
Abstract
Background
Idiopathic intracranial hypertension (IIH) is a cause of chronic headaches that are probably driven by raised intracranial pressure (ICP). Cerebral venous sinus pressure is thought to play a role in the underlying pathology, but its relation with intracranial pressure requires further investigation. We aimed to evaluate the concordance between lumbar puncture opening pressure (LPOP) as indicator of the ICP and cerebral venous sinus pressure in patients investigated for IIH.
Methods
In this case-series replication study, all patients with IIH suspicion and who underwent cerebral venous sinus pressure measurement followed immediately by LP opening pressure (LPOP) measurement were retrospectively included. Pearson’s correlation and measurement agreement (Bland-Altman plots) between venous pressure and LPOP were analyzed.
Results
52 consecutive patients (46 women; median age, 31 years [IQR = 25–42]) were included. The mean pressure in the superior sagittal sinus (SSS) and in the torcular were 20.9mmHg (SD ± 7.3) and 20.8 mmHg (SD ± 6.8), respectively. The mean LPOP was 22mmHg (SD ± 6.4). Pressure measured in the transverse venous sinus, the torcular, and the SSS correlated with LPOP (p < 0.001). Bland-Altman plots showed that torcular pressure strongly agreed with LPOP (mean difference of 1.7mmHg). The limit of agreement (LOA) (mean difference ± 1.96SD) contained 98.1% of the differences between the two methods, confirming the concordance between the two measures. Torcular pressure and LPOP were consistent in patients with a trans-stenotic pressure gradient ≥ or < to 8 mmHg (mean difference: 1mmHg and 2.4mmHg, respectively), and for those with a LP OP ≥ or < to 18mmHg (mean difference: 1.8mmHg and 1.95mmHg, respectively).
Conclusions
In patients investigated for IIH, the ICP measured at the LP is correlated and concordant with the torcular pressure. These results confirm previous findings and further corroborate the hypothesis that cerebral venous system plays a major role in CSF dynamics and ICP.
Similar content being viewed by others
Background
Idiopathic intracranial hypertension (IIH) is a pathology characterized by elevated intracranial pressure (ICP) causing disabling secondary headache, hearing disturbance, and papilledema with a risk of visual impairment [1]. Headache is usually temporally related to the increased ICP, although 50% of IIH patients describe a persistent chronic headache despite ICP normalization [2]. The exact etiology of IIH is still not well understood. A growing body of literature confirms that IIH is a complex metabolic disorder strongly associated with obesity and female sex [3]. The relationship between cerebral venous pressure and cerebrospinal fluid (CSF) resorption via the arachnoid granulations is a well described mechanism playing an important role in the homeostasis of ICP [4, 5]. Recent evidence suggests that venous sinus congestion promotes the ICP elevation by creating a positive feed-back loop: the ICP elevation augments the severity of the venous sinus stenosis, leading to progressive outflow obstruction and resulting in additional venous congestion, which then leads to further ICP elevation. Nevertheless, it is still debated whether the initial sinus stenosis is a contributing cause or a consequence of ICP elevation, but a close relationship between the cerebral venous outflow and ICP has been recently confirmed [6, 7].
The ICP, following IIH management guidelines, is estimated through lumbar punction (LP) in in lateral decubitus [1]. Consequently, various large studies aimed to elucidate the relationship between venous pressures and LP opening pressure (LPOP) [7,8,9]. Although strong correlations were observed, LPOP was generally measured at a different time and place, potentially impacting the validity of the observed correlation. To overcome this pitfall, Lee et al. (2021), evaluated the correlation between LPOP and cerebral venous pressure in IIH, when measured consecutively [6]. They demonstrated a near one-to-one correlation between the torcular pressure and the LPOP, that was significantly impacted by gender, race and BMI. Consequently, the authors suggested that elevations in ICP are proportionally linked to elevations in sinus pressure. And although a correlation provides important information about the relationship between two variables, it does not account for differences in the means. Indeed, their data showed an important difference between the absolute pressure values measured at LP and those obtained in the SSS or torcular: the mean pressures in SSS and torcular were 25.5mmHg and 23.8mmHg respectively, while the mean LPOP was 18.6mmHg. A simple way to address such differences in the mean, is by estimating the measure agreement through a concordance analysis rather than a correlation analysis, as a good agreement requires both a good correlation and a small measurement bias [10].
Thus all-in-all, a strong correlation between venous pressure and LPOP pressure has previously been demonstrated in a single operator and single center case series study. To confirm the generalizability of these findings and contribute to further understanding of the measures’ relationship, we here propose a replication study that (1) takes into account both the concordance and the correlation between measures, (2) using a standardized procedure that was performed by two different experienced operators and (3) subgroup analyses with clinically significant pressure cut-off values. Therefore, we included consecutive patients with suspicion of IIH who received venous sinus pressure measurement followed immediately by a LPOP using the same pressure measurement technology. We hypothesized that cerebral venous sinus pressure is concordant with LPOP in patients with suspicion of IIH, especially for patients with a gradient above trans-stenotic pressure gradient cut-off. If this is proven correct, it supports the idea that CSF pressure elevation occurs in concert with proportional venous sinus pressure elevation, and thus corroborating the hypothesis that venous sinus impairment is a pivotal element in the pathogenesis of IIH.
Materials and methods
Patient selection
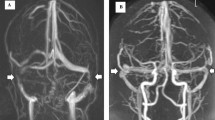
Since January 2021, in all patients with clinical and/or radiological suspicion of IIH intracranial venous sinus pressure and LPOP are standardly measured during the same procedure at our neuroradiological intervention unit following multidisciplinary IIH expert consensus. Patients with suspicion of IIH are referred (a) to the ophthalmological department, mostly when presented with visual disturbance or diagnosed with papilledema diagnosis at a peripheral hospital, (b) to the neurological department, mostly when presented with headache, or (c) to the emergency department, mostly in case of severe headache or sudden onset visual disturbance. IIH suspicion is confirmed by the presence of a combination of neurological (pressure headache, tinnitus, visual disturbances), ophthalmological (optic disc oedema), and MRI symptoms (empty sella, optic hydrops, transverse venous sinus stenosis, flattening of the posterior aspect of the globe, distension of the peri optic subarachnoid space). Accordingly, all consecutive patients with suspicion of IIH underwent intracranial venous sinus pressure and LPOP. Definite IIH diagnosis is based on the modified Dandy criteria [1], and it is confirmed after pressure measurement at the LP in lateral decubitus. Exclusion criteria included: (1) presence of other identifiable causes of ICP elevation; (2) patients < 18-year-old; and (3) presence of LP contraindications.
Data collection included demographic data, comprehensive venous sinus pressure evaluation, internal jugular (IJ) pressure, central venous pressure (CVP), location of stenosis, trans-stenotic gradient, and LPOP with CSF samples collected immediately after venous pressure measurement. MRI was used to obtain the degree of the transverse venous sinus (TVS) stenosis on MRI venography as a percent of stenosis following “1-(smallest diameter/normal diameter)” [11]; grade of loss of pituitary height (concavity) evaluated on sagittal T1-weighted images: I: normal, II: superior concavity that was mild (<1/3 the height of the sella), III: moderate (between 1/3 and 2/3), IV: severe (>1/3 concavity of height of sella), and V: empty sella [12]; length of the TVS; transverse diameter of the Meckel cave on T2-weighted coronal sequences; and posterior globe flattening and optic nerve sheath distension on T2-weighted axial and coronal sequences [13]. Clinical data included: presence of headache classified as episodic (< 15 episodes per month) and chronic (≥ 15 episodes/month for at least 3 months) [14]; visual acuity impairment (number of correct letters); optic disc swelling (Frisen classification: grades 0–5) [15].
Decision for pressure measurement was made after multidisciplinary consensus (neurologists, neuroradiologists, neurosurgeons, and ophthalmologists with experience in IIH). Procedures were performed by two neuroradiologists with over 5-years of experience in IIH management.
Study objectives
The primary objective of this study was to establish the concordance between the ICP values obtained with a transvenous access in the cerebral venous sinuses and ICP estimations obtained by LPOP in lateral decubitus, being the gold standard for ICP assessment in patients with suspected IIH [1].
The secondary objective was to evaluate whether the relation between cerebral venous sinus pressure and LPOP was modified by the degree of trans-stenotic pressure (< 8mmHg vs. ≥8mmHg), and/or LPOP pressure (< 18mmHg and ≥18mmHg). The trans-stenotic pressure gradient of 8mmHg was chosen because it is the commonly accepted cut-off for venous stenting [7]. The cut-off of 18mmHg at LP (approximately 25cmH2O) was selected as threshold between “normal” (< 18mmHg) and “pathological” (≥18mmHg) ICP in IIH patients, based on the diagnostic criteria of pseudo-tumor cerebri [1].
Procedure description
Before pressure measurements, all patients received full ophthalmological and neurological examination, as well as a contrast-enhanced cerebral MRI, as described above. Patients under acetazolamide treatment were instructed to stop intake 5 days prior to the procedure. Five days were considered sufficient based on acetazolamide’s 6-hour elimination half time [16] combined with the fact that about five half-times are required to eliminate roughly 97% of a drug from our body. No patients were under topiramate. The procedure was performed under pure local anesthesia to avoid confounding effects of sedation, as well as pressure changes because of ventilation [17, 18]. Patients were asked to avoid caffeine for at least six hours before intervention to prevent influence of caffeine on the ICP [19].
Cerebral venous sinus catheterization
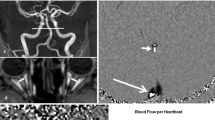
Right femoral venous access was gained through a 5 F introducer under local anesthesia. A 5 F catheter was placed in the IJV and a 0.021-inch Headway micro-catheter was navigated over a 0.014-inch Syncro micro-wire into the cerebral sinuses. Pressure was taken in the proximal S2 segment of the superior sagittal sinus (SSS), confluence of the sinus (Torcular), right and left transverse venous sinus (TVS) distal to the stenosis, right and left sigmoid venous sinus (SVS) proximal to the stenosis, right and left IJV, and in the right heart (CVP). Pressure measurement started at the SSS and then the micro-catheter was pulled back step-by-step to the other to-be-explored segments. The pressure gradient was calculated as the difference between the pressure measured at the confluence of the sinus and the pressure recorded at the sigmoid sinus proximal to the stenosis. Because the torcular is the confluence of the main cerebral sinus, its pressure gives us a single value that is thought to best summarize the cerebral venous pressure [6]. Pressure was recorded in mmHg. Navigation into the sinuses was performed following the bone landmarks without road-map guidance.
Cerebral venous sinus pressure measurement
The patient was positioned in dorsal decubitus and a pressure measurement system for central venous pressure was used for intracranial venous pressure and LPOP. First, the transducer was zeroed to atmospheric pressure, and it was placed at the level of the left external meatus (Fig. 1A). This is the standard landmark used to zero the pressure transducer when monitoring the ICP by an external ventricular drainage: the external meatus is considered to be in line with the foramen of Monro [20]. In addition, to ensure accurate pressure monitoring, care was taken to align the transducer placed at the external acoustic meatus (head in neutral position) with the phlebostatic axis which is located at the fourth intercostal space at the mid-anterior-posterior diameter of the chest wall: this is the approximate location of the right atrium and it is used to establish pressure in the circulatory system [21]. Air bubbles in the pressure tube were flushed [22]. During the pressure monitoring patients were instructed to avoid talking, holding breath, or performing a Valsalva maneuver. To assure accurate pressure evaluation, the micro-catheter was held in place in each segment for about 30 s and was flushed if catheter tip obstruction was doubted. Pressure was recorded on the anesthesiologist monitors. In case of unilateral hypoplastic venous sinus, pressure measurement was only performed when the microcatheter could be easily navigated inside the narrowed lumen. At the end of the procedure, compression was held on the venous access site.

(A-B). Patient position during cerebral venous pressure measurement (A): the transducer is zeroed to atmospheric pressure and is placed at the level of the left external meatus. Patient position during lumbar puncture opening pressure measurement (B): the pressure transducer is placed on the mid-sagittal line with the patient in left lateral decubitus
Opening pressure at lumbar puncture
Immediately after, the patient was rotated to the left lateral decubitus, flat on the interventional radiology table (Fig. 1B). Care was taken to position the head aligned with the spine: the external occipital protuberance (which is at the same level of the confluence of the sinus in lateral decubitus) [23] was aligned to the spine and the site of puncture. This line corresponds to the mid-sagittal line. The pressure transducer was placed on the mid-sagittal line that is considered the zero-level for the intraventricular pressure monitoring in lateral decubitus [20]. In addition, this line corresponds approximately with the phlebostatic point in the left lateral decubitus [24]. The head was straight (neutral position, neither flexed, nor extended) with moderate hip flexion to avoid the influence of the head and hip hyperflexion on the LPOP [25].
After local anesthesia, fluoroscopy was used to guide a 25-gauge atraumatic needle into the lumbar cistern at the L3L4 level. The CSF flow confirmed the intradural position of the needle and the LPOP was recorded with the pressure tube connected to the needle. During pressure monitoring patients were instructed avoid talking, holding breath, or performing a Valsalva maneuver. Measures were recorded for at least 60 s to reach the peak level of pressure, until stable reading with pulsations [26].
Statistical analysis
Categorical data were described by their frequency (%), whereas continuous data were summarized by their mean and standard deviation (SD). To compare pressure measures we performed a Pearson’s correlation analysis. Bland-Altman plots [27] were used evaluated the concordance between pressure measures and to verify the agreement between the two methods in subgroups of patients: (1) patients with a trans-stenotic pressure gradient < 8mmHg vs. ≥8mmHg; (2) and patients with a LPOP < 18mmHg vs. ≥18mmHg. All statistical analyses, descriptive and inferential, were performed with SPSS 29 (IBM, Armonk, NY).

Study flow chart
Results
Baseline population characteristics
From January 2021 to October 2023, 52 consecutive patients (46 women; median age, 31 years [IQR = 25–42]) with IIH suspicion received intracranial venous pressure measurement followed immediately by LPOP (Fig. 2). The mean body mass index was 32 (SD = ± 5.5). The mean symptoms duration was 28 months (SD = ± 36). Headache was reported in 50 patients (96%): being chronic in 40 (80%) and episodic in 10 (20%) patients. Other symptoms are reported in Table 1. Papilledema was confirmed in 39 patients (75%), with a mean Frisen grade of 1 in each eye. Loss of pituitary height was detected in 46 patients (88.5%) of which 6 (11.5%) exhibited a total empty sella. The median transverse diameter of the left and right Meckel cave was 4.2 mm [IQR = 3.6–5.3] and 4.1 mm [IQR = 3.5–4.7], respectively. Posterior globe flattening was detected in 29 (56%) patients, while optic nerve sheath distension was reported in 35 (67%) patients.
Thirty-nine patients received a definite diagnosis of IIH (modified Dandy criteria A to E); five patients had a probable diagnosis of IIH (modified Dandy criteria A to D); among the eight patients that did not present optic disc swelling, IIH without papilledema (IIHWOP) was suggested in five (LPOP > 18mmHg and presence of empty sella, flattening of the posterior aspect of the globe, distension of the perioptic subarachnoid space, and transverse venous sinus stenosis), while three patients were diagnosed with meningitis (Fig. 2).
There were neither technical failures during venous pressure measurement or LPOP, nor adverse events after venous pressure measurement or LPOP. All patients had some degree of TVS stenosis on MRI. That is, sixteen patients (31%) presented a bilateral TVS stenosis, 10 patients (19.5%) and 26 patients (50%) exhibited unilateral left and right TVS stenosis, respectively, with a hypoplastic contralateral one. The median degree of the left and right TVS stenosis was 0.79 [IQR = 0.72–0.82] and 0.79 [IQR = 0.68–0.84], respectively.
Intracranial venous pressure values
The mean pressure in the SSS and torcular were 20.9 mmHg (SD = ± 7.3) and 20.8 mmHg (SD = ± 6.8), respectively (Table 2). The mean pressure of the right TVS, right sigmoid sinus, and right IJV were 19.5mmHg (SD = ± 7.3), 10.5mmHg (SD = ± 3.1), and 9.6mmHg (SD = ± 2.6), respectively. The mean trans-stenotic pressure gradient on the right side was 9.8mmHg (SD = ± 6). The mean pressure of the left TVS, left sigmoid sinus, and left IJV were 19.5mmHg (SD = ± 6.2), 10.9mmHg (SD = ± 3), and 10.3mmHg (SD = ± 2.9), respectively. The mean trans-stenotic pressure gradient on the left side was 9.9mmHg (SD = ± 5.6). The central venous pressure was 8.6 mmHg (SD = ± 3.3).
Opening pressure at lumbar puncture
The mean LPOP was 22mmHg (SD ± 6.4). Thirteen patients (25%) had LPOP < 18mmHg, while 39 (75%) showed a pressure ≥18mmHg.
Correlation and concordance between intracranial venous pressure and opening pressure at lumbar puncture
Pressure measured in the right and left TVS, torcular, and SSS correlated with LPOP (p < 0.001). Pressure measured at LP was uncorrelated with the degree of stenosis (Table 3). The Bland-Altman analyses showed: a mean difference of 1.1 mmHg (central horizontal line, Fig. 3A) between the SSS pressure and the LPOP, with 94.3% of the data falling within the limits of agreement (LOA: mean difference ± 1.96SD); a mean difference of 1.71 mmHg between the torcular pressure and the LPOP (Fig. 3B), with 98.1% of the data within the LOA; a mean difference of 2.5mmHg the right TVS pressure and the LPOP (Fig. 3C), with 96.2% within the LOA; and finally a mean difference of 2.76 mmHg the left TVS pressure and the LPOP (Fig. 3D), with 98.1% within the LOA.

(A-B-C-D). Bland-Altman plots illustrating the agreement between the LPOP and cerebral venous pressure measured in the Superior Sagittal Sinus (A), Torcular (B), right (C) and left (D) Traverse Venous Sinus
Subgroup analysis
Figure 4A-B shows the Bland–Altman analysis of torcular and LPOP pressure agreement in patients having < 18mmHg (Fig. 3A) and ≥18mmHg LPOP (Fig. 4B). The concordance between the two measurements was significant in both groups with a comparable mean LPOP difference of 1.8mmHg for the < 18mmHg and 1.9mmHg for the ≥18mmHg group. Note that all measured values fell within the LOA.
Figure 4C-D shows the Bland–Altman plot analysis of torcular and LPOP pressure agreement for patients showing a trans-stenotic pressure gradient < 8mmHg (Fig. 4C) and ≥8mmHg (Fig. 4D). The concordance between the two measurements was significant in both groups, but with a mean difference of 1mmHg for the ≥8 mmHg group and 2.4mmHg for the < 8mmHg trans-stenotic pressure gradient group. Again, all measured values were within the LOA.

(A-B-C-D). Bland-Altman plots illustrating the agreement between the LPOP and pressure recorded in the torcular in the subgroups of patients with LPOP ≥ 18 mmHg (A) and < 18 mmHg (B), as well as in patients with a trans-stenotic pressure gradient ≥8 mmHg (C) and < 8 mmHg (D)
Discussion
In this large study with more than 50 consecutive cases, we directly confronted intracranial venous sinus pressure and LPOP, that were measured consecutively during the same procedure. First, we confirmed the relationship between venous sinus pressure and LPOP previously established, in a different center with a different method and different operators, confirming the generalizability of these findings. Second, and most importantly, intracranial venous pressure, and especially torcular pressure, is not only correlated, but also strongly agrees with the pressure measured at the LP. Finally, the mean difference between venous sinus pressure and LPOP was generally below 2 mmHg, except for patients that had a trans-stenotic pressure gradient below the clinical cut-off for venous stenting.
Previous large studies underlined the correlation between LPOP and venous manometry, but the main drawback of these series was that LP was performed in a separate setting, creating temporal and technical confounders [7, 8]. To overcome these pitfalls and reliably replicate the study of Lee and colleagues [6] we used a robust methodology: (1) patients were consecutive and LP was always concomitant to venous pressure measurement; (2) all the procedures were performed under pure local anesthesia, eliminating any confounders of the sedation; (3) the same size and type of spinal needle (25-gauge atraumatic needle), as well as the same micro-catheter (Headway 0.021inches) was used for all procedures; and (4) the same careful positioning of patient and instrument (pressure transducer) was adopted for venous and LP pressure measurements, rigorously respecting the zero point in dorsal and lateral decubitus (Fig. 2A-B). Unlike the study by Lee and colleagues, in which the LPOP was measured by a water column [6], in our study, the same pressure transducer was used to measure venous pressure and LPOP in mmHg. This methodology allowed to highlight a strong concordance between the two measures and a reproducibility of results in all the included patients. We demonstrated a general mean difference of only 1.7mmHg, whereby the pressure at LP was constantly above the torcular one. Moreover, the difference between the two methods was within the 95%CI in over 98% of the cases. The small but systematic difference in measured pressure makes sense as CSF reabsorption into the dural venous sinuses occurs via a pressure-dependent mechanism. CSF pressure must thus be slightly higher than the pressure in cerebral venous sinuses to allow the fluid to move through the arachnoid granulations into the veins.
There is a general consensus that a pressure gradient of at least 8mmHg highly predicts the efficacy of venous sinus stenting [28], despite some authors performing stenting for patients with pressure gradient ≥ 4mmHg [29]. An elevated LPOP is highly predictive of having a significant trans-stenotic pressure gradient, that is roughly 75% of the patients that show an LPOP ≥ 35cmH2O harbor a pressure gradient ≥ 8mmHg, versus 25% with a LPOP of ≤ 24cmH2O [7]. Interestingly, here we showed that independently of the trans-stenotic pressure gradient, the torcular pressure systematically agreed with the LPOP. Still, the difference in pressure was higher in patients with a pressure gradient below 8mmHg (1mmHg vs. 2.4mmHg). In general, higher trans-stenotic pressure gradients are associated with more pronounced ICP increases [30]. This is not surprising because the unidirectional flow of CSF through arachnoid granulations requires a 3–5mmHg pressure gradient from the subarachnoid space to the venous sinus [5, 31]. Accordingly, in case of cerebral venous hypertension, CSF pressure will concomitantly be elevated. This is in accordance with our observation that the difference between torcular pressure and LPOP, was higher (2.4mmHg) for patients with low gradients and smaller (∼ 1mmHg) for patients with high trans-stenotic pressure gradients. This low-pressure gradient between venous and CSF compartments will likely affect the capacity of CSF resorption, that is part of the complex mechanism of IIH. Canine models showed that under normal conditions the mean SSS pressure is approximately 0.6 of the CSF pressure, while in hydrocephalic dogs the ratio between SSS pressure and CSF pressure raised to 0.98, corroborating the theory that cerebral venous and CSF compartments are functionally related and that the pressure gradient between the two systems plays a pivotal role in the ICP homeostasis [32].
While a link between the degree of venous sinus stenosis and elevated ICP has been suggested [11], we were unable to confirm a consistent correlation and cannot further elaborate on the causality between both phenomenon. That said, there is still controversy in the literature whether venous sinus stenosis is a primary cause of IIH or a secondary manifestation. Especially as some patients with significant venous sinus stenosis do not exhibit elevated ICP, high-grade papilledema or headaches, while others with mild stenosis experience more important symptoms. This suggests that the presence of venous sinus stenosis alone is not always sufficient to cause an increase in ICP. It has therefore been suggested that compensatory mechanisms, like alternative venous drainage pathways or variations in venous anatomy mitigate the effects of venous sinus stenosis [33, 34]. Alternatively, it has been suggested that the extent and severity of venous sinus stenosis is associated with the degree of glymphatic clearance in IIH. A dysfunction of the glymphatic system is thereby thought to drive or exacerbate impaired CSF outflow or reabsorption [35].
Normal ICP is difficult to define, and it can vary with age and body position [36]. Accordingly, the critical ICP value is still a matter of debate [37]. In patients with suspected IIH, the LPOP of ≥25cmH2O in lateral decubitus is a diagnostic criteria of IIH [1]. Interestingly, although 25% of our patients had a ‘normal’ LPOP (< 18mmHg or < 25cmH2O), the agreement between torcular pressure and LPOP was maintained in these patients. This suggests that intracranial venous pressure may also be strongly related to CSF pressure in patients with normal ICP. In accordance, a consistent correlation between torcular and LP in patients with < 20cmH2O LPOP has already been described: that is almost 90% of patients with LPOP < 20cmH2O exhibited a torcular pressure < 18mmHg [6]. It may thus be likely that torcular pressure, being the confluent of the main cerebral sinuses, best summarizes the intracranial venous pressure and allows us to correlate venous pressure to CSF pressure. This is important because venous pressure measurement can be used not only to assess pressure gradient for stenting indication in IIH patients, but also as an alternative method to study and monitor ICP. This can be particularly useful in case of longitudinal follow-up of ICP in IIH patients, instead of repeated LP that is associated with post-dural puncture headache rates between 5% and 40%, based on technical and patients’ characteristics [38]. The venous approach may be also an alternative strategy in patients presenting LP contra-indications like for instance anticoagulant intake, morbid obesity, degenerative spine diseases, or scoliosis with deformity of the lumbar spine. Nevertheless, multicenter controlled studies should be performed to compare the benefit/risk ratios between venous (torcular) pressure-based follow-up and LP-based follow-up, as cerebral venous sinus navigation can be associated with increased risks of cerebral venous perforation [39], although we did not observe any in our patient group. Also, it should be taken into account that venous sinus navigation is more expensive and requires specialists trained in cerebral venous catheterization, limiting the availability of this technique compared to LP that can be performed by almost any physician with minimal costs. Accordingly, venous pressure manometry should be considered in specific cases needing stenting, or during post-stenting follow-up of the intracranial pressure and gradient in IIH patients.
Of course, this study also has its limitations. First, it is not known whether performing a LP immediately after invasive venous manometry may affect the accuracy of LPOP measurements. The invasive nature of manometry may cause stress and anxiety, which might affect physiological parameters such as blood pressure and intracranial pressure, potentially influencing LPOP readings. Second, we propose another single-center series, and pressure measurements, although performed by more than one neuroradiologist, were still performed by few. It is likely that variability in pressure measurement techniques due to different center preferences may affect the pressure values, as suggested by the difference between means between our study and Lee’s study [6]. Accordingly, the agreement between the two technics should equally be proven in multicenter studies.
Conclusions
Taken together, our study demonstrated that, in patients investigated for IIH, ICP measured at LP is consistent with the pressure detected in the torcular, confirming the generalizability of previous single center studies. Our findings corroborate the hypothesis that the cerebral venous system plays a major role in CSF dynamics and ICP. Torcular, being the confluent of the main cerebral sinuses, may summarize intracranial venous pressure and ICP. Clinically, the venous approach might thus be an interesting alternative method for ICP monitoring in patients with IIH, especially in case of patients with LP contra-indications.
Data availability
No datasets were generated or analysed during the current study.
Abbreviations
- BMI:
-
Body mass index
- CSF:
-
Cerebral spinal fluid
- CVP:
-
Central venous pressure
- ICP:
-
Intracranial pressure
- IIH:
-
Idiopathic intracranial hypertension
- IJV:
-
Internal jugular vein
- IQR:
-
Interquartile range
- LOA:
-
Limit of agreement
- LP OP:
-
Lumbar puncture opening pressure
- MRI:
-
Magnetic resonance imaging
- SD:
-
Standard deviation
- SSS:
-
Superior sagittal sinus
- SVS:
-
Sigmoid venous sinus
- TVS:
-
Transverse venous sinus
References
Friedman DI, Liu GT, Digre KB (2013) Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 81:1159–1165
Mollan SP, Grech O, Sinclair AJ (2021) Headache attributed to idiopathic intracranial hypertension and persistent post-idiopathic intracranial hypertension headache: a narrative review. Headache: J Head Face Pain 61:808–816
Markey KA, Mollan SP, Jensen RH, Sinclair AJ (2016) Understanding idiopathic intracranial hypertension: mechanisms, management, and future directions. Lancet Neurol 15:78–91
Fargen KM (2020) Idiopathic intracranial hypertension is not idiopathic: proposal for a new nomenclature and patient classification. J Neurointerv Surg 12:110–114
Pollay M (2010) The function and structure of the cerebrospinal fluid outflow system. Cerebrospinal Fluid Res 7:9
Lee K et al (2021) Correlation between intracranial pressure and venous sinus pressures in patients undergoing cerebral venography and manometry. J Neurointerv Surg 13:1162–1166
Fargen KM, Garner RM, Kittel C, Wolfe S (2020) Q. A descriptive study of venous sinus pressures and gradients in patients with idiopathic intracranial hypertension. J Neurointerv Surg 12:320–325
Kahan J et al (2021) Predicting the need for retreatment in venous sinus stenting for idiopathic intracranial hypertension. J Neurointerv Surg 13:574–579
Lalou A-D et al (2020) Coupling of CSF and sagittal sinus pressure in adult patients with pseudotumour cerebri. Acta Neurochir (Wien) 162:1001–1009
Liu J et al (2016) Correlation and agreement: overview and clarification of competing concepts and measures. Shanghai Arch Psychiatry 28:115–120
West JL et al (2019) Correlation between angiographic stenosis and physiologic venous sinus outflow obstruction in idiopathic intracranial hypertension. J Neurointerv Surg 11:90–94
Yuh WT et al (2000) MR imaging of pituitary morphology in idiopathic intracranial hypertension. J Magn Reson Imaging 12:808–813
Kwee RM, Kwee TC (2019) Systematic review and meta-analysis of MRI signs for diagnosis of idiopathic intracranial hypertension. Eur J Radiol 116:106–115
Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition - PubMed. https://pubmed.ncbi.nlm.nih.gov/29368949/
Frisén L (2017) Swelling of the Optic nerve head: a backstage view of a staging Scheme. J Neuroophthalmol 37:3–6
Yano I et al (1998) Pharmacokinetics and pharmacodynamics of acetazolamide in patients with transient intraocular pressure elevation. Eur J Clin Pharmacol 54:63–68
Raper DMS et al (2017) Intracranial venous pressures under conscious sedation and general anesthesia. J Neurointerv Surg 9:986–989
Fargen KM et al (2017) Comparison of venous sinus manometry gradients obtained while awake and under general anesthesia before venous sinus stenting. J Neurointerv Surg 9:990–993
Israelsen IME, Westgate CSJ, Kamp-Jensen C, Jensen RH, Eftekhari S (2023) Effects of caffeine on intracranial pressure and pain perception in freely moving rats. Headache 63:1220–1231
Greenberg MS (2016) Handbook of Neurosurgery. Thieme Medical Pub
Kee LL, Simonson JS, Stotts NA, Skov P (1993) Schiller, N. B. Echocardiographic determination of valid zero reference levels in supine and lateral positions. Am J Crit Care 2:72–80
Sjödin C, Sondergaard S, Johansson L (2019) Variability in alignment of central venous pressure transducer to physiologic reference point in the intensive care unit-A descriptive and correlational study. Aust Crit Care 32:213–217
Tsutsumi S, Ono H, Ishii H (2022) Correlation of the external occipital protuberance with venous sinuses: a magnetic resonance imaging study. Surg Radiol Anat 44:999–1006
Song I-K et al (2017) Reference levels for central venous pressure and pulmonary artery occlusion pressure monitoring in the lateral position. J Cardiothorac Vasc Anesth 31:939–943
Pedersen SH, Andresen M, Lilja-Cyron A, Petersen LG, Juhler M (2021) Lumbar puncture position influences intracranial pressure. Acta Neurochir (Wien) 163:1997–2004
Woo MS, Kessner SS, Schlemm E, Gerloff C (2022) Atraumatic spinal needle indicates correct CSF opening pressure. Sci Rep 12:21089
Bland JM, Altman DG (1986) Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1:307–310
Ahmed RM et al (2011) Transverse sinus stenting for idiopathic intracranial hypertension: a review of 52 patients and of model predictions. AJNR Am J Neuroradiol 32:1408–1414
Radvany MG et al (2013) Visual and neurological outcomes following endovascular stenting for pseudotumor cerebri associated with transverse sinus stenosis. J Neuroophthalmol 33:117–122
Inam ME et al (2022) Venous sinus stenting for low pressure gradient stenoses in idiopathic intracranial hypertension. Neurosurgery 91:734–740
Welch K, Friedman V (1960) The cerebrospinal fluid valves. Brain 83:454–469
Shulman K, Yarnell P, Ransohoff J (1964) Dural sinus pressure. In normal and hydrocephalic dogs. Arch Neurol 10:575–580
Eshtiaghi A, Zaslavsky K, Nicholson P, Margolin E (2022) Extent of transverse sinus stenosis does not predict visual outcomes in idiopathic intracranial hypertension. Eye (Lond) 36:1390–1395
Bono F, Quattrone A (2013) Clinical course of idiopathic intracranial hypertension with transverse sinus stenosis. Neurology 81:695
Schartz D, Finkelstein A, Bender M, Kessler A, Zhong J (2024) Association of Extent of transverse sinus stenosis with cerebral glymphatic clearance in patients with idiopathic intracranial hypertension. Neurology 103:e209529
Czosnyka M, Pickard JD (2004) Monitoring and interpretation of intracranial pressure. J Neurol Neurosurg Psychiatry 75:813–821
Brain Trauma, Foundation et al (2007) Guidelines for the management of severe traumatic brain injury. Introduction. J Neurotrauma 24(Suppl 1):S1–2
Uppal V et al (2023) Consensus Practice guidelines on Postdural puncture Headache from a Multisociety, International Working Group: a Summary Report. JAMA Netw Open 6:e2325387
Rk T et al (2022) Major complications of dural venous sinus stenting for idiopathic intracranial hypertension: case series and management considerations. J Neurointerventional Surg 14
Acknowledgements
Not applicable.
Funding
No funding to declare.
Author information
Authors and Affiliations
Contributions
FC: project coordination, data analysis, interpretation and manuscript writing; MV: data acquisition, project coordination and interpretation; LVD: manuscript writing, data analysis; RAR: data acquisition and data analysis; RC: data acquisition and data analysis; GG: data acquisition and data analysis; CD: data acquisition and data analysis; PHL: data acquisition and data analysis; ELB: MRI data aquisition and analysis; GR: data acquisition, data analysis; NM: project coordination and interpretation; AD project coordination and interpretation; VC: project coordination and interpretation. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This retrospective study was approved by the local ethical committee (IRB-MTP_2023_01_202201315). All procedures were in line with the declaration of Helsinki. All participants received an information letter and gave consent by non-opposition.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License, which permits any non-commercial use, sharing, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if you modified the licensed material. You do not have permission under this licence to share adapted material derived from this article or parts of it. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by-nc-nd/4.0/.
About this article

Cite this article
Cagnazzo, F., Villain, M., van Dokkum, L.E. et al. Concordance between venous sinus pressure and intracranial pressure in patients investigated for idiopathic intracranial hypertension. J Headache Pain 25, 153 (2024). https://doi.org/10.1186/s10194-024-01865-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s10194-024-01865-5