
Abstract
Meta-analyses support the involvement of different pathophysiological mechanisms (inflammation, hypothalamic–pituitary (HPA)-axis, neurotrophic growth and vitamin D) in major depressive disorder (MDD). However, it remains unknown whether dysregulations in these mechanisms are more pronounced when MDD progresses toward multiple episodes and/or chronicity. We hypothesized that four central pathophysiological mechanisms of MDD are not only involved in etiology, but also associated with clinical disease progression. Therefore, we expected to find increasingly more dysregulation across consecutive stages of MDD progression. The sample from the Netherlands Study of Depression and Anxiety (18–65 years) consisted of 230 controls and 2333 participants assigned to a clinical staging model categorizing MDD in eight stages (0, 1A, 1B, 2, 3A, 3B, 3C and 4), from familial risk at MDD (stage 0) to chronic MDD (stage 4). Analyses of covariance examined whether pathophysiological mechanism markers (interleukin (IL)-6, C-reactive protein (CRP), cortisol, brain-derived neurotrophic factor and vitamin D) showed a linear trend across controls, those at risk for MDD (stages 0, 1A and 1B), and those with full-threshold MDD (stages 2, 3A, 3B, 3C and 4). Subsequently, pathophysiological differences across separate stages within those at risk and with full-threshold MDD were examined. A linear increase of inflammatory markers (CRP P=0.026; IL-6 P=0.090), cortisol (P=0.025) and decrease of vitamin D (P<0.001) was found across the entire sample (for example, from controls to those at risk and those with full-threshold MDD). Significant trends of dysregulations across stages were present in analyses focusing on at-risk individuals (IL-6 P=0.050; cortisol P=0.008; vitamin D P<0.001); however, no linear trends were found in dysregulations for any of the mechanisms across more progressive stages of full-threshold MDD. Our results support that the examined pathophysiological mechanisms are involved in MDD’s etiology. These same mechanisms, however, are less important in clinical progression from first to later MDD episodes and toward chronicity.
Similar content being viewed by others

Introduction
Several biological mechanisms with a possible role in major depressive disorder (MDD)’s pathophysiology have been identified, and it has been hypothesized that these mechanisms may have a role both in the etiology and progression of the disorder. Here, we consider four central mechanisms that have substantial support in literature for their importance in depression etiology and that have previously been shown to be significantly different in MDD cases and controls in our own sample: inflammation,1 hypothalamic–pituitary (HPA) axis,2 neutrophic growth3 and vitamin D.4 We examined whether progression of MDD at a clinical level (that is, that what patient/clinicians experience as more advanced disease stage, which is multiple episodes and/or chronicity) is paralleled by more pronounced dysregulation in pathophysiological mechanisms, as evidence for that is scarce.
An upregulation of inflammation might be involved in the development of depression by decreasing the production of monoamines (for example, serotonin), and increasing the production of tryptophan catabolites that are toxic for the brain.5 Meta-analyses showed that depressed subjects in comparison with controls had significantly increased levels of the pro-inflammatory cytokine interleukin (IL)-6,6, 7, 8 and acute phase C-reactive protein (CRP).6 An example of inflammation and MDD progression is the finding that tumor necrosis factor alpha was significantly higher in those who experienced >3 episodes.5
Hyperactivity of the HPA-axis as a causal factor in MDD has been studied extensively.9 This hyperactivity is presumably caused by malfunctioning of glucocorticoid receptors impairing the negative feedback circuit of the HPA-axis. Glucocorticoid receptor malfunction might cause depression via impaired neurogenesis and reduced hippocampus volumes.10, 11 In depressed persons, cortisol levels might determine risk of12 and time to recurrence13 of an MDD episode. This suggest that HPA-axis dysfunctioning is associated with MDD progression.
Low levels of brain-derived neurotrophic factor (BDNF) are seen as an indicator of reduced neurotropic growth, a third important possible pathophysiological mechanism of MDD.14 A recent meta-analysis supports the idea that depressed patients have lower BDNF levels than controls.15 One study found that drug-free patients with a long index episode had significantly lower BDNF levels compared with patients with a shorter index episode.16
Recently low levels of vitamin D have been associated with depression in a meta-analysis.17 Different pathophysiological mechanisms have been suggested via which vitamin D might be involved with the etiology or progression of depression.18, 19 For instance, vitamin D might be neuroprotective20 by reducing neurotoxic calcium levels in the brain.21 To our knowledge, no studies exist that examined whether vitamin D is associated with the progression of depression.
The majority of previous studies were based on case–control comparisons, generally with highly heterogeneous groups with a different developmental history of depression in terms of severity, duration or number of experienced disease episodes. Examining differences in the pathophysiological mechanisms across groups of patients subdivided according to their developmental depression trajectory, for instance done by clinical staging, provides the opportunity to test whether mechanisms that are important for the etiology of depression are also important in progression of MDD at a clinical level toward multiple episodes and/or chronicity. Clinical staging is a tool to describe progression at a clinical level; it aims to divide the natural course of the disorder in clinically detectable phases that reflect disease progression and that possess clinical significance for prognosis and choice of treatment.22 Ultimately staging may contribute to early recognition of MDD development and lead to early intervention that prevents progression to later stages.23 Staging has proven useful in the fields of schizophrenia24, 25 and bipolar disorder.26 Currently, the most used staging model for MDD27 consists of eight stages. Three at-risk for MDD stages that are concerned with the initial phases of MDD development and five full-threshold MDD stages that reflect progression of MDD (Supplement Table 1). The staging model serves two purposes: (i) it puts the focus on early recognition of healthy people at risk for depression; (ii) people with a full-threshold disorder are assigned to consecutive stages of disease progression based on number and duration of the current episode, reflecting treatment necessity and prognosis.
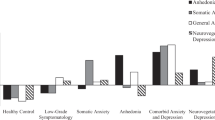
We examined whether progression of MDD at a clinical level was paralleled by more pronounced dysregulations in four central pathophysiological mechanisms. We used staging to define clinical progression of MDD. The pathophysiological mechanisms were studied via markers that reflect those mechanisms. In a large cohort, well characterized in terms of psychiatric diagnoses and clinical characteristics of MDD, we compared levels of inflammatory markers, HPA-axis hormones, BDNF and vitamin D across healthy controls (HCs), subjects in at-risk for MDD stages and full-threshold MDD stages. Using this approach, we could test two assumptions for our study (see Figure 1). First, pathophysiologic mechanisms are involved in the etiology but are not associated with clinical progression of MDD. In this case, we expect the markers to show an increasing gradient of dysregulation across ascending at-risk stages, which stabilizes across full-threshold stages. Second, the mechanisms are associated with clinical progression of MDD as well. If so, we expect the markers to show continuously increasing dysregulations across consecutive full-threshold stages. We hypothesized to find evidence for the second assumption, as a few previous studies5 suggest a role of these mechanisms beyond etiology.

Assumptions of this study. Current studies examined the association between pathophysiological mechanism in a heterogeneous group of MDD patients (a). We studied the association between pathophysiological mechanisms and groups of MDD patients divided according to the developmental course of the disorder using staging. We hypothesized that the pathophysiological mechanisms would be associated with both etiology and clinical progression of MDD. Therefore, we expected increasing dysregulations of the pathophysiological mechanisms across all the consecutive stages (progression, b). MDD, major depressive disorder.
Materials and methods
Sample
Participants were selected from the Netherlands Study of Depression and Anxiety (NESDA), an on-going cohort study into the etiology and prognosis of depressive and anxiety disorders. At baseline, 2981 adults (18–65 years) were selected from community (19%), general practice (54%) and specialized mental health care (27%) to represent the entire developmental spectrum of both disorders, including HCs. Uniform inclusion and exclusion criteria were used across recruitment settings and exactly similar measurement procedures, conducted by the same research staff, were followed in order to achieve uniform assessments. The methodology of NESDA has been extensively described elsewhere.28 The ethical review boards of contributing universities approved the study, and all participants signed informed consent. At baseline, participants gave blood samples and underwent a physical examination and a psychiatric interview. The presence of a depressive (MDD and/or dysthymia) and/or anxiety disorder (social phobia, agoraphobia, panic- and/or generalized anxiety disorder) was assessed with the DSM-IV Composite International Diagnostic Interview (CIDI) version 2.1.29 The number of MDD episodes experienced was extracted from the CIDI. The severity of depression was measured with the Inventory of Depressive Symptoms (IDS).30 The duration of depressive symptoms was examined with the Life Chart,31 calculated as the number of months with depressive symptoms in the 3 years prior to the baseline interview.
For the current study, we selected 2563 subjects of the baseline sample who were either HCs or assigned to one of the eight stages of MDD. HCs (n=230) were without a lifetime diagnosis of MDD or anxiety disorder, without depressive symptoms (IDS≤13) and without a first-degree family member with depression. The assignment of subjects to MDD stages is described in our previous paper32 and can be found in Supplement Table 1. In short, the assignment to stages is based on the lifetime presence of an MDD and/or anxiety disorder, the recency of an MDD episode (current if present in the 6 months prior to baseline, otherwise remitted), severity and duration of depressive symptoms and the number of episodes. The at-risk stages consisted of subjects without lifetime MDD or anxiety diagnosis, but with: stage 0 (n=287) a first-degree family member with depression; stage 1A (n=116) mild depressive symptoms; stage 1B (n=834) sub-threshold depressive symptoms and subjects with remitted MDD. Full-threshold stages included patients with a current MDD episode: stage 2 (n=230) first MDD episode; stage 3A (n=129) incomplete remission of first episode; stage 3B (n=127) recurrence or relapse of MDD; stage 3C (n=394) multiple relapses; stage 4 (n=216) chronic MDD.
Pathophysiological mechanism markers
Inflammatory markers
As described in more detail elsewhere,1 CRP and IL-6 were assayed at the Clinical Chemistry Department of the VU University Medical Centre from fasting blood samples obtained in the morning and kept frozen at −80 °C. High-sensitivity plasma levels of CRP were measured in duplicate by an in-house enzyme-linked immunosorbent assay based on purified protein and polyclonal anti-CRP antibodies (Dako, Glostrup, Denmark). Plasma IL-6 levels were measured in duplicate by a high-sensitivity enzyme-linked immunosorbent assay (PeliKine Compact ELISA, Sanquin, Amsterdam, The Netherlands). Intra- and inter-assay coefficients of variation were 5 and 10% for CRP, and 8% and 12% for IL-6, respectively.
A previous NESDA study1 found that currently depressed men, but not women, had higher levels of CRP (d=0.21) and IL-6 (d=0.10) than nondepressed peers. We selected 2526 (98.6%) participants with at least one available inflammatory marker. As the previous NESDA study found gender-specific associations between depression and inflammatory markers, we stratified all inflammation analyses by gender.
HPA-axis markers
As described in more detail elsewhere,2 participants collected saliva samples at home shortly after the baseline interview. Saliva samples were obtained using Salivettes (Sarstedt, Nümbrecht, Germany) at seven time points. We used four composite HPA-axis markers (i) the area under the curve with respect to the ground (AUCg, measure of the total morning cortisol secretion); and (ii) the area under the curve with respect to the increase (AUCi, measure of cortisol dynamic) were calculated if all four morning samples (T1=awakening time, T2=30, T3=45, T4=60 min later) were available by use of trapezoid formulas;33 (iii) evening cortisol (the mean of evening levels T5 at 2200 hours and T6 at 2300 hours); and (iv) the cortisol suppression ratio (a ratio obtained by dividing the cortisol value at awakening on the first day (T1) by the cortisol value at awakening on the next day (T7) after ingestion of 0.5 mg dexamethasone. This dexamethasone suppression test examines the functioning of the negative HPA-axis feedback mechanism. Our analyses included only those participants (n=1723, 67.2%) who had information on at least one of the four HPA-axis markers. Previous NESDA results2 showed that when compared with HCs, both current and remitted depressed participants had a (significantly) higher AUCg and AUCi, higher evening cortisol levels at 2200 hours, but not a different cortisol suppression ratio.
BDNF
As described in more detail elsewhere,34 serum was separated immediately after blood draw and stored (at −85 °C) until assay. Serum BDNF concentrations were determined using the Emax Immuno Assay system from Promega according to the manufacturer’s protocol (Madison, WI, USA). Absorbency was read in duplicate using a Bio-Rad Benchmark microplate reader (Hercules, CA, USA) at 450 nm. The coefficients of variance ranged between 2.9 and 8.1%. In total, 2498 (97.5%) of the subjects included in our sample had a BDNF value available. A previous NESDA paper3 showed that anti-depressant-free currently depressed participants had lower BDNF levels than both HCs and their medicated currently depressed peers.
Vitamin D
As described in more detail elsewhere,4 vitamin D was measured by assessing the blood’s circulating levels of 25(OH)D, which is the combined product of cutaneous synthesis from solar exposure and dietary sources. Serum 25(OH)D was measured using isotope dilution–online solid-phase extraction liquid chromatography–tandem mass spectrometry (ID-XLC-MS/MS).35 Intra- and inter-assay coefficients of variation were <6% and <8%, respectively, for concentrations between 25 and 180 nmol l−1. In our sample, 2514 (98.1%) subjects had a vitamin D value. A previous NESDA study4 showed that compared with controls, both currently depressed and remitted depressed had lower vitamin D levels.
Covariates
Putative covariates were selected a priori based on previous analyses and divided into general covariates and covariates specific per marker. General covariates included socio-demographic variables age (years), gender (male/female) and education (years), and health indicators smoking status (never, former and current), alcohol use (non-drinker <1 units per week; mild/moderate drinker female 1–14, male 1–21 units per week; heavy drinker female >14 and male >21 units per week),36 number of self-reported chronic diseases for which the subject received treatment (including cardiovascular diseases, diabetes, lung disease, arthritis, cancer, ulcer, intestinal problem, liver disease, epilepsy and thyroid gland disease), and body mass index expressed in kg/m2. Participants were asked to bring their medication packages to the interview after which medications were registered according to World Health Organization Anatomical Therapeutic Chemical classification.37 Covariates specific per marker included (1) for inflammation, the use of systemic anti-inflammatory drugs (M01A, M01B, A07EB and A07EC); (2) for the HPA-axis, as reported on the cortisol sampling form the factors awakening time (hh:mm), work status (yes/no) and season of saliva collection (light/dark); (3) for BDNF, the use of systemic anti-inflammatory drugs, non-opioid analgesic-antipyretics (N02BA and N02BE) and selective serotonin reuptake inhibitors (SSRI and N06AB); (4) for vitamin D, the sampling factor season of blood collection (light/dark). Season during saliva and blood collection were categorized in light months (March–September) and dark months (October–February). Inflammation, HPA-axis and vitamin D were not adjusted for antidepressant use, as previous NESDA studies1, 2, 4 showed that antidepressant use was not strongly associated with these pathophysiological markers, nor did they change the association found between depression and markers. In depressed persons, SSRI users had higher BDNF levels than non-SSRI users,3 therefore we adjusted our BDNF analyses for SSRI use.
Statistical analyses
Differences in demographic variables and covariates between HCs, the at-risk for MDD group (stages 0 through 1B) and the full-threshold MDD group (stages 2 through 4) were examined using analyses of variance and the χ2-test, followed by Games-Howell post hoc tests.
We compared levels of pathophysiological markers across subjects assembled using two different strategies (A and B). In strategy A, we contrasted the three main groups, namely, HCs, at-risk group (stages 0, 1A, and 1B combined) and full-threshold group (stages 2, 3A, 3B, 3C and 4 combined). In strategy B, we contrasted the separate stages (HCs, 0, 1A, 1B, 2, 3A, 3B, 3C and 4). For both strategy A and B, we conducted two analyses. First differences in adjusted means of the pathophysiological markers across the groups/stages were tested with analyses of covariance, followed by Tukey's Least Significant Difference (Tukey's LSD) post hoc pairwise comparisons. Second, we tested whether the biological measure showed a linear trend across the groups/stages. For strategy B (separate stages), we performed a third analysis. To examine whether a trend across all separate stages was caused by differences within at-risk stages and/or within full-threshold stages, trend analyses were repeated focusing on either the controls-at-risk stages (HCs, 0, 1A and 1B) or the full-threshold stages (2, 3A, 3B, 3C and 4).
Finally, we examined whether possible differences in pathophysiological markers across full-threshold stages could be explained by any of the more specific clinical characteristics that were used to create the MDD staging model: severity (continuous IDS score), duration (% of time with depressive symptoms in 3 years before baseline) and number of episodes. Analyses were additionally adjusted for socio-demographic factors (model 1), health indicators (model 2) and covariates specific per biological measure (model 3). Pathophysiological markers that were non-normally distributed (inflammatory markers, mean evening cortisol and cortisol suppression ratio) were log-transformed before analysis and presented back transformed. All analyses were performed with SPSS version 20.0. (SPSS, Chicago, IL, USA) Significance was set a P<0.05, using two-tailed tests.
Results
Table 1 shows the socio-demographic and health-related sample characteristics, and pathophysiological markers across HCs, the at-risk group and the full-threshold MDD group. As compared with controls, the at-risk and the full-threshold group were more often women and current smokers, had lower education, more chronic diseases and were more likely to use SSRI antidepressants or anti-inflammatory medication. Moreover, the full-threshold and at-risk groups as compared with HCs had higher CRP and cortisol levels and lower vitamin D.
Comparing pathophysiological mechanism markers
Between HCs, the at-risk for MDD group and full-threshold MDD group
Inflammatory markers: In men, we found a significant linear trend across the three main groups for both CRP and IL-6 (Table 2), even after full adjustment. The full-threshold MDD group had significantly higher CRP levels than both HCs and the at-risk group, and had significantly higher IL-6 levels than HCs. In women, no such associations were found.
HPA-axis: Both measures of the cortisol awakening response (AUCg and AUCi) were higher in the at-risk and full-threshold MDD groups when compared with controls. After full adjustment, AUCg showed an upward linear trend, but AUCi did not. Mean evening cortisol and the cortisol suppression ratio did not show a linear trend across groups after full adjustment.
BDNF: Unadjusted and fully adjusted analyses did not show a trend of BDNF levels across the three main groups.
Vitamin D: Both unadjusted and adjusted vitamin D levels showed a highly significant linear trend across the three main groups, with the at-risk group having significant lower vitamin D levels than the HCs and the full-threshold MDD group having significant lower vitamin D levels than the at-risk group.
Between separate stages
Inflammatory markers: In both men and women, CRP levels showed a significant linear trend across the separate stages from controls through stage 4, but no trend existed across the controls/at-risk stages from controls through stage 1B, or across full-threshold stages 2 through 4 (Table 3). Furthermore, in both men and women IL-6 levels showed no significant trend across all stages. However, in women across controls/at-risk stages a significant downward trend was found.
HPA-axis: AUCg showed a significant linear trend across the separate stages, a highly significant trend across HCs/at-risk stages, but no trend across full-threshold stages. AUCi only showed a linear trend across the HCs/at-risk stages. The lowest levels of AUCg and AUCi were for stage 1A, those without a history of MDD but mild symptoms. The highest levels were in stage 3A, those with an incomplete remission from a first episode. After full adjustment, no linear trend across the stages was found for the mean evening cortisol or for the cortisol suppression ratio.
BDNF: Unadjusted and fully adjusted analyses did not show any linear trend for BDNF across stages.
Vitamin D: After full adjustment, vitamin D showed a significant downward linear trend across the separate stages, meaning that later stages had lower vitamin D levels. However, follow-up trend analyses showed a significant downward linear trend across HCs/at-risk stages, but not across the full-threshold stages.
Full-threshold MDD stages explained by separate clinical characteristics
As we hardly found any indication that pathophysiological dysregulation was larger across more progressive MDD stages, we checked whether indeed associations were also absent for specific MDD clinical characteristics. Within full-threshold MDD patients, only two of the 30 tested associations between characteristics (severity-, duration- and number of episodes) and the biological markers were (borderline) significant (Table 4). Severity of depression showed a significant negative association with the AUCg level (β=−0.086, s.e.=0.040, P=0.034), and the number of episodes showed a borderline significant association with CRP in women (β=−0.067, s.e.=0.034, P=0.050).
Discussion
The present study examined whether progression of MDD at a clinical level (defined by clinical staging) was paralleled by more advanced pathophysiological dysregulations. We examined four central pathophysiological mechanisms (inflammation, HPA-axis, neurotrophic growth and vitamin D). We hypothesized that besides involvement in the etiology of MDD, these mechanisms are also associated with clinical progression of MDD, as reflected by continuously increasing dysregulation across consecutive full-threshold stages. That hypothesis was not upheld. Three (inflammation, HPA-axis and vitamin D) of the four examined pathophysiological mechanisms showed increasing trends of dysregulation across HCs and the at-risk stages (0, 1A and 1B) of depression, but not across the full-threshold stages (2, 3A, 3B, 3C and 4). These results suggest that mechanisms involved in the etiology of depression are not associated with clinical progression of depression.
Our finding that the pathophysiological mechanisms are involved in the etiology of depression confirms previous meta-analysis6, 7, 8, 9, 15, 17 and longitudinal studies.12, 38, 39, 40, 41 Interestingly, we did not find any association between BDNF and MDD groups/stages, which is in contrast with previous studies that found lower BDNF levels in untreated currently depressed patients that normalize in treated patients.15 However, our results are in line with more recent studies that showed that the association between BDNF and MDD etiology is still unclear and modest at the best; moreover, BDNF seems rather to modulate the treatment efficacy.42
We have tested the hypothesis that the examined mechanisms could also be associated with clinical progression of MDD. Although this intriguing research hypothesis generates mainly from data on animal studies,5 the few observational studies on humans supporting it included small sample sizes,43 consisted of very selective samples12, 44, 45 or only examined one aspect of depression progression, for example, recurrence.13 To our knowledge, this is the first study that, within a large sample, tested whether pathophysiological mechanisms show more dysregulation in clinically more progressed depression, as defined by the tool clinical staging. Using this approach, we found that the examined mechanisms are not more dysregulated in clinically progressed MDD. Moreover, when we examined whether the separate clinical measures (severity, duration and number of episodes) that build up the staging model were associated with more dysregulation in the pathophysiological mechanism, we did not find an association either. Together these results strongly suggest that the examined mechanisms are not more dysregulated in clinically progressed MDD. When the examined mechanisms would have shown more dysregulation in clinically progressed MDD, the mechanisms could have contributed to an index to separate different stages of MDD progression (=biomarker of stage46). The clinical utility of using pathophysiological markers as an objective measure to separate stages of disease progression is evident from somatic disorders. For instance, kidney failure knows five stadia based on the estimated glomerular filtration rate, inter alia based on serum creatinine level,47 a relatively easy and very objective measure. Stages of disease progression have clinical significance for prognosis and choice of therapeutic modality.22 For example, it has helped to make the case for early detection and to devise specific treatments for specific stages of kidney failure.47 It has been hypothesized that application of staging to MDD may have similar benefits.48, 49 However, the here examined mechanisms cannot be used as an index to separate different stages of MDD progression. It could be, however, that other pathophysiological mechanisms are more dysregulated in clinically progressed MDD. For instance, besides the mechanisms we studied for progression, Moylan et al.,5 suggest inter alia neurotransmitter systems, oxidative and nitrosative stress, mitochondrial dysfunction and epigenetic influences. Furthermore, it could be that the examined mechanisms are involved in disease progression only in certain subtypes of depression, or only in patients with certain clinical characteristics. For example, previous research has shown that upregulation of inflammation is mainly present in those with atypical depression, and hypercortisolemia in those with melancholic depression.50 Those that experienced a childhood trauma had instead lower cortisol levels.13, 51, 52 Moreover, as recently well described by Davis et al.46 it might be that the examined mechanism markers are not biomarkers of stage, but are biomarkers of diagnosis/trait (inflammation, cortisol and vitamin D) indicating whether in a person a depression is present or not, or biomarkers of treatment response (BDNF) indicating whether an individual is likely to respond to a certain treatment or not, ideally giving the clinician the opportunity to personalize treatments to individual needs. Finally, it is very well possible that clinical progression of MDD is not driven by increased dysregulation of the studied mechanisms, but rather by prolonged exposure to a chronic level of dysregulation that then leads to damage/alterations of cellular components, which subsequently could cause a person to be at further risk of recurrence or chronicity of MDD.
The main strengths of our study are the large number of well-diagnosed patients in the whole adult age range representing different developmental stages of MDD, and the availability of a wide range of important confounders regarding the examined pathophysiological mechanisms. However, our study also has some limitations. First, biological measurements were obtained via a blood draw or saliva collection, which are peripheral measurements that may not necessarily represent the ‘central/brain’ mechanism relevant for depression. However, they have been consistently associated with MDD status in previous studies.6, 7, 8, 9, 15, 17 Furthermore, whether the measured markers are the best indexes for the candidate mechanisms of depression pathophysiology has not been definitely established. Second, we used a staging model to define clinical progression of MDD in a cross-sectional sample. To make a definite statement about involvement of the mechanisms in clinical progression of MDD, a longitudinal study would be necessary in which markers are preferably measured before onset of depression, during and after the first and follow-up episodes. Third, we used the most applied staging model for MDD that stages patients mainly according to disease episode number and duration. When we separately tested the clinical characteristics of severity, duration and number of episodes, none of them were consistently associated with the measured mechanism markers. It might be that aspects of disease that were omitted in the staging model, such as complications, functional outcome and comorbidity, are of more importance for clinical MDD progression. Indeed some studies showed an association between the pathophysiological dysregulations and suicidal ideation (inflammation53 and HPA54) and comorbidity (inflammation,55 HPA56 and vitamin D57). Finally, we like to acknowledge that different staging models for MDD exist,58 besides the one we have chosen to use.27 The main difference is that those models collapse stage 3A—incomplete remission of first episode, stage 3B—first relapse and stage 3C—multiple recurrent episodes into one stage three-relapsing/reoccurring MDD. The decision to use the extensive staging model was based on our previous finding that stage 3A in general had worse characteristics than the sublevel 3B and 3C, and scores more similar as stage 4 (chronic MDD).32
In conclusion, three candidate pathophysiologic mechanisms (inflammation, HPA-axis and vitamin D) show increased dysregulation across controls and at-risk stages of development of MDD, suggesting involvement in the etiology of MDD. Nevertheless, the same mechanisms did not show more dysregulation in clinical progression of MDD toward multiple episodes and/or chronicity. This suggests that pathophysiological mechanisms for etiology and clinical disease progression are not necessarily overlapping. More (longitudinal) research on pathophysiological mechanisms that drive clinical disease progression is needed in order to be able to use dysregulations in those mechanisms as markers of clinical progression of depression and in such for staging.
References
Vogelzangs N, Duivis HE, Beekman a TF, Kluft C, Neuteboom J, Hoogendijk W et al. Association of depressive disorders, depression characteristics and antidepressant medication with inflammation. Transl Psychiatry 2012; 2: e79.
Vreeburg Sa, Hoogendijk WJ, van Pelt J, Derijk RH, Verhagen JC, van Dyck R et al. Major depressive disorder and hypothalamic-pituitary-adrenal axis activity. Arch Gen Psychiatry 2009; 66: 617–626.
Molendijk ML, Bus Baa, Spinhoven P, Penninx BW, Kenis G, Prickaerts J et al. Serum levels of brain-derived neurotrophic factor in major depressive disorder: state-trait issues, clinical features and pharmacological treatment. Mol Psychiatry 2011; 16: 1088–1095.
Milaneschi Y, Hoogendijk W, Lips P, Heijboer AC, Schoevers R, van Hemert AM et al. The association between low vitamin D and depressive disorders. Mol Psychiatry 2014; 19: 444–451.
Moylan S, Maes M, Wray NR, Berk M . The neuroprogressive nature of major depressive disorder: pathways to disease evolution and resistance, and therapeutic implications. Mol Psychiatry 2013; 18: 595–606.
Howren MB, Lamkin DM, Suls J . Associations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysis. Psychosom Med 2009; 71: 171–186.
Dowlati Y, Herrmann N, Swardfager W, Liu H, Sham L, Reim EK et al. A meta-analysis of cytokines in major depression. Biol Psychiatry 2010; 67: 446–457.
Liu Y, RC-M Ho, Mak A . Interleukin (IL)-6, tumour necrosis factor alpha (TNF-α) and soluble interleukin-2 receptors (sIL-2R) are elevated in patients with major depressive disorder: a meta-analysis and meta-regression. J Affect Disord 2012; 139: 230–239.
Stetler C, Miller GE . Depression and hypothalamic-pituitary-adrenal activation: a quantitative summary of four decades of research. Psychosom Med 2011; 73: 114–126.
Pariante CM, Lightman SL . The HPA axis in major depression: classical theories and new developments. Trends Neurosci 2008; 31: 464–468.
Manji HK, Quiroz Ja, Sporn J, Payne JL, Denicoff KA, Gray N et al. Enhancing neuronal plasticity and cellular resilience to develop novel, improved therapeutics for Difficult-to-Treat depression. Biol Psychiatry 2003; 53: 707–742.
Vrshek-Schallhorn S, Doane LD, Mineka S, Zinbarg RE, Craske MG, Adam EK . The cortisol awakening response predicts major depression: predictive stability over a 4-year follow-up and effect of depression history. Psychol Med 2013; 43: 483–493.
Bockting CLH, Lok A, Visser I, Assies J, Koeter MW, Schene AH . Lower cortisol levels predict recurrence in remitted patients with recurrent depression: a 5.5 year prospective study. Psychiatry Res 2012; 200: 281–287.
Maletic V, Robinson M, Oakes T, Iyengar S, Ball SG, Russell J . Neurobiology of depression: an integrated view of key findings. Int J Clin Pract 2007; 61: 2030–2040.
Molendijk ML, Spinhoven P, Polak M, Bus Baa, Penninx BWJH, Elzinga BM . Serum BDNF concentrations as peripheral manifestations of depression: evidence from a systematic review and meta-analyses on 179 associations (N=9484). Mol Psychiatry 2014; 19: 791–800.
Birkenhäger TK, Geldermans S, Van den Broek WW, van Beveren N, Fekkes D . Serum brain-derived neurotrophic factor level in relation to illness severity and episode duration in patients with major depression. J Psychiatr Res 2012; 46: 285–289.
Anglin RES, Samaan Z, Walter SD, McDonald SD . Vitamin D deficiency and depression in adults: systematic review and meta-analysis. Br J Psychiatry 2013; 202: 100–107.
Ganji V, Milone C, Cody MM, McCarty F, Wang YT . Serum vitamin D concentrations are related to depression in young adult US population: the Third National Health and Nutrition Examination Survey. Int Arch Med 2010; 3: 29.
Cherniack EP, Troen BR, Florez HJ, Roos Ba, Levis S . Some new food for thought: The role of vitamin D in the mental health of older adults. Curr Psychiatry Rep 2009; 11: 12–19.
Fernandes de Abreu DA, Eyles D, Féron F . Vitamin D, a neuro-immunomodulator: implications for neurodegenerative and autoimmune diseases. Psychoneuroendocrinology 2009; 34: S265–S277.
Kalueff a V, Eremin KO, Tuohimaa P . Mechanisms of neuroprotective action of vitamin D3. Biochem 2004; 69: 738–741.
Gonella J, Hornbrook M, Louis D . Staging of disease. A case-mix measurement. JAMA 1984; 251: 637–644.
Scott J, Hickie IB, McGorry P . Pre-emptive psychiatric treatments: pipe dream or a realistic outcome of clinical staging models? Neuropsychiatry (London) 2012; 2: 263–266.
Agius M, Goh C, Ulhaq S, Mcgorry P . The Staging model in schizophrenia, and its clinical implications. Psychiatr Danub 2010; 22: 211–220.
Fusar-Poli P, Yung a R, McGorry P, van Os J . Lessons learned from the psychosis high-risk state: towards a general staging model of prodromal intervention. Psychol Med 2014; 44: 17–24.
Kapczinski F, Magalhães PVS, Balanzá-Martinez V, Dias VV, Frangou S, Gama CS et al. Staging systems in bipolar disorder: an International Society for Bipolar Disorders Task Force Report. Acta Psychiatr Scand 2014; 130: 354–363.
Hetrick SE, Parker a G, Hickie IB, Purcell R, Yung a R, McGorry PD . Early identification and intervention in depressive disorders: towards a clinical staging model. Psychother Psychosom 2008; 77: 263–270.
Penninx BW, Beekman AT, Smit JH, Zitman FG, Nolen WA, Spinhoven P et al. The Netherlands Study of Depression and Anxiety (NESDA): rationale, objectives and methods. Int J Methods Psychiatr Res 2008; 17: 121–140.
Wittchen H-U . Reliability and validity studies of the WHO-Composite International Diagnostic (CIDI): a critical review. J Psychiatr Res 1994; 28: 57–84.
Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH . The Inventory of Depressive Symptomatology (IDS): psychometric properties. Psychol Med 1996; 26: 477–486.
Lyketsos CG, Nestadt G, Cwi J, Heithoff K, Eaton WW . The life chart interview: a standardized method to describe the course of psychopathology. Int J Methods Psychiatr Res 1994 4: 143–155.
Verduijn J, Milaneschi Y, van Hemert AM, Schoevers RA, Hickie IB, Penninx BWJH, et al. Clinical staging of major depressive disorder: an empirical exploration. J Clin Psychiatry 2015 76: 1–9 (in press).
Pruessner JC, Kirschbaum C, Meinlschmid G, Hellhammer DH . Two formulas for computation of the area under the curve represent measures of total hormone concentration versus time-dependent change. Psychoneuroendocrinology 2003; 28: 916–931.
Bus BAA, Molendijk ML, Penninx BJWH, Buitelaar JK, Kenis G, Prickaerts J et al. Determinants of serum brain-derived neurotrophic factor. Psychoneuroendocrinology 2011; 36: 228–239.
Heijboer AC, Blankenstein MA, Kema IP, Buijs MM . Accuracy of 6 routine 25-hydroxyvitamin D assays: influence of vitamin D binding protein concentration. Clin Chem 2012; 58: 543–548.
World Health Organization. The Alcohol Use Disorders Identification Test. Guidelines for Use in Primary Care. 2nd edn. WHO: Geneva, Switzerland, 2001.
World Health Organization Collaboration Centre for Drug Statistics Methodology Anatomical Therapeutic Chemical (ATC) Classification System. WHO: Oslo, Norway, 2007.
Valkanova V, Ebmeier KP, CRP AllanCL . IL-6 and depression: a systematic review and meta-analysis of longitudinal studies. J Affect Disord 2013; 150: 736–744.
Khandaker GM, Pearson RM, Zammit S, Lewis G, Jones PB . Association of serum interleukin 6 and C-reactive protein in childhood with depression and psychosis in young adult life: a population-based longitudinal study. JAMA Psychiatry 2014; 71: 1121–1128.
Milaneschi Y, Shardell M, Corsi AM, Vazzana R, Bandinelli S, Guralnik JM et al. Serum 25-hydroxyvitamin D and depressive symptoms in older women and men. J Clin Endocrinol Metab 2010; 95: 3225–3233.
Maddock J, Berry DJ, Geoffroy MC, Power C, Hyppönen E . Vitamin D and common mental disorders in mid-life: Cross-sectional and prospective findings. Clin Nutr 2013; 32: 758–764.
Duclot F, Kabbaj M . Epigenetic mechanisms underlying the role of brain-derived neurotrophic factor in depression and response to antidepressants. J Exp Biol 2015; 218: 21–31.
Karlović D, Serretti A, Vrkić N, Martinac M, Marčinko D . Serum concentrations of CRP, IL-6, TNF-α and cortisol in major depressive disorder with melancholic or atypical features. Psychiatry Res 2012; 198: 74–80.
Liukkonen T, Silvennoinen-Kassinen S, Jokelainen J, Räsänen P, Leinonen M, Meyer-Rochow VB et al. The association between C-reactive protein levels and depression: results from the northern Finland 1966 birth cohort study. Biol Psychiatry 2006; 60: 825–830.
Copeland WE, Shanahan L, Worthman C, Angold A, Costello EJ . Cumulative depression episodes predict later C-reactive protein levels: a prospective analysis. Biol Psychiatry 2012; 71: 15–21.
Davis J, Maes M, Andreazza A, McGrath JJ, Tye SJ, Berk M . Towards a classification of biomarkers of neuropsychiatric disease: from encompass to compass. Mol Psychiatry 2015; 20: 152–153.
NICE Chronic Kidney Disease: Early Identification and Management of Chronic kidney disease in adults in primary and secondary care. NICE, London, UK, 2015.
Mcgorry PD, Hickie IB, Yung AR, Pantelis C, Jackson HJ . Clinical staging of psychiatric disorders: a heuristic framework for choosing earlier, safer and more effective interventions. Aust N Z J Psychiatry 2006; 40: 616–622.
Fava G, Kellner R . Staging: a neglected dimension in psychiatric classification. Acta Psychiatr Scand 1993; 87: 225–230.
Penninx BWJH, Milaneschi Y, Lamers F, Vogelzangs N . Understanding the somatic consequences of depression: biological mechanisms and the role of depression symptom profile. BMC Med 2013; 11: 129.
Wiersma JE, JGFM Hovens, van Oppen P, Giltay EJ, van Schaik DJ, Beekman AT et al. The importance of childhood trauma and childhood life events for chronicity of depression in adults. J Clin Psychiatry 2009; 70: 983–989.
Berk M, Williams LJ, Jacka FN, O'Neil A, Pasco JA, Moylan S et al. So depression is an inflammatory disease, but where does the inflammation come from? BMC Med 2013; 11: 200.
O’Donovan A, Rush G, Hoatam G, Hughes BM, McCrohan A, Kelleher C et al. Suicidal ideation is associated with elevated inflammation in patients with major depressive disorder. Depress Anxiety 2013; 30: 307–314.
Hickman RJ, Khambaty T, Stewart JC . C-reactive protein is elevated in atypical but not nonatypical depression: data from the National Health and Nutrition Examination survey (NHANES) 1999-2004. J Behav Med 2014; 37: 621–629.
Hiles SA, Baker AL, de Malmanche T, Attia J . A meta-analysis of differences in IL-6 and IL-10 between people with and without depression: exploring the causes of heterogeneity. Brain Behav Immun 2012; 26: 1180–1188.
Vreeburg Sa, Hoogendijk WJG, DeRijk RH, van Dyck R, Smit JH, Zitman FG et al. Salivary cortisol levels and the 2-year course of depressive and anxiety disorders. Psychoneuroendocrinology 2013; 38: 1494–1502.
Grønli O, Kvamme JM, Jorde R, Wynn R . Vitamin D deficiency is common in psychogeriatric patients, independent of diagnosis. BMC Psychiatry 2014; 14: 134.
Cosci F, Fava Ga . Staging of mental disorders: systematic review. Psychother Psychosom 2013; 82: 20–34.
Acknowledgements
The infrastructure for the NESDA study (www.nesda.nl) is funded through the Geestkracht program of the Netherlands Organization for Health Research and Development (ZonMw, grant number 10-000-1002) and is supported by participating universities and mental health-care organizations (VU University Medical Centre, GGZ inGeest, Arkin, Leiden University Medical Centre, GGZ Rivierduinen, University Medical Centre Groningen, Lentis, GGZ Friesland, GGZ Drenthe, Institute for Quality of Health Care (IQ Healthcare), Netherlands Institute for Health Services Research (NIVEL) and Netherlands Institute of Mental Health and Addiction (Trimbos)).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
BWJHP has received research grants from NWO, BBRMI-NL, NIMH, EU-FP7 and Johnson & Johnson for research in NESDA. ATFB has been a speaker for Lundbeck and Eli Lilly, and received research grants from Astra Zeneca, Eli Lilly, Jansen and Shire for other studies, AMvH has been a speaker for Lundbeck and contributed to a web publication of GlaxoSmithKline B.V. The remaining authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Translational Psychiatry website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Verduijn, J., Milaneschi, Y., Schoevers, R. et al. Pathophysiology of major depressive disorder: mechanisms involved in etiology are not associated with clinical progression. Transl Psychiatry 5, e649 (2015). https://doi.org/10.1038/tp.2015.137
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/tp.2015.137
- Springer Nature Limited
This article is cited by
-
Effects of vitamin D supplementation on depression and some selected pro-inflammatory biomarkers: a double-blind randomized clinical trial
BMC Psychiatry (2022)
-
The effectiveness of Tai Chi on the depressive symptom of young adults with subthreshold depression: a study protocol for a randomized controlled trial
Trials (2021)
-
Brain structural network alterations related to serum cortisol levels in drug-naïve, first-episode major depressive disorder patients: a source-based morphometric study
Scientific Reports (2020)
-
Ernährung und psychische Erkrankungen
Der Nervenarzt (2017)
-
Lower Serum Zinc and Higher CRP Strongly Predict Prenatal Depression and Physio-somatic Symptoms, Which All Together Predict Postnatal Depressive Symptoms
Molecular Neurobiology (2017)