be associated with a decrease in endogenous dopaminergic activity.
The relationship to exogenously administered dopamine is more complex. Acute administration of low and moderate doses of amphetamine has been shown to decrease impulsive choice in rodents.13, 14, 15 In contrast, high chronic doses of methamphetamine and cocaine also increase impulsive choice in rodents,14, 16 which may be related either to a dose related effect or chronic adaptation. Similarly, levodopa, a precursor to dopamine, is associated with increased impulsive choice in healthy humans17 and increased delay aversion in PD patients.18
Taken together, this evidence suggests a possible role for a U-shaped curve in the relationship between dopamine and temporal discounting.19 Lower endogenous dopamine levels in preclinical studies and lower dopaminergic tone in PD patients are associated with greater temporal discounting. Acute administration of low and moderate doses and chronic high doses of exogenously administered drugs may have differential effects on temporal discounting dependent on how the administration shifts dopaminergic activity on this U-shaped curve.
Previous [11C]raclopride studies, including our earlier studies based on this imaging data, have remained inconclusive about group differences in striatal dopamine function in PG patients compared with healthy volunteers.20, 21 However, in PD patients, BAs seem to be related with increased cue- and reward-related striatal dopamine release22, 23 and lower dopamine transporter density,24, 25 but not with alterations in striatal dopamine synthesis capacity as shown in our earlier study from this sample.26
Here, we focus on the relationship between temporal discounting and measures of striatal dopamine function. We assess disorders shown to have abnormal temporal discounting, including PG subjects and PD subjects with and without BAs. Our first study focused on interindividual differences in temporal discounting and their relationship with [11C]raclopride PET in healthy volunteers and PG subjects. Subjects were tested with a baseline control and a gambling task with reward magnitude manipulation. Greater temporal discounting has been shown to correlate with premature or anticipatory responding,27 which is associated with lower nucleus accumbens D2/D3 receptor density in rodents without any associated changes in presynaptic dopamine release at baseline.28 Thus, we hypothesize that greater temporal discounting is associated with lower ventral striatal D2/D3 receptor density.
In the second study, we assessed the relationship between temporal discounting and striatal dopamine terminal function, which reflects dopamine synthesis capacity (aromatic amino acid carboxylase activity), by measuring the [18F]fluorodopa PET at rest.29 We investigated interindividual differences in temporal discounting in patients with PD with and without medication-induced BAs. Previous studies with [11C]raclopride PET have shown that PD patients with BAs have enhanced presynaptic striatal dopamine release in response to a gambling task or reward-related cues.22, 23 We hypothesized that greater temporal discounting would be associated with higher dopamine function particularly in PD subjects with BAs.
Materials and methods
Subjects
Twelve pathological gamblers, 12 healthy volunteers and 20 PD patients with (n=10) and without (n=10) medication-induced BAs participated in the study. The group comparisons of the imaging data between gamblers and healthy volunteers, and PD patients with and without BAs have been published earlier.20, 26 All subjects were male. For PD patients, the diagnosis had been established by a neurologist according to the UK Brain Bank Criteria30 and BA diagnoses were made by a consultant psychiatrist (SN) according to previously published criteria.31 The BAs in PD patients included PG in five patients, hypersexuality in four patients and binge eating disorder in one patient. All BAs had emerged following the initiation of dopamine replacement therapy and were active during the study. PD subjects were tested behaviorally on medication. Dementia, substance dependence, major axis-I disorders, clinically relevant medical conditions, medications known to affect dopamine function and substance use within 36 h or caffeine consumption within 12 h before the PET imaging were considered as exclusion criteria. The studies received approval from the local ethical committee, informed written consent was obtained and the study was conducted according to the principles of the Declaration of Helsinki.
Temporal discounting
Temporal discounting was assessed using a 27-item monetary choice questionnaire,1 where subjects were asked to choose between an immediate reward and a larger delayed reward. The hyperbolic temporal discounting rate k can be calculated with the formula (1)

where V is the present value of the delayed reward A at delay D. To estimate the magnitude effect, delayed rewards were divided into small, medium and large delayed rewards.1 The indifference points of the k-values were established and the k-value calculated as the geometric mean of the three magnitude categories. The subjects were instructed to carefully make the choices as they would in real life situations. Written instructions were given and the task was also explained by one of the investigators (J. Joutsa). Two PD subjects (one patient with pathological gambling and one without BAs) were excluded from the analyses because they had more than two choices inconsistent with their temporal discount rate in one or more of the reward magnitude categories.32 In addition, the task was too hard for one patient without BAs with cognitive impairment (Mini-Mental State Examination score of 22), leaving 17 PD patients in the final sample.
Imaging
All subjects underwent a 1.5T brain MRI scan to provide a structural reference for PET image analyses and to exclude structural brain abnormalities. T1, T2, DWI and FLAIR sequences were obtained and inspected by a consultant neuroradiologist.
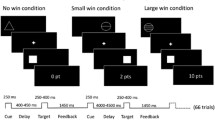
The PG and healthy volunteer subjects were scanned repeatedly under different conditions (a control task and two gambling tasks with a slot machine) with [11C]raclopride PET on the same day, and the order of the scans was fully counter balanced. The control task included pressing buttons A and B when lit with combined auditory stimulus, but without any gambling-related cues or monetary gain/loss. In the gambling tasks, subjects were instructed to gamble with ecologically valid slot machine software under two scenarios: high reward and low reward. The magnitude (but not the frequency) of wins was modified, resulting in a mean payback rate of 371% in the high-reward task and 93% in the low-reward task. The subjects were blinded to the gambling task outcomes. The tasks have been described in detail previously.20
PD patients were scanned once with [18F]fluorodopa in the resting condition in off-medication state. All dopaminergic medications were discontinued at least 12 h (24 h for extended release medications) before the tracer injection and a 150 mg oral dose of carbidopa was given 1 h before [18F]fluorodopa bolus administration to prevent peripheral decarboxylation of the tracer.
[11C]raclopride scanning was performed using GE Advance (General Electric Medical Systems, Milwaukee, WI, USA) and [18F]fluorodopa scanning using Siemens ECAT EXACT HR+ (Siemens, Münich, Germany) scanner, and preprocessing performed using Statistical Parametric Mapping (SPM8; Wellcome Department of Cognitive Neurology, London, UK; http://www.fil.ion.ucl.ac.uk/spm/) software, as described earlier.20, 26 Briefly, between-frame motion was corrected, and images were coregistered with individual structural images using the mutual information algorithm, and the images were normalized to Montreal Neurological Institute standard space using the structural information of the T1-weighted MR images. Regions of interest (ROIs) were drawn with Carimas software (version 2.0, Turku PET Centre, Turku, Finland) on the normalized T1-weighted MR images including the ventral striatum, caudate and putamen. The subdivision of the striatum was performed as described my Mawlawi et al.33 In addition, for [18F]fluorodopa images of PD patients, the putamen was divided into anterior and posterior parts. [18F]fluorodopa uptake (Kiref) was quantified by applying the Patlak plot to data from 15 to 90 min from the injection using the occipital cortex as the reference region.34 [11C]raclopride non-displaceable binding potential (BPND) was calculated using the simplified reference tissue model with cerebellar cortex as the reference region.35
Dopamine release was estimated from the change in [11C]raclopride BPND between the control and gambling task using the formula (2):

Thus, as [11C]raclopride competes for binding sites with dopamine, positive ΔBPND were considered to indicate endogenous dopamine release in the corresponding striatal subregion.36
Statistical analyses
The normality of the distributions was estimated by visual inspection of the histograms and using Shapiro–Wilk tests. Differences between the groups were analyzed using Student’s t-tests or Mann–Whitney U-tests, when appropriate. Within-subject differences were examined using paired t-tests or Wilcoxon signed-rank order tests. The differences in temporal discounting between the reward magnitude categories were tested using Friedman’s analysis of variance. The associations between striatal dopamine synthesis capacity and temporal discounting were analyzed with Spearman’s rank order correlation coefficients. Group differences in correlation coefficients were investigated using Fisher’s r-to-z transformations, which can also be applied for nonparametric tests. Due to the distribution of temporal discounting k-values and the number of subjects, logistic regression analyses or partial correlation analyses could not be performed. Instead, potential confounding variables were tested using Spearman correlation analyses. The statistical analyses were performed with PASW Statistics (version 19; SPSS, Chicago, IL, USA) and P-values <0.05 were considered statistically significant.
The issue of multiple comparisons due to several analyzed brain regions was addressed by voxel-wise analyses using Statistical nonParametric Mapping (SnPM5) run in SPM8. The images were smoothed with an 8 mm Gaussian kernel. Simple regression analyses were conducted using 10 mm variance smoothing. The analyses were restricted to the striatum and family-wise error (FWE) corrected P-values <0.05 were considered statistically significant.
Results
Demographics
The demographic data and discounting rates are presented in Table 1. The temporal discounting rate did not correlate with age, duration of PG, SOGS score or age of PG onset in PG or healthy volunteers. However, in PD patients, temporal discounting correlated with age (r=−0.68, P=0.003) and age of PD onset (r=−0.66, P=0.006) but not with PD duration, Unified Parkinson’s Disease Rating Scale off-motor score, levodopa equivalent daily dose or dopamine agonist levodopa equivalent daily dose. Subject age and age of PD onset were strongly intercorrelated (r=0.96, P<0.001).
[11C]raclopride binding and dopamine release
In Study 1, in the entire sample (n=24), there was a negative correlation between k-value and the bilateral ventral striatum BPND (r=−0.44, P=0.03; Figure 1), which was verified in voxel-wise analyses (FWE corrected P<0.05, cluster extent 34 voxels, peak pseudo-T=3.58 at −9 15 −9). The correlation was, however, significantly different between groups (z=3.36, P<0.001), and it was observed in PG (r=−0.89, P<0.001) but not in healthy volunteers (r=0.15, P=0.65; Figure 1). Again, the findings were confirmed using voxel-wise analysis revealing a significant cluster in PG but not in healthy volunteers (Figure 2). The BPND in the right ventral striatum (ipsilateral to the hand controlling the sensorimotor task in all except one subject) was lower compared with the left side (mean (s.d.) 2.15 (0.29) vs 2.37 (0.29), P<0.001). In addition, the caudate BPND correlation with k-value differed between the groups (z=2.15, P=0.03), but k-value did not correlate with BPND in either of the groups (r=−0.46, P=0.13 in gamblers; and r=0.47, P=0.12 in controls). In the voxel-wise analysis, there was also a correlation in the PG group, but not in the control group, in the left dorsal caudate in addition to the ventral striatum (Figure 2).

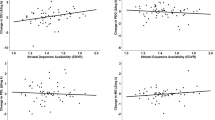
Temporal discounting and dopamine function in the ventral striatum. Spearman nonparametric correlations between temporal discounting rate (k) and dopamine release (Vstr dBPND; positive values indicate dopamine release) in pathological gamblers (a) and controls (b). Correlations between the baseline ventral striatum D2/D3 availability (Vstr BPND) and k in pathological gamblers (c) and controls (d). Solid circles represent PG subjects. Open circles represent healthy volunteers. BPND, non-displaceable binding potential; Vstr, ventral striatum; PG, pathological gambling.

Lower ventral striatal D2/D3 binding associated with higher temporal discounting. The t-values for negative correlation between [11C]raclopride BPND and overall temporal discounting rate k in PG subjects (n=12) overlaid on the average T1-weighted image of the studied sample in Study 1. The images are thresholded to PFWE<0.05, showing clusters of 147 voxels with peak pseudo-T 4.06 at 12, 15, 7 and 126 voxels with peak pseudo-T 4.03 at −10 16 −2. Pseudo-T values are indicated with a red–yellow scale. The images are displayed in radiological convention (that is, the right side of the image corresponds to the left side of the patient) and coordinates are in Montreal Neurological Institute space (mm). BPND, non-displaceable binding potential; FWE, family-wise error.
Temporal discounting values correlated negatively with high-reward ΔBPND (that is, the higher the k-value, the lower the dopamine release) in the bilateral ventral striatum over the whole sample (r=−0.45, P=0.03). The correlation was observed only in PG (r=−0.70, P=0.01; control group r=−0.01, P=0.98; Figure 1). However, the difference in correlation coefficients between the groups did not reach statistical significance (z=1.84, P=0.07). There were no correlations between temporal discounting and ΔBPND in other regions in the high-reward task or any of the ROIs in the low-reward task.
[18F]fluorodopa uptake
In Study 2, there was a positive correlation between k-value and [18F]fluorodopa Kiref in the left caudate nucleus over the whole sample (r=0.64, P=0.005; Figure 3). The correlation between k-value and [18F]fluorodopa uptake was also significant in the left anterior putamen (r=0.51, P=0.04). There were no correlations between k-value and [18F]fluorodopa uptake in other ROIs. The correlation was verified and spatial extent of the correlation explored using voxel-wise analysis, which revealed significant clusters located in the left dorsal caudate and anterior putamen confirming the ROI findings (Figure 3).

Higher dorsal striatal dopamine synthesis capacity associated with higher temporal discounting in Parkinson patients. (a) The correlation between the left caudate FDOPA uptake (Kiref) and temporal discounting rate (k). Solid circles represent patients with BAs. Open circles represent patients without BAs. (b) The pseudo-T values (red–yellow scale) for positive correlations between FDOPA Kiref and temporal discounting rate k (peak at 22 30 −23, cluster size k=494, PFWE=0.003). The image is thresholded to show only clusters with PFWE<0.05. The background image is the average normalized T1-weighted MRI of the subjects in Study 2. The images are displayed in radiological convention (that is, the right side of the image corresponds to the left side of the patient). BA, behavioral addiction; FDOPA, fluorodopa; FWE, family-wise error.
When examining the PD patients with and without BAs separately, the correlation between the left caudate Kiref and overall temporal discounting was similar in both groups (r=0.67, P=0.05 for patients with and r=0.74, P=0.04 for patients without BAs). In addition, the left anterior putamen Kiref correlated with k-value in patients with BAs (r=0.75, P=0.02). There were no significant differences in the correlation coefficients between the groups. Correlation analyses were not performed separately by specific BAs due to the low number of patients in these subgroups.
The left hemiphere was contralateral to the predominant motor symptoms in 8/17 patients and the k-value did not differ according to the side of the predominant motor symptoms (P=0.81). When examining the effect of PD-related factors on [18F]fluorodopa uptake, Kiref values correlated with PD duration only in the posterior putamen (r=−0.65, P=0.007). Off-medication Unified Parkinson’s Disease Rating Scale motor scores did not correlate with striatal [18F]fluorodopa uptake in any of the regions (P>0.08) in the present sample.
Discussion
Converging evidence suggests that temporal discounting is associated with dopaminergic mechanisms. We assessed temporal discounting using two different dopaminergic ligands and three populations in which temporal discounting has been shown to be impaired. Consistent with rodent studies, we showed a relationship between greater temporal discounting and lower ventral striatal D2/D3 receptor density.28 We further showed a relationship between greater temporal discounting and lower ventral striatal dopamine release as a function of high-reward magnitude in a gambling task, suggesting a role for dopamine-mediated interindividual discounting of delayed rewards in influencing intertemporal choice preference. In contrast, in all PD subjects, higher temporal discounting correlated with greater left caudate dopaminergic terminal function suggesting a role for abnormal dopaminergic dorsal striatal function possibly related to the neuropathology of PD. In PD subjects with BA, higher temporal discounting also correlated with greater left anterior putamen dopaminergic terminal function, suggesting a further engagement of dorsal striatal regions. Our findings can be explained by a U-shaped relationship between temporal discounting and dopamine function.19
Ventral striatal D2/D3 receptors
PG subjects, as expected, had greater temporal discounting compared with healthy volunteers.37 We found that greater temporal discounting correlated with lower ventral striatal [11C]raclopride binding potential during the motor control task across all the subjects. We suggest that this may reflect lower D2/D3 receptor density at baseline rather than greater presynaptic dopamine release at baseline or to a simple motor task. As the right ventral striatal binding potentials were lower compared with left and all but one of the subjects used their right hand for motor responses, it is highly unlikely that the findings were related to motor activation during a simple control task. In rodent studies, premature responding (responding before target onset) is correlated with delay discounting.27 Premature responding (and delay discounting) is associated with lower [18F]fallypride binding potential in the nucleus accumbens but not with changes in dopamine metabolites, indicating a specific relationship with lower D2/D3 receptors rather than presynaptic dopamine release.28 Given the relationship between premature responding and delay discounting, our findings in humans provide translational support for the preclinical findings. A questionnaire-based subtype of impulsivity, specifically the factor of mood-related ‘urgency’, has also been shown to be negatively correlated with striatal D2/D3 receptor availability in PG.38 Similarly, questionnaire-based impulsivity was associated with lower striatal midbrain D2/D3 receptors in healthy volunteers.39 Our study extends these findings to a form of decisional impulsivity.
Ventral striatal presynaptic dopamine release
We also showed that across all subjects greater temporal discounting correlated with lower ventral striatal dopamine release to a simulated gambling task to high but not low-reward magnitude. Temporal discounting can be parcellated into several cognitive mechanisms including but not limited to the incentive salience of the immediate choice, the discounting effects of the delay, the uncertainty of the delayed choice or decreasing subjective valuation of increasing magnitude.2, 40 The fact that the findings are specific to the anticipation and receipt of a high but not low-reward magnitude is argumentative against an effect of uncertainty, cue conditioning (as a function of the gambling task design) or motor response, all of which were equal across high and low magnitude conditions.
Lesions of the rodent nucleus accumbens core, amygdala and hippocampus increase impulsive choice, suggesting that these structures are critical to the evaluative process.12, 41, 42 In human functional magnetic resonance imaging studies, the ventral striatum, prefrontal cortex, insula, amygdala, posterior cingulate and parietal cortex have been implicated in intertemporal choice for secondary43, 44, 45, 46 and primary rewards.47 The ventral striatum is a key structure implicated in valuation theories of temporal discounting. The ventral striatum and medial prefrontal cortex have been implicated in overvaluing immediate reward choice, whereas lateral prefrontal and parietal cortices are activated across all decisions.46 Delay has been suggested to be coded in the lateral prefrontal cortex and magnitude coded in the ventral striatum.43 In contrast, the ventral striatum has also been suggested to represent the subjective value of the delayed choice.45 Along these lines, single-unit striatal recordings of cue-predicting rewards in primates show that dopaminergic neuronal activity both increases monotonically with magnitude and decreases with delay, reflecting the subjective devaluation of the delayed reward.11 Our findings suggest that ventral striatal dopaminergic activity may reflect choice preference and encode the devalued delayed reward. Were this to represent the incentive value of the immediate reward, one might anticipate the opposite correlation with increased temporal discounting and increased dopaminergic activity representing enhanced incentive value of the immediate reward. We speculate that the relationship between dopaminergic activity and temporal discounting may be driven by the enhanced ventral striatal discounting of delayed rewards.
Our findings are consistent with preclinical studies on endogenous dopamine activity showing that greater temporal discounting is associated with lower dopamine reactivity in the nucleus accumbens core and shell3 and that single-unit striatal recordings encode the subjective devaluation of a delayed reward.11 These findings suggest that interindividual endogenous dopamine release to delayed high-reward magnitude may influence choice preference for intertemporal choices. In contrast, exogenous administration of dopaminergic agents presents a mixed picture, with low and moderate doses of amphetamine decreasing impulsive choice in rodents13, 14, 15 but high chronic doses of stimulants increasing impulsive choice.14, 16 Exogenous levodopa in healthy humans increases impulsive choice.17 In healthy humans, questionnaire-based impulsivity is associated with enhanced amphetamine-induced striatal dopamine release.39 These inconsistent findings may be related to dose differences, with a U-shaped relationship between dopamine activity and temporal discounting.19
Dorsal striatal dopamine function
Using [18F]fluorodopa PET, we further showed that greater temporal discounting is associated with greater left caudate dopaminergic terminal function in PD patients with and without BA. The fact that PD has been associated with temporal discounting irrespective of dopaminergic medication status6, 7 suggests that the neuropathology of PD affecting dorsal striatal functioning might have a role in temporal discounting. In line with this, caudate activity has been associated with greater temporal discounting in healthy volunteers.48, 49 In addition, in PD patients, levodopa administration has been shown to change their betting strategies to more impulsive and dopamine agonists increase impulsive choice rather than diminish behavioral control.18, 50 In PD subjects and healthy controls, the caudate is anatomically connected to the lateral prefrontal cortex.51 The dorsolateral prefrontal cortex (DLPFC) is implicated in temporal discounting, particularly in the representation of the delay.43, 46 Studies using low-frequency repetitive transcranial magnetic stimulation (rTMS), which inhibits cortical excitability, show that disruption of the left, but not right DLPFC increases choice preference for the immediate reward but does not affect valuation processes.52 Similarly, in smokers, high frequency repetitive transcranial magnetic stimulation to increase left DLPFC activity was associated with greater preference for the delayed reward.53 Repetitive transcranial magnetic stimulation inhibition of the left DLPFC is associated with caudate dopamine release in depressed patients54 and healthy volunteers.55 Our findings being lateralized to the left caudate dovetails with these reports, suggesting that inhibition of left DLPFC activity via stimulation may increase preference for the immediate reward possibly by increasing downstream left caudate dopaminergic function.
In our study, greater temporal discounting was also associated with greater presynaptic dopaminergic availability in the left anterior putamen in PD patients with BA but not in those without BA. We have previously shown in this same population that PD subjects with and without BAs exhibited no differences in striatal presynaptic dopaminergic function.26 In PD subjects and healthy controls, the anterior putamen is functionally connected to the pre-supplementary motor area.51 An imbalance in dopaminergic function in associative, relative to motor, striatal regions may contribute to the emergence of BAs.
Limitations
We did not compare PG patients using [18F]fluorodopa or PD patients using [11C]raclopride. The study was also limited by relatively small sample size and lack of healthy volunteer group matched to PD patients. Several correlation analyses with multiple ROIs were performed, which might increase the type I error rate. However, the issue of multiple comparisons was stringently addressed in the voxel-wise analyses by using family-wise error correction.
Conclusions
Our results support the concept of a U-shaped relationship between striatal dopaminergic function and intertemporal choice and provide insight into its potential role in pathological disorders and the mechanisms underlying treatment interventions.
References
Kirby KN, Petry NM, Bickel WK . Heroin addicts have higher discount rates for delayed rewards than non-drug-using controls. J Exp Psychol Gen 1999; 128: 78–87.
Bickel WK, Koffarnus MN, Moody L, Wilson AG . The behavioral- and neuro-economic process of temporal discounting: a candidate behavioral marker of addiction. Neuropharmacology 2013; 76: 518–527.
Diergaarde L, Pattij T, Poortvliet I, Hogenboom F, de Vries W, Schoffelmeer AN et al. Impulsive choice and impulsive action predict vulnerability to distinct stages of nicotine seeking in rats. Biol Psychiatry 2008; 63: 301–308.
Perry JL, Nelson SE, Carroll ME . Impulsive choice as a predictor of acquisition of IV cocaine self- administration and reinstatement of cocaine-seeking behavior in male and female rats. Exp Clin Psychopharmacol 2008; 16: 165–177.
Broos N, Diergaarde L, Schoffelmeer AN, Pattij T, De Vries TJ . Trait impulsive choice predicts resistance to extinction and propensity to relapse to cocaine seeking: a bidirectional investigation. Neuropsychopharmacology 2012; 37: 1377–1386.
Milenkova M, Mohammadi B, Kollewe K, Schrader C, Fellbrich A, Wittfoth M et al. Intertemporal choice in Parkinson's disease. Mov Disord 2011; 26: 2004–2010.
Voon V, Dalley JW . Parkinson disease: impulsive choice-Parkinson disease and dopaminergic therapy. Nat Rev Neurol 2011; 7: 541–542.
Voon V, Reynolds B, Brezing C, Gallea C, Skaljic M, Ekanayake V et al. Impulsive choice and response in dopamine agonist-related impulse control behaviors. Psychopharmacology (Berl) 2010; 207: 645–659.
Housden CR, O'Sullivan SS, Joyce EM, Lees AJ, Roiser JP . Intact reward learning but elevated delay discounting in Parkinson's disease patients with impulsive-compulsive spectrum behaviors. Neuropsychopharmacology 2010; 35: 2155–2164.
Leroi I, Barraclough M, McKie S, Hinvest N, Evans J, Elliott R et al. Dopaminergic influences on executive function and impulsive behaviour in impulse control disorders in Parkinson's disease. J Neuropsychol 2013; 7: 306–325.
Kobayashi S, Schultz W . Influence of reward delays on responses of dopamine neurons. J Neurosci 2008; 28: 7837–7846.
Cardinal RN, Pennicott DR, Sugathapala CL, Robbins TW, Everitt BJ . Impulsive choice induced in rats by lesions of the nucleus accumbens core. Science 2001; 292: 2499–2501.
Floresco SB, Tse MT, Ghods-Sharifi S . Dopaminergic and glutamatergic regulation of effort- and delay-based decision making. Neuropsychopharmacology 2008; 33: 1966–1979.
Richards JB, Sabol KE, de Wit H . Effects of methamphetamine on the adjusting amount procedure, a model of impulsive behavior in rats. Psychopharmacology (Berl) 1999; 146: 432–439.
van Gaalen MM, van Koten R, Schoffelmeer AN, Vanderschuren LJ . Critical involvement of dopaminergic neurotransmission in impulsive decision making. Biol Psychiatry 2006; 60: 66–73.
Roesch MR, Takahashi Y, Gugsa N, Bissonette GB, Schoenbaum G . Previous cocaine exposure makes rats hypersensitive to both delay and reward magnitude. J Neurosci 2007; 27: 245–250.
Pine A, Shiner T, Seymour B, Dolan RJ . Dopamine, time, and impulsivity in humans. J Neurosci 2010; 30: 8888–8896.
Cools R, Barker RA, Sahakian BJ, Robbins TW . L-Dopa medication remediates cognitive inflexibility, but increases impulsivity in patients with Parkinson's disease. Neuropsychologia 2003; 41: 1431–1441.
Kayser AS, Allen DC, Navarro-Cebrian A, Mitchell JM, Fields HL . Dopamine, corticostriatal connectivity, and intertemporal choice. J Neurosci 2012; 32: 9402–9409.
Joutsa J, Johansson J, Niemelä S, Ollikainen A, Hirvonen MM, Piepponen P et al. Mesolimbic dopamine release is linked to symptom severity in pathological gambling. Neuroimage 2012; 60: 1992–1999.
Linnet J, Peterson E, Doudet DJ, Gjedde A, Møller A . Dopamine release in ventral striatum of pathological gamblers losing money. Acta Psychiatr Scand 2010; 122: 326–333.
Steeves TD, Miyasaki J, Zurowski M, Lang AE, Pellecchia G, Van Eimeren T et al. Increased striatal dopamine release in Parkinsonian patients with pathological gambling: a [11C] raclopride PET study. Brain 2009; 132: 1376–1385.
O'Sullivan SS, Wu K, Politis M, Lawrence AD, Evans AH, Bose SK et al. Cue-induced striatal dopamine release in Parkinson's disease-associated impulsive-compulsive behaviours. Brain 2011; 134: 969–978.
Cilia R, Ko JH, Cho SS, van Eimeren T, Marotta G, Pellecchia G et al. Reduced dopamine transporter density in the ventral striatum of patients with Parkinson's disease and pathological gambling. Neurobiol Dis 2010; 39: 98–104.
Voon V, Rizos A, Chakravartty R, Mulholland N, Robinson S, Howell NA et al. Impulse control disorders in Parkinson's disease: decreased striatal dopamine transporter levels. J Neurol Neurosurg Psychiatry 2013; 85: 148–152.
Joutsa J, Martikainen K, Niemelä S, Johansson J, Forsback S, Rinne JO et al. Increased medial orbitofrontal [18F]fluorodopa uptake in Parkinsonian impulse control disorders. Mov Disord 2012; 27: 778–782.
Robinson ES, Eagle DM, Economidou D, Theobald DE, Mar AC, Murphy ER et al. Behavioural characterisation of high impulsivity on the 5-choice serial reaction time task: specific deficits in 'waiting' versus 'stopping'. Behav Brain Res 2009; 196: 310–316.
Dalley JW, Fryer TD, Brichard L, Robinson ES, Theobald DE, Laane K et al. Nucleus accumbens D2/3 receptors predict trait impulsivity and cocaine reinforcement. Science 2007; 315: 1267–1270.
Brown WD, Taylor MD, Roberts AD, Oakes TR, Schueller MJ, Holden JE et al. FluoroDOPA PET shows the nondopaminergic as well as dopaminergic destinations of levodopa. Neurology 1999; 53: 1212–1218.
Gibb WR, Lees AJ . The relevance of the Lewy body to the pathogenesis of idiopathic Parkinson's disease. J Neurol Neurosurg Psychiatry 1988; 51: 745–752.
Voon V, Fox SH . Medication-related impulse control and repetitive behaviors in Parkinson disease. Arch Neurol 2007; 64: 1089–1096.
Kirby KN, Petry NM . Heroin and cocaine abusers have higher discount rates for delayed rewards than alcoholics or non-drug-using controls. Addiction 2004; 99: 461–471.
Mawlawi O, Martinez D, Slifstein M, Broft A, Chatterjee R, Hwang DR et al. Imaging human mesolimbic dopamine transmission with positron emission tomography: I. Accuracy and precision of D(2) receptor parameter measurements in ventral striatum. J Cereb Blood Flow Metab 2001; 21: 1034–1057.
Patlak CS, Blasberg RG . Graphical evaluation of blood-to-brain transfer constants from multiple-time uptake data. Generalizations. J Cereb Blood Flow Metab 1985; 5: 584–590.
Lammertsma AA, Hume SP . Simplified reference tissue model for PET receptor studies. Neuroimage 1996; 4: 153–158.
Laruelle M . Imaging synaptic neurotransmission with in vivo binding competition techniques: a critical review. J Cereb Blood Flow Metab 2000; 20: 423–451.
Petry NM . Pathological gamblers, with and without substance use disorders, discount delayed rewards at high rates. J Abnorm Psychol 2001; 110: 482–487.
Clark L, Stokes PR, Wu K, Michalczuk R, Benecke A, Watson BJ et al. Striatal dopamine D(2)/D(3) receptor binding in pathological gambling is correlated with mood-related impulsivity. Neuroimage 2012; 63: 40–46.
Buckholtz JW, Treadway MT, Cowan RL, Woodward ND, Li R, Ansari MS et al. Dopaminergic network differences in human impulsivity. Science 2010; 329: 532.
Pine A, Seymour B, Roiser JP, Bossaerts P, Friston KJ, Curran HV et al. Encoding of marginal utility across time in the human brain. J Neurosci 2009; 29: 9575–9581.
Cardinal RN, Winstanley CA, Robbins TW, Everitt BJ . Limbic corticostriatal systems and delayed reinforcement. Ann N Y Acad Sci 2004; 1021: 33–50.
Winstanley CA, Theobald DE, Cardinal RN, Robbins TW . Contrasting roles of basolateral amygdala and orbitofrontal cortex in impulsive choice. J Neurosci 2004; 24: 4718–4722.
Ballard K, Knutson B . Dissociable neural representations of future reward magnitude and delay during temporal discounting. Neuroimage 2009; 45: 143–150.
Tanaka SC, Doya K, Okada G, Ueda K, Okamoto Y, Yamawaki S . Prediction of immediate and future rewards differentially recruits cortico-basal ganglia loops. Nat Neurosci 2004; 7: 887–893.
Kable JW, Glimcher PW . The neural correlates of subjective value during intertemporal choice. Nat Neurosci 2007; 10: 1625–1633.
McClure SM, Laibson DI, Loewenstein G, Cohen JD . Separate neural systems value immediate and delayed monetary rewards. Science 2004; 306: 503–507.
McClure SM, Ericson KM, Laibson DI, Loewenstein G, Cohen JD . Time discounting for primary rewards. J Neurosci 2007; 27: 5796–5804.
Onoda K, Okamoto Y, Kunisato Y, Aoyama S, Shishida K, Okada G et al. Inter-individual discount factor differences in reward prediction are topographically associated with caudate activation. Exp Brain Res 2011; 212: 593–601.
Wittmann M, Leland DS, Paulus MP . Time and decision making: differential contribution of the posterior insular cortex and the striatum during a delay discounting task. Exp Brain Res 2007; 179: 643–653.
Antonelli F, Ko JH, Miyasaki J, Lang AE, Houle S, Valzania F et al. Dopamine-agonists and impulsivity in Parkinson's disease: impulsive choices vs impulsive actions. Hum Brain Mapp 2014; 35: 2499–2506.
Helmich RC, Derikx LC, Bakker M, Scheeringa R, Bloem BR, Toni I . Spatial remapping of cortico-striatal connectivity in Parkinson's disease. Cereb Cortex 2010; 20: 1175–1186.
Figner B, Knoch D, Johnson EJ, Krosch AR, Lisanby SH, Fehr E et al. Lateral prefrontal cortex and self-control in intertemporal choice. Nat Neurosci 2010; 13: 538–539.
Sheffer CE, Mennemeier M, Landes RD, Bickel WK, Brackman S, Dornhoffer J et al. Neuromodulation of delay discounting, the reflection effect, and cigarette consumption. J Subst Abuse Treat 2013; 45: 206–214.
Pogarell O, Koch W, Popperl G, Tatsch K, Jakob F, Zwanzger P et al. Striatal dopamine release after prefrontal repetitive transcranial magnetic stimulation in major depression: preliminary results of a dynamic [123I] IBZM SPECT study. J Psychiatr Res 2006; 40: 307–314.
Strafella AP, Paus T, Barrett J, Dagher A . Repetitive transcranial magnetic stimulation of the human prefrontal cortex induces dopamine release in the caudate nucleus. J Neurosci 2001; 21: RC157.
Acknowledgements
We are grateful to the staff of Turku PET Centre for their skilled assistance in the study. This work was supported by the Finnish Alcohol Research Foundation, the Finnish Medical Foundation, the Turku University Hospital (EVO-funds) and the Finnish Brain Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
J Joutsa has received lecturer honoraria from Boehringer-Ingelheim and a research grant from Lundbeck. VV is a Wellcome Trust Intermediate Clinical Fellow (093705/Z/10/Z). SN has received lecture fees from Janssen-Cilag, Lundbeck, Orion-Pharma and Sanofi-Aventis, a travel grant from Lundbeck, and served as a member of advisory board of Lundbeck. VK has received speaker honoraria and/or travel grants from Merck, Medtronic, Orion-Pharma, Abbvie, UCB and Lundbeck; and has served as a member of the advisory board of UCB and as a consultant for Orion-Pharma and Lundbeck. The remaining authors declare no conflict of interest.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Joutsa, J., Voon, V., Johansson, J. et al. Dopaminergic function and intertemporal choice. Transl Psychiatry 5, e491 (2015). https://doi.org/10.1038/tp.2014.133
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/tp.2014.133
- Springer Nature Limited
This article is cited by
-
Impulse Control Disorders in Parkinson’s Disease: An Overview of Risk Factors, Pathogenesis and Pharmacological Management
CNS Drugs (2024)
-
Dopamine D2 receptors in nucleus accumbens cholinergic interneurons increase impulsive choice
Neuropsychopharmacology (2023)
-
Drug-Induced Gambling Disorder: Epidemiology, Neurobiology, and Management
Pharmaceutical Medicine (2023)
-
Motor impulsivity and delay intolerance are elicited in a dose-dependent manner with a dopaminergic agonist in parkinsonian rats
Psychopharmacology (2020)
-
Presynaptic dopamine function measured with [18F]fluorodopa and L-DOPA effects on impulsive choice
Scientific Reports (2019)