
Abstract
Background
Behaviors of substance dependence are common among patients with medication-overuse headache (MOH). Whether MOH, like other substance use disorders, is associated with an increased risk for suicide is unknown.
Methods
In this cross-sectional study, newly diagnosed chronic migraine (CM) patients with or without coexisting MOH were enrolled prospectively. Headache diagnoses were made through face-to-face interviews by headache specialists, and a specifically designed questionnaire was used to collect demographics, headache profiles, Migraine Disability Assessment, Hospital Anxiety and Depression Scale, Pittsburgh Sleep Quality Index, etc. Suicidal ideation and prior suicide attempt were specifically questioned.
Results
In total, 603 CM patients (485F/118M, mean age 42.03 ± 12.18 years) were recruited, including 320 with MOH (257F/63M, mean age 42.8 ± 11.7 years) (53.1%), and 214 (35.5%) and 81 (13.4%) had suicidal ideation and prior suicide attempt, respectively. Among CM patients, the presence of MOH increased the risks of suicidal ideation (odds ratio [OR] = 1.75 [95% CI = 1.20–2.56], p = 0.004) and prior suicide attempt (OR = 1.88 [1.09–3.24], p = 0.024), after controlling for demographics, headache profile, disabilities, symptoms of anxiety and depression, and sleep quality.
Conclusions
In CM patients, MOH is associated with an increased risk for suicidal ideation and prior suicide attempt, which deserves attention for clinicians taking care of headache patients. However, further studies are needed to determine the causal relationship, as well as the underlying pathophysiology.
Similar content being viewed by others


Background
Medication-overuse headache (MOH) is a secondary headache disorder resulting from long-term overuse of acute medications for migraine, and its prevalence was estimated at about 1% (range 0.5–7.2%) in the general population [1,2,3,4,5,6,7,8]. Prolonged excessive use of migraine acute medications could lead to worsening of the pre-existing primary headache disorders [7, 8]. In particular, overuse of acute medications is among one of the most important risk factors for migraine chronification [9,10,11]. MOH frequently coexists with chronic migraine (CM), and these two diagnoses are no longer mutually exclusive according to the Third Edition of the International Classification of Headache Disorders (ICHD-3) [12, 13]. MOH ranked among the most disabling neurological conditions according to the 2015 Global Burden of Disease study [14], and in addition to headache per se, MOH could be associated with psychiatric comorbidities [7], which makes the condition even more disabling.
Suicide is an important public health issue, and has been one of the leading causes of premature mortality, as estimated by years of life lost, around the world [15]. Patients with migraine and other chronic pain disorders are at increased risks for suicidal ideation or attempts [16,17,18,19,20,21]. Whether psychiatric comorbidities or certain psychological factors, such as mental turmoil, hopelessness, extreme sensory processing patterns, could be involved in the association remains to be elucidated [22,23,24]. On the other hand, suicide is also common in patients with substance use disorders involving alcohol, opioid, cocaine, etc., and up to 40% of patients who sought medical attention for substance use disorders had a history of suicide attempt [25]. It was also reported that cannabis use is associated with an increased risk for suicidal attempt and behavior [26], which could provide indirect evidence supportive of the association between substance use disorders and suicidal risks. The underlying mechanisms are uncertain, although reports on patients with alcohol use disorders suggested that comorbid depression is an important risk factor for suicide [27, 28]. Since two thirds of MOH patients could fulfill the criteria for substance dependence [29, 30], it could be hypothesized that MOH could share some clinical features with substance use disorders, including suicidal risks, and whether symptoms of depression or anxiety could have a role deserves exploration.
The primary objective of the present study is to compare the suicidal risks between CM patients with and without coexisting MOH, as well as to determine whether psychiatric comorbidities could be involved in the association between MOH and suicidal risks.
Methods
Patients
In this cross-sectional study, consecutive patients newly diagnosed with CM with or without a coexisting diagnosis of MOH were enrolled prospectively from the Headache Clinic of Taipei Veterans Hospital. Patients were recruited at their first visit, and were asked to complete a specifically designed questionnaire, which was followed by face-to-face interviews by headache specialists. The diagnoses of CM and MOH were made according to the ICHD-3 criteria [13]. Patients were included if they were (a) willing to participate in the study, (b) aged between 20 and 65 years, and (c) fulfilling the ICHD-3 criteria for CM. The exclusion criteria included (a) an acute headache disorder (within one month of headache onset), (b) a secondary headache disorder, and (c) difficulties completing history taking or questionnaire-based interview. The study protocol was approved by the Institutional Review Board of the Taipei Veterans General Hospital. All participants provided informed consent prior to participation.
Questionnaire-based interview
The questionnaire was designed to collect the demographic and clinical characteristics of headache patients, and included general data, past medical and surgical histories, general physical condition, headache characteristics, medication use, psychological disturbances, etc. Headache-related disability was measured by using Migraine Disability Assessment (MIDAS), and moderate and severe disability was defined as MIDAS sore ≥ 11 [31]. MIDAS has been widely used in clinical studies and drug trials, and provides a measure for lost productivities related to headache attacks [32]. Symptoms of anxiety and depression were screened with Hospital Anxiety and Depression Scale (HADS), and depression and anxiety were defined as a depression score (HADS-D) ≥ 11 and an anxiety score (HADS-A) ≥ 11, respectively [33]. HADS is a 14-item instrument commonly used in the screening of anxiety and depressive disorders in the hospital setting [32, 33]. Sleep disturbances were assessed by using Pittsburgh Sleep Quality Index (PSQI), and a PSQI of > 5 was defined as poor sleep quality [34]. PSQI includes 19 self-rated questions designed to evaluate the quality and patterns of sleep in the previous month [34]. Lifetime suicidal ideation and attempt were assessed by two separate direct questions, i.e. “have you ever had ideational thoughts of engaging in suicidal behavior?” and have you ever had engaged in any self-injurious behavior with the intent to die?” These two questions, along with other parts of the questionnaire, were answered by the patients themselves, and the responses were confirmed at the time of subsequent face-to-face interviews by headache specialists.
Statistical analysis
Descriptive data were expressed as mean ± standard deviation or number (percentages). Subjects with incomplete questionnaires, i.e. those with > 5% of the items unanswered, were excluded from analysis. Continuous variables, such as age, headache frequency, number of days with analgesic use, scores of neuropsychological instruments, etc. between groups were compared by using student’s t test. Chi-square test was used to compare categorical variables, such as sex, marital status, education level, employment status, suicidal ideation, prior suicide attempt, etc. Logistic regression modeling (backward stepwise, conditional) was carried out to estimate the odds ratios (ORs), as well the 95% confidence intervals (CIs), for suicide risks in patients with MOH as compared with those without, adjusted for potential confounders. All statistical analyses were carried out with SAS 9.4 (SAS Institute Inc., Cary, NC, USA). Statistical significance was defined as p < 0.05.
Results
Study participants
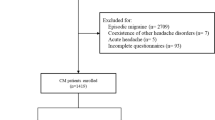
During the study period, 2736 consecutive headache patients (1924F/812M, mean age 41.41 ± 13.38 years, range 20–65) were screened at their first visit, and 2107 were excluded for diagnosis other than CM. Among patients diagnosed as CM, 26 were further excluded for incomplete questionnaires. In total, 603 CM patients (485F/118M, mean age 42.0 ± 12.2 years) were included for the analysis, consisting of 320 with MOH (257F/63M, mean age 42.8 ± 11.7 years) (53.1%) and 283 without (228F/55M, mean age 41.2 ± 12.7 years) (Table 1) (Fig. 1).

Patient recruitment in the present study
Comparisons between chronic migraine patients with and without medication overuse headache
Patients with MOH had lower education levels (high school or below: 57.5% vs. 44.5%, p = 0.002), earlier onset of migraine (mean age at onset: 20.7 ± 9.1 vs. 23.0 ± 10.9 years, p = 0.004), and more frequent analgesic use (19.4 ± 7.8 vs. 4.5 ± 6.3 days per month with analgesic use, p < 0.001), when compared with those without (Table 1). Besides, there was a trend toward an older age (mean age 42.8 ± 1.7 vs. 41.2 ± 12.7 years, p = 0.093), higher headache frequencies (23.3 ± 6.9 vs. 22.4 ± 7.4, p = 0.098) in MOH patients. However, the distributions of patient with moderate to severe disability (MIDAS ≥11) (75.5% vs. 70.5%, p = 0.168), depression (HADS-D ≥ 11) (29.2% vs. 25.1%, p = 0.272), anxiety (HADS-A ≥ 11) (43.7% vs. 43.1%, p = 0.934), or poor sleep quality (PSQI > 5) (90.2% vs. 90.4%, p = 1.000) were comparable.
Medication-overuse headache as a risk factor for suicide
Among the study participants, 214 (35.5%) and 81 (13.4%) had suicidal ideation and prior suicide attempt at some time in their lives, respectively. As compared with those without, CM patients with MOH were more likely to have suicidal ideation (41.6% vs. 29.4%, p = 0.002) and prior suicide attempt (16.7% vs. 10.1%, p = 0.018) (Fig. 2). Among CM patients, the presence of MOH was associated with increased risks of suicidal ideation (OR = 1.71 [95% CI = 1.22–2.41], p = 0.002) and prior suicide attempt (OR = 1.78 [1.10–2.92], p = 0.019). The associations remained significant after controlling for demographics, headache profile, migraine-related disability, and the presence of depression, anxiety, and poor sleep quality (suicidal ideation: OR = 1.75 [1.20–2.56], p = 0.004; prior suicide attempt: OR = 1.88 [1.09–3.24], p = 0.024) (Table 2).

Proportions of patients with suicidal ideation and prior suicide attempt in chronic migraine patients with and without medication-overuse headache
Discussion
Among CM patients, patients with MOH were more likely to have suicidal ideation (41.6% vs. 29.4%, p = 0.002) and prior suicide attempt (16.7% vs. 10.1%, p = 0.018) (Fig. 2) when compared with those without. The presence of MOH was associated with increased risks for suicidal ideation (OR = 1.75 [95% CI = 1.20–2.56], p = 0.004) and suicide attempt (OR = 1.88 [1.09–3.24], p = 0.024), and the association was not accounted for by potential confounders, including demographics, headache profiles, migraine-related disability, psychiatric comorbidities, or sleep quality (Table 2). The findings highlight the importance of paying special attention to the risks of suicide in the management of patients with MOH.
One of the most important strengths is the relatively large sample size. More than 600 newly diagnosed CM patients with or without MOH were enrolled consecutively, which could potentially reduce selection bias. The data were of high quality and reliability. The diagnoses of CM and MOH were made through face-to-face interviews by experienced headache specialists, rather than just questionnaires, and well-validated and widely accepted neuropsychological instruments were utilized in the current study. Third, suicidal risks in MOH were assessed by using single direct questions followed by confirmation by the headache specialists, rather than psychiatric interviews. Such an approach could be more readily implemented in routine daily practice. Patients at risk could be efficiently identified and subsequently referred for formal psychiatric assessment. Therefore, the findings could have a more practical implication for neurologists.
In the current study, an association between MOH and suicidal risks was identified. In particular, comparisons were made between CM patients with and without MOH, and therefore, the finding were more likely to be pertinent to MOH per se. According to data of World Mental Health Surveys (WMHS), which were a series of national surveys for mental disorders by the World Health Organization, alcohol use disorders and drug use disorders were associated with increased risks for suicidal ideation (alcohol: OR = 2.0–2.5; drug: OR = 2.3–3.0) and attempt (alcohol: OR = 2.6–3.7; drug: OR = 2.0–4.0) [35, 36]. As MOH share many clinical features of substance use disorders [29, 30], the findings of the current study were actually in keeping with those in the WMHS, although suicidal risks in MOH were not as high as those in substance use disorders. Suicidal ideation and prior suicide attempts were reported to increase the risk of completed suicide [35, 37, 38], and identification of patients at risk is crucial in the prevention of suicide [39]. Besides, suicidal risks were found to be associated with compromised quality of life in patients with chronic daily headache (CDH) and MOH [22]. Therefore, it is important to be alert to the potential risk of suicide in taking care of patients with MOH.
The mechanisms underlying the association between MOH and suicide risks are unknown. It could be possible that psychiatric comorbidities might play a role. In particular, depressive and anxiety disorders are not uncommon in patients with migraine and CDH with MOH, and it could be possible that these psychiatric comorbidities could potentially participate in the association [22, 23]. However, the association between suicidal risks and MOH remained significant after controlling for depression and anxiety in the present cohort (Table 2). On the other hand, certain psychosocial factors shared by suicide, chronic pain, and even substance use disorders, could be involved, such as perceived burdensomeness, thwarted belongingness, defeat, etc. [40,41,42,43,44]. Besides, extreme sensory processing patterns implicated in emotional processes, depression, and suicidality could also have a role [24]. However, further studies are needed to clarify whether there could be mediating effects from these factors. Besides, since it is not uncommon for MOH patients to have concomitant overuse of tobacco, caffeine, or sedatives/anxiolytics [30], whether these centrally acting agents could also have a role remains to be determined. Further studies are needed to confirm our findings, as well as to explore the underlying mechanisms.
There are also some limitations. The study recruited patients from a tertiary referral center, and therefore, there could be concerns about the generalizability of the results. However, a relatively large cohort of consecutive patients were enrolled, which could potentially minimize selection bias. A formal referral system is being developed in the healthcare system of our country, and most of our patients accessed us directly without referral. Therefore, the results could reflect what could be seen in the general population to a certain extent. Second, the risk of suicidal ideation or prior suicide attempt was evaluated by two self-administered single-item direct questions rather than formal face-to-face interviews by psychiatrists, and the validity of such an approach is not without doubt [45, 46]. However, self-report was, in fact, demonstrated to be comparable to clinical interviews in suicide assessment [47]. Besides, even though single-item questions could lead to misclassification, the majority of patients with a positive response were still qualified as having increased suicidal risks [47]. Nevertheless, the lack of a validated measure for suicide remains an important concern. The findings were, in fact, extrapolated from the answers to these two self-administered questions at the time of clinical evaluation, and whether those with a positive response would really have suicidal ideation or behavior in the future needs to be further confirmed. Third, the levels of depression or anxiety, as defined by scores of HADS, rather than formal psychiatric diagnoses, were used in this study, which could potentially introduce some concerns. However, this approach has been commonly used and widely accepted in clinical studies involving questionnaires, and the cut-off scores were actually validated in clinical studies [33]. Fourth, patients with > 5% of the items in the questionnaire unanswered were excluded from the analysis, which could introduce some selection bias as such patients might have clinical profiles different from those included in the analysis. However, only a small proportion of patients were excluded for this reason (n = 26) (Fig. 1), which could have little impact on the results in the current study. Fifth, what the current study reported was an association between MOH and suicidality. The causal relationship could be further investigated by longitudinal studies involving MOH patients without prior suicidal ideation or attempt at baseline, and new-onset suicidal ideation or attempt at follow-up would help determine the causality or directionality of the association. Besides, complete psychological evaluations in these patients would help clarify the psychological mechanisms that could be involved.
Conclusions
The present study identified an association between MOH and suicidal risks in patients with CM, suggestive of a potential link between behaviors of dependence and suicide. The potential risks of suicide should not be overlooked in clinical practice for clinicians taking care of patients with MOH. However, the causal relationship and underlying mechanisms are uncertain, and further longitudinal studies are needed to clarify the causal relationship and the directionality of the association.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CDH:
-
Chronic daily headache
- CI:
-
Confidence interval
- CM:
-
Chronic migraine
- HADS:
-
Hospital Anxiety and Depression Scale
- HADS-A:
-
Anxiety subscale of Hospital Anxiety and Depression Scale
- HADS-D:
-
Depression subscale of Hospital Anxiety and Depression Scale
- ICHD-3:
-
Third Edition of the International Classification of Headache Disorders
- MIDAS:
-
Migraine Disability Assessment Scale
- MOH:
-
Medication-overuse headache
- OR:
-
Odds ratio
- PSQI:
-
Pittsburgh Sleep Quality Index
- WMHS:
-
World Mental Health Surveys
References
Scher AI, Stewart WF, Liberman J, Lipton RB (1998) Prevalence of frequent headache in a population sample. Headache. 38(7):497–506. https://doi.org/10.1046/j.1526-4610.1998.3807497.x
Wang SJ, Fuh JL, Lu SR, Liu CY, Hsu LC, Wang PN, Liu HC (2000) Chronic daily headache in Chinese elderly: prevalence, risk factors, and biannual follow-up. Neurology. 54(2):314–319. https://doi.org/10.1212/WNL.54.2.314
Lu SR, Fuh JL, Chen WT, Juang KD, Wang SJ (2001) Chronic daily headache in Taipei, Taiwan: prevalence, follow-up and outcome predictors. Cephalalgia. 21(10):980–986. https://doi.org/10.1046/j.1468-2982.2001.00294.x
Prencipe M, Casini AR, Ferretti C, Santini M, Pezzella F, Scaldaferri N, Culasso F (2001) Prevalence of headache in an elderly population: attack frequency, disability, and use of medication. J Neurol Neurosurg Psychiatry 70(3):377–381. https://doi.org/10.1136/jnnp.70.3.377
Lanteri-Minet M, Auray JP, El Hasnaoui A, Dartigues JF, Duru G, Henry P et al (2003) Prevalence and description of chronic daily headache in the general population in France. Pain. 102(1–2):143–149. https://doi.org/10.1016/s0304-3959(02)00348-2
Westergaard ML, Glumer C, Hansen EH, Jensen RH (2014) Prevalence of chronic headache with and without medication overuse: associations with socioeconomic position and physical and mental health status. Pain. 155(10):2005–2013. https://doi.org/10.1016/j.pain.2014.07.002
Diener HC, Dodick D, Evers S, Holle D, Jensen RH, Lipton RB, et al (2019) Pathophysiology, prevention, and treatment of medication overuse headache. Lancet Neurol 18(9):891–902. https://doi.org/10.1016/S1474-4422(19)30146-2
Chen PK, Wang SJ (2019) Medication overuse and medication overuse headache: risk factors, comorbidities, associated burdens and nonpharmacologic and pharmacologic treatment approaches. Curr Pain Headache Rep 23(8):60. https://doi.org/10.1007/s11916-019-0796-7
Scher AI, Stewart WF, Ricci JA, Lipton RB (2003) Factors associated with the onset and remission of chronic daily headache in a population-based study. Pain. 106(1–2):81–89. https://doi.org/10.1016/S0304-3959(03)00293-8
Zwart JA, Dyb G, Hagen K, Svebak S, Holmen J (2003) Analgesic use: a predictor of chronic pain and medication overuse headache: the head-HUNT study. Neurology. 61(2):160–164. https://doi.org/10.1212/01.WNL.0000069924.69078.8D
Katsarava Z, Schneeweiss S, Kurth T, Kroener U, Fritsche G, Eikermann A, Diener HC, Limmroth V (2004) Incidence and predictors for chronicity of headache in patients with episodic migraine. Neurology. 62(5):788–790. https://doi.org/10.1212/01.WNL.0000113747.18760.D2
May A, Schulte LH (2016) Chronic migraine: risk factors, mechanisms and treatment. Nat Rev Neurol 12(8):455–464. https://doi.org/10.1038/nrneurol.2016.93
Headache Classification Committee of the International Headache Society (IHS) (2018) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 38(1):1–211
Group GBDNDC (2017) Global, regional, and national burden of neurological disorders during 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet Neurol 16(11):877–897
Naghavi M (2019) Global Burden of Disease Self-Harm C. Global, regional, and national burden of suicide mortality 1990 to 2016: systematic analysis for the Global Burden of Disease Study 2016. BMJ 364:l94
Wang SJ, Juang KD, Fuh JL, Lu SR (2007) Psychiatric comorbidity and suicide risk in adolescents with chronic daily headache. Neurology. 68(18):1468–1473. https://doi.org/10.1212/01.wnl.0000260607.90634.d6
Pompili M, Serafini G, Di Cosimo D, Dominici G, Innamorati M, Lester D et al (2010) Psychiatric comorbidity and suicide risk in patients with chronic migraine. Neuropsychiatr Dis Treat 6:81–91. https://doi.org/10.2147/ndt.s8467
Breslau N, Schultz L, Lipton R, Peterson E, Welch KM (2012) Migraine headaches and suicide attempt. Headache. 52(5):723–731. https://doi.org/10.1111/j.1526-4610.2012.02117.x
Fuller-Thomson E, Schrumm M, Brennenstuhl S (2013) Migraine and despair: factors associated with depression and suicidal ideation among Canadian Migraineurs in a population-based study. Depress Res Treat 2013:401487
Liu HY, Fuh JL, Lin YY, Chen WT, Wang SJ (2015) Suicide risk in patients with migraine and comorbid fibromyalgia. Neurology. 85(12):1017–1023. https://doi.org/10.1212/WNL.0000000000001943
Tang NK, Crane C (2006) Suicidality in chronic pain: a review of the prevalence, risk factors and psychological links. Psychol Med 36(5):575–586. https://doi.org/10.1017/S0033291705006859
De Filippis S, Erbuto D, Gentili F, Innamorati M, Lester D, Tatarelli R et al (2008) Mental turmoil, suicide risk, illness perception, and temperament, and their impact on quality of life in chronic daily headache. J Headache Pain. 9(6):349–357. https://doi.org/10.1007/s10194-008-0072-4
Pompili M, Di Cosimo D, Innamorati M, Lester D, Tatarelli R, Martelletti P (2009) Psychiatric comorbidity in patients with chronic daily headache and migraine: a selective overview including personality traits and suicide risk. J Headache Pain 10(4):283–290. https://doi.org/10.1007/s10194-009-0134-2
Serafini G, Gonda X, Canepa G, Pompili M, Rihmer Z, Amore M, Engel-Yeger B (2017) Extreme sensory processing patterns show a complex association with depression, and impulsivity, alexithymia, and hopelessness. J Affect Disord 210:249–257. https://doi.org/10.1016/j.jad.2016.12.019
Yuodelis-Flores C, Ries RK (2015) Addiction and suicide: a review. Am J Addict 24(2):98–104. https://doi.org/10.1111/ajad.12185
Serafini G, Pompili M, Innamorati M, Rihmer Z, Sher L, Girardi P (2012) Can cannabis increase the suicide risk in psychosis? A critical review. Curr Pharm Des 18(32):5165–5187. https://doi.org/10.2174/138161212802884663
Conner KR, Beautrais AL, Conwell Y (2003) Risk factors for suicide and medically serious suicide attempts among alcoholics: analyses of Canterbury suicide project data. J Stud Alcohol 64(4):551–554. https://doi.org/10.15288/jsa.2003.64.551
Sher L, Stanley BH, Harkavy-Friedman JM, Carballo JJ, Arendt M, Brent DA, Sperling D, Lizardi D, Mann JJ, Oquendo MA (2008) Depressed patients with co-occurring alcohol use disorders: a unique patient population. J Clin Psychiatry 69(6):907–915. https://doi.org/10.4088/JCP.v69n0604
Fuh JL, Wang SJ, Lu SR, Juang KD (2005) Does medication overuse headache represent a behavior of dependence? Pain. 119(1–3):49–55. https://doi.org/10.1016/j.pain.2005.09.034
Radat F, Creac'h C, Guegan-Massardier E, Mick G, Guy N, Fabre N et al (2008) Behavioral dependence in patients with medication overuse headache: a cross-sectional study in consulting patients using the DSM-IV criteria. Headache. 48(7):1026–1036. https://doi.org/10.1111/j.1526-4610.2007.00999.x
Stewart WF, Lipton RB, Kolodner KB, Sawyer J, Lee C, Liberman JN (2000) Validity of the migraine disability assessment (MIDAS) score in comparison to a diary-based measure in a population sample of migraine sufferers. Pain. 88(1):41–52. https://doi.org/10.1016/S0304-3959(00)00305-5
Peng KP, Wang SJ (2012) Migraine diagnosis: screening items, instruments, and scales. Acta Anaesthesiol Taiwanica 50(2):69–73. https://doi.org/10.1016/j.aat.2012.05.002
Zigmond AS, Snaith RP (1983) The hospital anxiety and depression scale. Acta Psychiatr Scand 67(6):361–370. https://doi.org/10.1111/j.1600-0447.1983.tb09716.x
Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ (1989) The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res 28(2):193–213. https://doi.org/10.1016/0165-1781(89)90047-4
Nock MK, Borges G, Bromet EJ, Alonso J, Angermeyer M, Beautrais A, Bruffaerts R, Chiu WT, de Girolamo G, Gluzman S, de Graaf R, Gureje O, Haro JM, Huang Y, Karam E, Kessler RC, Lepine JP, Levinson D, Medina-Mora ME, Ono Y, Posada-Villa J, Williams D (2008) Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry 192(2):98–105. https://doi.org/10.1192/bjp.bp.107.040113
Borges G, Loera CR (2010) Alcohol and drug use in suicidal behaviour. Curr Opin Psychiatry 23(3):195–204. https://doi.org/10.1097/YCO.0b013e3283386322
Haukka J, Suominen K, Partonen T, Lonnqvist J (2008) Determinants and outcomes of serious attempted suicide: a nationwide study in Finland, 1996-2003. Am J Epidemiol 167(10):1155–1163. https://doi.org/10.1093/aje/kwn017
Hubers AAM, Moaddine S, Peersmann SHM, Stijnen T, van Duijn E, van der Mast RC, Dekkers OM, Giltay EJ (2018) Suicidal ideation and subsequent completed suicide in both psychiatric and non-psychiatric populations: a meta-analysis. Epidemiol Psychiatr Sci 27(2):186–198. https://doi.org/10.1017/S2045796016001049
Mann JJ, Apter A, Bertolote J, Beautrais A, Currier D, Haas A, Hegerl U, Lonnqvist J, Malone K, Marusic A, Mehlum L, Patton G, Phillips M, Rutz W, Rihmer Z, Schmidtke A, Shaffer D, Silverman M, Takahashi Y, Varnik A, Wasserman D, Yip P, Hendin H (2005) Suicide prevention strategies: a systematic review. JAMA. 294(16):2064–2074. https://doi.org/10.1001/jama.294.16.2064
Kirtley OJ, Rodham K, Crane C (2020) Understanding suicidal ideation and behaviour in individuals with chronic pain: a review of the role of novel transdiagnostic psychological factors. Lancet Psychiatry 7(3):282–290. https://doi.org/10.1016/S2215-0366(19)30288-3
Buckner JD, Lemke AW, Walukevich KA (2017) Cannabis use and suicidal ideation: test of the utility of the interpersonal-psychological theory of suicide. Psychiatry Res 253:256–259. https://doi.org/10.1016/j.psychres.2017.04.001
Lamis DA, Malone PS (2011) Alcohol-related problems and risk of suicide among college students: the mediating roles of belongingness and burdensomeness. Suicide Life Threat Behav 41(5):543–553. https://doi.org/10.1111/j.1943-278X.2011.00052.x
Conner KR, Britton PC, Sworts LM, Joiner TE Jr (2007) Suicide attempts among individuals with opiate dependence: the critical role of belonging. Addict Behav 32(7):1395–1404. https://doi.org/10.1016/j.addbeh.2006.09.012
Montagud-Romero S, Blanco-Gandia MC, Reguilon MD, Ferrer-Perez C, Ballestin R, Minarro J et al (2018) Social defeat stress: mechanisms underlying the increase in rewarding effects of drugs of abuse. Eur J Neurosci 48(9):2948–2970. https://doi.org/10.1111/ejn.14127
Millner AJ, Lee MD, Nock MK (2015) Single-item measurement of suicidal behaviors: validity and consequences of misclassification. PLoS One 10(10):e0141606. https://doi.org/10.1371/journal.pone.0141606
Hom MA, Joiner TE, Bernert RA (2016) Limitations of a single-item assessment of suicide attempt history: implications for standardized suicide risk assessment. Psychol Assess 28(8):1026–1030. https://doi.org/10.1037/pas0000241
Kaplan ML, Asnis GM, Sanderson WC, Keswani L, De Lecuona JM, Joseph S (1994) Suicide assessment: clinical interview vs. self-report. J Clin Psychol 50(2):294–298. https://doi.org/10.1002/1097-4679(199403)50:2<294::AID-JCLP2270500224>3.0.CO;2-R
Acknowledgements
The authors would like to thank the study participants for their contributions.
Funding
The study was sponsored in part by Taiwan Ministry of Science and Technology [MOST 109–2314-B-075 -054 (to YFW), and MOST 108–2321-B-010-014 -MY2, 108–2321-B-010-001, 108–2314-B-010-023-MY3, and 110–2321-B-010-005 (to SJW)]; and Taipei Veterans General Hospital [VGH 108-C-092, VGH 109-C-096, and VGH 110-C-111 (to YFW)]; this work was also supported by the Brain Research Center, National Yang Ming Chiao Tung University from The Featured Areas Research Center Program within the framework of the Higher Education Sprout Project by the Ministry of Education (MOE) in Taiwan. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
YFW and SJW conceived and designed the study, acquired the data, and completed the first draft. YFW, CCY, ASK, and SJW analyzed the data. SPC participated in the discussion and critical revision of the manuscript. The authors have read and approved the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board at the Taipei Veterans General Hospital (VGHTPE IRB No. 2018–07-020 BC, 2019–07-002CC). All participants provided informed consent prior to participation.
Consent for publication
Not applicable.
Competing interests
YFW has received honoraria as a speaker from Taiwan branches of AbbVie, Eli Lilly, Novartis, Pfizer, Sanofi, and UCB. He has received research grants from the Taiwan Ministry of Science and Technology, and Taipei Veterans General Hospital. SJW has served on the advisory boards of Eli Lilly, Daiichi-Sankyo, and Taiwan Novartis. He has received honoraria as a moderator from Taiwan branches of AbbVie, Bayer, Eisai, Eli Lilly, and Pfizer. He has received research grants from the Taiwan Ministry of Science and Technology, National Yang-Ming University, Taipei Veterans General Hospital, Taiwan Headache Society, and Taiwan branches of Eli Lilly, Novartis, and Pfizer. CCY, ASK and SPC reported no disclosures relevant to the manuscript.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Wang, YF., Yu, CC., Kuan, A.S. et al. Association between suicidal risks and medication-overuse headache in chronic migraine: a cross-sectional study. J Headache Pain 22, 36 (2021). https://doi.org/10.1186/s10194-021-01248-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-021-01248-0