
Abstract
Background
Persons experiencing homelessness (PEH) often use hospital Emergency Department (ED) as the only source of healthcare. The aim of this study was to undertake a systematic review to identify the prevalence, clinical reasons and outcomes in relation to ED visits by PEH.
Methods
A protocol-led (CRD42020189263) systematic review was conducted using search of MEDLINE, EMBASE, CINAHL and Google Scholar databases. Studies that reported either the prevalence of homelessness in the ED or clinical reasons for presentation to ED by PEH and published in English language were included. Definitions of homelessness used by study authors were accepted.
Results
From the screening of 1349 unique titles, a total of 36 studies were included. Wide variations in the prevalence and key cause of presentations were identified across the studies often linked to differences in country, study setting, disease classification and data collection methods. The proportion of ED visits contributed by PEH ranged from 0.41 to 19.6%. PEH made an average of 0.72 visits to 5.8 visits per person per year in the ED [rate ratio compared to non-homeless 1.63 to 18.75]. Up to a third and quarter of the visits were contributed by alcohol-related diagnoses and substance poisoning respectively. The percentage of PEH who died in the ED ranged from 0.1 to 0.5%.
Conclusions
Drug-, alcohol- and injury-related presentations dominate the ED visits by PEH. Wide variations in the data were observed in regard to attendance and treatment outcomes. There is a need for prevention actions in the community, integrated discharge and referral pathways between health, housing and social care to minimise frequent usage and improve attendance outcomes.
Similar content being viewed by others


Introduction
The global prevalence of homelessness is estimated to be around 2%, with approximately 150 million people experiencing homelessness. Additionally, 20% of the world’s population are estimated to lack adequate housing [1]. The definition of homelessness differs between countries. The US Department of Housing and Urban Development (HUD) defines homelessness as the lack of a fixed, regular and adequate night-time residence [2]. In the UK, the statutory definition of homelessness includes those living in temporary shelters, hostels and squats; street dwellers or those living (sofa surfing) in family and friends’ houses; and those who currently have an accommodation but are not able to ‘reasonably occupy’ it due to threat of eviction or violence [3, 4]. Homelessness has been on the rise in industrial economies and particularly those street dwelling in urban areas since the 2010 global recession. In the USA, it is known that approximately 1.5 million people experience homelessness every year [5]. In England, over 200,000 households experience homelessness every year [6].
Statistics show that approximately 25% of persons experiencing homelessness (PEH) have a diagnosis of at least one serious mental illness. These include bipolar disorder, schizophrenia, major depression and post-traumatic stress disorder [7]. Multi-morbidity, defined as the presence of multiple, simultaneous, chronic conditions, is also highly prevalent in PEH [8]. The average life expectancy among the homeless population in the USA is a mere 48 years [7], and in the UK, the mean age at death is 45 years for males and 43 years for females [9]. Cardiovascular health conditions, drug overdose and accidents have been recorded as contributing factors to the higher mortality rates seen in this community [9].
There remain important disparities in access to health between PEH and non-homeless populations. One US study reported that one in four homeless respondents had been unable to access medical care when they required it [10]. In England, PEH are approximately 40 times less likely to be registered with a mainstream general practice than non-homeless persons [11]. Physical and mental inability to navigate services, healthcare costs and perceived stigma surrounding PEH when accessing these services have been shown to be significant barriers to accessing primary healthcare. These barriers to accessing primary healthcare and substance misuse services are known to contribute to higher rates of utilisation of the emergency department (ED) by PEH [8, 12]. The ED, however, represents a high cost and resource intense environment, making it challenging for healthcare professionals to care for PEH who often have a multitude of diagnosed and undiagnosed health conditions, in addition to poor social circumstances. It is imperative that service providers are acquainted with up-to-date evidence in relation to homelessness and its relationship with causes, pattern, frequency and outcomes of ED presentations. Comparison of PEH data with the general population can enable identification of the extent of disparity in access and outcomes.
Currently, there lacks a comprehensive systematic review which incorporates the range of literature on patient experience of homelessness and its link to the utilisation of ED for healthcare. PEH often frequent urban areas and streets and many are known to use the ED as their only source of healthcare. In particular, the prevalence of homelessness among users of the ED, frequency of (repeat) visits to the ED by PEH, primary reasons for presentation and mortality outcomes of PEH in the ED have not been synthesised using systematic review methodology. The aim of this study is to undertake a systematic review to identify the prevalence of ED visits made by PEH, primary reasons for presentation to the ED and associated prevalence, and mortality (deaths) of PEH in the ED. This study will also aim to compare the data with non-homeless populations from the same study setting where available.
Methods
Study design and method
This study was conducted according to the PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses) guideline (Additional file 1). A protocol was registered with PROSPERO (CRD42020189263).
Data source and selection process
A systematic search of the literature was undertaken in MEDLINE, Embase, CINAHL and Google Scholar databases published between 2009 and October 2020. The key search terms and medical subject headings included homelessness, homeless persons, emergency department, accident and emergency (Additional file 2).
Inclusion and exclusion criteria
Studies were included if they were primary research studies of any design, including prospective observational studies, retrospective database review and interventional studies that reported either the prevalence of homelessness in persons who present to the ED or reasons for presentation to ED by PEH, and published in English language. The definitions of homelessness used by study authors were accepted for the purpose of the review.
Study selection
All stages of the screening and selection process were carried out according to the inclusion and exclusion criteria. Title and abstract screening were followed by full-text screening. Two reviewers (NV and VP) undertook the screening.
Data extraction and quality assessment
The data extraction form was developed based on the review’s aims and objectives. The tool was refined, reviewed and piloted before use. The following information was extracted: study author(s), study year, study country, study aims, study design and duration, setting and study population, number and/or proportion of unique patients from the study populations identified as PEH, number and/or proportion of visits to the ED contributed by PEH, primary reason for presentation to the ED by PEH including number and proportions, mean number of ED visits per person per year, and deaths of PEH in the ED. Data were also extracted for non-homeless populations from the same study setting where available for the purpose of comparison.
Quality assessment of the included studies was conducted by two authors (NV and VP) using an adapted tool developed to assess quality of prevalence studies [13]. The tool consisted of 10 risk of bias items and included quality criteria referring to the target population representativeness, non-response bias, appropriateness of numerator(s) and denominator(s) for the parameters and summary of the overall risk of bias. The summary of the overall risk gives each study a total score from 0 to 9 which classifies each study into either low risk of bias (0–3 points), moderate risk of bias (4–6 points) or high risk of bias (7–9 points) [13].
Data synthesis and analysis
Where sufficient data were reported, the prevalence of homelessness among the ED attendees was calculated for each study in two ways: (a) the number of unique PEH attending the ED was divided by the total number of unique persons attending the ED during the study period and (b) the number of ED visits by PEH was divided by the total number of ED visits during the study period.
Meta-analysis was planned for the following category of data including the prevalence of presentations to the ED contributed by PEH, the primary reasons for presentation to the ED (%), the mean number of visits to the ED by homeless persons, per person, per year [14], and the number of deaths of homeless persons in the ED. However, due to the high levels of heterogeneity, it was decided that meta-analysis was not appropriate.
A number of studies reported the mean number of ED visits but few reported the standard deviation. We used the mean number of ED visits in each group together with the study follow-up period to calculate the mean yearly attendance rates. We then calculated the log rate ratio and its standard error assuming a Poisson distribution for the rate in each group. These were then exponentiated.
Results
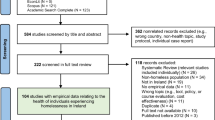
The electronic searches returned a total of 1726 records, from which 1349 unique titles were screened for full texts, of which 36 studies [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50] fulfilled the eligibility criteria and were included (Fig. 1). The majority of these studies were published in the USA (n = 27), followed by Australia (n = 4), the UK (n = 1), Canada (n = 1), Turkey (n = 1), Ireland (n = 1) and Finland (n = 1) (Table 1).

PRISMA flowchart
Quality assessment measuring risk of bias
Of the 36 included studies, only 8 studies received a score of 0 for all the risk of bias criteria. Risk of bias criteria were lacking in relation to generalisability of the study findings to the wider populations. This was often due to the study populations belonging to one or a few hospitals in a single city. Non-response bias was unclear where survey or interview methodologies were used to collect data (Table 2).
Overview of included studies and study populations
Twelve studies reported secondary analysis of existing national data sources, including the National Hospital Ambulatory Care Survey (NHAMCS) [15, 16, 20, 22, 32, 40, 49], National Electronic Injury Surveillance System (NEISS) [29], Veterans Affairs (VA) administrative data [26, 35] and Veterans Health Administration (VHA) databases [41, 47]. The extent of data overlap across studies which used similar databases could not be accurately estimated due to lack of clarity in the data inclusion criteria (Table 1). A further ten studies used retrospective analysis of secondary data sources focusing on smaller sub-populations such as one or a few hospital EDs [28, 33, 37,38,39, 42, 43, 45, 48, 50]. Six studies used a combination of both retrospective sampling techniques and prospective data collection, such as interviews or surveys [19, 21, 24, 34, 44, 46] and five studies prospectively interviewed or assessed patients presenting to the ED [17, 23, 27, 30, 31]. One study employed both a secondary analysis of retrospective data and prospective screening of a sample at one inner metropolitan hospital ED [25]. Some studies focused on only one presentation, such as injuries [29], as the cause of ED presentation by PEH (Table 1).
Prevalence of homelessness in the ED
A total of 30 studies included data on the prevalence of homelessness in the ED, either reporting the proportion of unique patients who were experiencing homelessness or the proportion of ED visits made by PEH (Tables 3 and 4). Four studies reported both patient-level and visit-level data [31, 42, 45, 48]. The proportion of ED visits contributed by PEH ranged from 0.41% [15, 16] in two retrospective studies analysing NHAMCS data for 2005 to 19.6% [30] in a prospective study which assessed a random sample of patients presenting to an urban public hospital ED.
Four studies focused on the utilisation of the ED by veterans experiencing homelessness [26, 35, 41, 47]. Three of these studies used national veterans’ affairs (VA) administrative data [26, 35, 41]. Two of these studies reported that veterans experiencing homelessness contributed to approximately 6.9% of all ED visits made by homeless persons [26, 35]. One study [51] found that homeless VA service users were approximately three times more likely to use the ED than domiciled VA service users.
Mean number of visits to the ED by PEH in a year
Ten studies reported data on the mean number of visits to the ED per person, per annum, among the PEH. The value ranged from 0.72 visits to 5.8 visits per PEH, per year within the study period (Table 5). Five studies compared the mean number of visits to the ED between PEH and non-homeless populations, with the number of visits being consistently higher in the PEH compared with the non-homeless population [15, 22, 26, 27, 37]. Rate ratio ranged from 1.63 to 18.75 (Fig. 2). A study conducted in the USA also demonstrated that the proportion of ED visits contributed by PEH were rising at a faster pace than the non-homeless populations [15].

Rate ratio of number of ED visits per person, per year made by PEH compared with non-homeless populations. ED, emergency department; PEH, persons experiencing homelessness
Reasons for presentation to the ED by PEH
Nineteen studies reported the primary reasons for presentation to the ED by PEH. Nine studies had a comparator group, providing the reasons for presentation to the ED among both PEH and non-homeless populations, allowing data comparisons [15, 22, 27, 29, 35, 37, 40, 48, 50].
The proportion of ED visits contributed by alcohol-related diagnoses ranged from 8% to 34% with four studies reporting a prevalence between 8.0% and 15.2%. The fifth study by Holtyn et al. [17] which reported 34% of visits contributed by alcohol-related diagnosis also used random breath collection in addition to self-reports. Among the two studies which compared homeless and non-homeless presentations, the relative risks (RR) ranged from 4.73 [50] to 6.83 [26].
The proportion of visits contributed by drugs, poisoning and substance misuse-related presentations ranged from 1.1% to 25%. Out of the three studies which compared PEH with non-homeless populations, RRs ranged from 1.05 [50] to 9.54 [26].
Injury-related diagnoses contributed between 7.8% and 55% of diagnoses. Among the two studies which compared the injury-related presentations between PEH and non-homeless populations, the RR ranged from 0.67 [50] to 1.55 [22].
The proportion of visits for pain or due to the need of analgesia ranged from 13% to 28%. Two studies which compared this data with non-homeless persons reported RRs of 0.92 [50] and 1.41 [26].
The proportion of ED visits attributed to non-substance misuse-related psychiatric and mental health-related conditions ranged from 5.8% to 36%. Out of the three studies which reported both homeless and non-homeless data, the RR ranged from 1.22 [22] to 4.42 [40]. One study using a veterans homeless population dataset showed that a high prevalence of psychiatric and mental health-related conditions contributed to the ED visits [26].
The proportion of patients presenting to the ED for cardiovascular conditions among the PEH ranged from 1.1% [40], in a study using national population data from the NHAMCS database, to 28% in a study utilising a homeless veteran dataset [26]. The RR, when comparing this value to non-homeless persons, ranged from 0.89 [26] to 1.03 [40].
Respiratory conditions contributed between 1.8% of ED attendance, in a study using national population data from the NHAMCS database, [40] to 15% in a study evaluating data of those brought by ambulance and non-trauma-related attendance [38]. Three studies reported both PEH and non-homeless data, producing RRs which ranged from 0.63 [40] to 1.01 [26].
Deaths of PEH in the ED
Four studies reported the number of homeless patients who died in the ED [29, 33, 37, 50]. The percentage of deaths reported by homeless persons in the ED ranged from 0.1% [37, 50] to 0.5% [33]. Three studies compared the proportion of homeless and non-homeless patients who died in the ED, producing RRs ranging from 0.13 [37] to 5.00 [29] (Fig. 3).

Relative risk of deaths in PEH attending the ED compared to non-homeless populations. ED, emergency department; PEH, persons experiencing homelessness
Discussion
This study summarises the nature, extent and outcomes of presentations to the ED by PEH using systematic review methodology. PEH experience fragmentation of services, are often denied healthcare based on eligibility criteria and costs, and face stigma and discrimination at healthcare settings [12, 51,52,53,54]. Tailored services, including outreach-based interventions that are able to deliver primary healthcare to patients’ temporary residence or in the urban streets where they frequent, are likely to bring positive changes and minimise the need for ED visits [55]. Such outreach services can also minimise physical and disability-related barriers to accessing primary healthcare.
Injury-related diagnoses were one of the most common reasons for presentation to the ED among PEH. Consistent with previous findings, PEH suffer a disproportionate burden of injuries compared to non-homeless persons [32]. Mental health and psychiatric-related diagnoses were identified as another important primary reason for presentation to the ED. Psychiatric diagnoses were particularly prevalent in homeless veterans [26]. A previous study has shown than severe mental health is more prevalent in veteran populations than non-veteran populations [56].
Only four papers reported on the number of deaths among PEH in the ED. Recent literature has reported that a very high proportion of PEH leave the ED before being treated [51]. Further research is required to obtain a more accurate comparison of the death rates in the ED between PEH and the general population. This comparison may provide useful insights regarding the severity of health conditions when PEH present to the ED and offer a comparison between the standard of care received by PEH in the ED versus the non-homeless population.
This study has illustrated that injury-, mental health- and substance misuse-related health conditions dominate the reasons for presentations to the ED by PEH. This highlights the importance of factoring homelessness into the ED triage prioritisation process to improve patient outcomes. There is a continued need to improve the provision and implementation of mental health- and psychiatric-related support in the community. Furthermore, ED service providers should work closely with primary healthcare services to break down barriers to accessing healthcare among homeless populations. PEH are known to be less likely to be registered with a mainstream general practice compared with the general population. Although specialist primary healthcare centres for homeless persons have been established in an attempt to address such disparities, there is a need for the mainstream services to be more inclusive of homeless populations [54].
The COVID-19 pandemic has resulted in job losses and increases in domestic violence which is likely to result in a rise in homelessness. Therefore, public services must identify those who are in an unstable housing situation and assist them before they are pushed into homelessness [57, 58]. Innovative methods of support offered to PEH during the pandemic need to be sustained, for example emergency housing and the use of technology-assisted methods of counselling and communication, [59]. Strengthening primary care, including specialist homelessness services [60], community pharmacy [61], and enabling ED personnel to triage and treat PEH for overlapping health conditions, is imperative to prevent ill health and promote outcomes when they present to the ED. Clinical guidelines need to be further inclusive of multi-morbidity, including dual diagnosis of substance misuse and mental health, to prevent and mitigate the impact of homelessness on health [62]. Further research should include outreach-based innovative and integrated interventions offering preventative services and healthcare that can promote health, offer early diagnoses and treatment, and minimise ED attendance [63, 64].
Limitations
This systematic review has some limitations. Homelessness status is often based upon self-reported data [15, 51]. In addition, PEH who reside in temporary shelters such as emergency accommodation, hostels or charity services may use corresponding addresses when presenting to the ED. Therefore, within the included studies, it is likely that street dwellers are more commonly identified as PEH in the ED records compared with patients experiencing other forms of homelessness. Many patients may also be using the postcode of their last permanent domicile when presenting to health services. As a result, the numbers presented in the literature likely underestimate the actual number of attendances made by PEH. The definition of homelessness also varies between countries and study settings. In addition, psychiatric-, substance misuse-, alcohol- and injury-related presentations often overlap when reporting primary reasons for presentation to the ED. Therefore, it may be useful to apply specific classification methods to record the primary reason for presentation in order to prevent such overlap. Data overlap was observed across studies included in this review which used the same database for the study purpose. Furthermore, some of the studies relied on self-reported data gathered through interviews [52]. In addition, the included studies represented a small number of countries where the studies were conducted.
Conclusions
Drug-, alcohol- and injury-related presentations dominate the reasons for ED visits by PEH. Wide variations in the data were observed in regard to attendance and treatment outcomes. There is a need for an integrated discharge and referral pathway between ED and primary health, housing and social care to minimise frequent usage and improve attendance outcomes.
Availability of data and materials
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PEH:
-
Persons experiencing homelessness
- ED:
-
Emergency department
- HUD:
-
Housing and Urban Development
- NHAMCS:
-
National Hospital Ambulatory Care Survey
- NEISS:
-
National Electronic Injury Surveillance System
- VA:
-
Veterans Affairs
- VHA:
-
Veterans Health Administration
- RR:
-
Relative risk
References
Chamie J. As cities grow, so do the numbers of homeless. 2017. Available at: https://archive-yaleglobal.yale.edu/content/cities-grow-so-do-numbers-homeless. Accessed July 20, 2021.
HUD. Criteria and recordkeeping requirements for definition of homelessness. 2012. Available at: https://www.hudexchange.info/resource/1974/criteria-and-recordkeeping-requirements-for-definition-of-homeless/. Accessed July 20, 2021.
FEANTSA. ETHOS. European typology on homelessness and housing exclusion. 2005. Available at: https://www.feantsa.org/en/toolkit/2005/04/01/ethos-typology-on-homelessness-and-housing-exclusion. Accessed 10 Apr 2021.
Allison C. UK official statistics on homelessness: comparisons, definitions, and processes. 2019. Available at: https://gss.civilservice.gov.uk/policy-store/homelessness/. Accessed April 10, 2021.
Henry M, Mahathey A, Takashima M. The 2018 annual homeless assessment report (AHAR) to congress. Part 2: estimates of homelessness in the United States. 2020. Available at: https://www.huduser.gov/portal/sites/default/files/pdf/2018-AHAR-Part-2.pdf. Accessed June 1, 2021.
Crisis UK. About homelessness. Available at: https://www.crisis.org.uk/ending-homelessness/about-homelessness/. Accessed July 20, 2021.
Health Care for the Homeless. Homelessness makes you sick. 2021. Available at: https://www.hchmd.org/homelessness-makes-you-sick. Accessed July 20, 2021.
Bowen M, Marwick S, Marshall T, et al. Multimorbidity and emergency department visits by a homeless population: a database study in specialist general practice. BJGP. 2019;69(685):e515–25.
Office for National Statistics. Deaths of homeless people in England and Wales 2019 registrations. 2020. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsofhomelesspeopleinenglandandwales/2019registrations. Accessed April 10, 2021.
Kushel MB, Vittinghoff E, Haas J. Factors associated with the health care utilization of homeless persons. JAMA. 2001;285(2):200–6.
Elwell-Sutton T, Fok J, Albanese F, et al. Factors associated with access to care and healthcare utilization in the homeless population of England. J Public Health. 2017;39(1):26–33.
Gunner E, Chandan SK, Marwick S, et al. Provision and accessibility of primary healthcare services for people who are homeless: a qualitative study of patient perspectives in the UK. BJGP. 2019;69(685):e526–36.
Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, et al. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. J Clin Epidemiol. 2012;65(9):934–9.
Higgins JPT, Thompson SG, Spiegelhalter DJ. A re-evaluation of random-effects meta-analysis. J R Stat Soc Series A. 2009;172(1):137–59.
Tadros A, Layman SM, Brewer MP, et al. A 5-year comparison of ED visits by homeless and nonhomeless patients. Am J Emerg Med. 2016;34(5):805–8.
Oates G, Tadros A, Davis SM. A comparison of national emergency department use by homeless versus non-homeless people in the United States. JHCPU. 2009;20(3):840–5.
Holtyn AF, Jarvis BP, Subramaniam S, et al. An intensive assessment of alcohol use and emergency department utilization in homeless alcohol-dependent adults. Drug Alcohol Depend. 2017;178:28–31.
Brown AJ, Goodacre SW, Cross S. Do emergency department attendances by homeless people increase in cold weather? EMJ. 2010;27(7):526–9.
Cheung A, Somers JM, Moniruzzaman A, et al. Emergency department use and hospitalizations among homeless adults with substance dependence and mental disorders. Addict Sci Clin Pract. 2015;10(1):17.
Brown RT, Steinman MA. Characteristics of emergency department visits by older versus younger homeless adults in the United States. Am J Public Health. 2013;103(6):1046–51.
Raven MC, Tieu L, Lee CT, et al. Emergency department use in a cohort of older homeless adults: results from the HOPE HOME study. Acad Emerg Med. 2017;24(1):63–74.
Ku BS, Scott KC, Kertesz SG, et al. Factors associated with use of urban emergency departments by the U.S. homeless population. Public Health Rep. 2010;125(3):398–405.
Feldman BJ, Calogero CG, Elsayed KS, et al. Prevalence of homelessness in the emergency department setting. West J Emerg Med. 2017;18(3):366–72.
Jackson TS, Moran TP, Lin J, et al. Homelessness among patients in a Southeastern Safety Net Emergency Department. South Med J. 2019;112(9):476–82.
Lee SJ, Thomas P, Newnham H, et al. Homeless status documentation at a metropolitan hospital emergency department. Emerg Med Aust. 2019;31(4):639–45.
Tsai J, Doran KM, Rosenheck RA. When health insurance is not a factor: national comparison of homeless and nonhomeless US veterans who use Veterans Affairs Emergency Departments. Am J Public Health. 2013;103(S2):S225–31.
Rodriguez RM, Fortman J, Chee C, et al. Food, shelter and safety needs motivating homeless persons’ visits to an urban emergency department. Ann Emerg Med. 2008;53(5):598–602.e1.
Lin W, Bharel M, Zhang J, et al. Frequent emergency department visits and hospitalizations among homeless people with Medicaid: implications for Medicaid expansion. Am J Public Health. 2015;105 Suppl 5(S5):S716–22.
Mackelprang JL, Graves JM, Rivara FP. Homeless in America: injuries treated in US emergency departments. Int J Inj Control Saf Promot. 2014;21(3):289–97.
Doran KM, Kunzler NM, Mijanovich T, et al. Homelessness and other social determinants of health among emergency department patients. J Sociol. 2016;25(2):71–7.
Moore G, Hepworth G, Weiland T, et al. Prospective validation of a predictive model that identifies homeless people at risk of re-presentation to the emergency department. AENJ. 2012;15(1):2–13.
Hammig B, Jozkowski K, Jones C, et al. Injury-related visits and comorbid conditions among homeless persons presenting to emergency departments. Acad Emerg Med. 2014;21(4):449–55.
Mackelprang JL, Qiu Q, Rivara FP. Predictors of emergency department and inpatient readmissions among homeless adolescents and young adults. Med Care. 2015;53(12):1010–7.
Feldman BJ, Craen AM, Enyart J, et al. Prevalence of homelessness by gender in an emergency department population in Pennsylvania. JOM. 2018;118(2):85–91.
Tsai J, Rosenheck RA. Risk factors for ED use among homeless veterans. Am J Emerg Med. 2013;31(5):855–8.
Moulin A, Evans EJ, Xing G, et al. Substance use, homelessness, mental illness and Medicaid coverage: a set-up for high emergency department utilization. West J Emerg Med. 2018;19(6):902–6.
Ní Cheallaigh C, Cullivan S, Sears J, et al. Usage of Unscheduled Hospital Care by Homeless Individuals in Dublin, Ireland: A Cross-Sectional Study. BMJ Open. 2017;7(11):e016420.
Yeniocak S, Kalkan A, Sogut O, et al. Demographic and clinical characteristics among Turkish homeless patients presenting to the emergency department. Turk J Emerg Med. 2017;17(4):136–40.
Lloyd C, Hilder J, Williams PL. Emergency department presentations of people who are homeless: the role of occupational therapy. BJOT. 2017;80(9):533–8.
Lombardi K, Pines JM, Mazer-Amirshahi M, et al. Findings of a national dataset analysis on the visits of homeless patients to US emergency departments during 2005-2015. Public Health. 2020;178:82–9.
Hastings SN, Smith VA, Weinberger M, et al. Health services use of older veterans treated and released from Veterans Affairs Medical Center emergency departments. J Am Geriatr Soc. 2013;61(9):1515–21.
Lam CN, Arora S, Menchine M. Increased 30-day emergency department revisits among homeless patients with mental health conditions. West J Emerg Med. 2016;17(5):607–12.
Stenius-Ayoade A, Haaramo P, Erkkilä E, et al. Mental disorders and the use of primary health care services among homeless shelter users in the Helsinki metropolitan area, Finland. BMC Health Serv Res. 2017;17(1):428.
Post L, Vaca FE, Doran KM, et al. New media use by patients who are homeless: the potential of mHealth to build connectivity. J Med Internet Res. 2013;15(9):e195.
Moore G, Gerdtz MF, Hepworth G, et al. Homelessness: patterns of emergency department use and risk factors for re-presentation. EMJ. 2011;28(5):422–7.
Doran KM, Rahai N, McCormack RP, et al. Substance use and homelessness among emergency department patients. Drug Alcohol Depend. 2018;188:328–33.
Doran K, Raven MC, Rosenheck RA. What drives frequent emergency department use in an integrated health system? National data from the Veterans Health Administration. Ann Emerg Med. 2013;62(2):151–9.
Ku BS, Fields JM, Santana A, et al. The urban homeless: super-users of the emergency department. Popul Health Manag. 2014;17(6):366–71.
Coe AB, Moczygemba LR, Harpe SE, et al. Homeless patientsʼ use of urban emergency departments in the United States. J Ambul Care Manag. 2015;38(1):48–58.
Amato S, Nobay F, Amato DP, et al. Sick and unsheltered: homelessness as a major risk factor for emergency care utilization. Am J Emerg Med. 2019;37(3):415–20.
Paudyal V, Ghani A, Shafi T, et al. Clinical characteristics, attendance outcomes and deaths of homeless persons in the emergency department: implications for primary health care and community prevention programmes. Public Health. 2021;196:117–23.
Salhi BA, White MH, Pitts SR, et al. Homelessness and emergency medicine: a review of the literature. Acad Emerg Med. 2018;25(5):577–93.
Paudyal V, MacLure K, Buchanan C, et al. ‘When you are homeless, you are not thinking about your medication, but your food, shelter or heat for the night’: behavioural determinants of homeless patients’ adherence to prescribed medicines. Public Health. 2017;148:1–8.
Smith KG, Paudyal V, MacLure K, et al. Relocating patients from a specialist homeless healthcare centre to general practices: a multi-perspective study. BJGP. 2018;68(667):e105–13.
Lowrie R, Stock K, Lucey S, et al. Pharmacist led homeless outreach engagement and non-medical independent prescribing (rx) (PHOENIx) intervention for people experiencing homelessness: a non-randomised feasibility study. Int J Equity Health. 2021;20(1):19.
Pemberton MR, Forman-Hoffman VL, Lipari RN, et al. Prevalence of past year substance use and mental illness by veteran status in a nationally representative sample. SAMHSA Center for Behavioral Health Statistics and Quality. 2016. Available: https://www.samhsa.gov/data/sites/default/files/NSDUH-DR-VeteranTrends-2016/NSDUH-DR-VeteranTrends-2016.htm#:~:text=With%20respect%20to%20mental%20health,8.5%20percent. Accessed 12 June 2022.
British Medical Association. Impact of COVID-19 (coronavirus) on homelessness and the private rented sector. 2020. https://committees.parliament.uk/work/271/impact-of-covid19-coronavirus-on-homelessness-and-the-private-rented-sector/. Accessed 14 November 2011.
Paudyal V, Saunders K. Homeless reduction act in England: impact on health services. Lancet. 2018;392(10143):195–7.
Kaur S, Jagpal P, Paudyal V. Provision of services to persons experiencing homelessness during the COVID-19 pandemic: a qualitative study on the perspectives of homelessness service providers. Health Soc Care Commun. 2021.
Khan A, Kurmi O, Lowrie R, et al. Medicines prescribing for homeless persons: analysis of prescription data from specialist homelessness general practices. Int J Clin Pharm. 2022;23:1–8.
Paudyal V, Hansford D, Cunningham S, et al. Pharmacists’ perceived integration into practice of over-the-counter simvastatin five years post reclassification. Int J Clin Pharm. 2012;34(5):733–8.
Alsuhaibani R, Smith DC, Lowrie R, et al. Scope, quality and inclusivity of international clinical guidelines on mental health and substance misuse in relation to dual diagnosis, social and community outcomes: a systematic review. BMC Psychiatry. 2021;21(209):2021.
Jagpal P, Barnes N, Lowrie R, et al. Clinical pharmacy intervention for persons experiencing homelessness: evaluation of patient perspectives in service design and development. Pharmacy. 2019;7:153.
Jagpal P, Saunders K, Plahe G, et al. Research priorities in healthcare of persons experiencing homelessness: outcomes of a national multi-disciplinary stakeholder discussion in the United Kingdom. Int J Equity Health. 2020;19(1):1–7.
Acknowledgements
None.
Funding
None.
Author information
Authors and Affiliations
Contributions
NV: acquisition of the data, analysis and interpretation of the data and drafting of the manuscript; MJP: analysis and interpretation of the data, critical revision of the manuscript for important intellectual content and statistical expertise; VP: concept and design, analysis and interpretation of the data, drafting of the manuscript, critical revision of the manuscript for important intellectual content and acquisition of funding. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Additional file 1.
PRISMA Checklist (contains completed checklist).
Additional file 2.
Example Search strategy.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated in a credit line to the data.
About this article

Cite this article
Vohra, N., Paudyal, V. & Price, M.J. Homelessness and the use of Emergency Department as a source of healthcare: a systematic review. Int J Emerg Med 15, 32 (2022). https://doi.org/10.1186/s12245-022-00435-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s12245-022-00435-3