
Abstract
The vulnerability to suicidal behavior has been modeled in deficits in both valuation and cognitive control processes, mediated by ventral and dorsal prefrontal cortices. To uncover potential markers of suicidality based on this model, we measured several brain morphometric parameters using 1.5T magnetic resonance imaging in a large sample and in a specifically designed study. We then tested their classificatory properties. Three groups were compared: euthymic suicide attempters with a past history of mood disorders and suicidal behavior (N=67); patient controls with a past history of mood disorders but not suicidal behavior (N=82); healthy controls without any history of mental disorder (N=82). A hypothesis-driven region-of-interest approach was applied targeting the orbitofrontal cortex (OFC), ventrolateral (VLPFC), dorsal (DPFC) and medial (including anterior cingulate cortex; MPFC) prefrontal cortices. Both voxel-based (SPM8) and surface-based morphometry (Freesurfer) analyses were used to comprehensively evaluate cortical gray matter measure, volume, surface area and thickness. Reduced left VLPFC volume in attempters vs both patient groups was found (P=0.001, surviving multiple comparison correction, Cohen’s d=0.65 95% (0.33–0.99) between attempters and healthy controls). In addition, reduced measures in OFC and DPFC, but not MPFC, were found with moderate effect sizes in suicide attempters vs healthy controls (Cohen’s d between 0.34 and 0.52). Several of these measures were correlated with suicidal variables. When added to mood disorder history, left VLPFC volume increased within-sample specificity in identifying attempters in a significant but limited way. Our study, therefore, confirms structural prefrontal alterations in individuals with histories of suicide attempts. A future clinical application of these markers will, however, necessitate further research.
Similar content being viewed by others


Introduction
One million individuals commit suicide each year worldwide.1 Improving our ability to predict and subsequently prevent it has become an important priority. However, the current assessment of suicide risk is based upon numerous socio-demographic and clinical risk factors often yielding a high sensitivity but a low specificity.2 It is expected that using specific neurobiological markers, in addition to the clinical assessment, may improve the future evaluation of suicide risk. Uncovering some of these biomarkers is the goal of the present study.
The current understanding of suicidal behavior is based on a stress-vulnerability model, which suggests that some individuals are at higher risk of committing suicide in stressful situations like interpersonal conflicts or loss.3 This model has been supported by in vivo neuroimaging studies.4 When comparing suicide attempters (SAs) with patient controls (PCs) and/or healthy controls (HCs), functional neuroimaging studies have revealed dysfunctional ventral, dorsomedial and dorsolateral prefrontal cortices among other regions in various conditions, from resting state5 to viewing angry faces,6 making decisions7 or listening to suicidal scripts.8 Finally, structural neuroimaging has reported various brain alterations in SAs, affecting both gray and white matter (see below).
On the basis of this literature, we recently proposed a neuroanatomical model accounting for the vulnerability to suicidal behavior at the neurocognitive level.4 In this model, we suggested that the ventral prefrontal cortex including the orbitofrontal cortex (OFC) would be mainly implicated in valuation deficits, explaining decision-making impairments in SAs,9 while more dorsal parts of the prefrontal cortex (including anterior cingulate cortex, ACC) may explain deficits in cognitive control and emotion regulation processes.10 In the present study, we aimed at confirming the involvement of these prefrontal brain regions, and their potential as biomarkers, by examining their morphometric properties using structural neuroimaging in a large sample. Certainly, the ease of implementing structural neuroimaging compared with functional neuroimaging is potentially a great advantage and highly relevant for future clinical application.
However, previous results using this technique suffer from various limitations. First, many studies assessed samples of small size, as few as seven to ten SAs.11, 12 Only one large study, in psychotic disorders, has been published to date.13 Recent papers have highlighted a frequent lack of replication of findings in neuroscience, partly in relation to underpowered studies.14 Second, of the six published studies evaluating whole-brain gray matter alterations, six different types of statistical thresholds have been used.15, 16, 17, 18, 19, 20 However, recent discussions about the lack of reliability of the P-value suggest that calculating effect sizes may be a more relevant approach.21 Third, these studies have focused on one particular standard analysis method, usually measuring brain volume differences using voxel-based morphometry (VBM), but have seldom applied concurrent surface-based morphometry (SBM) analyses. Only two studies explored cortical thickness to date.13, 22 To our knowledge, only one group has combined two analysis methods in two different publications.15, 22 Yet, recent analyses have suggested that different SBM measures account for VBM gray matter variation in different regions but also that VBM may be more sensitive than SBM to detect some abnormalities.23 The combination of both analyses could therefore improve our understanding of structural neuroimaging markers of disease.
We addressed several of these issues in the present study. First, we pooled data from three separate studies conducted in two locations with identical study designs to increase power. This has resulted in the largest neuroimaging study conducted on vulnerability to suicidal behavior in mood disorders to date. Second, we calculated effect sizes for the main contrasts, namely SAs vs PCs, and SAs vs HCs. Third, we used two complementary analysis approaches in parallel, namely VBM and SBM. Finally, we used a validated study group design to specifically examine the vulnerability to suicidal behavior by including non-depressed patients to exclude the acute effects of the depressive state, and a group of patients with a history of mood disorder but no suicide attempt to exclude the effect of comorbid disorders.
On the basis of previous studies, we hypothesized that SAs when compared with control groups would show a reduction in structural measures of prefrontal cortex. To test the potential clinical applicability of these measures, we additionally conducted sensitivity and specificity calculations.
Materials and methods
Samples and assessment
Three samples were recruited, one at the Institute of Psychiatry in London, UK (Sample 1), and two at the academic hospital of Montpellier, France (Samples 2 and 3). For all the three samples, participants were recruited through advertisement with an initial screening via telephone interview, or in clinical settings. They were then interviewed in person by experienced psychiatrists. All participants were right-handed24 and euthymic at the time of scanning with a HDRS (Hamilton Depression Rating Scale) score below nine.25 Exclusion criteria were a lifetime history of severe head trauma, central nervous system disorders, schizophrenia and substance use disorder over the last 12 months, suicide attempt using firearms, pregnancy and contraindications to magnetic resonance imaging (MRI). Details on exclusions from each sample are given in Supplementary Information.
The three samples differed in two selection criteria: (1) Samples 1 and 2 comprised only males aged between 18 and 60, whereas Sample 3 comprised only non-menopausal females aged between 18 and 50; (2) All patients in Sample 1 suffered from major depressive disorder, whereas Samples 2 and 3 included both major depressive disorder and bipolar disorders.
All diagnoses were made according to the Diagnostic and Statistical Manual of Mental Disorders IV criteria using the Mini-International Neuropsychiatric Interview, version 5.0.0.26 The French or English versions of the National Adult Reading Test27 were used to provide an estimation of verbal IQ and the Beck Depression Inventory28 for a subjective measure of current depressive state. Participants also completed the Barratt Impulsiveness Scale version 10.29
Within each sample, three groups were recruited as described above: (1) SAs, individuals with a personal history of both mood disorder and suicidal behavior; (2) PCs, individuals with a history of mood disorder but no lifetime history of suicidal behavior; (3) HCs, individuals with no current or past history of any Diagnostic and Statistical Manual of Mental Disorders IV Axis I diagnoses or suicidal behavior or psychotropic medication. The overall population included 82 HCs, 82 PCs and 67 SAs.
As in our previous studies, suicidal act was defined as any nonfatal, self-directed potentially injurious behaviors with any intent to die as a result.3 The last and the most severe suicidal acts were assessed using the Risk Rescue Rating Scale30 and the Suicide Intent Scale.31
Participants from Sample 3 additionally fullfilled the Childhood Trauma Questionaire,32 and participants from Sample 1 played the Iowa Gambling Task, a decision-making test.33
After complete description of the study to the subjects, written informed consent was obtained from all the participants. The studies were approved by the respective Research Ethics Committee (Institute of Psychiatry and Montpellier Research Ethics Board). The participants were paid £30 and €100, respectively.
Functional neuroimaging and behavioral results (but not structural results) from Sample 1 have previously been published6, 7 but data from Samples 2 and 3 have not.
MRI acquisition procedures
For Sample 1, T1-weighted magnetic resonance images were acquired using a GE Signa 1.5 T Neuro-optimized MR system (General Electric, Milwaukee, WI, USA) at the Institute of Psychiatry, London, UK. A spoiled gradient echo sequence was used for the T1-weighted acquisition with the following parameters: isotropic voxel dimension of 1.1 mm with field-of-view at 280 × 180 mm; TE (echo time) of 5 ms and TR (repetition time) of 10.8 ms. Two-dimensional matrix 256 × 160 with 150 slices acquired, bandwidth of 122 Hz per pixel.
For Samples 2 and 3, T1-weighted magnetic resonance images were acquired with a 1.5 T whole-body MRI system (MAGNETON AVANTO, Siemens, Erlangen, Germany) in Montpellier Academic Hospital, France. Sample 2 used three-dimensional T1 FLASH sequence with voxel dimension of 0.93 × 0.93 × 1 mm, field-of-view at 240 × 240 mm, matrix 256 × 256, 15 degrees flip angle, TE of 5.2 ms and TR of 11 ms with 160 slices, bandwidth of 130 Hz per pixel. Sample 3 used three-dimensional T1 MPRAGE with voxel dimension of 0.98 mm × 0.98 mm × 1 mm, field-of-view at 250 × 250 mm, matrix 256 × 256 with 160 slices, 15 degrees flip angle, TE of 4.1 ms, TR of 2100 ms and TI of 1100 ms, bandwidth of 140 Hz per pixel.
MRI analyses
We conducted VBM analyses using SPM8 v.4667, and SBM analyses with FreeSurfer 5.1.0. (Details in the Supplementary Information). In brief, after quality control checks, SPM segments the T1 structural data and produces a group template based on the entire group data set by nonlinearly warping each participant to the common brain template space while preserving local anatomical alterations. VBM analyses yield normalized gray matter volume measurement since it is sampled in template MNI space, not the individual space before normalization. In contrast, Freesurfer registers each vertices at individual gyrus/sulcus level to template but ultimately produce individualized measurement of volume, area and surface based on personally modeled brain morphometry and gray matter/white matter boundary contours. VBM data were smoothed using an 8-mm full width at half maximum Gaussian kernel in volume space, whereas SBM data were smoothed using 20 mm full width at half maximum Gaussian kernel in surface space to maximize sensitivities toward smaller clusters of structural differences as suggested by previous studies testing variety of full width at half maximum sizes in different sample sizes.34, 35
We used a region-of-interest (ROI) approach due to robust a priori hypotheses17 and its elevated statistical sensitivity. Four ROIs (Figure 1) were defined using independently a priori defined anatomical atlases (detailed in Supplementary Information), on the basis of regions previously reported to show structural and/or functional alterations associated with suicidal behavior, and differentiated on the basis of different brain connections36 and functional roles notably in valuation processes and cognitive control:37, 38 (1) the OFC,6, 7, 12, 13 (corresponding to the lateral part of Brodmann areas (BAs) 11, and BA 47); (2) the ventrolateral prefrontal cortex (referred to as VLPFC and corresponding to BA 44 and 45);39 (3) the ventromedial prefrontal cortex (including the medial part of BA 11, BA 10 and the ACC, both rostral and dorsal parts (BA 24/32); ROI referred to medial prefrontal cortex, MPFC)15 and (4) the dorsal and lateral prefrontal cortex (referred to as DPFC and corresponding to BA 46/8/9).5, 19, 20 Average measures of all the voxels (for VBM) or vertex (for SBM) measures within that ROI were used.

Representation of the four regions-of-interest of the prefrontal cortex examined in this article. Blue: medial prefrontal cortex (MPFC; including anterior cingulate cortex, not shown); red: dorsal prefrontal cortex (DPFC); green: orbitofrontal cortex (OFC); violet: ventrolateral prefrontal cortex (VLPFC). VBM, voxel-based morphometry.
Although multi-site neuroimaging poses challenges, samples can be combined and analyzed when groups are balanced across samples (which is the case here) and samples multi-site are properly controlled for in the analysis.40, 41 The total volume and surface area, and the average thickness in individual space and normalized gray matter volume in template space for each ROI were extracted and analyzed after covarying for relevant covariables consecutively. Group comparisons in normalized gray matter volume, and SBM volumes/areas were systematically controlled for intracranial volume.42
Statistical analyses
General linear model, followed by Tukey’s post hoc, were used to compare quantitative variables between groups, and Pearson’s correlation to examine associations between quantitative variables. Qualitative variables were compared using χ2 tests.
We additionally calculated effect sizes (Cohen’s d) and its 95% confidence interval based on marginal means and standard error output from the general linear model (after accounting for the appropriate covariates) for the main contrasts between SA and both control groups.
A binary logistic regression model was used for sensitivity and specificity analyses.
When applying, the alpha level was set at 0.05 unless a Bonferroni correction was necessary. The threshold for ROI analyses was set at a very conservative Bonferroni-corrected P<0.002 (P<0.05 divided by four ROIs, two sides and four different measures).
Statistical analyses were carried out with SPSS 20 (SPSS, Chicago, IL, USA).
Results
Socio-demographic and clinical variables
Groups were equally distributed across samples (see Supplementary Information). Similar between-groups differences were observed across all three samples and the pooled sample (Table 1). Although euthymic, HDRS and Beck Depression Inventory scores were higher in patients as expected. These variables were not used as covariates as they are related to the group profile. Level of education was higher in HCs than SAs. Moreover, there were more males in HC than both patient groups.
SAs did not differ significantly from PCs on socio-demographic or clinical variables. However, they received significantly more antipsychotics with a trend for more anxiolytics/hypnotics. Most suicidal acts (85%) were drug overdose.
Neuroimaging findings
Voxel-based morphometry
See Table 2 for group comparisons of all measures, Figure 2 for effect size analyses and Figure 3 for a correlation map between all measured examined here.

Effect sizes between suicide attempters and both control groups for the four regions-of-interest. DPFC, dorsal prefrontal cortex; MPFC, medial prefrontal cortex; OFC, orbitofrontal cortex; VBM, voxel-based morphometry; VLPFC, ventrolateral prefrontal cortex. Blue: suicide attempters vs patient controls; black: suicide attempters vs healthy controls.

Correlation map between all magnetic resonance imaging measures for the four regions-of-interest. DPFC, dorsal prefrontal cortex; L, left; MPFC, medial prefrontal cortex; OFC, orbitofrontal cortex; R, right; VBM, voxel-based morphometry; VLPFC, ventrolateral prefrontal cortex.
After covarying for sample and intracranial volume, general linear models based on normalized cortical gray matter volumes showed between-group differences in left VLPFC (P=0.01), left OFC (P=0.03) and right DPFC (P=0.04), but not MPFC, although nonsignificant after multiple comparison correction. Post hoc analyses showed decreased normalized regional measures in SAs relative to HCs with no significant differences between SAs and PCs, and between HCs and PCs. Effect size calculation additionally suggests a significant effect between SAs and HCs for left DPFC, right VLPFC, right OFC and right MPFC (Figure 2).
In exploratory whole-brain VBM analyses, SPM revealed lower measure in SAs than PCs in right lateral OFC (BA 47; family-wise error-corrected cluster P-value=0.03; peak voxel=48, 21, 0; cluster size=1).
Surface-based morphometry
After covarying for sample and intracranial volume, there were group differences in gray matter volume in left VLPFC (P=0.001, surviving multiple comparison correction) with reduced volume in SAs vs both control groups, and between PCs and HCs, and right DPFC (P=0.03, not surviving multiple comparison correction), with reduced measures in SAs vs HCs. There was no difference for OFC or MPFC. Effect size calculation additionally suggests a significant effect between SAs and HCs for left DPFC and right VLPFC.
After covarying for sample and intracranial volume, there were group differences in gray matter area in left VLPFC (P=0.01, not surviving multiple comparison correction), with reduced measures in SAs vs HCs, but not in OFC, DPFC or MPFC.
After covarying for sample only, there were group differences in thickness in right VLPFC (P=0.04, not surviving multiple comparison correction) with reduced measure in SAs vs HCs, but not in OFC, DPFC or MPFC. Effect size calculation additionally suggests a significant effect between SA and HC for right DPFC.
Figure 3 shows that structural measures were highly intercorrelated, notably SBM volumes together and area measures together. Only thickness measures were poorly correlated with area or volume measures as expected.
Effect of covariates
Only left VLPFC SBM volume and left VLPFC area remained significant after controlling for all main covariates (age, gender, level of education, bipolar disorder, lithium or antipsychotic intake). Left VLPFC VBM volume was not significant anymore when covarying for gender or bipolar disorder; left OFC VBM volume for age, gender, bipolar disorder or lithium; right DPFC VBM or SBM volumes for age, gender or bipolar disorder; right VLPFC thickness for bipolar disorder or antipsychotics.
Correlation with clinical variables
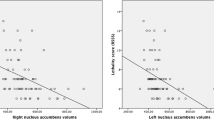
In SAs, lethality of the last suicidal act was correlated with all measures except left VLPFC area and right VLPFC thickness (all P<0.05; strongest correlations with right DPFC VBM and SBM volumes: r=−0.45; P<10−3; left OFC: r=−0.38, P=0.001; left VLPFC SBM volume: r=−0.33; P=0.007); number of suicidal acts was correlated with right DPFC VBM volume (r=−0.25, P=0.04) and left OFC VBM (r=−0.24; P=0.05); age at first suicidal act with right DPFC SBM volume (r=−0.40; P=0.001) and right VLPFC thickness (r=−0.26, P=0.03). No measure was correlated with Suicide Intent Scale.
In patients, HDRS score was correlated with all measures except left VLPFC area and right VLPFC thickness (r between −0.15 and −0.21; all P<0.07); age at first mood episode with right VLPFC thickness only (r=−0.21; P=0.01); number of mood episodes with right DPFC SBM volume (r=−0.20, P=0.01); Barratt Impulsiveness Scale version 10 total score with all measures except right DPFC SBM volume (all P<0.07; strongest correlation with left VLPFC area: r=0.26, P=0.001; left OFC: r=0.23, P=0.005); and Childhood Trauma Questionaire total score with right VLPFC thickness (r=−0.24; P=0.03). No measure was correlated with Beck Depression Inventory.
There was no significant assocation between the Iowa Gambling Task total score and any measure, but data were only available in the small Sample 1.
Potential for clinical application
We examined the sensitivity and specificity of the neuroimaging measures in correctly classifying individuals with histories of suicide attempt among the 231 participants. As expected, a history of mood disorder had a 100% sensitivity (as all SAs suffered from mood disorder in our study) but a lower specificity (71%). Adding left VLPFC area or volume into the model improved specificity in identifying attempters in a significant but limited manner, reaching 74.9 and 75.3%, respectively. Other measures had smaller effects. Of note, these findings cannot be generalized and may be inflated, and should therefore be seen as indicative of the clinical potential of these measures when added to clinical signs and symptoms.
Discussion
This study examined structural alterations associated with the vulnerability to suicidal behavior in mood disorders using two complementary analyses in 231 subjects including 67 SAs. It represents the largest neuroimaging study of suicidal behavior in mood disorders to date and was specifically designed to investigate the neural basis of suicidal behavior. After covarying for sample, intracranial volume, gender, age, education, bipolar disorder and medication intake, ROI analyses showed significant group differences in left VLPFC volume measured by Freesurfer, the only measure that discriminated SA from both control groups in our study. Additional measures in VLPFC, OFC and DPFC, although not surviving a very conservative multiple comparison correction, were also different between SAs and HCs, with moderate effect sizes (Cohen’s d up to 0.50). The link between these neuroimaging measures and the vulnerability to suicidal acts is further supported by significant correlations with suicidal variables including suicidal lethality, age at first suicidal act and number of previous acts. It is important to emphasize that patients were euthymic at the time of scanning, suggesting that these differences may reflect trait-like alterations. Our findings, therefore, tend to support the involvement of structural impairments in VLPFC, DPFC and OFC, but not MPFC (including ACC), in the pathophysiology of suicidal behavior.
Our results are in agreement with several results from previous studies in mood disorders. For dorsal regions, reduced VBM volumes in DPFC in SAs vs PCs have been reported in bipolar disorder20 and in elderly individuals with major depressive disorder.19 Wagner et al.22 also reported reduced cortical thickness in the same region. Reduced volume of ACC in SAs vs PCs has been found in depressive disorders,15 bipolar disorder20 but not in a small sample of depressed women.12 However, our study showed no structural differences in ACC. For ventral regions, previous studies have also shown reduced VBM measure20 and thickness22 in OFC in SAs. Similarly, Wagner et al.22 reported reduced thickness in a region that encompassed our left VLPFC. Between-study differences in sample size, choice of threshold and lack of control for intracranial volume may explain some discrepancies with previous studies.
The role of these prefrontal regions in suicidal vulnerability has to be clarified. Two recent meta-analyses confirmed deficits in decision-making, cognitive control and working and long-term memory in SA.9, 43 The OFC, which receives connections from the amygdala and thalamus, has a significant role in the interpretation of stimuli in the environment, notably in attributing value to stimuli (stimuli–outcome association),37 which may be important for the triggering of the suicidal crisis in the face of environmental stressors. The lateral PFC receives motivational inputs from ACC44 and represents cognitive information from memory, which is deficient in SA. Dorsal and lateral PFC notably confronts various informations to outcomes and, therefore, exert a cognitive control by ensuring the most advantageous choice in addition to some forms of behavioral flexibility.37 Dysfunction of this interconnected prefrontal network may, therefore, be instrumental in the suicidal process by corrupting information acquisition and processing, resulting in impaired decision-making. At the clinical level, this would be reflected by negative assessments of life events and the automatic triggering of intense emotional responses, and the inability to control the evoked emotional responses and particular negative thoughts (including hopelessness, ruminations and suicidal ideas), and to prevent choosing to commit a suicidal act over alternative options.
At a translational level, our findings suggest that simple 1.5 T 10-min structural MRI sequences, relatively easy to implement in clinical practice, are unfortunately not sufficient to differentiate patients at higher risk of committing a suicidal act from non-attempters. Although some measures investigated here significantly improved within-sample specificity in identifying SAs among patients with mood disorders, the improvement was not sufficiently large enough to support clinical application. Advancements, in terms of acquisition (for example, higher field or multi-morphometric sequences), analysis methods (for example, quantitative MRI) or examination of particular subregions, are expected and may also increase accuracy.
One must keep in mind that patients who attempt suicide are likely a heterogeneous group. Different subgroups of SAs (and PCs) may, therefore, show different structural alterations. This has previously been suggested in SAs when comparing decision-making performance in patients who committed violent vs nonviolent suicidal acts,45 and for resting-state activity in high vs low lethality attempters.5 It may be more relevant in future studies to focus on particular subgroups as suggested,46 for example, those with particular neurocognitive alterations, and assess the predictive value of these alterations in prospective studies and clinical trials. This should notably be tested with the imaging markers revealed here.
Our study presents several limitations. First, pooled data analysis adds heterogeneity when not designed a priori as a multicenter study, due to different acquisition parameters and scanners, which contributes to increased risk of type II errors47 but not type I error and does not undermine highlighted findings. Second, we included moderately to severely ill and often medicated patients to be more representative of the general clinical population. This may have added heterogeneity although several clinical factors (including bipolar disorder and medication) were controlled for in analyses. Finally, determination of ROIs largely depends on their definition and the atlases, and these only partly overlap for SBM and VBM. This could explain the lack of convergence in statistically significant results between the two analysis methods. Our ROIs were also large in size, which may have reduced our ability to detect more localized differences.
In conclusion, we confirmed the role of several prefrontal regions in the vulnerability to suicidal behavior. Further research is nonetheless required for the application of MRI in the prediction of suicidal behavior.
References
Hawton K, van Heeringen K . Suicide. Lancet 2009; 373: 1372–1381.
Mann JJ, Currier D . A review of prospective studies of biologic predictors of suicidal behavior in mood disorders. Arch Suicide Res 2007; 11: 3–16.
Mann JJ . Neurobiology of suicidal behaviour. Nat Rev Neurosci 2003; 4: 819–828.
Jollant F, Lawrence NL, Olie E, Guillaume S, Courtet P . The suicidal mind and brain: a review of neuropsychological and neuroimaging studies. World J Biol Psychiatry 2011; 12: 319–339.
Oquendo MA, Placidi GP, Malone KM, Campbell C, Keilp J, Brodsky B et al. Positron emission tomography of regional brain metabolic responses to a serotonergic challenge and lethality of suicide attempts in major depression. Arch Gen Psychiatry 2003; 60: 14–22.
Jollant F, Lawrence NS, Giampietro V, Brammer MJ, Fullana MA, Drapier D et al. Orbitofrontal cortex response to angry faces in men with histories of suicide attempts. Am J Psychiatry 2008; 165: 740–748.
Jollant F, Lawrence NS, Olie E, O'Daly O, Malafosse A, Courtet P et al. Decreased activation of lateral orbitofrontal cortex during risky choices under uncertainty is associated with disadvantageous decision-making and suicidal behavior. Neuroimage 2010; 51: 1275–1281.
Reisch T, Seifritz E, Esposito F, Wiest R, Valach L, Michel K . An fMRI study on mental pain and suicidal behavior. J Affect Disord 2010; 126: 321–335.
Richard-Devantoy S, Berlim MT, Jollant F . A meta-analysis of neuropsychological markers of vulnerability to suicidal behavior in mood disorders. Psychol Med 2014; 44: 1663–1674.
Richard-Devantoy S, Jollant F, Kefi Z, Turecki G, Olié JP, Annweiler C et al. Deficit of cognitive inhibition in depressed elderly: a neurocognitive marker of suicidal risk. J Affect Disord 2012; 140: 193–199.
Vang FJ, Ryding E, Traskman-Bendz L, van Westen D, Lindstrom MB . Size of basal ganglia in suicide attempters, and its association with temperament and serotonin transporter density. Psychiatry Res 2010; 183: 177–179.
Monkul ES, Hatch JP, Nicoletti MA, Spence S, Brambilla P, Lacerda AL et al. Fronto-limbic brain structures in suicidal and non-suicidal female patients with major depressive disorder. Mol Psychiatry 2007; 12: 360–366.
Giakoumatos CI, Tandon N, Shah J, Mathew IT, Brady RO, Clementz BA et al. Are structural brain abnormalities associated with suicidal behavior in patients with psychotic disorders? J Psychiatr Res 2013; 47: 1389–1395.
Button KS, Ioannidis JP, Mokrysz C, Nosek BA, Flint J, Robinson ES et al. Power failure: why small sample size undermines the reliability of neuroscience. Nat Rev Neurosci 2013; 14: 365–367.
Wagner G, Koch K, Schachtzabel C, Schultz CC, Sauer H, Schlosser RG . Structural brain alterations in patients with major depressive disorder and high risk for suicide: evidence for a distinct neurobiological entity? Neuroimage 2011; 54: 1607–1614.
Rusch N, Spoletini I, Wilke M, Martinotti G, Bria P, Trequattrini A et al. Inferior frontal white matter volume and suicidality in schizophrenia. Psychiatry Res 2008; 164: 206–214.
Aguilar EJ, Garcia-Marti G, Marti-Bonmati L, Lull JJ, Moratal D, Escartí MJ et al. Left orbitofrontal and superior temporal gyrus structural changes associated to suicidal behavior in patients with schizophrenia. Prog Neuropsychopharmacol Biol Psychiatry 2008; 32: 1673–1676.
Jia Z, Huang X, Wu Q, Zhang T, Lui S, Zhang J et al. High-field magnetic resonance imaging of suicidality in patients with major depressive disorder. Am J Psychiatry 2010; 67: 1381–1390.
Hwang JP, Lee TW, Tsai SJ, Chen TJ, Yang CH, Lirng JF et al. Cortical and subcortical abnormalities in late-onset depression with history of suicide attempts investigated with MRI and voxel-based morphometry. J Geriatr Psychiatry Neurol 2010; 23: 171–184.
Benedetti F, Radaelli D, Poletti S, Locatelli C, Falini A, Colombo C et al. Opposite effects of suicidality and lithium on gray matter volumes in bipolar depression. J Affect Disord 2011; 135: 139–147.
Nuzzo R . Scientific method: statistical errors. Nature 2014; 506: 150–152.
Wagner G, Schultz CC, Koch K, Schachtzabel C, Sauer H, Schlosser RG . Prefrontal cortical thickness in depressed patients with high-risk for suicidal behavior. J Psychiatr Res 2012; 46: 1449–1455.
Palaniyappan L, Liddle PF . Differential effects of surface area, gyrification and cortical thickness on voxel based morphometric deficits in schizophrenia. Neuroimage 2012; 60: 693–699.
Oldfield RC . The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 1971; 9: 97–113.
Hamilton M . A rating scale for depression. J Neurol Neurosurg Psychiatry 1960; 23: 56–62.
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 1998; 59 (Suppl 20): 22–33, quiz 34.
Beardsall L, Brayne C . Estimation of verbal intelligence in an elderly community: a prediction analysis using a shortened NART. Br J Clin Psychol 1990; 29: 83–90.
Beck AT, Ward CH, Mendelson M . An inventory for measuring depression. Arch Gen Psychiatry 1961; 4: 561–571.
Patton JH, Stanford MS, Barratt ES . Factor structure of the Barratt impulsiveness scale. J Clin Psychol 1995; 51: 768–774.
Weisman AD, Worden JW . Risk-rescue rating in suicide assessment. Arch Gen Psychiatry 1972; 26: 553–560.
Beck RW, Morris JB, Beck AT . Cross-validation of the Suicidal Intent Scale. Psychol Rep 1974; 34: 445–446.
Bernstein DP, Fink L, Handelsman L, Foote J, Lovejoy M, Wenzel K et al. Initial reliability and validity of a new retrospective measure of child abuse and neglect. Am J Psychiatry 1994; 151: 1132–1136.
Bechara A, Damasio H, Damasio AR, Lee GP . Different contributions of the human amygdala and ventromedial prefrontal cortex to decision-making. J Neurosci 1999; 19: 5473–5481.
Shen S, Sterr A . Is DARTEL-based voxel-based morphometry affected by width of smoothing kernel and group size? A study using simulated atrophy. J Magn Reson Imaging 2013; 37: 1468–1475.
Lerch JP, Evans AC . Cortical thickness analysis examined through power analysis and a population simulation. Neuroimage 2005; 24: 163–173.
Saleem KS, Miller B, Price JL . Subdivisions and connectional networks of the lateral prefrontal cortex in the macaque monkey. J Comp Neurol 2014; 522: 1641–1690.
Dixon ML, Christoff K . The lateral prefrontal cortex and complex value-based learning and decision making. Neurosci Biobehav Rev 2014; 45C: 9–18.
Banich MT, Depue BE . Recent advances in understanding neural systems that support inhibitory control. Curr Opin Behav Sci 2015; 1: 17–22.
Sublette ME, Milak MS, Galfalvy HC, Oquendo MA, Malone KM, Mann JJ . Regional brain glucose uptake distinguishes suicide attempters from non-attempters in major depression. Arch Suicide Res 2013; 17: 434–447.
Pardoe H, Pell GS, Abbott DF, Berg AT, Jackson GD . Multi-site voxel-based morphometry: methods and a feasibility demonstration with childhood absence epilepsy. Neuroimage 2008; 42: 611–616.
Takao H, Hayashi N, Ohtomo K . Effects of study design in multi-scanner voxel-based morphometry studies. Neuroimage 2014; 84: 133–140.
Buckner RL, Head D, Parker J, Fotenos AF, Marcus D, Morris JC et al. A unified approach for morphometric and functional data analysis in young, old, and demented adults using automated atlas-based head size normalization: reliability and validation against manual measurement of total intracranial volume. Neuroimage 2004; 23: 724–738.
Richard-Devantoy S, Berlim MT, Jollant F . Suicidal behaviour and memory: a systematic review and meta-analysis. World J Biol Psychiatry 2014; 1–23 (in press).
Kouneiher F, Charron S, Koechlin E . Motivation and cognitive control in the human prefrontal cortex. Nat Neurosci 2009; 12: 939–945.
Jollant F, Bellivier F, Leboyer M, Astruc B, Torres S, Verdier R et al. Impaired decision making in suicide attempters. Am J Psychiatry 2005; 162: 304–310.
Kapur S, Phillips AG, Insel TR . Why has it taken so long for biological psychiatry to develop clinical tests and what to do about it? Mol Psychiatry 2012; 17: 1174–1179.
Glover GH, Mueller BA, Turner JA, van Erp TG, Liu TT, Greve DN et al. Function biomedical informatics research network recommendations for prospective multicenter functional MRI studies. J Magn Reson Imaging 2012; 36: 39–54.
Acknowledgements
Preliminary data and partial data were previously presented at the 2012 and 2013 Organization for Human Brain Mapping Conferences, and 2013 International Academy of Suicide Research Conferences. Study 1 was supported by the American Foundation for Suicide Prevention (to FJ), Fondation pour la Recherche Médicale (Action Dynamique en Psychiatrie to FJ) and the Royal Society and University of London Central Research Fund (to NL). Study 2 was funded by a Projet Hospitalier de Recherche Clinique (to FJ and PC). EO received a grant from Académie Nationale de Médecine. Study 3 was funded by the Institut Servier (to FJ), who also funded FC's M.c. YD currently holds a Fond de Recherche du Québec—Santé (FRQS) PhD Grant #24117. FJ currently holds a ‘FRQS chercheur-boursier clinicien’ salary award. We thank Ms Corina Nagy for her helpful comments. See also our database of neuropsychological and neuroimaging studies at www.bdsuicide.disten.com.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Translational Psychiatry website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/4.0/
About this article

Cite this article
Ding, Y., Lawrence, N., Olié, E. et al. Prefrontal cortex markers of suicidal vulnerability in mood disorders: a model-based structural neuroimaging study with a translational perspective. Transl Psychiatry 5, e516 (2015). https://doi.org/10.1038/tp.2015.1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/tp.2015.1
- Springer Nature Limited
This article is cited by
-
Suicidality and homelessness: prevalence and associated factors of suicidal behaviour among homeless young adults in Southern Ethiopia
BMC Psychology (2023)
-
Machine learning based identification of structural brain alterations underlying suicide risk in adolescents
Discover Mental Health (2023)
-
Functional network alterations differently associated with suicidal ideas and acts in depressed patients: an indirect support to the transition model
Translational Psychiatry (2021)
-
Imaging suicidal thoughts and behaviors: a comprehensive review of 2 decades of neuroimaging studies
Molecular Psychiatry (2020)
-
Alterations in functional brain networks in depressed patients with a suicide attempt history
Neuropsychopharmacology (2020)